
Type of Ground Surface during Plyometric Training Affects the Severity of Exercise-Induced Muscle Damage



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Plyometric Exercise Protocol
2.4. Dependent Variables
2.5. Plasma Creatine Kinase Activity (CK)
2.6. Delayed Onset Muscle Soreness (DOMS)
2.7. Knee Flexion Range of Motion (KROM)
2.8. Maximal Isometric Voluntary Contraction (MIVC)
2.9. Vertical Jump (VJ)
2.10. The 10-m Sprint
2.11. Rating of Perceived Exertion (RPE)
2.12. Statistical Analysis
3. Results
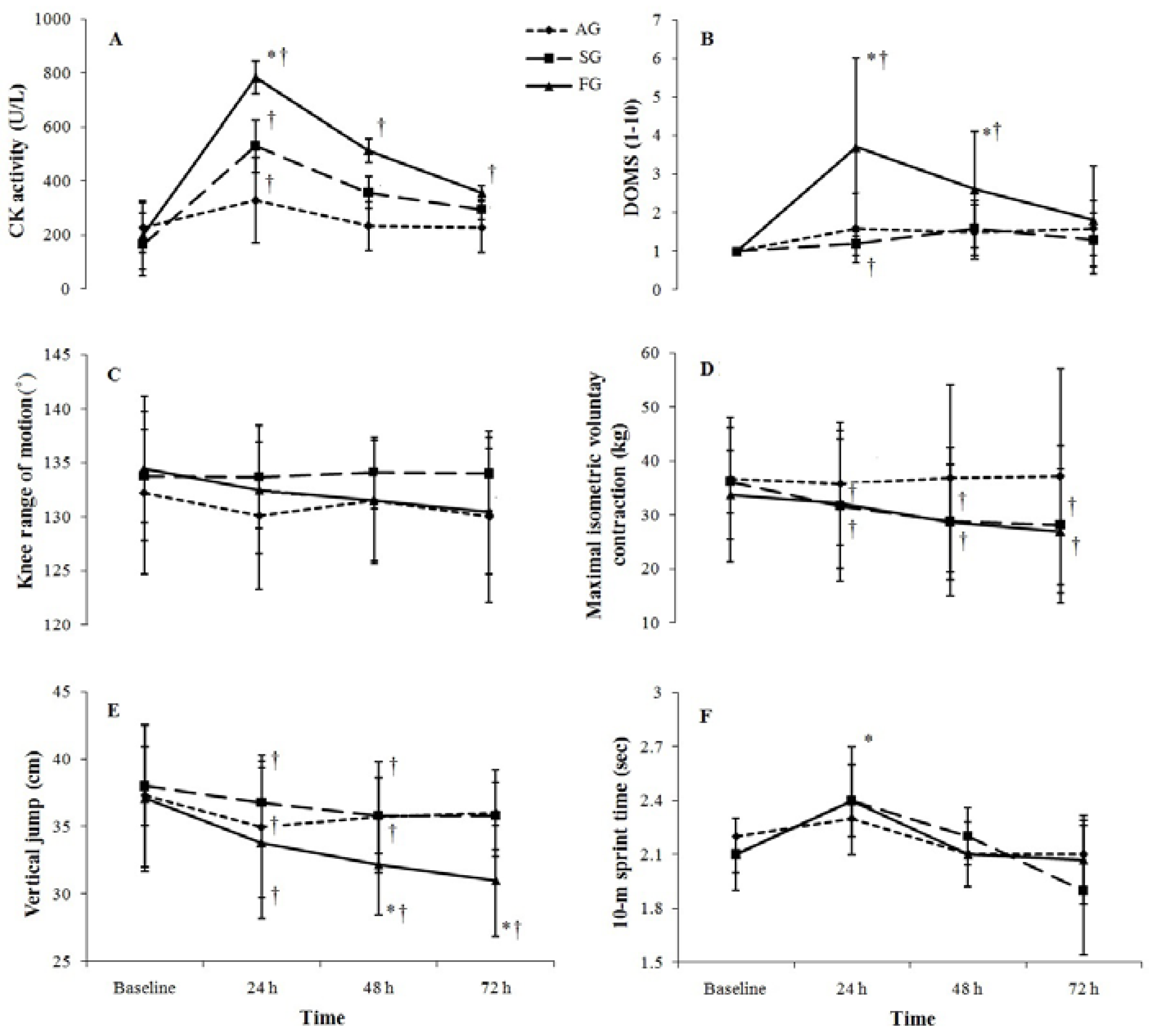
3.1. CK Activity
3.2. Muscle Soreness
3.3. Knee Range of Motion (KROM)
3.4. Maximal Isometric Voluntary Contraction (MIVC)
3.5. Vertical Jump
3.6. 10-m Sprint Times
4. Rating of Perceived Exertion (RPE)
5. Discussion
6. Evidence of Muscle Damage
7. Muscle Function during Recovery from Plyometric Exercise
8. Perceived Exertion
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Potach, D.; Chu, D.A. Plyometric training. In Essential of Strength and Conditioning; Bachle, T., Erale, R., Eds.; Human Kinetic: Champaign, IL, USA, 2000; pp. 135–141. [Google Scholar]
- Arazi, H.; Asadi, A. The effect of aquatic and land plyometric training on strength, sprint, and balance in young basketball players. J. Hum. Sport Exerc. 2011, 6, 101–111. [Google Scholar] [CrossRef]
- Asadi, A.; Arazi, H. Effects of high-intensity plyometric training on dynamic balance, agility, vertical jump and sprint performance in young male basketball players. J. Sport Health Res. 2012, 4, 34–44. [Google Scholar]
- Robinson, L.E.; Décor, S.T.; Merrick, M.A.; Buckworth, J. The effects of land vs. aquatic plyometrics on power, torque, velocity, and muscle soreness in women. J. Strength Cond. Res. 2004, 18, 84–91. [Google Scholar] [PubMed]
- Asadi, A.; Saez de Villarreal, E.; Arazi, H. The effects of plyometric type neuromuscular training on postural control performance of male team basketball players. J. Strength Cond. Res. 2015, 29, 1870–1875. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.M.; Owings, M.; Schwane, J.A. Improvement in running economy after 6 weeks of plyometric training. J. Strength Cond. Res. 2003, 17, 60–67. [Google Scholar] [PubMed]
- Byrne, C.; Twist, C.; Eston, R.G. Neuromuscular function after exercise-induced muscle damage: Theoretical and applied implications. Sports Med. 2004, 34, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Eston, R.G.; Byrne, C.; Twist, C. Muscle function after exercise-induced muscle damage: Considerations for athletic performance in children and adults. J. Exerc. Sci. Fit. 2003, 1, 85–96. [Google Scholar]
- Jakeman, J.R.; Byrne, C.; Eston, R.G. Lower limb compression garment improves recovery from exercise-induced muscle damage in young, active females. Eur. J. Appl. Physiol. 2010, 109, 1137–1144. [Google Scholar] [CrossRef] [PubMed]
- Marginson, V.; Rowland, A.V.; Gleeson, N.P.; Eston, R.G. Comparison of the symptoms of exercise-induced muscle damage after an initial and repeated bout of plyometric exercise in men and boys. J. Appl. Physiol. 2005, 99, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Twist, C.; Eston, R.G. The effects of exercise-induced muscle damage on maximal intensity intermittent exercise performance. Eur. J. Appl. Physiol. 2005, 94, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Twist, C.; Eston, R.G. The effect of muscle-damaging exercise on maximal intensity cycling and drop jump performance. J. Exerc. Sci. Fit 2007, 5, 79–87. [Google Scholar]
- Twist, C.; Eston, R.G. The effect of exercise-induced muscle damage on perceived exertion and cycling endurance performance. Eur. J. Appl. Physiol. 2009, 105, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Tofas, T.; Jumurtas, A.Z.; Fatouros, I.; Nikolaidis, M.G.; Koutedakis, Y.; Sinouris, E.A.; Papageorgakopoulou, N.; Theochathios, D.A. Plyometric exercise increases serum indices of muscle damage and collagen breakdown. J. Strength Cond. Res. 2008, 22, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Eston, R.G. The effects of exercise-induced muscle damage on isometric and dynamic knee extensor strength and vertical jump performance. J. Sports Sci. 2002, 20, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Chatzinikolaou, A.; Fatouros, I.G.; Gourgoulis, V.; Avloniti, A.; Jamurtas, A.Z.; Nikolaidis, M.G.; Douroudos, I.; Michailidis, Y.; Beneka, A.; Malliou, P.; et al. Time course of changes in performance and inflammatory responses after acute plyometric exercise. J. Strength Cond. Res. 2010, 24, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C.; Chen, H.-L.; Wu, C.-J.; Lin, M.-R.; Chen, C.-H.; Wang, L.-L.; Wang, S.-Y.; Tu, J.-H. Changes in running economy following a repeated bout of downhill running. J. Exerc. Sci. Fit. 2007, 5, 109–117. [Google Scholar] [CrossRef]
- Eston, R.G.; Peters, D. Effects of cold water immersion on the symptoms of exercise-induced muscle damage. J. Sports Sci. 1999, 17, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Miyama, M.; Nosaka, K. Influence of surface on muscle damage and soreness induced by consecutive drop jumps. J. Strength Cond. Res. 2004, 18, 206–211. [Google Scholar] [PubMed]
- Martel, G.F.; Harmer, M.L.; Logan, J.M.; Parker, C.B. Aquatic plyometric training increases vertical jump in female volleyball players. Med. Sci. Sports Exerc. 2005, 37, 1814–1819. [Google Scholar] [CrossRef] [PubMed]
- Barrett, R.S.; Neal, R.J.; Roberts, L.J. The dynamic loading response of surfaces encountered in beach running. J. Sci. Med. Sport 1997, 1, 1–11. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Rampinini, E.; Castagna, C.; Martino, F.; Fiorini, S.; Wisloff, U. Effect of plyometric training on sand versus grass on muscle soreness and jumping and sprinting ability in soccer players. Br. J. Sports Med. 2008, 42, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Harriss, D.J.; Atkinson, G. Ethical standards in sport and exercise science research. Int. J. Sports Med. 2011, 32, 819–821. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3, a flexible statistical power analysis program for the social, behavioural and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, H.M. Joint Motion and Function Assessment; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; pp. 177–178. [Google Scholar]
- Byrne, C.; Eston, R.G.; Edwards, R.H.T. Characteristics of isometric and dynamic strength loss following eccentric exercise-induced muscle damage. Scan. J. Med. Sci. Sports 2003, 11, 134–140. [Google Scholar] [CrossRef]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Leeds, UK, 1998. [Google Scholar]
- Brown, A.G.; Ray, M.W.; Abbey, B.M.; Shaw, B.S.; Shaw, I. Oxygen consumption, heart rate, and blood lactate responses to an acute bout of plyometric depth jumps in college-aged men and women. J. Strength Cond. Res. 2010, 24, 2475–2482. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.C.; Eston, R.G.; Poole, D.C.; Rowlands, A.V.; Dimenna, F.; Wilkerson, D.P.; Jones, A.M. The effect of eccentric exercise induced muscle damage on the dynamics of muscle oxygenation and pulmonary oxygen uptake. J. Appl. Physiol. 2008, 105, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.; Isaacs, A.W.; Myburgh, K.H. Preferntial type II muscle fiber damage from plyometric exercise. J. Athl. Train. 2012, 47, 414–420. [Google Scholar] [PubMed]
- Macaluso, F.; Isaacs, A.W.; di Felice, V.; Myburgh, K.H. Acute change of titin at mid-sarcomer remains despite 8 wk of plyometric training. J. Appl. Physiol. 2014, 116, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Eston, R.G. Maximal-intensity isometric and dynamic exercise performance after eccentric muscle actions. J. Sports Sci. 2002, 20, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Houmard, J.; Fraser, D.; Dudek, R.; Lambert, J.; Tracy, J. Normal forces and myofibrillar disruption after repeated eccentric exercise. J. Appl. Physiol. 1998, 84, 492–498. [Google Scholar] [PubMed]
- Costill, D.L.; Pascoe, D.D.; Fink, W.J. Impaired muscle glycogen synthesis after eccentric exercise. J. Appl. Physiol. 1990, 69, 46–50. [Google Scholar] [PubMed]
- Ingalls, C.P.; Warren, G.L.; Williams, J.H.; Ward, C.W.; Armstrong, R.B. E-C coupling failure in mouse EDL muscle after in vivo eccentric contractions. J. Appl. Physiol. 1999, 85, 58–67. [Google Scholar]
- Avela, J.; Kyrolainen, H.; Komi, P.V.; Rama, D. Reduced reflex sensivity persists several days after long-lasting stretch-shortening cycle exercise. J. Appl. Physiol. 1999, 86, 1292–1300. [Google Scholar] [PubMed]
- Komi, P.V. Stretch-shortening cycle: A powerful model to study normal and fatigued muscle. J. Biomech. 2000, 33, 1197–1206. [Google Scholar] [CrossRef]
- Warren, G.L.; Lowe, D.A.; Hayes, D.A.; Farmer, M.A.; Armstrong, R.B. Excitation failure in eccentric contraction-induced injury of mouse soleus muscle. J. Appl. Physiol. 1993, 68, 487–490. [Google Scholar] [CrossRef]
- Brockett, C.L.; Morgan, D.L.; Gregory, J.E.; Proske, U. Damage in different types of motor units following repeated active lengthening of the medial gastrocnemius muscle of the cat. J. Appl. Physiol. 2002, 92, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Highton, J.M.; Twist, C.; Eston, R.G. The effects of exercise-induced muscle damage on agility and sprint running performance. J. Exerc. Sci. Fit. 2009, 7, 24–30. [Google Scholar] [CrossRef]
- Semark, A.; Noakes, T.D.; St Clair Gibson, A.; Lambert, M.I. The effect of a prophylactic dose of flurbiprofen on muscle soreness and sprinting performance in trained subjects. J. Sports Sci. 1999, 17, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Binnie, M.J.; Dawson, B.; Pinnington, H.; Landers, G.; Peeling, P. Sand training: A review of current research and practical applications. J. Sports Sci. 2014, 32, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Binnie, M.J.; Dawson, B.; Arnot, M.A.; Pinnington, H.; Landers, G.; Peeling, P. Effect of sand versus grass training syrfaces during an 8-week pre-season conditioning programme in team sport athletes. J. Sports Sci. 2014, 32, 1001–1012. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, B.; Norasteh, A.; Saez de Villarreal, E.; Asadi, A. Effects of 6 weeks of depth jump vs. countermovement jump training on sand on muscle soreness and performance. Kinesiology 2014, 46, 97–108. [Google Scholar]

{kind=link}
| Group | Sets | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 * | 5 † | 6 | 7 | 8 | 9 ‡ | 10 ‡ | |
| AG | 8.25 ± 2.3 | 9 ± 2.3 | 9.1 ± 2.1 | 9.7 ± 2 | 10.8 ± 2.2 | 10.6 ± 2 | 11.2 ± 2.1 | 11.8 ± 1.8 | 12.7 ± 2.1 | 13.5 ± 2.1 |
| SG | 7.5 ± 0.9 | 8.5 ± 0.7 | 9.3 ± 1.1 | 10.3 ± 1.9 | 10.8 ± 2.1 | 11.7 ± 2.6 | 12.3 ± 2.6 | 12.8 ± 2.9 | 13.3 ± 2 | 14.1 ± 2 |
| FG | 7.1 ± 0.8 | 7 ± 1.4 | 8.62 ± 1.8 | 8.8 ± 2.1 | 9.1 ± 2.4 | 9.8 ± 2.8 | 10.5 ± 2.8 | 11 ± 3 | 11.2 ± 3.4 | 12 ± 3.8 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arazi, H.; Eston, R.; Asadi, A.; Roozbeh, B.; Saati Zarei, A. Type of Ground Surface during Plyometric Training Affects the Severity of Exercise-Induced Muscle Damage. Sports 2016, 4, 15. https://doi.org/10.3390/sports4010015
Arazi H, Eston R, Asadi A, Roozbeh B, Saati Zarei A. Type of Ground Surface during Plyometric Training Affects the Severity of Exercise-Induced Muscle Damage. Sports. 2016; 4(1):15. https://doi.org/10.3390/sports4010015
Chicago/Turabian StyleArazi, Hamid, Roger Eston, Abbas Asadi, Behnam Roozbeh, and Alireza Saati Zarei. 2016. "Type of Ground Surface during Plyometric Training Affects the Severity of Exercise-Induced Muscle Damage" Sports 4, no. 1: 15. https://doi.org/10.3390/sports4010015
APA StyleArazi, H., Eston, R., Asadi, A., Roozbeh, B., & Saati Zarei, A. (2016). Type of Ground Surface during Plyometric Training Affects the Severity of Exercise-Induced Muscle Damage. Sports, 4(1), 15. https://doi.org/10.3390/sports4010015