
Differences in the Dominant and Non-Dominant Knee Valgus Angle in Junior Elite and Amateur Soccer Players after Unilateral Landing




Abstract
:1. Introduction
- (1)
- Are there any statistically significant differences between the frontal knee angles of the dominant leg (DOM) and the non-dominant leg (NON) in junior soccer players when they land on one leg?
- (2)
- Are there any differences between the knee angles of the dominant and non-dominant leg in professional and amateur junior soccer players?
2. Materials and Methods
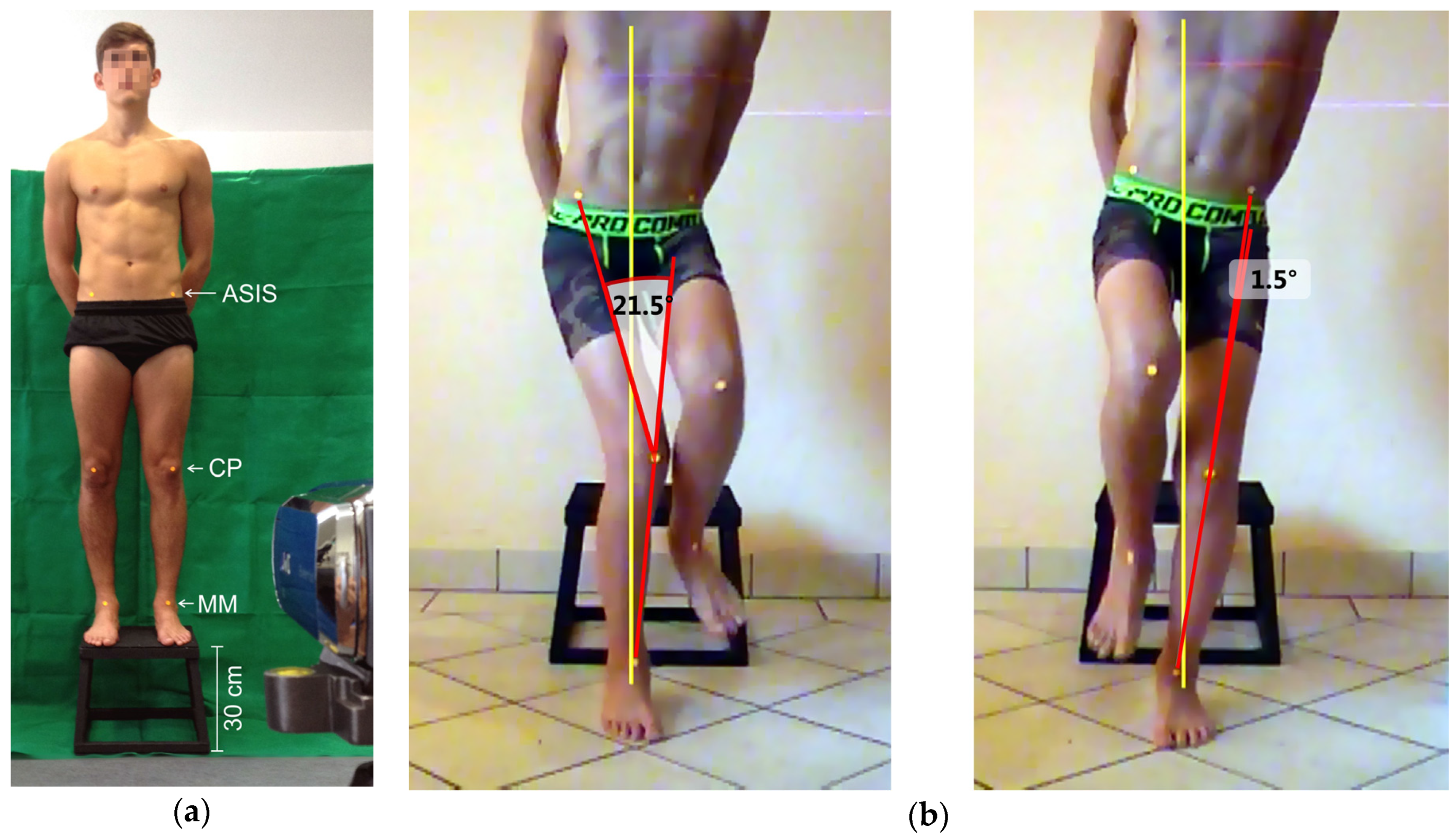
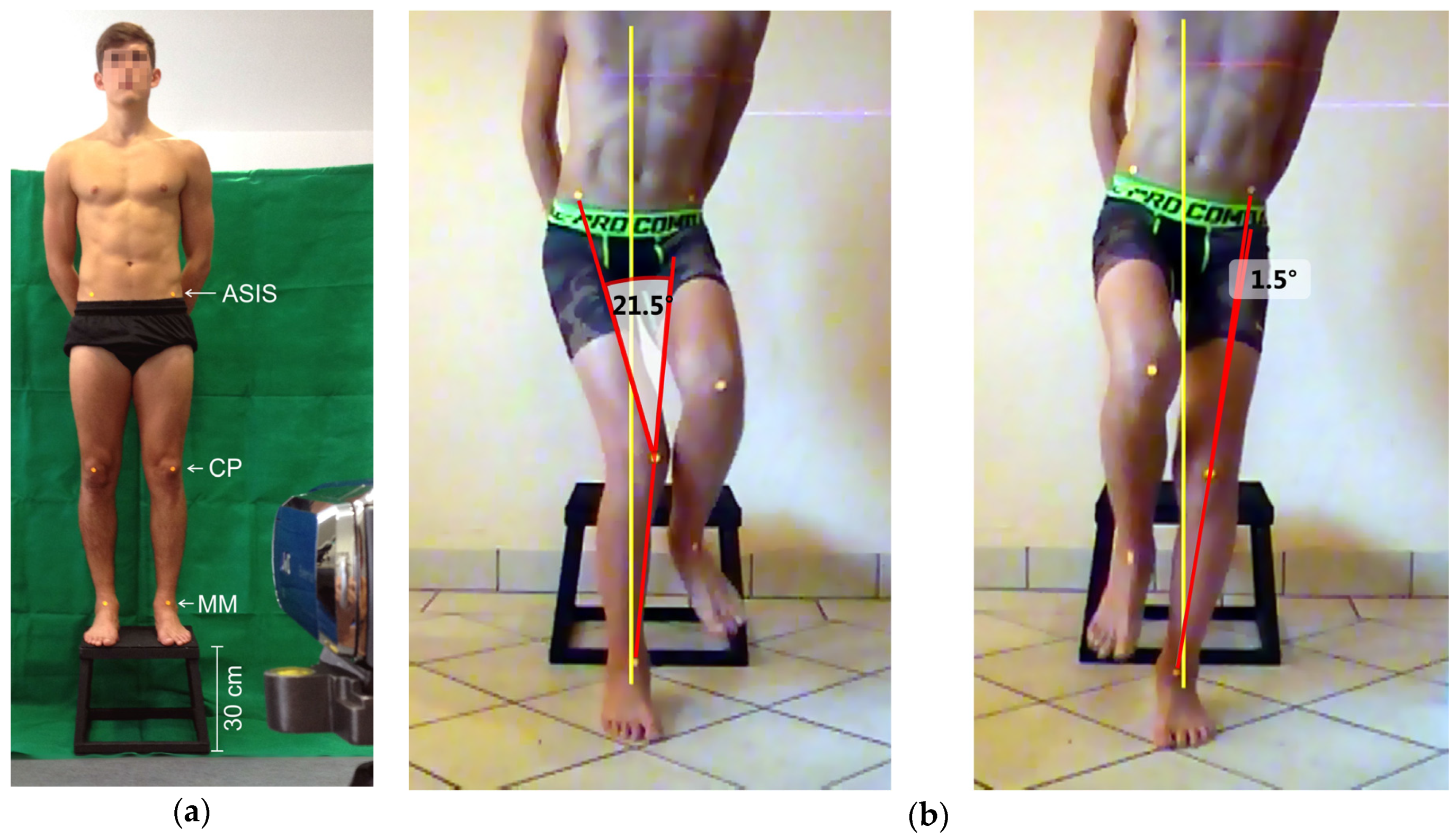
2.1. Test Procedure
2.2. Data Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S., Jr.; Colosimo, A.J.; McLean, S.G.; van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Powers, C.M. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: A theoretical perspective. J. Orthop. Sports Phys. Ther. 2003, 33, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Aerts, I.; Cumps, E.; Verhagen, E.; Verschueren, J.; Meeusen, R. A systematic review of different jump-landing variables in relation to injuries. J. Sports Med. Phys. Fit. 2013, 53, 509–519. [Google Scholar]
- Dai, B.; Mao, D.; Garrett, W.E.; Yu, B. Anterior cruciate ligament injuries in soccer: Loading mechanisms, risk factors, and prevention programs. J. Sport Health Sci. 2014, 3, 299–306. [Google Scholar] [CrossRef]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of injury incidences in male professional adult and elite youth soccer players: A systematic review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, T.; Ostenberg, A.H.; Alricsson, M. Injury profile among elite male youth soccer players in a Swedish first league. J. Exerc. Rehabil. 2016, 12, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Brito, J.; Malina, R.M.; Seabra, A.; Massada, J.L.; Soares, J.M.; Krustrup, P.; Rebelo, A. Injuries in portuguese youth soccer players during training and match play. J. Athl. Train. 2012, 47, 191–197. [Google Scholar] [PubMed]
- Rossler, R.; Junge, A.; Chomiak, J.; Dvorak, J.; Faude, O. Soccer injuries in players aged 7 to 12 years: A descriptive epidemiological study over 2 seasons. Am. J. Sports Med. 2016, 44, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Junge, A.; Cheung, K.; Edwards, T.; Dvorak, J. Injuries in youth amateur soccer and rugby players—Comparison of incidence and characteristics. Br. J. Sports Med. 2004, 38, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Junge, A.; Dvorak, J. Soccer injuries: A review on incidence and prevention. Sports Med. 2004, 34, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Alentorn-Geli, E.; Myer, G.D.; Silvers, H.J.; Samitier, G.; Romero, D.; Lazaro-Haro, C.; Cugat, R. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 705–729. [Google Scholar] [CrossRef] [PubMed]
- Fauno, P.; Wulff Jakobsen, B. Mechanism of anterior cruciate ligament injuries in soccer. Int. J. Sports Med. 2006, 27, 75–79. [Google Scholar] [CrossRef]
- Shimokochi, Y.; Shultz, S.J. Mechanisms of noncontact anterior cruciate ligament injury. J. Athl. Train. 2008, 43, 396–408. [Google Scholar] [CrossRef] [PubMed]
- Kagaya, Y.; Fujii, Y.; Nishizono, H. Association between hip abductor function, rear-foot dynamic alignment, and dynamic knee valgus during single-leg squats and drop landings. J. Sport Health Sci. 2015, 4, 182–187. [Google Scholar] [CrossRef]
- Barber-Westin, S.D.; Noyes, F.R.; Smith, S.T.; Campbell, T.M. Reducing the risk of noncontact anterior cruciate ligament injuries in the female athlete. Phys. Sportsmed. 2009, 37, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Claiborne, T.L.; Armstrong, C.W.; Gandhi, V.; Pincivero, D.M. Relationship between hip and knee strength and knee valgus during a single leg squat. J. Appl. Biomech. 2006, 22, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Santamaria, L.J.; Webster, K.E. The effect of fatigue on lower-limb biomechanics during single-limb landings: A systematic review. J. Orthop. Sports Phys. Ther. 2010, 40, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Kearns, C.F.; Isokawa, M.; Abe, T. Architectural characteristics of dominant leg muscles in junior soccer players. Eur. J. Appl. Physiol. 2001, 85, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Kellis, E.; Katis, A.; Gissis, I. Knee biomechanics of the support leg in soccer kicks from three angles of approach. Med. Sci. Sports Exerc. 2004, 36, 1017–1028. [Google Scholar] [CrossRef] [PubMed]
- Knight, A.C.; Weimar, W.H. Difference in response latency of the peroneus longus between the dominant and nondominant legs. J. Sport Rehab. 2011, 20, 321–332. [Google Scholar] [CrossRef]
- Brophy, R.; Silvers, H.J.; Gonzales, T.; Mandelbaum, B.R. Gender influences: The role of leg dominance in acl injury among soccer players. Br. J. Sports Med. 2010, 44, 694–697. [Google Scholar] [CrossRef] [PubMed]
- Brophy, R.H.; Schmitz, L.; Wright, R.W.; Dunn, W.R.; Parker, R.D.; Andrish, J.T.; McCarty, E.C.; Spindler, K.P. Return to play and future ACL injury risk after ACL reconstruction in soccer athletes from the Multicenter Orthopaedic Outcomes Network (MOON) group. Am. J. Sports Med. 2012, 40, 2517–2522. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.; Herrington, L.; Comfort, P. Comparison of landing knee valgus angle between female basketball and football athletes: Possible implications for anterior cruciate ligament and patellofemoral joint injury rates. Phys. Ther. Sport 2012, 13, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Śliwowski, R.; Jadczak, Ł.; Hejna, R.; Wieczorek, A. The effects of individualized resistance strength programs on knee muscular imbalances in junior elite soccer players. PLoS ONE 2015, 10, e0144021. [Google Scholar]
- Herrington, L.; Munro, A. Drop jump landing knee valgus angle; normative data in a physically active population. Phys. Ther. Sport 2010, 11, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.; Herrington, L.; Carolan, M. Reliability of 2-dimensional video assessment of frontal-plane dynamic knee valgus during common athletic screening tasks. J. Sport Rehab. 2012, 21, 7–11. [Google Scholar] [CrossRef]
- Vieira, O., Jr.; Coelho, D.B.; Teixeira, L.A. Asymmetric balance control between legs for quiet but not for perturbed stance. Exp. Brain Res. 2014, 232, 3269–3276. [Google Scholar] [CrossRef] [PubMed]
- Thorborg, K.; Couppé, C.; Petersen, J.; Magnusson, P.; Holmich, P. Eccentric hip adduction and abduction strength in elite soccer players and matched controls a cross-sectional study. Br. J. Sports Med. 2011, 45, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Ergün, M.; İşlegen, Ç.; Taşkıran, E. A cross-sectional analysis of sagittal knee laxity and isokinetic muscle strength in soccer players. Int. J. Sports Med. 2004, 25, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Gstöttner, M.; Neher, A.; Scholtz, A.; Millonig, M.; Lembert, S.; Raschner, C. Balance ability and muscle response of the preferred and nonpreferred leg in soccer players. Motor Control 2009, 13, 218–231. [Google Scholar] [CrossRef] [PubMed]
- Rahnama, N.; Lees, A.; Bambaecichi, E. A comparison of muscle strength and flexibility between the preferred and non-preferred leg in English soccer players. Ergonomics 2005, 48, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Paillard, T.; Noé, F.; Rivière, T.; Marion, V.; Montoya, R.; Dupui, P. Postural performance and strategy in the unipedal stance of soccer players at different levels of competition. J. Athl. Train. 2006, 41, 172–176. [Google Scholar] [PubMed]
- Sorenson, B.; Kernozek, T.W.; Willson, J.D.; Ragan, R.; Hove, J. Two- and three-dimensional relationships between knee and hip kinematic motion analysis: Single-leg drop-jump landings. J. Sport Rehab. 2015, 24, 363–372. [Google Scholar] [CrossRef] [PubMed]
- McLean, S.G.; Walker, K.; Ford, K.R.; Myer, G.D.; Hewett, T.E.; van den Bogert, A.J. Evaluation of a two dimensional analysis method as a screening and evaluation tool for anterior cruciate ligament injury. Br. J. Sports Med. 2005, 39, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Willson, J.D.; Davis, I.S. Utility of the frontal plane projection angle in females with patellofemoral pain. J. Orthop. Sports Phys. Ther. 2008, 38, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, N.F.N.; Ocarino, J.M.; Mendonça, L.D.; Hewett, T.E.; Fonseca, S.T. Foot and hip contributions to high frontal plane knee projection angle in athletes: A classification and regression tree approach. J. Orthop. Sports Phys. Ther. 2012, 42, 996–1004. [Google Scholar] [CrossRef]
- Donohue, M.R.; Ellis, S.M.; Heinbaugh, E.M.; Stephenson, M.L.; Zhu, Q.; Dai, B. Differences and correlations in knee and hip mechanics during single-leg landing, single-leg squat, double-leg landing, and double-leg squat tasks. Res. Sport Med. 2015, 23, 394–411. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.; Steele, J.R.; Cook, J.L.; Purdam, C.R.; McGhee, D.E. Lower limb movement symmetry cannot be assumed when investigating the stop-jump landing. Med. Sci. Sports Exerc. 2012, 44, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Kameda, M.; Kageyama, M.; Kiba, K.; Kanehisa, H.; Maeda, A. Asymmetry between the dominant and non-dominant legs in the kinematics of the lower extremities during a running single leg jump in collegiate basketball players. J. Sports Sci. Med. 2014, 13, 951–957. [Google Scholar] [PubMed]
- Faude, O.; Rossler, R.; Junge, A. Football injuries in children and adolescent players: Are there clues for prevention? Sports Med. 2013, 43, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Van Beijsterveldt, A.M.; van der Horst, N.; van de Port, I.G.; Backx, F.J. How effective are exercise-based injury prevention programmes for soccer players? A systematic review. Sports Med. 2013, 43, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Cashman, G.E. The effect of weak hip abductors or external rotators on knee valgus kinematics in healthy subjects: A systematic review. J. Sport Rehab. 2012, 21, 273–284. [Google Scholar] [CrossRef]
- Greska, E.K.; Cortes, N.; Van Lunen, B.L.; Oñate, J.A. A feedback inclusive neuromuscular training program alters frontal plane kinematics. J. Strength Cond Res. 2012, 26, 1609–1619. [Google Scholar] [CrossRef] [PubMed]
- Grimm, N.L.; Jacobs, J.C., Jr.; Kim, J.; Denney, B.S.; Shea, K.G. Anterior cruciate ligament and knee injury prevention programs for soccer players: A systematic review and meta-analysis. Am. J. Sports Med. 2015, 43, 2049–2056. [Google Scholar] [CrossRef] [PubMed]
- Herrington, L.; Munro, A.; Comfort, P. A preliminary study into the effect of jumping-landing training and strength training on frontal plane projection angle. Man Ther. 2015, 20, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.; Herrington, L. The effect of videotape augmented feedback on drop jump landing strategy: Implications for anterior cruciate ligament and patellofemoral joint injury prevention. Knee 2014, 21, 891–895. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Level | N | Age (years) | Height (cm) | Weight (kg) |
|---|---|---|---|---|
| Amateur | 48 | 15.4 ± 1.4 | 174.1 ± 6.8 | 64.1 ± 10.9 |
| Elite | 66 | 14.0 ± 0.2 | 169.3 ± 8.6 | 55.3 ± 8.8 |
| Level | Leg | df | M | SD | CV | p | d |
|---|---|---|---|---|---|---|---|
| Amateur | DOM | 47 | 1.419 | 13.597 | 9.58 | 0.046 | 0.28 |
| NON | 47 | −1.856 | 9.729 | −5.24 | |||
| Elite | DOM | 65 | 3.758 | 10.036 | 2.67 | 0.000 | 0.64 |
| NON | 65 | −2.715 | 10.281 | 3.79 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ludwig, O.; Simon, S.; Piret, J.; Becker, S.; Marschall, F. Differences in the Dominant and Non-Dominant Knee Valgus Angle in Junior Elite and Amateur Soccer Players after Unilateral Landing. Sports 2017, 5, 14. https://doi.org/10.3390/sports5010014
Ludwig O, Simon S, Piret J, Becker S, Marschall F. Differences in the Dominant and Non-Dominant Knee Valgus Angle in Junior Elite and Amateur Soccer Players after Unilateral Landing. Sports. 2017; 5(1):14. https://doi.org/10.3390/sports5010014
Chicago/Turabian StyleLudwig, Oliver, Steven Simon, Joe Piret, Stephan Becker, and Franz Marschall. 2017. "Differences in the Dominant and Non-Dominant Knee Valgus Angle in Junior Elite and Amateur Soccer Players after Unilateral Landing" Sports 5, no. 1: 14. https://doi.org/10.3390/sports5010014
APA StyleLudwig, O., Simon, S., Piret, J., Becker, S., & Marschall, F. (2017). Differences in the Dominant and Non-Dominant Knee Valgus Angle in Junior Elite and Amateur Soccer Players after Unilateral Landing. Sports, 5(1), 14. https://doi.org/10.3390/sports5010014