Impact of Training Protocols on Lifting Velocity Recovery in Resistance Trained Males and Females



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
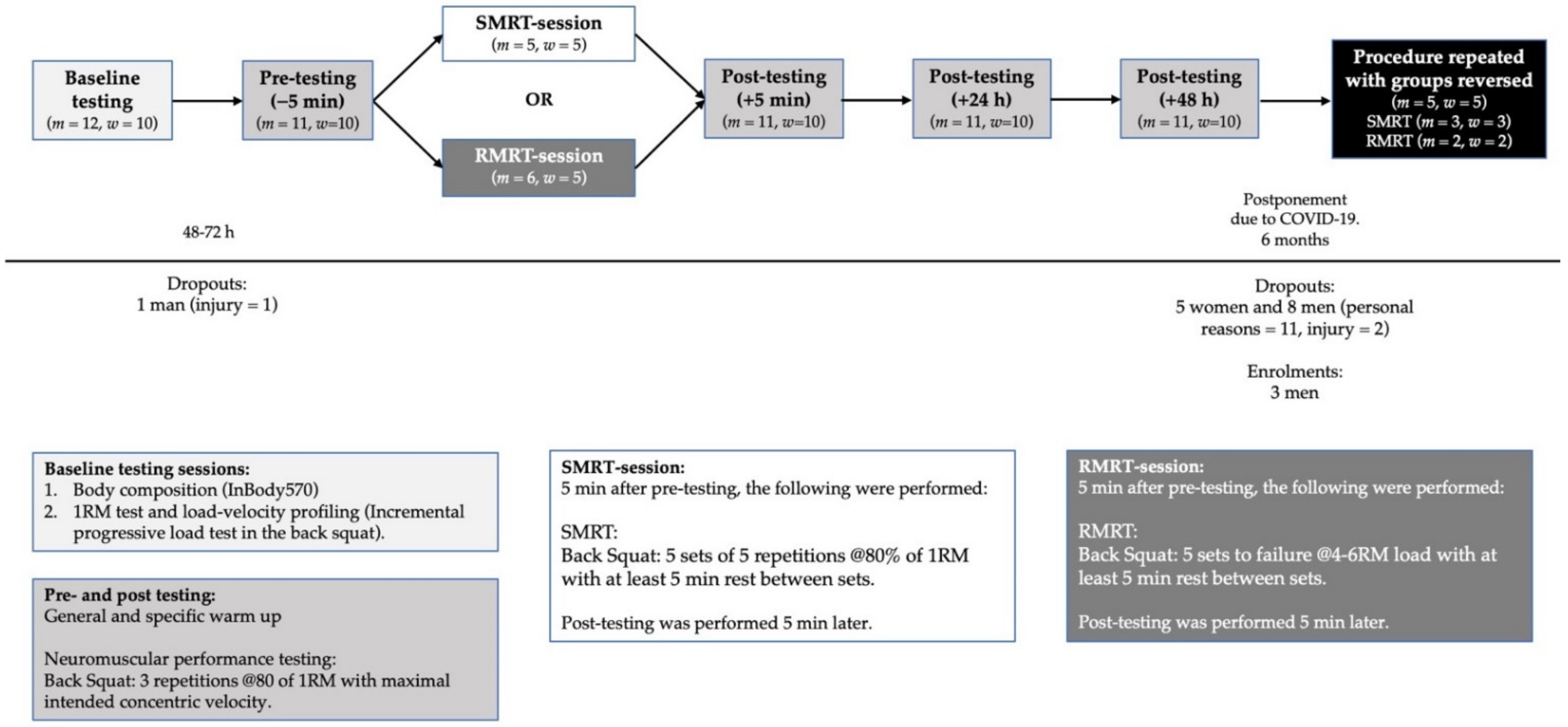
2.2. Experimental Procedures
2.3. Baseline Testing
2.3.1. Body Composition
2.3.2. Load-Velocity Profiling and 1RM Strength Assessment
2.4. Performance Assessment and RT Protocols
2.4.1. SMRT
2.4.2. RMRT
2.5. Instrumentation
2.6. Statistical Analysis
3. Results
3.1. Training Variables
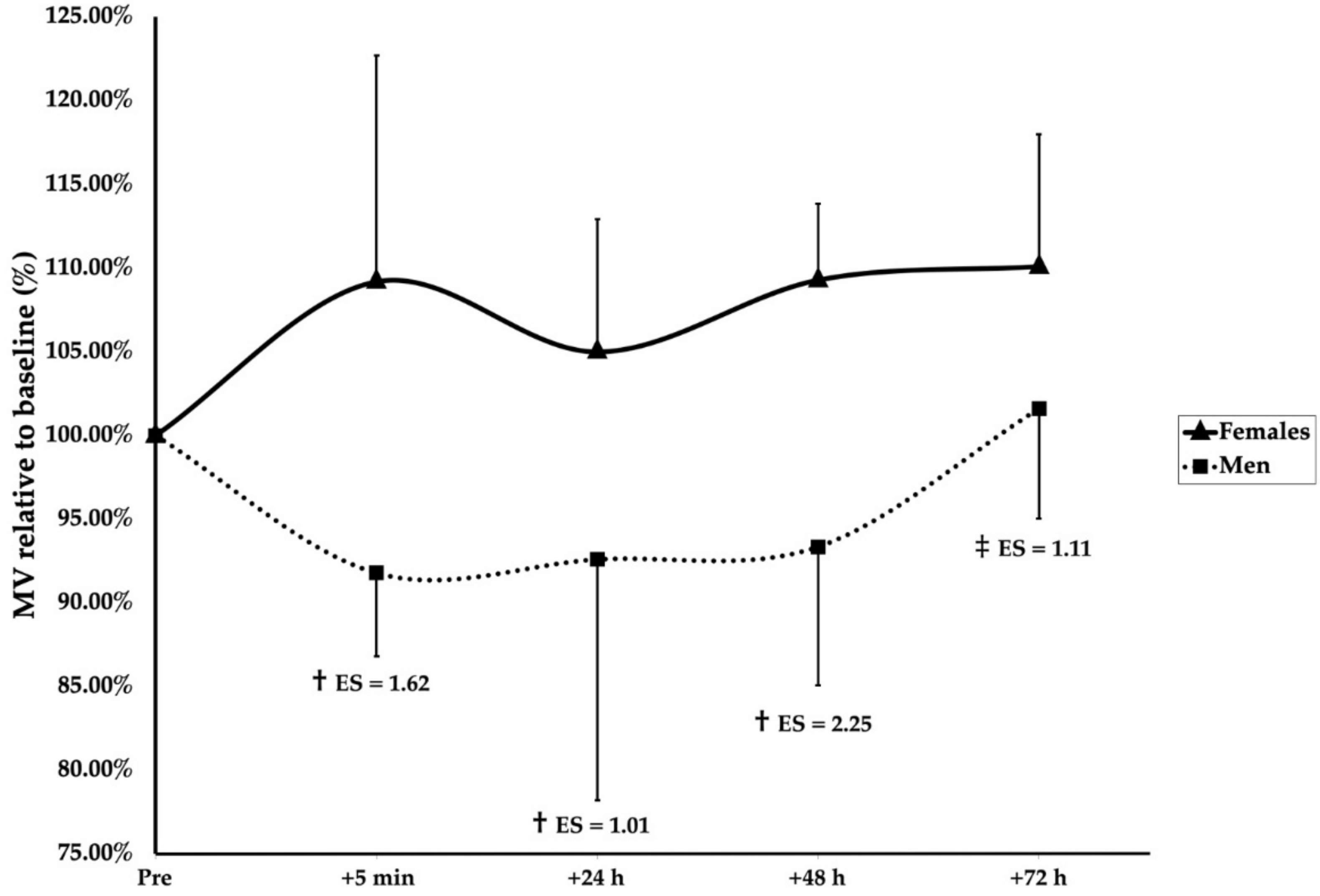
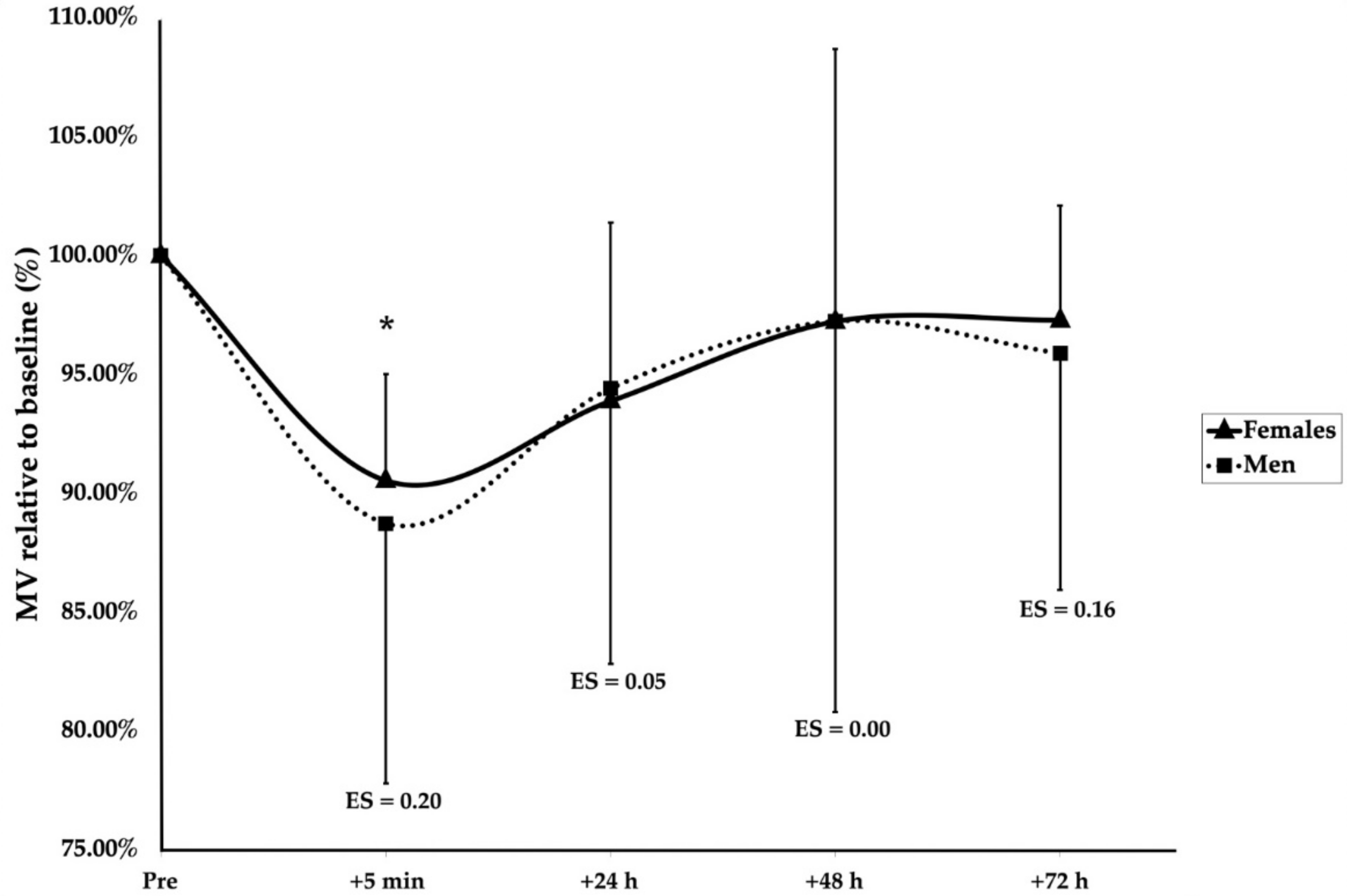
3.2. Recovery Kinetics
4. Discussion
5. Practical Applications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RT | Resistance training |
| FFM | Fat-free mass |
| BM | Body mass |
| BSq | Back squat |
| RM | Repetition maximum |
| MF | Muscular failure |
| MV | Mean concentric velocity |
| Peak MV | Fastest MV of the set |
| Last MV | Last MV of the set |
| Last MVmean | Average of last MVs across all sets of RT |
| MEV1RM | Maximal effort velocity–MV of their 1RM |
| SMRT | Submaximal resistance training protocol |
| RMRT | Repetition maximum resistance training protocol |
| FM | Fat mass |
| ICC | Intra class correlation |
| Reps | Repetitions |
| MLM | Mixed linear modeling |
| MVC | Maximal voluntary contraction |
References
- Brentano, M.A.; Martins Kruel, L.F. A review on strength exercise-induced muscle damage: Applications, adaptation mechanisms and limitations. J. Sports Med. Phys. Fit. 2011, 51, 1–10. [Google Scholar]
- Zając, A.; Chalimoniuk, M.; Maszczyk, A.; Gołaś, A.; Lngfort, J. Central and peripheral fatigue during resistance exercise—A critical review. J. Hum. Kinet. 2015, 49, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.W.; Carson, B.P.; Jakeman, P.M. Sex differences in the temporal recovery of neuromuscular function following resistance training in resistance trained men and women 18 to 35 years. Front. Physiol. 2018, 9, 1480. [Google Scholar] [CrossRef] [PubMed]
- Amorim, M.Z.; Machado, M.; Hackney, A.C.; de Oliveira, W.; Luz, C.P.N.; Pereira, R. Sex differences in serum CK activity but not in glomerular filtration rate after resistance exercise: Is there a sex dependent renal adaptative response? J. Physiol. Sci. 2014, 64, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Baranauskienė, N.; Kilikevičienė, S.; Stasiulė, L.; Civinskienė, G.; Stasiulis, A. Gender differences in residual effect of prior drop jumps on oxygen uptake during heavy cycling exercise. Medicina 2017, 53, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.R.; Fragala, M.S.; Volek, J.S.; Denegar, C.R.; Anderson, J.M.; Comstock, B.A.; Dunn-Lewis, C.; Hooper, D.R.; Szivak, T.K.; Luk, H.-Y.; et al. Sex differences in creatine kinase after acute heavy resistance exercise on circulating granulocyte estradiol receptors. Eur. J. Appl. Physiol. 2012, 112, 3335–3340. [Google Scholar] [CrossRef] [PubMed]
- Benini, R.; Nunes, P.R.P.; Orsatti, C.L.; Portari, G.V.; Orsatti, F.L. Influence of sex on cytokines, heat shock protein and oxidative stress markers in response to an acute total body resistance exercise protocol. J. Exerc. Sci. Fit. 2015, 13, 1–7. [Google Scholar] [CrossRef]
- Clark, B.C.; Manini, T.M.; Thé, D.J.; Doldo, N.A.; Ploutz-Snyder, L.L. Gender differences in skeletal muscle fatigability are related to contraction type and EMG spectral compression. J. Appl. Physiol. 2003, 94, 2263–2272. [Google Scholar] [CrossRef]
- Hunter, S.K. The relevance of sex differences in performance fatigability. Med. Sci. Sports Exerc. 2016, 48, 2247–2256. [Google Scholar] [CrossRef]
- Maughan, R.J.; Harmon, M.; Leiper, J.B.; Sale, D.; Delman, A. Endurance capacity of untrained males and females in isometric and dynamic muscular contractions. Eur. J. Appl. Physiol. 1986, 55, 395–400. [Google Scholar] [CrossRef]
- Ansdell, P.; Thomas, K.; Hicks, K.M.; Hunter, S.K.; Howatson, G.; Goodall, S. Physiological sex differences affect the integrative response to exercise: Acute and chronic implications. Exp. Physiol. 2020, 105, 2007–2021. [Google Scholar] [CrossRef] [PubMed]
- Lundsgaard, A.-M.; Kiens, B. Gender differences in skeletal muscle substrate metabolism—Molecular mechanisms and insulin sensitivity. Front. Endocrinol. 2014, 5, 195. [Google Scholar] [CrossRef] [PubMed]
- Häkkinen, K. Neuromuscular fatigue in males and females during strenuous heavy resistance loading. Electromyogr. Clin. Neurophysiol. 1994, 34, 205–214. [Google Scholar] [PubMed]
- Häkkinen, K. Neuromuscular fatigue and recovery in male and female athletes during heavy resistance exercise. Int. J. Sports Med. 1993, 14, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Judge, L.W.; Burke, J.R. The effect of recovery time on strength performance following a high-intensity Bbnch press workout in males and females. Int. J. Sports Physiol. Perform. 2010, 5, 184–196. [Google Scholar] [CrossRef]
- Marshall, P.W.; Metcalf, E.; Hagstrom, A.D.; Cross, R.; Siegler, J.C.; Enoka, R.M. Changes in fatigue are the same for trained men and women after resistance exercise. Med. Sci. Sports Exerc. 2020, 52, 196–204. [Google Scholar] [CrossRef]
- Pareja-Blanco, F.; Villalba-Fernández, A.; Cornejo-Daza, P.J.; Sánchez-Valdepeñas, J.; González-Badillo, J.J. Time course of recovery following resistance exercise with different loading magnitudes and velocity loss in the set. Sports 2019, 7, 59. [Google Scholar] [CrossRef]
- Conceição, F.; Fernandes, J.; Lewis, M.; Gonzaléz-Badillo, J.J.; Jimenéz-Reyes, P. Movement velocity as a measure of exercise intensity in three lower limb exercises. J. Sports Sci. 2016, 34, 1099–1106. [Google Scholar] [CrossRef]
- Vernon, A.; Joyce, C.; Banyard, H.G. Readiness to train: Return to baseline strength and velocity following strength or power training. Int. J. Sports Sci. Coach. 2020, 15, 204–211. [Google Scholar] [CrossRef]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and agreement of various InBody body composition analyzers as compared to dual-energy x-ray absorptiometry in healthy men and women. J. Clin. Densitom. 2018, 23, 443–450. [Google Scholar] [CrossRef]
- Sánchez-Medina, L.; Pallarés, J.G.; Pérez, C.E.; Morán-Navarro, R.; González-Badillo, J.J. Estimation of relative load from bar velocity in the full back squat exercise. Sports Med. Int. Open 2017, 1, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.M.; Akyildiz, Z.; Pino-Ortega, J.; Rico-González, M. Validity and reliability of the inertial measurement unit for barbell velocity assessments: A systematic review. Sensors 2021, 21, 2511. [Google Scholar] [CrossRef]
- Lake, J.; Augustus, S.; Austin, K.; Comfort, P.; McMahon, J.; Mundy, P.; Haff, G.G. The reliability and validity of the bar-mounted PUSH BandTM 2.0 during bench press with moderate and heavy loads. J. Sports Sci. 2019, 37, 2685–2690. [Google Scholar] [CrossRef]
- Rhea, M.R. Determining the magnitude of treatment effects in strength training research through the use of the effect size. J. Strength Cond. Res. 2004, 18, 918–920. [Google Scholar] [PubMed]
- Ialongo, C. Understanding the effect size and its measures. Biochem. Med. 2016, 26, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuis, S.; Forstmann, B.U.; Wagenmakers, E.-J. Erroneous analyses of interactions in neuroscience: A problem of significance. Nat. Neurosci. 2011, 14, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.C.R.; Lysenko, E.A.; Semenova, E.A.; Borisov, O.V.; Andryushchenko, O.N.; Andryushchenko, L.B.; Vepkhvadze, T.F.; Lednev, E.M.; Zmijewski, P.; Popov, D.V.; et al. Prediction of muscle fiber composition using multiple repetition testing. Biol. Sport 2020, 38, 277–283. [Google Scholar] [CrossRef]
- Terzis, G.; Spengos, K.; Manta, P.; Sarris, N.; Georgiadis, G. Fiber type composition and capillary density in relation to submaximal number of repetitions in resistance exercise. J. Strength Cond. Res. 2008, 22, 845–850. [Google Scholar] [CrossRef]
- Hickson, R.C.; Dvorak, B.A.; Gorostiaga, E.M.; Kurowski, T.T.; Foster, C. Potential for strength and endurance training to amplify endurance performance. J. Appl. Physiol. 1988, 65, 2285–2290. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Brightwell, C.R.; Phalen, D.E.; McKenna, C.F.; Lane, S.J.; Porter, C.; Volpi, E.; Rasmussen, B.B.; Fry, C.S. Low skeletal muscle capillarization limits muscle adaptation to resistance exercise training in older adults. Exp. Gerontol. 2019, 127, 110723. [Google Scholar] [CrossRef] [PubMed]
- Tesch, P.A.; Lindeberg, S. Blood lactate accumulation during arm exercise in world class kayak paddlers and strength trained athletes. Eur. J. Appl. Physiol. 1984, 52, 441–445. [Google Scholar] [CrossRef]
- Dos Santos, W.M.; Junior, A.C.T.; Braz, T.V.; Lopes, C.R.; Brigatto, F.A.; Dos Santos, J.W. Resistance-trained individuals can underestimate the intensity of the resistance training session: An analysis among genders, training experience, and exercises. J. Strength Cond. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Emmonds, S.; Heyward, O.; Jones, B. The challenge of applying and undertaking research in female sport. Sports Med.-Open 2019, 5, 51. [Google Scholar] [CrossRef] [PubMed]
- Nimphius, S. Exercise and sport science failing by design in understanding female athletes. Int. J. Sports Physiol. Perform. 2019, 14, 1157–1158. [Google Scholar] [CrossRef]
- Zourdos, M.C.; Klemp, A.; Dolan, C.; Quiles, J.M.; Schau, K.A.; Jo, E.; Helms, E.; Esgro, B.; Duncan, S.; Garcia Merino, S.; et al. Novel resistance training-specific rating of perceived exertion scale measuring repetitions in reserve. J. Strength Cond. Res. 2016, 30, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Elliott-Sale, K.J.; Minahan, C.L.; de Jonge, X.A.K.J.; Ackerman, K.E.; Sipilä, S.; Constantini, N.W.; Lebrun, C.M.; Hackney, A.C. Methodological considerations for studies in sport and exercise science with women as participants: A working guide for standards of practice for research on women. Sports Med. 2021, 51, 843–861. [Google Scholar] [CrossRef] [PubMed]
- Janse de Jonge, X.; Thompson, B.; Han, A. Methodological recommendations for menstrual cycle research in sports and exercise. Med. Sci. Sports Exerc. 2019, 51, 2610–2617. [Google Scholar] [CrossRef] [PubMed]
- Blagrove, R.C.; Bruinvels, G.; Pedlar, C.R. Variations in strength-related measures during the menstrual cycle in eumenorrheic women: A systematic review and meta-analysis. J. Sci. Med. Sport 2020, 23, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Pereira, H.M.; Larson, R.D.; Bemben, D.A. Menstrual cycle effects on exercise-induced fatigability. Front. Physiol. 2020, 11, 517. [Google Scholar] [CrossRef] [PubMed]
- McNulty, K.L.; Elliott-Sale, K.J.; Dolan, E.; Swinton, P.A.; Ansdell, P.; Goodall, S.; Thomas, K.; Hicks, K.M. The effects of menstrual cycle phase on exercise performance in eumenorrheic women: A systematic review and meta-analysis. Sports Med. 2020, 50, 1813–1827. [Google Scholar] [CrossRef]
- Elliott-Sale, K.J.; McNulty, K.L.; Ansdell, P.; Goodall, S.; Hicks, K.M.; Thomas, K.; Swinton, P.A.; Dolan, E. The effects of oral contraceptives on exercise performance in women: A systematic review and meta-analysis. Sports Med. 2020, 50, 1785–1812. [Google Scholar] [CrossRef] [PubMed]
- Sipavičienė, S.; Daniusevičiutė, L.; Klizienė, I.; Kamandulis, S.; Skurvydas, A. Effects of estrogen fluctuation during the menstrual cycle on the response to stretch-shortening exercise in females. BioMed Res. Int. 2013, 2013, 243572. [Google Scholar] [CrossRef]
- Anderson, L.J.; Baker, L.L.; Schroeder, E.T. Blunted myoglobin and quadriceps soreness after electrical stimulation during the luteal phase or oral contraception. Res. Q. Exerc. Sport 2017, 88, 193–202. [Google Scholar] [CrossRef]
- Mackay, K.; González, C.; Zbinden-Foncea, H.; Peñailillo, L. Effects of oral contraceptive use on female sexual salivary hormones and indirect markers of muscle damage following eccentric cycling in women. Eur. J. Appl. Physiol. 2019, 119, 2733–2744. [Google Scholar] [CrossRef] [PubMed]
- Romero-Parra, N.; Rael, B.; Alfaro-Magallanes, V.M.; Janse de Jonge, X.; Cupeiro, R.; Peinado, A.B. The effect of the oral contraceptive cycle phase on exercise-induced muscle damage after eccentric exercise in resistance-trained women. J. Strength Cond. Res. 2020, 35, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Oosthuyse, T.; Bosch, A.N. The effect of gender and menstrual phase on serum creatine kinase activity and muscle soreness following downhill running. Antioxidants 2017, 6, 16. [Google Scholar] [CrossRef]
- Romero-Parra, N.; Barba-Moreno, L.; Rael, B.; Alfaro-Magallanes, V.M.; Cupeiro, R.; Díaz, Á.E.; Calderón, F.J.; Peinado, A.B. Influence of the menstrual cycle on blood markers of muscle damage and inflammation following eccentric exercise. Int. J. Environ. Res. Public Health 2020, 17, 1618. [Google Scholar] [CrossRef]
- Timon, R.; Corvillo, M.; Brazo, J.; Robles, M.C.; Maynar, M. Strength training effects on urinary steroid profile across the menstrual cycle in healthy women. Eur. J. Appl. Physiol. 2013, 113, 1469–1475. [Google Scholar] [CrossRef]
- Hyldahl, R.D.; Chen, T.C.; Nosaka, K. Mechanisms and mediators of the skeletal muscle repeated bout effect. Exerc. Sport Sci. Rev. 2017, 45, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Orkin, A.M.; Gill, P.J.; Ghersi, D.; Campbell, L.; Sugarman, J.; Emsley, R.; Steg, P.G.; Weijer, C.; Simes, J.; Rombey, T.; et al. Guidelines for reporting trial protocols and completed trials modified due to the COVID-19 pandemic and other extenuating circumstances: The CONSERVE 2021 statement. JAMA 2021, 326, 257–265. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| SMRT Group (n = 16) | RMRT Group (n = 15) | |||
|---|---|---|---|---|
| Men (n = 8) | Women (n = 8) | Men (n = 8) | Women (n = 7) | |
| Age (years) | 29 ± 5 | 26 ± 4 | 28 ± 4 | 25 ± 4 |
| Height (cm) * | 182 ± 9 † | 165 ± 9 † | 182 ± 5 † | 161 ± 8 † |
| Body Mass (kg) * | 86 ± 14.4 † | 70.3 ± 8.8 † | 82.8 ± 6.2 † | 61.8 ± 6 † |
| Fat Mass (kg) | 14.3 ± 3.3 | 18.7 ± 8.2 | 11.2 ± 4.6 | 14.3 ± 5.2 |
| Fat Free Mass (kg) * | 71.7 ± 13 † | 51.6 ± 7.6 † | 71.6 ± 6.1 † | 47.4 ± 5.7 † |
| 1RM Back Squat (kg) * § | 141.6 ± 29.0 † | 85.1 ± 18.8 † | 148.1 ± 26.5 † | 80 ± 8.4 † |
| Relative strength (kg/kg) ^ * | 1.97 ± 0.16 † | 1.67 ± 0.35 † | 2.07 ± 0.32 † | 1.7 ± 0.24 † |
| MEV1RM (m/s) ^^ | 0.33 ± 0.07 | 0.34 ± 0.09 | 0.37 ± 0.08 | 0.41 ± 0.1 |
| Baseline MV80% of 1RM (m/s) * | 0.72 ± 0.09 † | 0.58 ± 0.1 † | 0.71 ± 0.08 | 0.67 ± 0.1 |
| Standardized Warm-Up Routines | |
|---|---|
| General warm-up | 2 rounds of 5 reps of: Cossack Squat (per side), Kang Squat, Inch Worms, World’s Greatest Stretch (per side), and Off-set Squat with a 5 kg plate in front. |
| Specific warm-up | 3 reps in the BSq with maximally intended concentric velocity with: 20 kg bar, 45%, 50%, 60%, and 70% of 1RM |
| SMRT Group (n = 16) | RMRT Group (n = 15) | |||
|---|---|---|---|---|
| Males (n = 8) | Females (n = 8) | Males (n = 8) | Females (n = 7) | |
| Total tonnage performed (kg) * | 2787.5 ± 272 † | 1673.8 ± 371.5 † | 2911.4 ± 389.6 † | 1873 ± 181 † |
| Pre tonnage (kg) § | 0 ± 0 € | 0 ± 0 € | 889.4 ± 462.6 € | 893.4 ± 552.3 € |
| Training load (kg) *§ | 113.3 ± 23.2 † € | 68.1 ± 15 † € | 130.0 ± 23.5 † € | 71.7 ± 7.4 † € |
| Training intensity (% of 1RM) § | 80 ± 0 € | 80 ± 0 € | 87.7 ± 1.5 † € | 89.7 ± 2.6 † € |
| Total reps completed § * | 25 ± 0 € | 24 ± 1.1 € | 17.1 ± 1.6 † € | 15.1 ± 2.3 † € |
| Mean Set Velocity Loss (%) | 19.3 ± 7.2 | 21.0 ± 5.4 | 18.8 ± 6.1 | 15.9 ± 8.3 |
| Mean Velocity Increase Between Sets (%) | 25.6 ± 8.8 | 29.1 ± 11.2 | 23.2 ± 11.2 | 18.2 ± 18.4 |
| Last MVmean (m/s) § * Last MVmean–MEV1RM (m/s) § * | 0.53 ± 0.1 € 0.2 ± 0.08 € | 0.46 ± 0.1 € 0.12 ± 0.09 € | 0.38 ± 0.06 † € 0.02 ± 0.08 † € | 0.32 ± 0.05 † € −0.1 ± 0.12 † € |
| SMRT Group (n = 16) | RMRT Group (n = 15) | |||
|---|---|---|---|---|
| Males (n = 8) | Females (n = 8) | Males (n = 8) | Females (n = 7) | |
| Set 1 | ||||
| Reps performed § | 5 ± 0 | 5 ± 0 € | 4.8 ± 0.7 † | 4.3 ± 0.5 † € |
| Peak MV (m/s) § * | 0.66 ± 0.04 € | 0.60 ± 0.14 € | 0.51 ± 0.09 † € | 0.41 ± 0.06 † € |
| Last MV (m/s) § | 0.52 ± 0.12 € | 0.46 ± 0.13 € | 0.38 ± 0.09 € | 0.32 ± 0.05 € |
| Set 2 | ||||
| Reps performed § * | 5 ± 0 € | 5 ± 0 € | 4.3 ± 0.5 † € | 3.3 ± 0.8 † € |
| Peak MV (m/s) § * | 0.66 ± 0.09 † € | 0.57 ± 0.09 † € | 0.49 ± 0.06 † € | 0.4 ± 0.04 † € |
| Last MV (m/s) § * | 0.53 ± 0.09 † € | 0.44 ± 0.1 † € | 0.40 ± 0.08 € | 0.33 ± 0.06 € |
| Set 3 | ||||
| Reps performed § | 5 ± 0 € | 5 ± 0 € | 3.5 ± 0.8 € | 3 ± 1.2 € |
| Peak MV (m/s) § * | 0.66 ± 0.09 € | 0.59 ± 0.16 € | 0.49 ± 0.1 † € | 0.38 ± 0.09 † € |
| Last MV (m/s) § | 0.52 ± 0.09 € | 0.47 ± 0.11 € | 0.4 ± 0.07 € | 0.33 ± 0.07 € |
| Set 4 | ||||
| Reps performed § | 5 ± 0 € | 4.9 ± 0.4 € | 2.6 ± 0.9 € | 2.6 ± 0.5 € |
| Peak MV (m/s) § * | 0.66 ± 0.09 € | 0.59 ± 0.16 € | 0.46 ± 0.07 € | 0.37 ± 0.08 € |
| Last MV (m/s) § * | 0.55 ± 0.12 € | 0.46 ± 0.11 € | 0.36 ± 0.07 € | 0.3 ± 0.05 € |
| Set 5 | ||||
| Reps performed § | 5 ± 0 € | 4.8 ± 0.7 € | 2 ± 0.9 € | 2 ± 0.8 € |
| Peak MV (m/s) § * | 0.65 ± 0.07 † € | 0.57 ± 0.11 † € | 0.43 ± 0.07 † € | 0.34 ± 0.10 † € |
| Last MV (m/s) § | 0.54 ± 0.12 € | 0.47 ± 0.1 € | 0.36 ± 0.09 € | 0.30 ± 0.06 € |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amdi, C.H.; Cleather, D.J.; Tallent, J. Impact of Training Protocols on Lifting Velocity Recovery in Resistance Trained Males and Females. Sports 2021, 9, 157. https://doi.org/10.3390/sports9110157
Amdi CH, Cleather DJ, Tallent J. Impact of Training Protocols on Lifting Velocity Recovery in Resistance Trained Males and Females. Sports. 2021; 9(11):157. https://doi.org/10.3390/sports9110157
Chicago/Turabian StyleAmdi, Christian Houmann, Daniel John Cleather, and Jamie Tallent. 2021. "Impact of Training Protocols on Lifting Velocity Recovery in Resistance Trained Males and Females" Sports 9, no. 11: 157. https://doi.org/10.3390/sports9110157
APA StyleAmdi, C. H., Cleather, D. J., & Tallent, J. (2021). Impact of Training Protocols on Lifting Velocity Recovery in Resistance Trained Males and Females. Sports, 9(11), 157. https://doi.org/10.3390/sports9110157