
Comparison of Lower Limb COP and Muscle Activation During Single-Leg Deadlift Using Elastic and Inelastic Barbells

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Measurement Tools and Procedures
2.3.1. COP and EMG Assessment
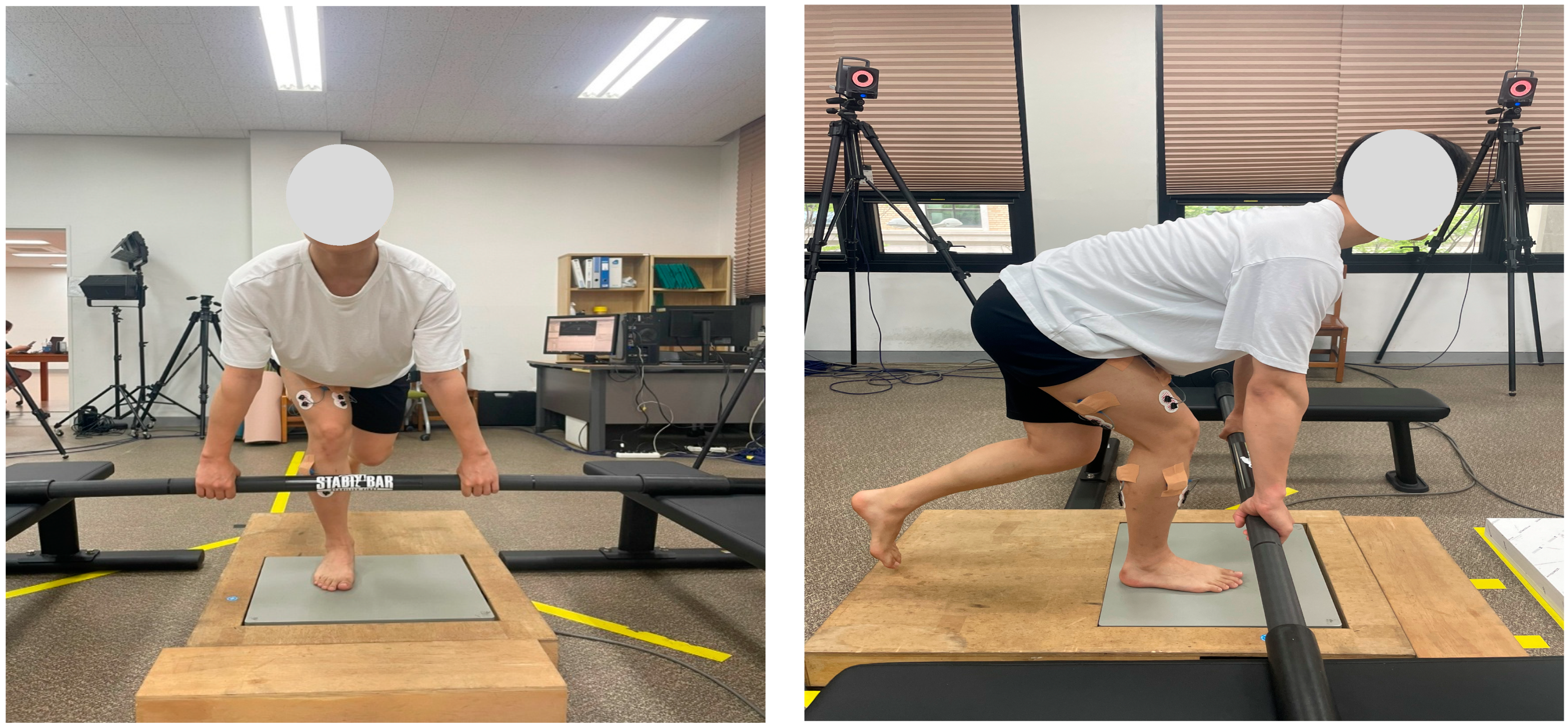
2.3.2. Data Collection Protocol
2.3.3. Data Processing and Analysis
2.4. Statistical Analysis
3. Results
3.1. Center of Pressure (COP)
3.2. Electromyography (EMG)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diamant, W.; Geisler, S.; Havers, T.; Knicker, A. Comparison of EMG activity between single-leg deadlift and conventional bilateral deadlift in trained amateur athletes: An empirical analysis. Int. J. Exerc. Sci. 2021, 14, 187–201. [Google Scholar] [PubMed]
- Mo, R.C.Y.; Ngai, D.C.W.; Ng, C.C.M.; Sin, K.H.S.; Luk, J.T.C.; Ho, I.M.K. Effects of loading positions on the activation of trunk and hip muscles during flywheel and dumbbell single-leg Romanian deadlift exercise. Front. Physiol. 2023, 14, 1264604. [Google Scholar] [CrossRef] [PubMed]
- Brughelli, M.; Cronin, J. Preventing hamstring injuries in sport. Strength Cond. J. 2008, 30, 55–64. [Google Scholar] [CrossRef]
- Weaver, A.; Kerksick, C. Implementing landmine single-leg Romanian deadlift into an athlete’s training program. Strength Cond. J. 2017, 39, 85–90. [Google Scholar] [CrossRef]
- DiStefano, L.J.; Blackburn, J.T.; Marshall, S.W.; Padua, D.A. Gluteal muscle activation during common therapeutic exercises. J. Orthop. Sports Phys. Ther. 2009, 39, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, S.; Azevedo, D.C.; Van Dillen, L. Diagnosis and treatment of movement system impairment syndromes. Braz. J. Phys. Ther. 2017, 21, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Llurda-Almuzara, L.; Pérez-Bellmunt, A.; Labata-Lezaun, N.; López-de-Celis, C.; Canet-Vintró, M.; Cadellans-Arroniz, A.; Moure-Romero, L.; Aiguadé-Aiguadé, R. Relationship between lower limb EMG activity and knee frontal plane projection angle during a single-legged drop jump. Phys. Ther. Sport 2021, 52, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Llurda-Almuzara, L.; Pérez-Bellmunt, A.; López-de-Celis, C.; Aiguadé, R.; Seijas, R.; Casasayas-Cos, O.; Labata-Lezaun, N.; Alvarez, P. Normative data and correlation between dynamic knee valgus and neuromuscular response among healthy active males: A cross-sectional study. Sci. Rep. 2020, 10, 17206. [Google Scholar] [CrossRef] [PubMed]
- Begalle, R.; DiStefano, L.; Blackburn, T.; Padua, D. Quadriceps and hamstrings coactivation during common therapeutic exercises. J. Athl. Train. 2012, 47, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Kuki, S.; Yoshida, T.; Okudaira, M.; Konishi, Y.; Ohyama-Byun, K.; Tanigawa, S. Force generation and neuromuscular activity in multi-joint isometric exercises: Comparison between unilateral and bilateral stance. J. Phys. Fit. Sports Med. 2018, 7, 289–296. [Google Scholar] [CrossRef]
- Biscarini, A.; Benvenuti, P.; Botti, F.M.; Brunetti, A.; Brunetti, O.; Pettorossi, V.E. Voluntary enhanced cocontraction of hamstring muscles during open kinetic chain leg extension exercise: Its potential unloading effect on the anterior cruciate ligament. Am. J. Sports Med. 2014, 42, 2103–2112. [Google Scholar] [CrossRef] [PubMed]
- Maniar, N.; Cole, M.H.; Bryant, A.L.; Opar, D.A. Muscle force contributions to anterior cruciate ligament loading. Sports Med. 2022, 52, 1737–1750. [Google Scholar] [CrossRef] [PubMed]
- van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2009, 53, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Liebenson, C. The Functional Training Handbook; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Juan, C.S. Single-leg training for two-legged sports: Efficacy of strength development in athletic performance. Strength Cond. J. 2001, 23, 35–37. [Google Scholar] [CrossRef]
- Boyle, M. Advances in Functional Training: Training Techniques for Coaches, Personal Trainers, and Athletes; Lotus Publishing: Terrace Park, OH, USA, 2011. [Google Scholar]
- Correa, R.V.; Verhagen, E.; Resende, R.A.; Ocarino, J.M. Performance in field tests and dynamic knee valgus in soccer players psychologically ready and not ready to return to sports after ACL reconstruction. Knee 2023, 42, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Gholami, F.; Letafatkar, A.; Moghadas Tabrizi, Y.; Gokeler, A.; Rossettini, G.; Abbaszadeh Ghanati, H.; Abbaszadeh Ghanati, W. Comparing the effects of differential and visuo-motor training on functional performance, biomechanical, and psychological factors in athletes after ACL reconstruction: A randomized controlled trial. J. Clin. Med. 2023, 12, 2845. [Google Scholar] [CrossRef] [PubMed]
- Makaruk, H.; Winchester, J.B.; Sadowski, J.; Czaplicki, A.; Sacewicz, T. Effects of unilateral and bilateral plyometric training on power and jumping ability in women. J. Strength Cond. Res. 2011, 25, 3311–3318. [Google Scholar] [CrossRef] [PubMed]
- Wyland, T.; Reyes, G.F. The implications of unilateral training on performance. Int. J. Exerc. Sci. Conf. Proc. 2013, 8, 23. [Google Scholar]
- Speirs, D.E.; Bennett, M.A.; Finn, C.V.; Turner, A.P. Unilateral vs. bilateral squat training for strength, sprints, and agility in academy rugby players. J. Strength Cond. Res. 2016, 30, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Howe, L.; Goodwin, J.; Blagrove, R. The integration of unilateral strength training for the lower extremity within an athletic performance programme. Prof. Strength Cond. 2014, 33, 19–24. [Google Scholar]
- McGill, S. Low Back Disorders: Evidence-Based Prevention and Rehabilitation, 3rd ed.; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Gonzalo-Skok, O.; Tous-Fajardo, J.; Suárez-Arrones, L.; Arjol-Serrano, J.L.; Casajús, J.A.; Méndez-Villanueva, A. Single-leg power output and between-limbs imbalances in team-sport players: Unilateral versus bilateral combined resistance training. Int. J. Sports Physiol. Perform. 2017, 12, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Navarro, F.; Casaña, J.; Pérez-Domínguez, B.; Ricart-Luna, B.; Cotolí-Suárez, P.; Calatayud, J. Dynamic balance and explosive strength appear to better explain single-leg hop test results among young elite female basketball athletes. Sci. Rep. 2023, 13, 5476. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Anderson, K.G. The role of instability with resistance training. J. Strength Cond. Res. 2006, 20, 716–722. [Google Scholar] [PubMed]
- Drinkwater, E.J.; Pritchett, E.J.; Behm, D.G. Effect of instability and resistance on unintentional squat-lifting kinetics. Int. J. Sports Physiol. Perform. 2007, 2, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Park, I.B.; Park, C.H.; Kim, K.T.; Cha, Y.J. The effects of dynamic neuromuscular stability exercise on scoliosis and pain control in youth baseball players. J. Mech. Med. Biol. 2021, 21, 2140030. [Google Scholar] [CrossRef]
- Nairn, B.C.; Sutherland, C.A.; Drake, J.D. Motion and muscle activity are affected by instability location during a squat exercise. J. Strength Cond. Res. 2017, 31, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Smania, N.; Corato, E.; Tinazzi, M.; Stanzani, C.; Fiaschi, A.; Girardi, P.; Gandolfi, M. Effect of balance training on postural instability in patients with idiopathic Parkinson’s disease. Neurorehabil. Neural Repair 2010, 24, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Pai, Y.C.; Bhatt, T.; Yang, F.; Wang, E. Perturbation training can reduce community-dwelling older adults’ annual fall risk: A randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1586–1594. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, A.; Wong, J.S.; Bryce, J.; Knorr, S.; Patterson, K.K. Does perturbation-based balance training prevent falls? Systematic review and meta-analysis of preliminary randomized controlled trials. Phys. Ther. 2014, 95, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Stephen, C.; Kamryn, A. Effect of instability training on compensatory muscle activation during perturbation challenge in young adults. J. Funct. Morphol. Kinesiol. 2023, 158, 136. [Google Scholar] [CrossRef] [PubMed]
- Randolph, E.; Anthony, C. Comparison of peak ground reaction force, joint kinetics and kinematics, and muscle activity between a flexible and steel barbell during the back squat exercise. J. Hum. Kinet. 2019, 68, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Morrissey, M.C.; Harman, E.A.; Johnson, M.J. Resistance training modes: Specificity and effectiveness. Med. Sci. Sports Exerc. 1995, 27, 648–660. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Selected Topics in Surface Electromyography for Use in the Occupational Setting: Expert Perspectives; NIOSH: Washington, DC, USA, 1992.
- Park, I.B.; Yeo, N.H.; Kim, J.T. A comparison analysis of EMG according to weight class and increase record of clean and jerk techniques in high school female weightlifters. Korean J. Sports Biomech. 2008, 18, 105–114. [Google Scholar] [CrossRef]
- Lee, S.; An, D.-H. Comparison of hip extensor muscle activities according to forward trunk lean angles during a single-leg deadlift. Phys. Ther. Korea 2023, 30, 8–14. [Google Scholar] [CrossRef]
- López-de-Celis, C.; Sánchez-Alfonso, N.; Rodríguez-Sanz, J.; Romaní-Sánchez, S.; Labata-Lezaun, N.; Canet-Vintró, M.; Aiguadé, R.; Pérez-Bellmunt, A. Quadriceps and gluteus medius activity during stable and unstable loading exercises in athletes: A cross-sectional study. J. Orthop. Res. 2024, 42, 317–325. [Google Scholar] [CrossRef] [PubMed]
- So, W.Y.; Hong, J.Y.; Choi, D.H. Regression analysis of one-repetition maximal strength from a 7–10, 11–15 repetition submaximal strength test in untrained men in their 20s. Exerc. Sci. 2009, 18, 419–428. [Google Scholar]
- Lafond, D.; Corriveau, H.; Hébert, R.; Prince, F. Intrasession reliability of center of pressure measures of postural steadiness in healthy elderly people. Arch. Phys. Med. Rehabil. 2004, 85, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, D.J.; Hubley-Kozey, C.L.; Stanish, W.D. Maximal voluntary isometric contraction exercise: A methodological investigation in moderate knee osteoarthritis. J. Electromyogr. Kinesiol. 2011, 21, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Badier, M.; Guillot, C.; Lagier-Tessonnier, F.; Burnet, H.; Jammes, Y. EMG power spectrum of respiratory and skeletal muscles during static contraction in healthy man. Muscle Nerve 1993, 16, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Saeterbakken, A.H.; Fimland, M.S. Muscle force output and electromyographic activity in squats with various unstable surfaces. J. Strength Cond. Res. 2013, 27, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Ditroilo, M.; O’Sullivan, R.; Harnan, B.; Crossey, A.; Gillmor, B.; Dardis, W.; Grainger, A. Water-filled training tubes increase core muscle activation and somatosensory control of balance during squat. J. Sports Sci. 2018, 36, 2002–2008. [Google Scholar] [CrossRef] [PubMed]
- Park, I.B. A comparison analysis of EMG on arm and trunk muscle between elastic and inelastic bar during the overhead press exercise. Korean J. Sports Biomech. 2022, 32, 128–133. [Google Scholar]
- Kowalski, T.; Schumann, M.; Klich, S.; Zanini, M. Equity in training load: Research design considerations for intervention assessment in sports science and physical therapy. Eur. J. Appl. Physiol. 2025, 125, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Perrey, S.; Quaresima, V.; Ferrari, M. Muscle oximetry in sports science: An updated systematic review. Sports Med. 2024, 54, 975–996. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Equipment | Model | Manufacture |
|---|---|---|
| Force platform | OR6 | AMTI, MA, USA |
| COP analysis software | Nexus v2.15 | Vicon, Oxford, UK |
| EMG equipment | Ultium System | Noraxon, AZ, USA |
| EMG analysis software | MR 3.20 | Noraxon, AZ, USA |
| 3D motion capture | MX-T20 | Vicon, Oxford, UK |
| Inelastic | Elastic | Source | F | p | η2 | ω2 | Bonferroni | ||
|---|---|---|---|---|---|---|---|---|---|
| AP | Normal a | 0.95 ± 0.21 | 0.90 ± 0.17 | Type | 6.509 | 0.017 * | 0.200 | 0.164 | a < b * |
| Fast b | 0.85 ± 0.26 | 0.81 ± 0.18 | Speed | 3.984 | 0.025 * | 0.133 | 0.052 | ||
| Power c | 0.91 ± 0.16 | 0.82 ± 0.13 | Type × Speed | 0.978 | 0.383 | 0.036 | 0.000 | ||
| ML | Normal a | 1.23 ± 0.20 | 1.18 ± 0.20 | Type | 9.996 | 0.004 ** | 0.278 | 0.243 | a < c *** b < c ** |
| Fast b | 1.21 ± 0.22 | 1.12 ± 0.25 | Speed | 18.330 | 0.000 *** | 0.413 | 0.243 | ||
| Power c | 1.10 ± 0.12 | 0.99 ± 0.10 | Type × Speed | 0.925 | 0.403 | 0.034 | 0.000 |
| Inelastic | Elastic | Source | F | p | η2 | ω2 | Bonferroni | ||
|---|---|---|---|---|---|---|---|---|---|
| GMed | Normal a | 30.93 ± 10.82 | 32.16 ± 11.74 | Type | 38.02 | 0.000 *** | 0.594 | 0.569 | a < b < c |
| Fast b | 32.94 ± 11.96 | 35.54 ± 12.51 | Speed | 64.327 | 0.000 *** | 0.712 | 0.531 | ||
| Power c | 42.73 ± 16.69 | 48.33 ± 17.57 | Type × Speed | 13.737 | 0.000 *** | 0.346 | 0.176 | ||
| RF | Normal a | 5.98 ± 3.21 | 5.79 ± 2.80 | Type | 2.035 | 0.166 | 0.073 | 0.036 | a < c b < c |
| Fast b | 6.38 ± 3.01 | 6.61 ± 3.24 | Speed | 101.176 | 0.000 *** | 0.796 | 0.643 | ||
| Power c | 12.12 ± 4.69 | 12.98 ± 5.73 | Type × Speed | 1.352 | 0.260 | 0.049 | 0.000 | ||
| VM | Normal a | 14.23 ± 5.89 | 13.63 ± 6.16 | Type | 0.028 | 0.869 | 0.001 | 0.000 | a < c b < c |
| Fast b | 14.95 ± 5.87 | 14.47 ± 5.61 | Speed | 74.909 | 0.000 *** | 0.742 | 0.570 | ||
| Power c | 24.25 ± 10.27 | 25.13 ± 9.71 | Type × Speed | 1.534 | 0.229 | 0.056 | 0.000 | ||
| VL | Normal a | 19.05 ± 7.06 | 18.03 ± 6.94 | Type | 0.497 | 0.487 | 0.019 | 0.000 | a < c b < c |
| Fast b | 19.48 ± 6.82 | 18.86 ± 6.72 | Speed | 104.290 | 0.000 *** | 0.800 | 0.650 | ||
| Power c | 28.96 ± 8.99 | 29.75 ± 9.40 | Type × Speed | 2.561 | 0.106 | 0.090 | 0.010 | ||
| BF | Normal a | 23.69 ± 9.76 | 24.58 ± 8.76 | Type | 21.976 | 0.000 *** | 0.485 | 0.428 | a < c b < c |
| Fast b | 23.58 ± 10.00 | 26.29 ± 10.65 | Speed | 30.430 | 0.000 *** | 0.539 | 0.341 | ||
| Power c | 27.46 ± 9.73 | 30.14 ± 12.05 | Type × Speed | 1.721 | 0.194 | 0.062 | 0.000 | ||
| ST | Normal a | 24.21 ± 9.92 | 24.47 ± 9.42 | Type | 15.165 | 0.001 ** | 0.368 | 0.336 | a < b < c |
| Fast b | 24.83 ± 10.19 | 26.86 ± 10.50 | Speed | 56.494 | 0.000 *** | 0.685 | 0.498 | ||
| Power c | 31.58 ± 13.08 | 34.69 ± 14.79 | Type × Speed | 6.757 | 0.002 ** | 0.206 | 0.080 | ||
| GCN | Normal a | 32.82 ± 11.17 | 33.34 ± 9.48 | Type | 13.063 | 0.001 ** | 0.334 | 0.301 | a < b < c |
| Fast b | 34.23 ± 11.29 | 36.73 ± 13.95 | Speed | 91.073 | 0.000 *** | 0.778 | 0.618 | ||
| Power c | 45.49 ± 15.08 | 49.62 ± 16.11 | Type × Speed | 3.135 | 0.052 | 0.108 | 0.020 | ||
| TA | Normal a | 24.56 ± 9.13 | 22.77 ± 7.41 | Type | 0.289 | 0.595 | 0.011 | 0.000 | a < c |
| Fast b | 25.08 ± 8.43 | 25.65 ± 8.59 | Speed | 146.662 | 0.000 *** | 0.849 | 0.725 | ||
| Power c | 38.28 ± 9.16 | 40.72 ± 11.64 | Type × Speed | 3.617 | 0.034 * | 0.122 | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, J.; Park, I. Comparison of Lower Limb COP and Muscle Activation During Single-Leg Deadlift Using Elastic and Inelastic Barbells. Sports 2025, 13, 242. https://doi.org/10.3390/sports13080242
Jeong J, Park I. Comparison of Lower Limb COP and Muscle Activation During Single-Leg Deadlift Using Elastic and Inelastic Barbells. Sports. 2025; 13(8):242. https://doi.org/10.3390/sports13080242
Chicago/Turabian StyleJeong, Jihwan, and Ilbong Park. 2025. "Comparison of Lower Limb COP and Muscle Activation During Single-Leg Deadlift Using Elastic and Inelastic Barbells" Sports 13, no. 8: 242. https://doi.org/10.3390/sports13080242
APA StyleJeong, J., & Park, I. (2025). Comparison of Lower Limb COP and Muscle Activation During Single-Leg Deadlift Using Elastic and Inelastic Barbells. Sports, 13(8), 242. https://doi.org/10.3390/sports13080242