
Adaptations of the Autonomic Nervous System and Body Composition After 8 Weeks of Specific Training and Nutritional Re-Education in Amateur Muay Thai Fighters: A Clinical Trial

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Training Program and Intervention
2.4. Measures
2.4.1. 10 s Frequency Speed of Kick Test (FSKT-10s)
2.4.2. Multiple Frequency Speed of Kick Test (FSKT-Mult)
2.4.3. Bioimpedance Analysis (BIA)
2.4.4. Cardiac Autonomic Modulation (CAM)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANS | Autonomic nervous system |
| ApEn | Approximate entropy |
| BIA | Bioimpedance analysis |
| BMR | Basal metabolic rate |
| CAM | Cardiac autonomic modulation |
| FSKT-10s | 10 s frequency speed of kick test |
| FSKT-multi | Multiple frequency speed of kick test |
| HF | The high frequency range |
| HR | Heart rate |
| HRV | Heart rate variability |
| LF | The low frequency range |
| MT | Muay Thai |
| pNN50 | The percentage of adjacent RR intervals with a difference in duration greater than 50 ms |
| PNS | Parasympathetic nervous system |
| rMSSD | The square root of the mean squared differences of consecutive RR intervals |
| RR mean | Mean RR intervals |
| SD1 | The standard deviation measuring the dispersion of points in the plot perpendicular to the line of identity |
| SD2 | The standard deviation measuring the dispersion of points along the line of identity |
| SDNN | Standard deviation of RR intervals |
| SNS | Sympathetic nervous system |
| TINN | Triangular interpolation of RR interval histogram |
| UNISUAM | Centro Universitário Augusto Motta |
References
- Prasetyo, Y.T.; Cahigas, M.M.L.; Patrick, E.; Rodney, M.; Nadlifatin, R.; Persada, S.F. Indonesian martial artists’ preferences in martial arts schools: Sustaining business competitiveness through conjoint analysis. PLoS ONE 2024, 19, e0301229. [Google Scholar] [CrossRef] [PubMed]
- Monterrosa Quintero, A.; Rios, A.R.E.; Fuentes-Garcia, J.P.; Sanchez, J.C.G. Levels of physical activity and psychological well-being in non-athletes and martial art athletes during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4004. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, B.T.C.; Ritti-Dias, R.M.; Farah, B.Q.; Suetake, V.Y.B.; Diniz, T.A.; Costa Júnior, P.; Milanez, V.F.; Christofaro, D.G.D. Cardiovascular effects of 16 weeks of martial arts training in adolescents. Rev. Bras. Med. Esporte 2018, 24, 212–215. [Google Scholar] [CrossRef]
- Saraiva, B.T.C.; Franchini, E.; Ribeiro, A.S.; Gobbo, L.A.; Correia, M.A.; Vanderlei, L.C.M.; Ferrari, G.; Tebar, W.R.; Christofaro, D.G.D. Effects of 12 weeks of functional training vs. Muay Thai on cardiac autonomic modulation and hemodynamic parameters in older adults: A randomized clinical trial. BMC Cardiovasc. Disord. 2024, 24, 433. [Google Scholar] [CrossRef]
- Saraiva, B.T.C.; Franchini, E.; Vanderlei, L.C.M.; Milanez, V.F.; Tebar, W.R.; Beretta, V.S.; Ritti-Dias, R.M.; Christofaro, D.G.D. Effects of 16-week Muay Thai practice on cardiovascular parameters in children and adolescents with overweight/obesity. Sport Sci. Health 2024, 20, 647–657. [Google Scholar] [CrossRef]
- Blais, L.; Trilles, F. The progress achieved by judokas after strength training with a judo-specific machine. J. Sports Sci. Med. 2006, 5, 132–135. [Google Scholar]
- Aminaei, M.; Yazdani, S.; Amirseifadini, M. Effects of Plyometric and Cluster Resistance Training on Explosive Power and Maximum Strength in Karate Players. Int. J. Appl. Exerc. Physiol. 2017, 6, 34–44. [Google Scholar] [CrossRef]
- Apollaro, G.; Panascì, M.; Ouergui, I.; Falcó, C.; Franchini, E.; Ruggeri, P.; Faelli, E. Influence of body composition and muscle power performance on multiple frequency speed of kick test in taekwondo athletes. Sports 2024, 12, 322. [Google Scholar] [CrossRef]
- Ojeda-Aravena, A.; Herrera-Valenzuela, T.; Valdés-Badilla, P.; Cancino-López, J.; Zapata-Bastias, J.; García-García, J.M. Effects of 4 weeks of a technique-specific protocol with high-intensity intervals on general and specific physical fitness in taekwondo athletes: An inter-individual analysis. Int. J. Environ. Res. Public Health 2021, 18, 3643. [Google Scholar] [CrossRef]
- Suetake, V.Y.B.; Franchini, E.; Saraiva, B.T.C.; Da Silva, A.K.F.; Bernardo, A.F.B.; Gomes, R.L.; Vanderlei, L.C.M.; Christofaro, D.G.D. Effects of 9 months of martial arts training on cardiac autonomic modulation in healthy children and adolescents. Pediatr. Exerc. Sci. 2018, 30, 487–494. [Google Scholar] [CrossRef]
- Catai, A.M.; Pastre, C.M.; de Godoy, M.F.; da Silva, E.; de Takahashi, A.C.M.; Vanderlei, L.C.M. Heart rate variability: Are you using it properly? Standardisation checklist of procedures. Braz. J. Phys. Ther. 2020, 24, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Rapkiewicz, J.A.; Nunes, J.P.; Mayhew, J.L.; Ribeiro, A.S.; Nabuco, H.C.; Favero, M.T.; Franchini, E.; Do Nascimento, M.A. Effects of Muay Thai training frequency on body composition and physical fitness in healthy untrained women. J. Sports Med. Phys. Fit. 2018, 58, 1808–1814. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, P.; Eick, C.; Blum, S.; Schlageter, V.; Bauer, A.; Rizas, K.D.; Eken, C.; Coslovsky, M.; Aeschbacher, S.; Krisai, P.; et al. Heart rate variability triangular index as a predictor of cardiovascular mortality in patients with atrial fibrillation. J. Am. Heart Assoc. 2020, 9, e016075. [Google Scholar] [CrossRef] [PubMed]
- Latorre-Román, P.Á.; de la Casa Pérez, A.; Pancorbo-Serrano, D.; Consuegra-Gonzalez, P.J.; Salas-Sánchez, J.; Muñoz-Jiménez, M.; Aragón-Vela, J.; Ramírez Lucas, J.M.; Cabrera-Linares, J.C.; Párraga-Montilla, J.A. Influence of physical fitness and weight status on autonomic cardiac modulation in children. Pediatr. Res. 2023, 94, 1754–1763. [Google Scholar] [CrossRef]
- Abreu, R.M.; Rehder-Santos, P.; Simões, R.P.; Catai, A.M. Can high-intensity interval training change cardiac autonomic control? A systematic review. Braz. J. Phys. Ther. 2019, 23, 279–289. [Google Scholar] [CrossRef]
- Machado, L.M.A.; de Medeiros, K.C.M. Perfil nutricional de praticantes de Muay Thai. RBNE Rev. Bras. Nutr. Esportiva 2017, 11, 558–569. [Google Scholar]
- Dias, S.B.C.D.; Oliveira, E.B.; Júnior, A.G.B. Teoria e Prática do Treinamento para MMA; Phorte: São Paulo, Brazil, 2017. [Google Scholar]
- Doherty, C.S.; Fortington, L.V.; Barley, O.R. Rapid weight changes and competitive outcomes in Muay Thai and mixed martial arts: A 14-month study of 24 combat sports events. Sports 2024, 12, 280. [Google Scholar] [CrossRef]
- Bueno, J.C.A.; Aoki, M.S.; Coswig, V.S.; Silveira, E.P.; Alves, R.C.; Andrade, A.; Souza Junior, T.P. Anthropometric profile and dietary intake of amateurs and professional mixed martial arts athletes. Rev. Artes Marciales Asiáticas 2024, 19, 115–128. [Google Scholar] [CrossRef]
- Zimmermann, L.C.; Cezar, T.M. Avaliação de sinais e sintomas através do rastreamento metabólico em grupo de emagrecimento realizado com colaboradores de um centro universitário do oeste do Paraná. FAG J. Health 2019, edição especial, 20–21. [Google Scholar] [CrossRef]
- Discursos da Gastronomia Brasileira: Gêneros e Identidade Nacional Postos à Mesa. Available online: https://lume.ufrgs.br/handle/10183/13731 (accessed on 18 February 2025).
- Ouergui, I.; Delleli, S.; Messaoudi, H.; Chtourou, H.; Bouassida, A.; Bouhlel, E.; Franchini, E.; Ardigò, L.P. Acute effects of different activity types and work-to-rest ratio on post-activation performance enhancement in young male and female taekwondo athletes. Int. J. Environ. Res. Public Health 2022, 19, 1764. [Google Scholar] [CrossRef]
- Chiu, C.H.; Chen, C.H.; Yang, T.J.; Chou, K.M.; Chen, B.W.; Lin, Z.Y.; Lin, Y.C. Carbohydrate mouth rinsing decreases fatigue index of taekwondo frequency speed of kick test. Chin. J. Physiol. 2022, 65, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Micheli, M.L.; Pagani, L.; Marella, M.; Gulisano, M.; Piccoli, A.; Angelini, F.; Burtscher, M.; Gatterer, H. Bioimpedance and impedance vector patterns as predictors of league level in male soccer players. Int. J. Sports Physiol. Perform. 2014, 9, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Ramos, E.; Vanderlei, L.; Ramos, D.; Teixeira, L.; Pitta, F.; Veloso, M. Influence of pursed-lip breathing on heart rate variability and cardiorespiratory parameters in subjects with chronic obstructive pulmonary disease (COPD). Braz. J. Phys. Ther. 2009, 13, 288–293. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Slimani, M.; Chaabene, H.; Miarka, B.; Franchini, E.; Chamari, K.; Cheour, F. Kickboxing review: Anthropometric, psychophysiological and activity profiles and injury epidemiology. Biol. Sport 2017, 34, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, D.; Climstein, M.; Whitting, J.; Del Vecchio, L. Impact force and velocities for kicking strikes in combat sports: A literature review. Sports 2024, 12, 74. [Google Scholar] [CrossRef]
- Ouergui, I.; Delleli, S.; Messaoudi, H.; Bridge, C.A.; Chtourou, H.; Franchini, E.; Ardigò, L.P. Effects of conditioning activity mode, rest interval and effort to pause ratio on post-activation performance enhancement in taekwondo: A randomized study. Front. Physiol. 2023, 14, 1179309. [Google Scholar] [CrossRef]
- Ramakrishnan, K.R.; Wang, H.; Shankar, K.; Fien, A. A new method for the measurement and analysis of biomechanical energy delivered by kicking. Sports Eng. 2018, 21, 53–62. [Google Scholar] [CrossRef]
- Yu, D.; Yu, Y.; Wilde, B.; Shan, G. Biomechanical characteristics of the Axe Kick in Tae Kwon-Do. Arch. Budo 2012, 8, 213–218. [Google Scholar] [CrossRef]
- Anyżewska, A.; Dzierżanowski, I.; Woźniak, A.; Leonkiewicz, M.; Wawrzyniak, A. Rapid weight loss and dietary inadequacies among martial arts practitioners from Poland. Int. J. Environ. Res. Public Health 2018, 15, 2476. [Google Scholar] [CrossRef]
- Cha, J.Y.; Jee, Y.S. Wushu Nanquan training is effective in preventing obesity and improving heart function in youth. J. Exerc. Rehabil. 2018, 14, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Granero-Gallegos, A.; González-Quílez, A.; Plews, D.; Carrasco-Poyatos, M. HRV-based training for improving VO2max in endurance athletes. A systematic review with meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 7999. [Google Scholar] [CrossRef]
- Slimani, M.; Davis, P.; Franchini, E.; Moalla, W. Rating of perceived exertion for quantification of training and combat loads during combat sport-specific activities: A short review. J. Strength Cond. Res. 2017, 31, 2889–28902. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Pre-Training | Post-Training | p-Value |
|---|---|---|---|
| Body mass (kg) | 83.4 ± 18 | 84.2 ± 16.7 | 0.28 |
| BMI (kg/m2) | 26.3 ± 4.6 | 26.6 ± 4 | 0.20 |
| Body fat (%) | 13 (10–14) | 12 (11–13) | 0.89 |
| Body fat (kg) | 10.1 (7.5–13.3) | 9.9 (7.4–12.9) | 0.81 |
| FFM (%) | 87 (78–89) | 88 (86–90) | 0.088 |
| FFM (kg) | 68 (62–85) | 71 (62–84) | 0.031 |
| TBW (%) | 64 (64–65) | 64 (63–66) | 0.68 |
| TBW (L) | 50 (45–63) | 52 (46–60) | 0.27 |
| BMR (kcal) | 1878 (1748–2125) | 2063 (1806–2414) | 0.020 |
| Variables | Pre-Training | Post-Training | p-Value |
|---|---|---|---|
| RR mean (ms) | 765 (662–891) | 810 (738–900) | 0.57 |
| Maximum HR (bpm) | 78 (67–91) | 74 (66.5–81.5) | 0.63 |
| SDNN (ms) | 80 (62–106) | 87 (57–254) | 0.34 |
| rMSSD (ms) | 78 (60–125) | 87 (62–323) | 0.41 |
| pNN50 (%) | 30.9 (10.3–40.1) | 34.5 (30.5–48.3) | 0.11 |
| TINN (ms) | 546 (409–966) | 537 (333–2376) | 0.43 |
| LF (nu) | 51.8 (37.7–55.9) | 49.5 (32.2–52.8) | 0.09 |
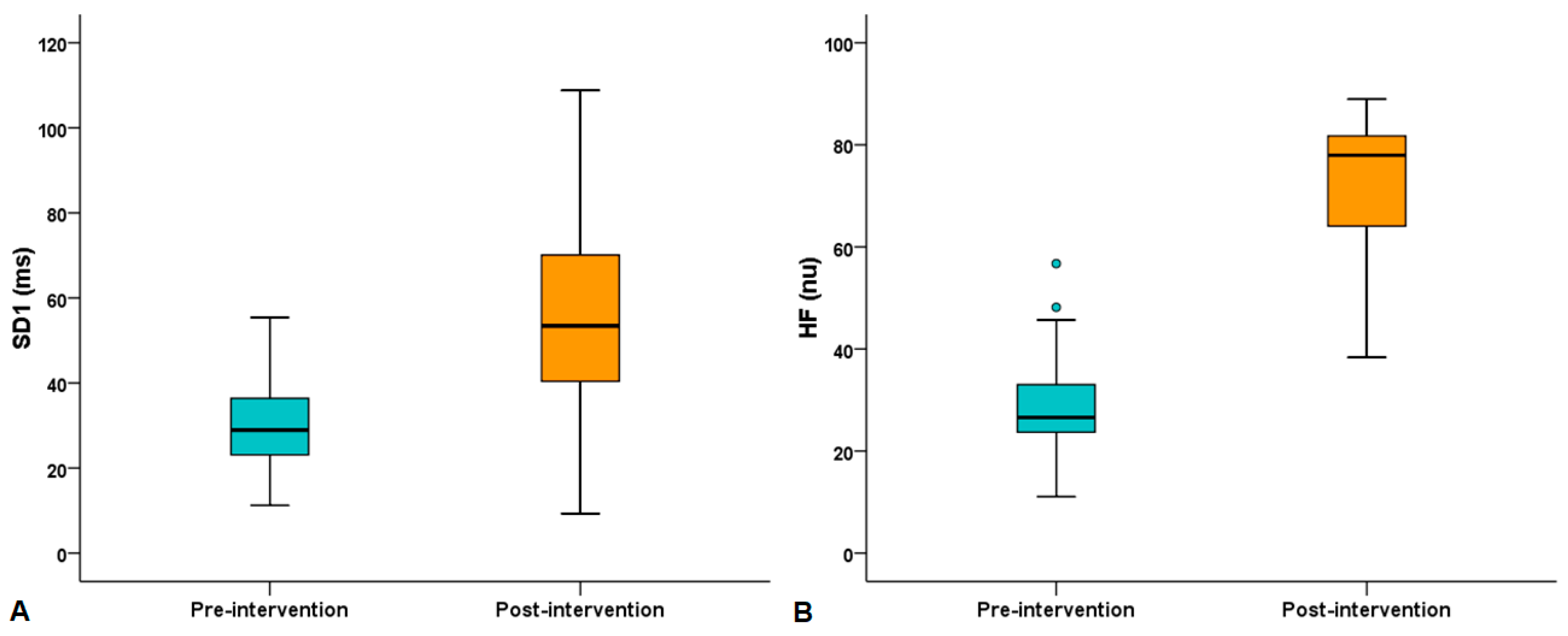
| HF (nu) | 26.6 (23.2–34.8) | 78 (62.9–82) | <0.0001 |
| LF/HF | 1.47 (0.73–2.69) | 1.07 (0.61–1.27) | 0.073 |
| SD1 (ms) | 28.9 (22.9–36.8) | 53.4 (40–77.8) | 0.001 |
| SD2 (ms) | 90 (73–121) | 102 (67–276) | 0.26 |
| SD2/SD1 | 1.38 (1.18–1.77) | 1.61 (1.32–2.12) | 0.29 |
| ApEn | 61 (0.85–134) | 125 (0.77–229) | 0.41 |
| PNS index | 0.71 (−0.56–2.27) | 0.82 (−0.33–7.13) | 0.54 |
| SNS index | 0.37 (738–900) | −0.05 (−0.87–0.95) | 0.57 |
| Variables | Pre-Training | Post-Training | p-Value |
|---|---|---|---|
| RR mean (ms) | 403 (382–452) | 387 (379–420) | 0.48 |
| Maximum HR (bpm) | 149 (133–157) | 155 (143–158.5) | 0.41 |
| SDNN (ms) | 71 (45–128) | 46 (38–82) | 0.60 |
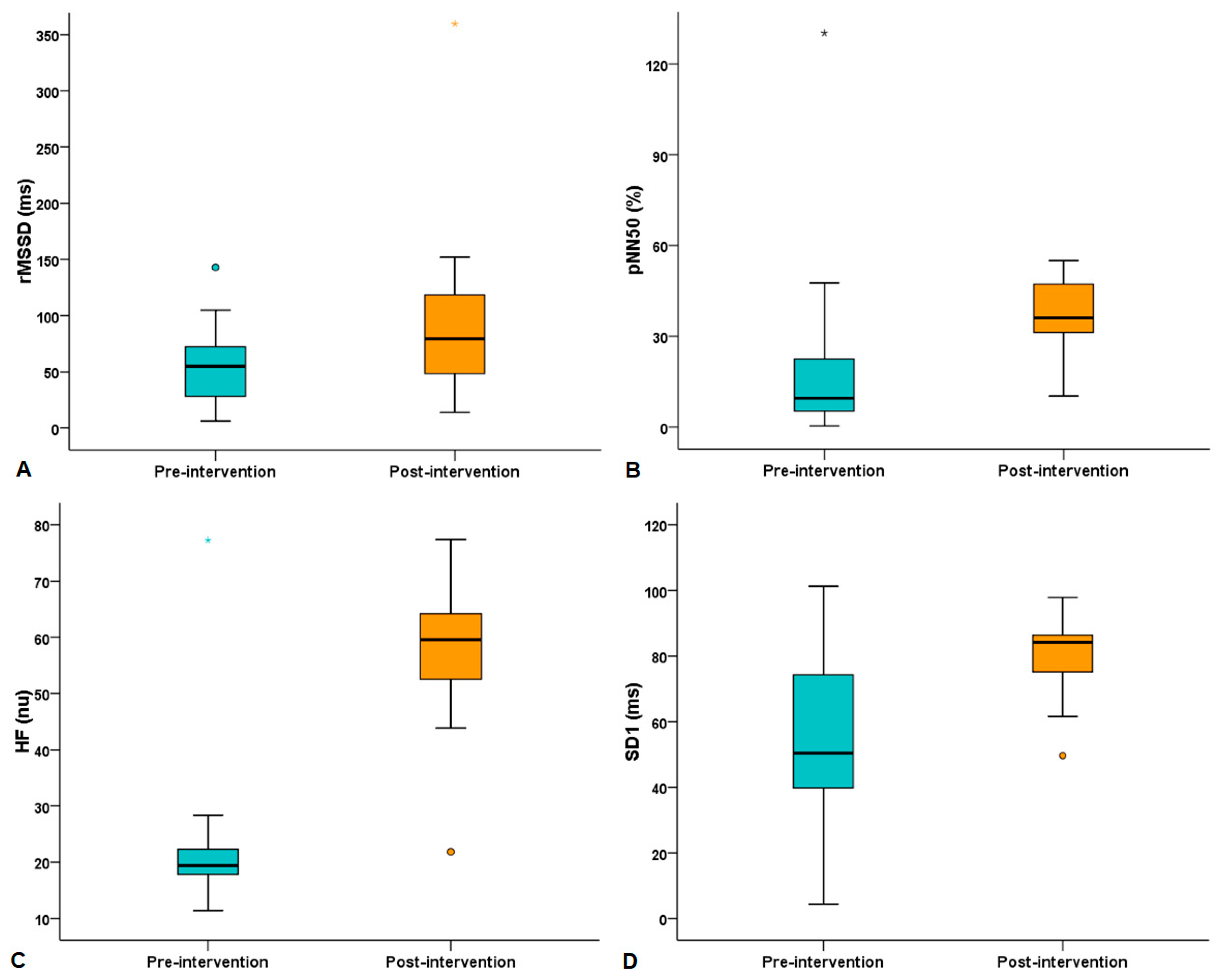
| rMSSD (ms) | 55 (27–76) | 79 (47–131) | 0.005 |
| pNN50 (%) | 9.6 (5–26.1) | 36.2 (24.4–48) | 0.002 |
| TINN (ms) | 539 (357–722) | 431 (286–708) | 0.74 |
| LF (nu) | 55.8 (33.2–69.3) | 39 (29.6–67.2) | 0.36 |
| HF (nu) | 19.5 (16.9–22.5) | 59.5 (51.5–65.6) | <0.0001 |
| LF/HF | 1.26 (0.50–2.07) | 0.64 (0.42–2.20) | 0.45 |
| SD1 (ms) | 50.4 (39.4–79.5) | 84.2 (74.8–88.1) | 0.004 |
| SD2 (ms) | 50 (41–85) | 72 (44–146) | 0.69 |
| SD2/SD1 | 1.13 (1–1.27) | 1.17 (1–1.74) | 0.54 |
| ApEn | 0.32 (0.27–0.50) | 0.44 (0.34–0.71) | 0.071 |
| PNS index | −2.38 (−2.81–0.82) | −0.77 (−2.11–1.03) | 0.16 |
| SNS index | 7.66 (5.38–8.56) | 6.75 (4.87–7.81) | 0.61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Andrade Junior, A.B.; de Andrade, E.M.P.R.; de Souza, G.R.; Lopes, A.J. Adaptations of the Autonomic Nervous System and Body Composition After 8 Weeks of Specific Training and Nutritional Re-Education in Amateur Muay Thai Fighters: A Clinical Trial. Sports 2025, 13, 72. https://doi.org/10.3390/sports13030072
de Andrade Junior AB, de Andrade EMPR, de Souza GR, Lopes AJ. Adaptations of the Autonomic Nervous System and Body Composition After 8 Weeks of Specific Training and Nutritional Re-Education in Amateur Muay Thai Fighters: A Clinical Trial. Sports. 2025; 13(3):72. https://doi.org/10.3390/sports13030072
Chicago/Turabian Stylede Andrade Junior, Antonio Beira, Elena Marie Peixoto Ruthes de Andrade, Guilherme Rodrigues de Souza, and Agnaldo José Lopes. 2025. "Adaptations of the Autonomic Nervous System and Body Composition After 8 Weeks of Specific Training and Nutritional Re-Education in Amateur Muay Thai Fighters: A Clinical Trial" Sports 13, no. 3: 72. https://doi.org/10.3390/sports13030072
APA Stylede Andrade Junior, A. B., de Andrade, E. M. P. R., de Souza, G. R., & Lopes, A. J. (2025). Adaptations of the Autonomic Nervous System and Body Composition After 8 Weeks of Specific Training and Nutritional Re-Education in Amateur Muay Thai Fighters: A Clinical Trial. Sports, 13(3), 72. https://doi.org/10.3390/sports13030072