
The Significance of Maximal Squat Strength for Neuromuscular Knee Control in Elite Handball Players: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedure
2.3. Measurements
2.3.1. Muscle Strength Test
2.3.2. Unilateral Vertical Drop Jump
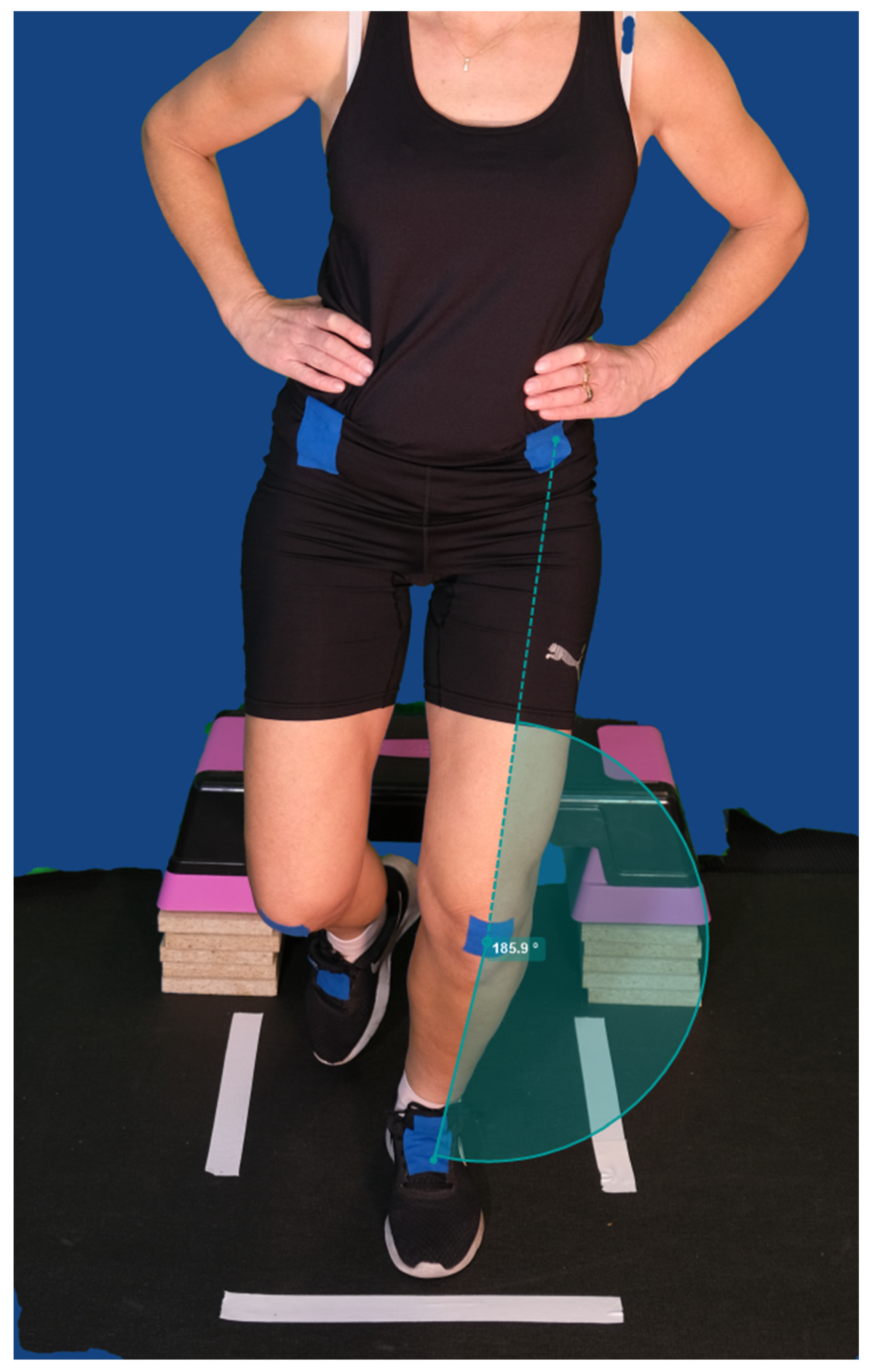
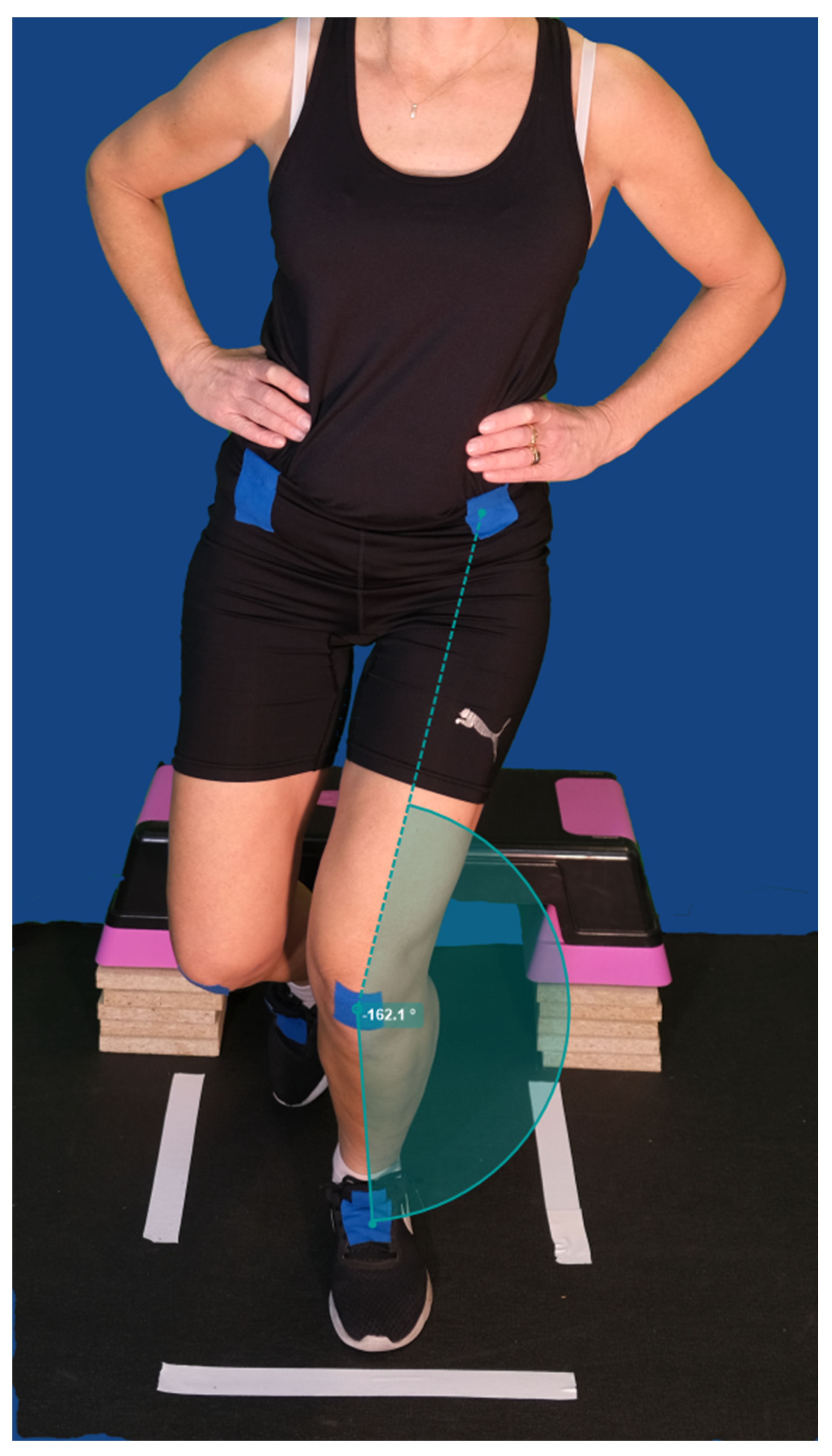
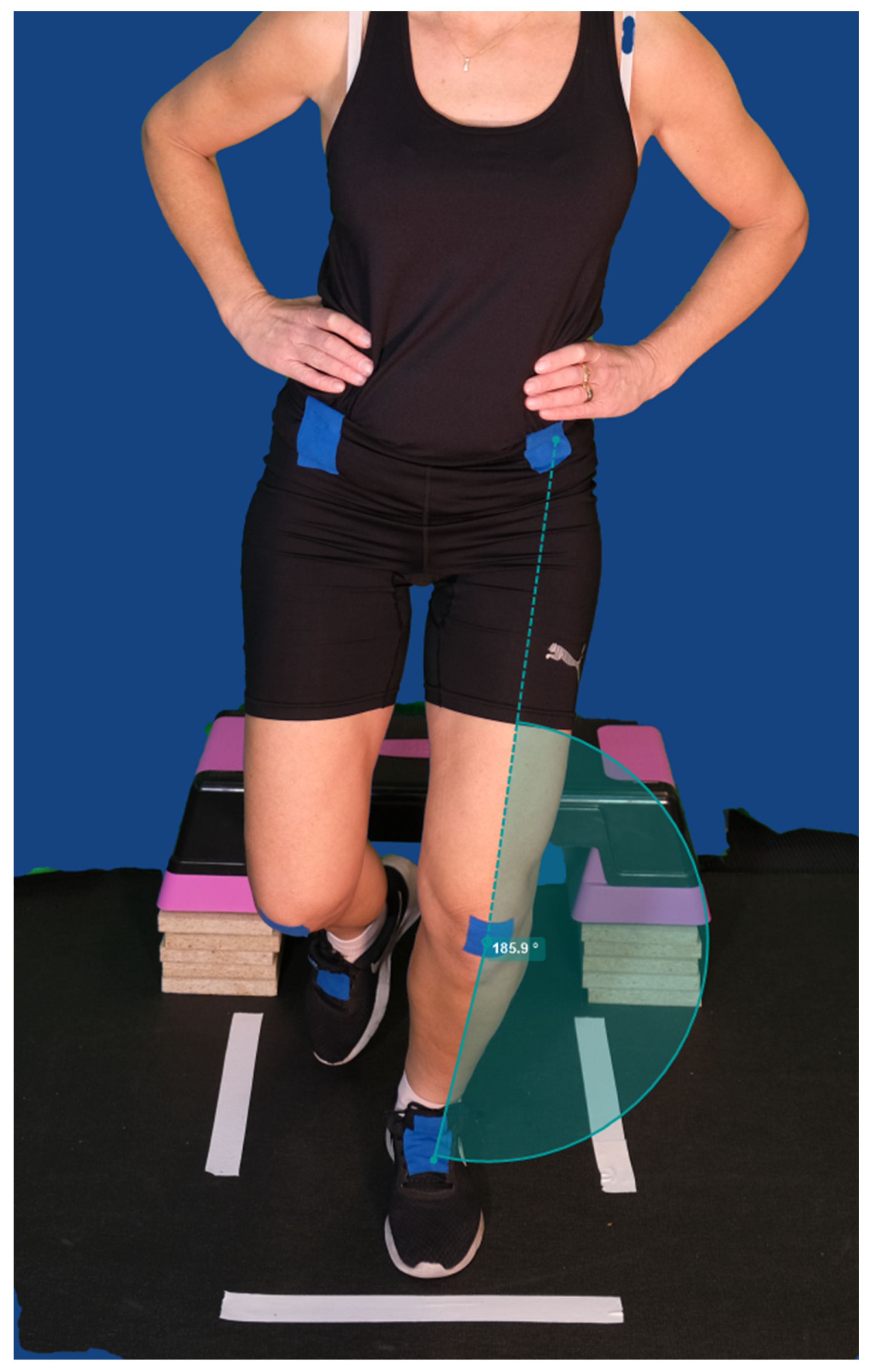
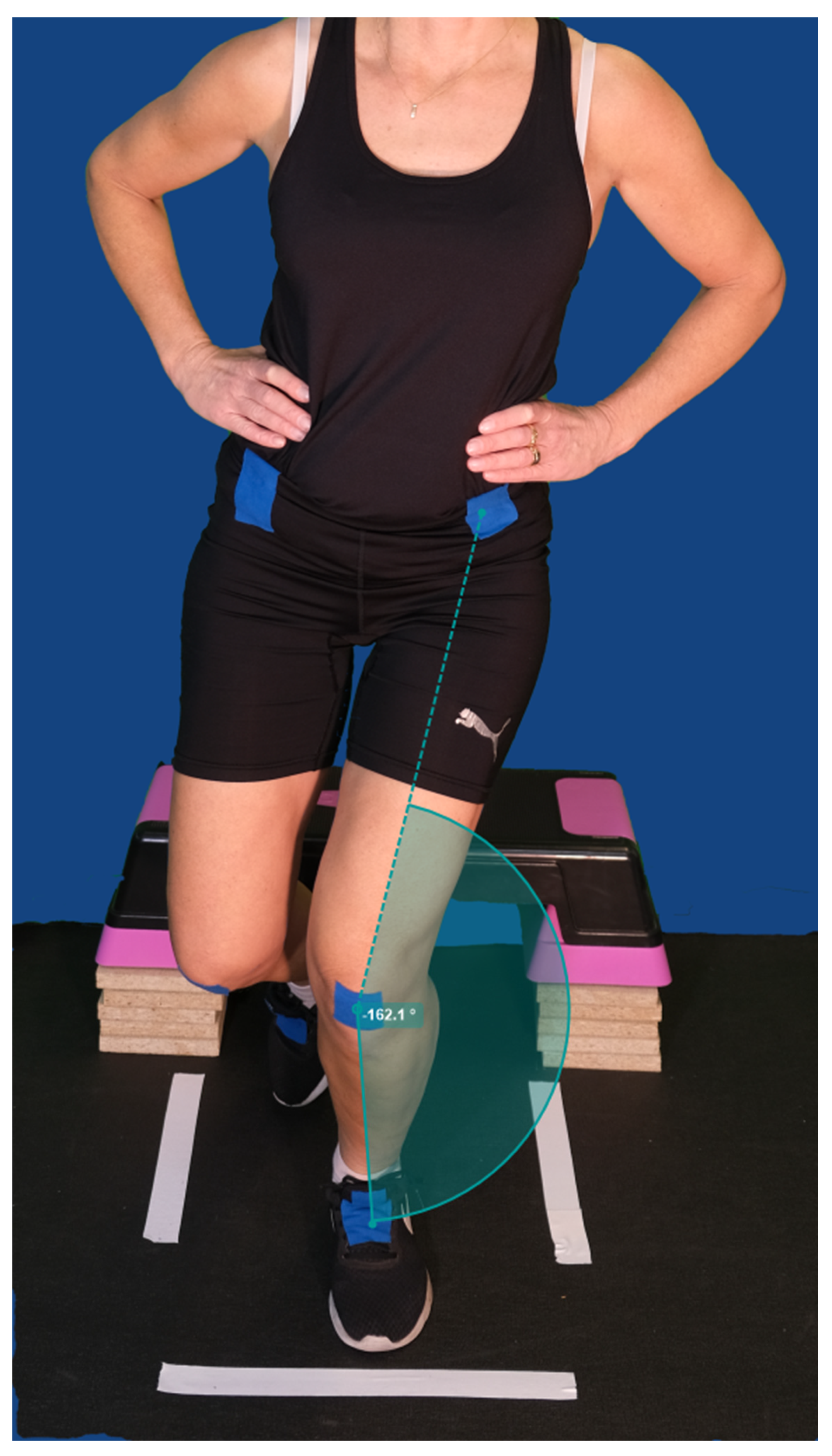
2.3.3. Assessment of Dynamic Knee Valgus
2.4. Statistical Analysis
3. Results
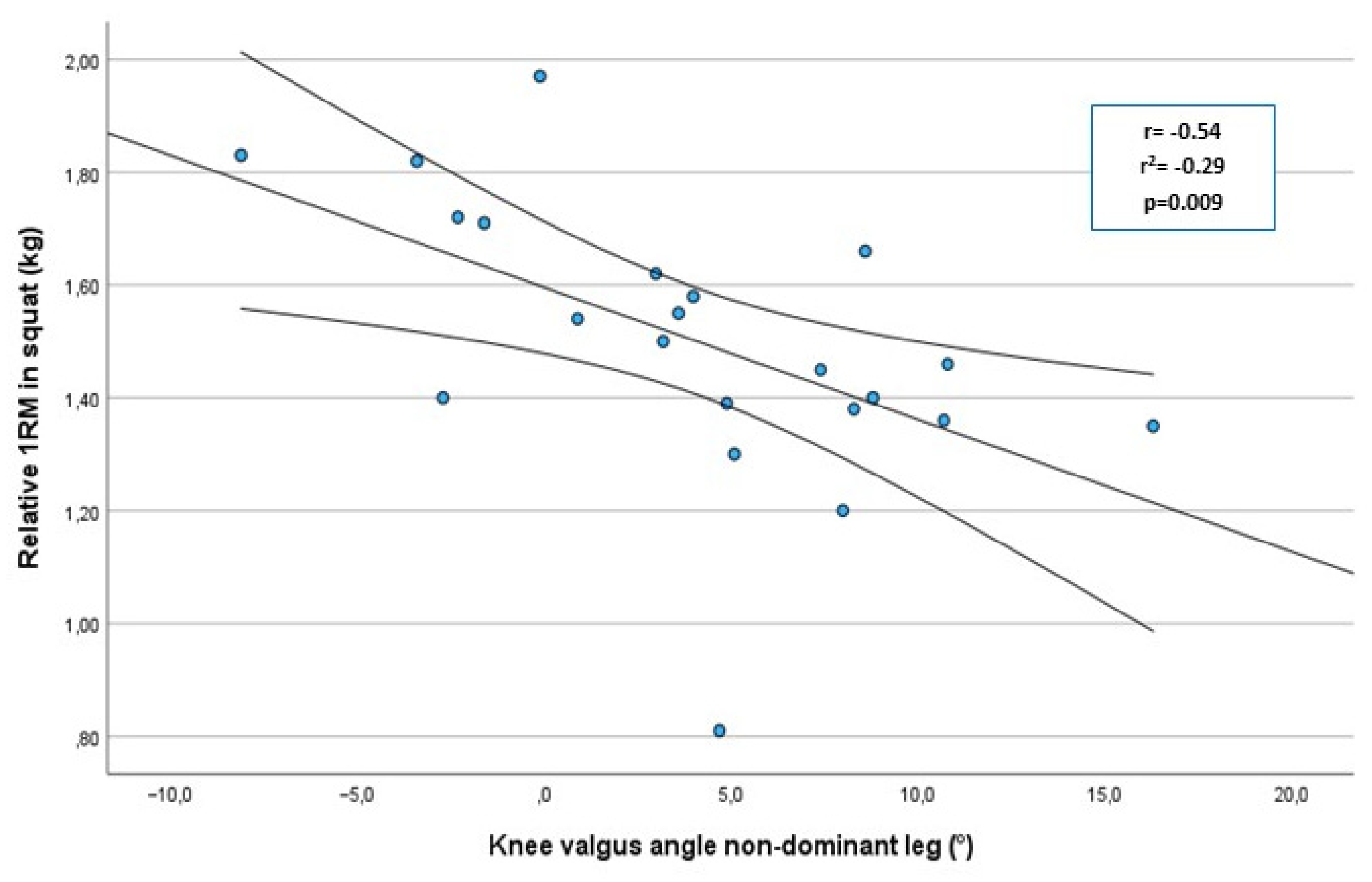
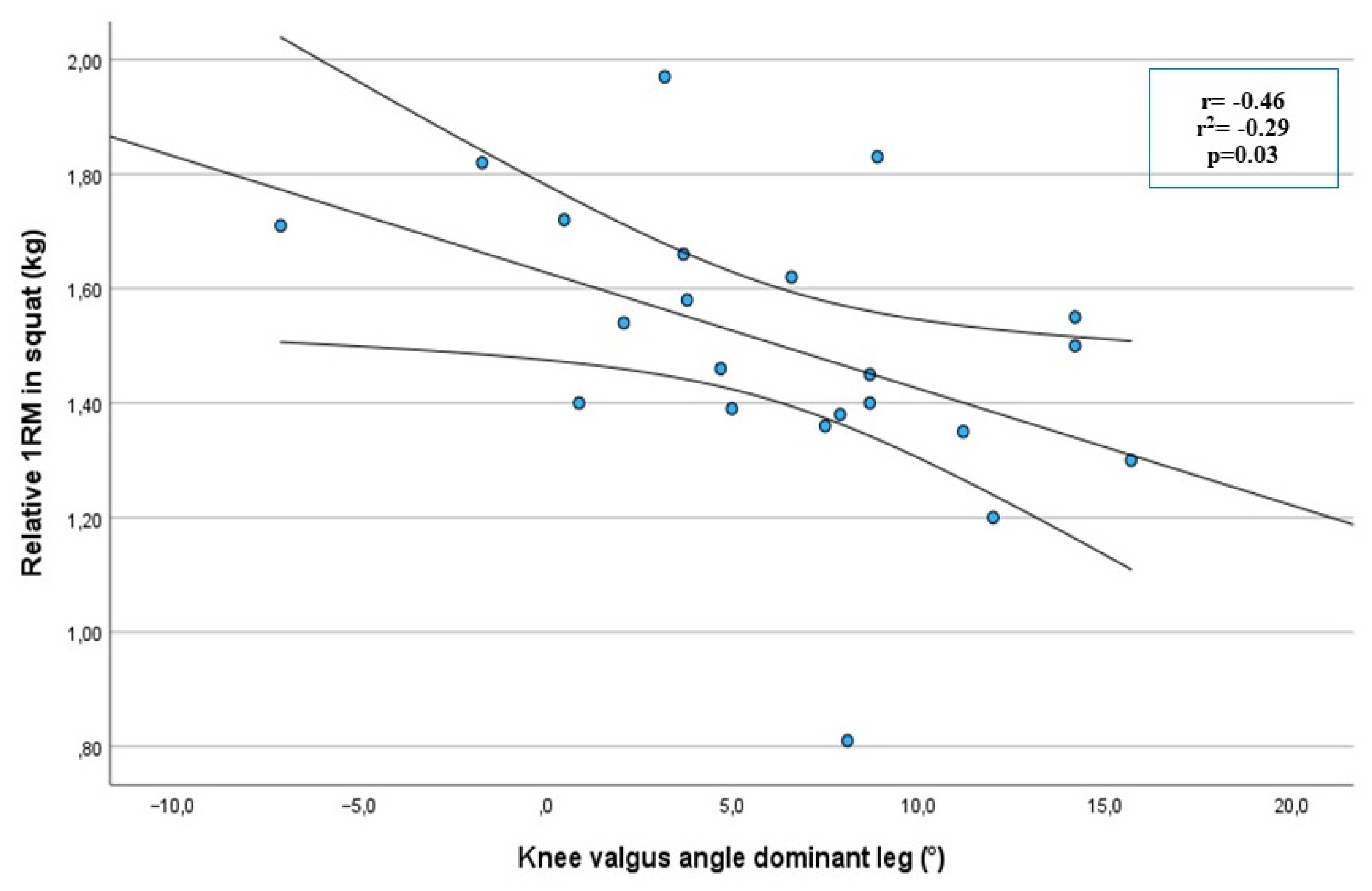
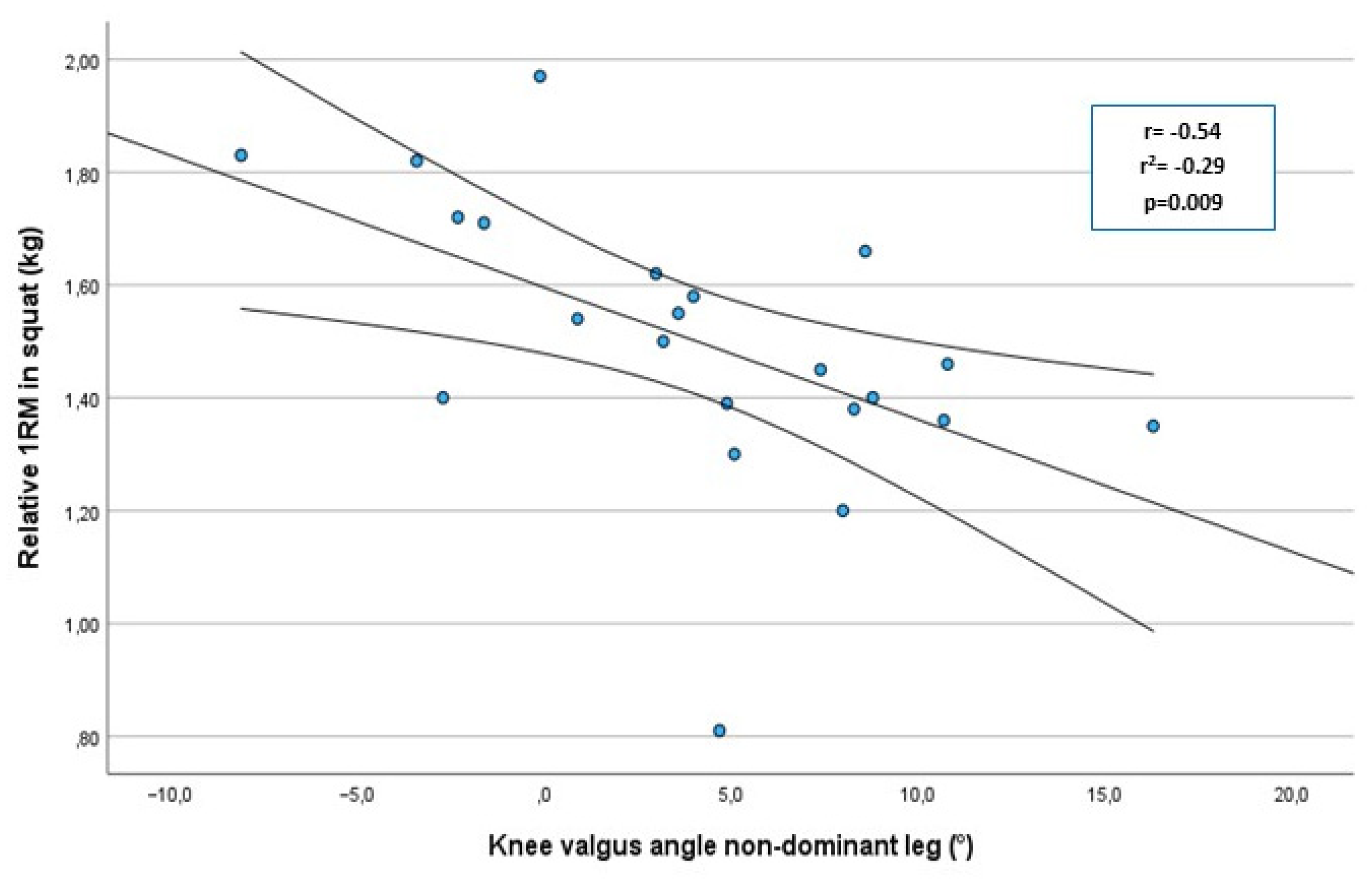
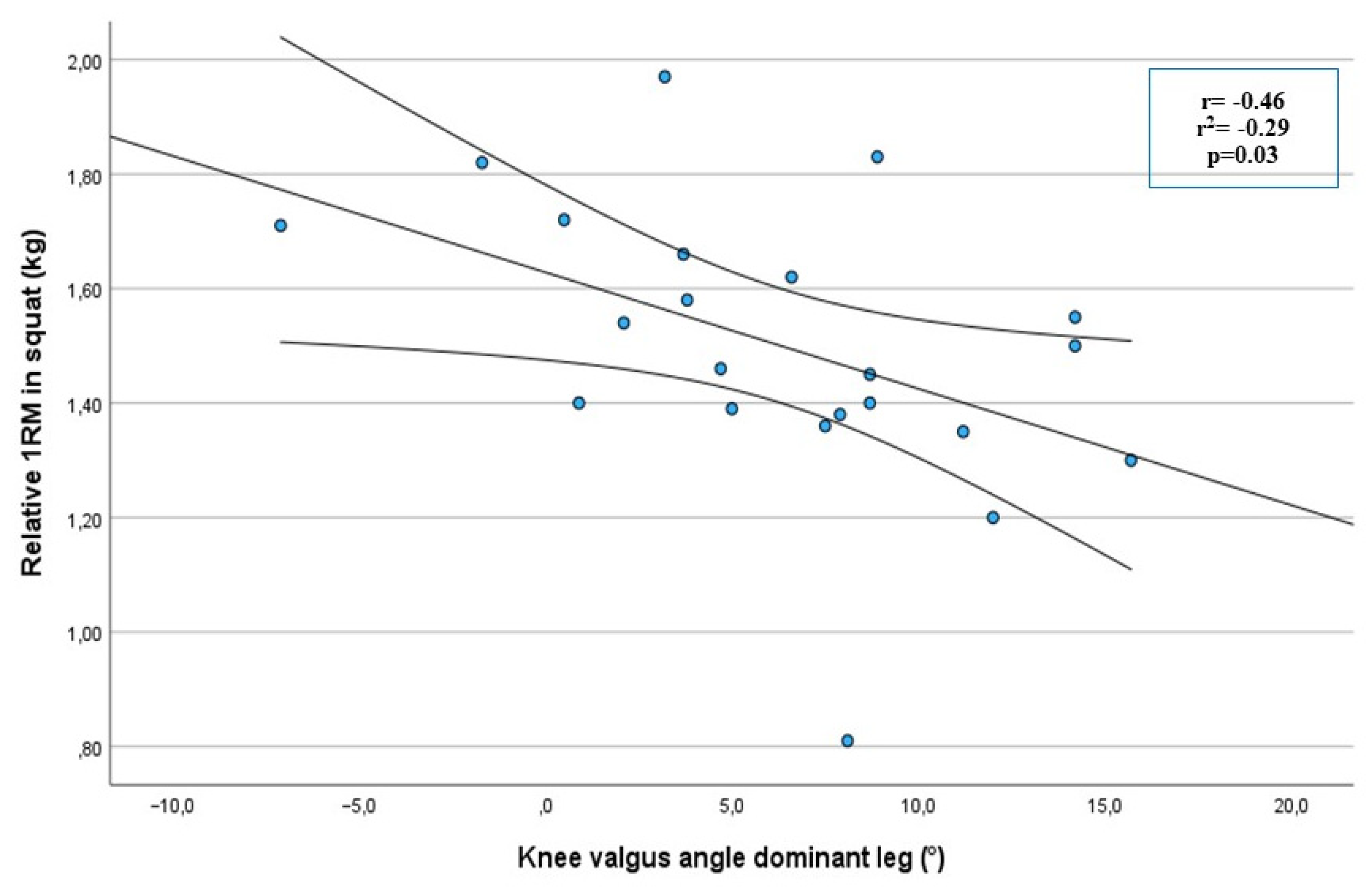
3.1. Correlations and the Influence of Maximal Squat Strength on Dynimic Knee Valgus
3.2. Differences between Men and Women
4. Discussion
4.1. Correlations and the Influence of Maximal Squat Strength on Dynamic Knee Valgus
4.2. Differences between Men and Women
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reckling, C.; Zantop, T.; Petersen, W. Epidemiology of injuries in juvenile handball players. Sport. Sportschaden 2003, 17, 112–117. [Google Scholar] [CrossRef]
- Renstrom, P.; Ljungqvist, A.; Arendt, E.; Beynnon, B.; Fukubayashi, T.; Garrett, W.; Georgoulis, T.; Hewett, T.E.; Johnson, R.; Krosshaug, T.; et al. Non-contact ACL injuries in female athletes: An International Olympic Committee current concepts statement. Br. J. Sports Med. 2008, 42, 394–412. [Google Scholar] [CrossRef] [PubMed]
- Khayambashi, K.; Ghoddosi, N.; Straub, R.K.; Powers, C.M. Hip Muscle Strength Predicts Noncontact Anterior Cruciate Ligament Injury in Male and Female Athletes: A Prospective Study. Am. J. Sports Med. 2016, 44, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Ryman Augustsson, S.; Ageberg, E. Weaker lower extremity muscle strength predicts traumatic knee injury in youth female but not male athletes. BMJ Open Sport Exerc. Med. 2017, 3, e000222. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S., Jr.; Colosimo, A.J.; McLean, S.G.; van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.; Myer, G.D.; Lloyd, R.S. Neuromuscular Risk Factors for Knee and Ankle Ligament Injuries in Male Youth Soccer Players. Sports Med. 2016, 46, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Paterno, M.V.; Quatman, C.E. Mechanisms, prediction, and prevention of ACL injuries: Cut risk with three sharpened and validated tools. J. Orthop. Res. 2016, 34, 1843–1855. [Google Scholar] [CrossRef] [PubMed]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for noncontact anterior cruciate ligament injuries: Knee joint kinematics in 10 injury situations from female team handball and basketball. Am. J. Sports Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef]
- Ageberg, E.; Link, A.; Roos, E.M. Feasibility of neuromuscular training in patients with severe hip or knee OA: The individualized goal-based NEMEX-TJR training program. BMC Musculoskelet. Disord. 2010, 11, 126. [Google Scholar] [CrossRef]
- Kamath, A.F.; Israelite, C.; Horneff, J.; Lotke, P.A. Editorial: What is varus or valgus knee alignment?: A call for a uniform radiographic classification. Clin. Orthop. Relat. Res. 2010, 468, 1702–1704. [Google Scholar] [CrossRef]
- Wilczynski, B.; Zorena, K.; Slezak, D. Dynamic Knee Valgus in Single-Leg Movement Tasks. Potentially Modifiable Factors and Exercise Training Options. A Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 8208. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, L.; Krutsch, V.; Weber, J.; Nerlich, M.; Luig, P.; Loose, O.; Angele, P.; Krutsch, W. Neuromuscular exercises prevent severe knee injury in adolescent team handball players. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1901–1908. [Google Scholar] [CrossRef] [PubMed]
- Myklebust, G.; Engebretsen, L.; Braekken, I.H.; Skjolberg, A.; Olsen, O.E.; Bahr, R. Prevention of anterior cruciate ligament injuries in female team handball players: A prospective intervention study over three seasons. Clin. J. Sport Med. 2003, 13, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Olsen, O.E.; Myklebust, G.; Engebretsen, L.; Holme, I.; Bahr, R. Exercises to prevent lower limb injuries in youth sports: Cluster randomised controlled trial. BMJ 2005, 330, 449. [Google Scholar] [CrossRef] [PubMed]
- Zebis, M.K.; Andersen, L.L.; Brandt, M.; Myklebust, G.; Bencke, J.; Lauridsen, H.B.; Bandholm, T.; Thorborg, K.; Holmich, P.; Aagaard, P. Effects of evidence-based prevention training on neuromuscular and biomechanical risk factors for ACL injury in adolescent female athletes: A randomised controlled trial. Br. J. Sports Med. 2016, 50, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Augustsson, S.R.; Tranberg, R.; Zugner, R.; Augustsson, J. Vertical drop jump landing depth influences knee kinematics in female recreational athletes. Phys. Ther. Sport 2018, 33, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Cashman, G.E. The effect of weak hip abductors or external rotators on knee valgus kinematics in healthy subjects: A systematic review. J. Sport Rehabil. 2012, 21, 273–284. [Google Scholar] [CrossRef]
- Herrington, L.; Munro, A.; Comfort, P. A preliminary study into the effect of jumping-landing training and strength training on frontal plane projection angle. Man. Ther. 2015, 20, 680–685. [Google Scholar] [CrossRef]
- Augustsson, S. Maximum Strength in Squats Determines Jumping Height in Young Female Volleyball Players. Open Sports Sci. J. 2013, 6, 41–46. [Google Scholar] [CrossRef]
- Nuzzo, J.L.; McBride, J.M.; Cormie, P.; McCaulley, G.O. Relationship between countermovement jump performance and multijoint isometric and dynamic tests of strength. J. Strength Cond. Res. 2008, 22, 699–707. [Google Scholar] [CrossRef]
- Wisloff, U.; Castagna, C.; Helgerud, J.; Jones, R.; Hoff, J. Strong correlation of maximal squat strength with sprint performance and vertical jump height in elite soccer players. Br. J. Sports Med. 2004, 38, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.R.; Lambert, M.I.; Hunter, A.M. Muscle activation in the loaded free barbell squat: A brief review. J. Strength Cond. Res. 2012, 26, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Kushner, A.M.; Brent, J.L.; Schoenfeld, B.J.; Hugentobler, J.; Lloyd, R.S.; Vermeil, A.; Chu, D.A.; Harbin, J.; McGill, S.M. The back squat: A proposed assessment of functional deficits and technical factors that limit performance. Strength Cond. J. 2014, 36, 4–27. [Google Scholar] [CrossRef] [PubMed]
- STROBE. STROBE Statement. Available online: http://www.strobe-statement.org/checklists/ (accessed on 1 November 2022).
- Bryanton, M.A.; Carey, J.P.; Kennedy, M.D.; Chiu, L.Z. Quadriceps effort during squat exercise depends on hip extensor muscle strategy. Sports Biomech. 2015, 14, 122–138. [Google Scholar] [CrossRef] [PubMed]
- Ryman Augustsson, S.; Svantesson, U. Reliability of the 1 RM bench press and squat in young women. Eur. J. Physiother. 2013, 15, 118–126. [Google Scholar] [CrossRef]
- McCurdy, K.; Walker, J.; Saxe, J.; Woods, J. The effect of short-term resistance training on hip and knee kinematics during vertical drop jumps. J. Strength Cond. Res. 2012, 26, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- Puig-Divi, A.; Escalona-Marfil, C.; Padulles-Riu, J.M.; Busquets, A.; Padulles-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Cohen, J. Weighted kappa: Nominal scale agreement with provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213–220. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Herrington, L.; Munro, A. Drop jump landing knee valgus angle; normative data in a physically active population. Phys. Ther. Sport 2010, 11, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Nilstad, A.; Krosshaug, T.; Mok, K.M.; Bahr, R.; Andersen, T.E. Association Between Anatomical Characteristics, Knee Laxity, Muscle Strength, and Peak Knee Valgus During Vertical Drop-Jump Landings. J. Orthop. Sports Phys. Ther. 2015, 45, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Fleisig, G.S.; Zheng, N.; Lander, J.E.; Barrentine, S.W.; Andrews, J.R.; Bergemann, B.W.; Moorman, C.T., 3rd. Effects of technique variations on knee biomechanics during the squat and leg press. Med. Sci. Sports Exerc. 2001, 33, 1552–1566. [Google Scholar] [CrossRef] [PubMed]
- Van den Tillaar, R.; Saeterbakken, A.H. Comparison of Core Muscle Activation between a Prone Bridge and 6-RM Back Squats. J. Hum. Kinet. 2018, 62, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Saki, F.; Shafiee, H.; Tahayori, B.; Ramezani, F. The effects of core stabilization exercises on the neuromuscular function of athletes with ACL reconstruction. Sci. Rep. 2023, 13, 2202. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Hinman, R.S.; Wrigley, T.V.; Roos, E.M.; Hodges, P.W.; Staples, M.; Bennell, K.L. The effects of neuromuscular exercise on medial knee joint load post-arthroscopic partial medial meniscectomy: ‘SCOPEX’, a randomised control trial protocol. BMC Musculoskelet. Disord. 2012, 13, 233. [Google Scholar] [CrossRef]
- Herman, K.; Barton, C.; Malliaras, P.; Morrissey, D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: A systematic review. BMC Med. 2012, 10, 75. [Google Scholar] [CrossRef]
- Sale, D.G. Neural adaptation to resistance training. Med. Sci. Sports Exerc. 1988, 20, S135–S145. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Nimphius, S.; Bellon, C.R.; Stone, M.H. The Importance of Muscular Strength: Training Considerations. Sports Med. 2018, 48, 765–785. [Google Scholar] [CrossRef]
- Skarabot, J.; Brownstein, C.G.; Casolo, A.; Del Vecchio, A.; Ansdell, P. The knowns and unknowns of neural adaptations to resistance training. Eur. J. Appl. Physiol. 2021, 121, 675–685. [Google Scholar] [CrossRef]
- Salles, J.I.; Velasques, B.; Cossich, V.; Nicoliche, E.; Ribeiro, P.; Amaral, M.V.; Motta, G. Strength training and shoulder proprioception. J. Athl. Train. 2015, 50, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Radaelli, R.; Botton, C.E.; Wilhelm, E.N.; Bottaro, M.; Lacerda, F.; Gaya, A.; Moraes, K.; Peruzzolo, A.; Brown, L.E.; Pinto, R.S. Low- and high-volume strength training induces similar neuromuscular improvements in muscle quality in elderly women. Exp. Gerontol. 2013, 48, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Kenney, W.; Wilmore, W.; Costill, D. Physiology of Sport and Exercise, 6th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Roberts, B.M.; Nuckols, G.; Krieger, J.W. Sex Differences in Resistance Training: A Systematic Review and Meta-Analysis. J. Strength Cond. Res. 2020, 34, 1448–1460. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.A.; Palmieri, R.M.; Zinder, S.M.; Ingersoll, C.D. Sex differences in valgus knee angle during a single-leg drop jump. J. Athl. Train. 2006, 41, 166–171. [Google Scholar] [PubMed]
- Schmitz, R.J.; Shultz, S.J.; Nguyen, A.D. Dynamic valgus alignment and functional strength in males and females during maturation. J. Athl. Train. 2009, 44, 26–32. [Google Scholar] [CrossRef]
- Crowell, K.R.; Nokes, R.D.; Cosby, N.L. Weak Hip Strength Increases Dynamic Knee Valgus in Single-Leg Tasks of Collegiate Female Athletes. J. Sport Rehabil. 2021, 30, 1220–1223. [Google Scholar] [CrossRef]
- Coratella, G.; Tornatore, G.; Caccavale, F.; Longo, S.; Esposito, F.; Ce, E. The Activation of Gluteal, Thigh, and Lower Back Muscles in Different Squat Variations Performed by Competitive Bodybuilders: Implications for Resistance Training. Int. J. Environ. Res. Public Health 2021, 18, 772. [Google Scholar] [CrossRef]
- Mitani, Y. Gender-related differences in lower limb alignment, range of joint motion, and the incidence of sports injuries in Japanese university athletes. J. Phys. Ther. Sci. 2017, 29, 12–15. [Google Scholar] [CrossRef]
- Banyard, H.G.; Nosaka, K.; Haff, G.G. Reliability and Validity of the Load–Velocity Relationship to Predict the 1RM Back Squat. J. Strength Cond. Res. 2017, 31, 1897–1904. [Google Scholar] [CrossRef]
- Ortiz, A.; Rosario-Canales, M.; Rodriguez, A.; Seda, A.; Figueroa, C.; Venegas-Rios, H.L. Reliability and concurrent validity between two-dimensional and three-dimensional evaluations of knee valgus during drop jumps. Open Access J. Sports Med. 2016, 7, 65–73. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Females (n = 7) | Males (n = 15) | |
|---|---|---|
| Mean (SD) | Mean (SD) | |
| Age (years) | 20 (3) | 25 (5) |
| Weight (kg) | 70 (6) | 91 (12) |
| Height (cm) | 171 (6) | 188 (5) |
| Strong Players (n = 11) | Weak Players (n = 11) | Differences | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |
| Non-dominant leg (°) | 1.6 (4) | 6.7 (4) * | 5.1 (6) * |
| Dominant leg (°) | 4.2 (6) | 8.5 (4) | 3.8 (7) * |
| Females (n = 7) | Males (n = 15) | Differences | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |
| r1RM barbell squat (kg) | 1.29 (0.2) | 1.6 (0.2) | 0.3 (2) * |
| Knee valgus non-dominant leg (°) | 7.3° (4) | 2.5° (5) | 4.8 (7) * |
| Knee valgus dominant leg (°) | 10.7° (3) | 4.2° (5) | 6.5 (8) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augustsson, S.R.; Gannby, E. The Significance of Maximal Squat Strength for Neuromuscular Knee Control in Elite Handball Players: A Cross-Sectional Study. Sports 2023, 11, 236. https://doi.org/10.3390/sports11120236
Augustsson SR, Gannby E. The Significance of Maximal Squat Strength for Neuromuscular Knee Control in Elite Handball Players: A Cross-Sectional Study. Sports. 2023; 11(12):236. https://doi.org/10.3390/sports11120236
Chicago/Turabian StyleAugustsson, Sofia Ryman, and Erik Gannby. 2023. "The Significance of Maximal Squat Strength for Neuromuscular Knee Control in Elite Handball Players: A Cross-Sectional Study" Sports 11, no. 12: 236. https://doi.org/10.3390/sports11120236
APA StyleAugustsson, S. R., & Gannby, E. (2023). The Significance of Maximal Squat Strength for Neuromuscular Knee Control in Elite Handball Players: A Cross-Sectional Study. Sports, 11(12), 236. https://doi.org/10.3390/sports11120236