

Preschool Children with Hearing Loss: Social Communication and Parenting Stress

 , ,
, ,
Abstract
:1. Introduction
1.1. Behavioral Problems
1.2. Delay in Language and Communication Development
1.3. Rationale of the Current Study
2. Materials and Methods
2.1. Assessments
2.1.1. Parenting Stress Index—Short Form (PSI-SF)
2.1.2. Strength and Difficulties Questionnaire (SDQ)
2.1.3. Child Behavior Checklist 1½-5 (CBCL)
2.1.4. Behavior Rating Inventory of Executive Functioning—Preschool Version (BRIEF-P)
2.1.5. Language Use Inventory (LUI)
2.1.6. Children’s Communication Checklist-2 (CCC-2)
2.1.7. Snijders-Oomen NonVerbal Intelligence Test 2½-7 (SON-R)
2.2. Audiological Measures
2.3. Statistical Analysis
3. Results
3.1. Participants
3.2. Confirmatory Factor Analysis and Factor Score Estimation
3.3. Descriptive Statistics for the Main Study Variables
3.4. Correlations with PS
3.5. Partial Effects of Problem Behavior on PS
3.6. Degree of Hearing Loss as Moderator of Problem Behavior Effects
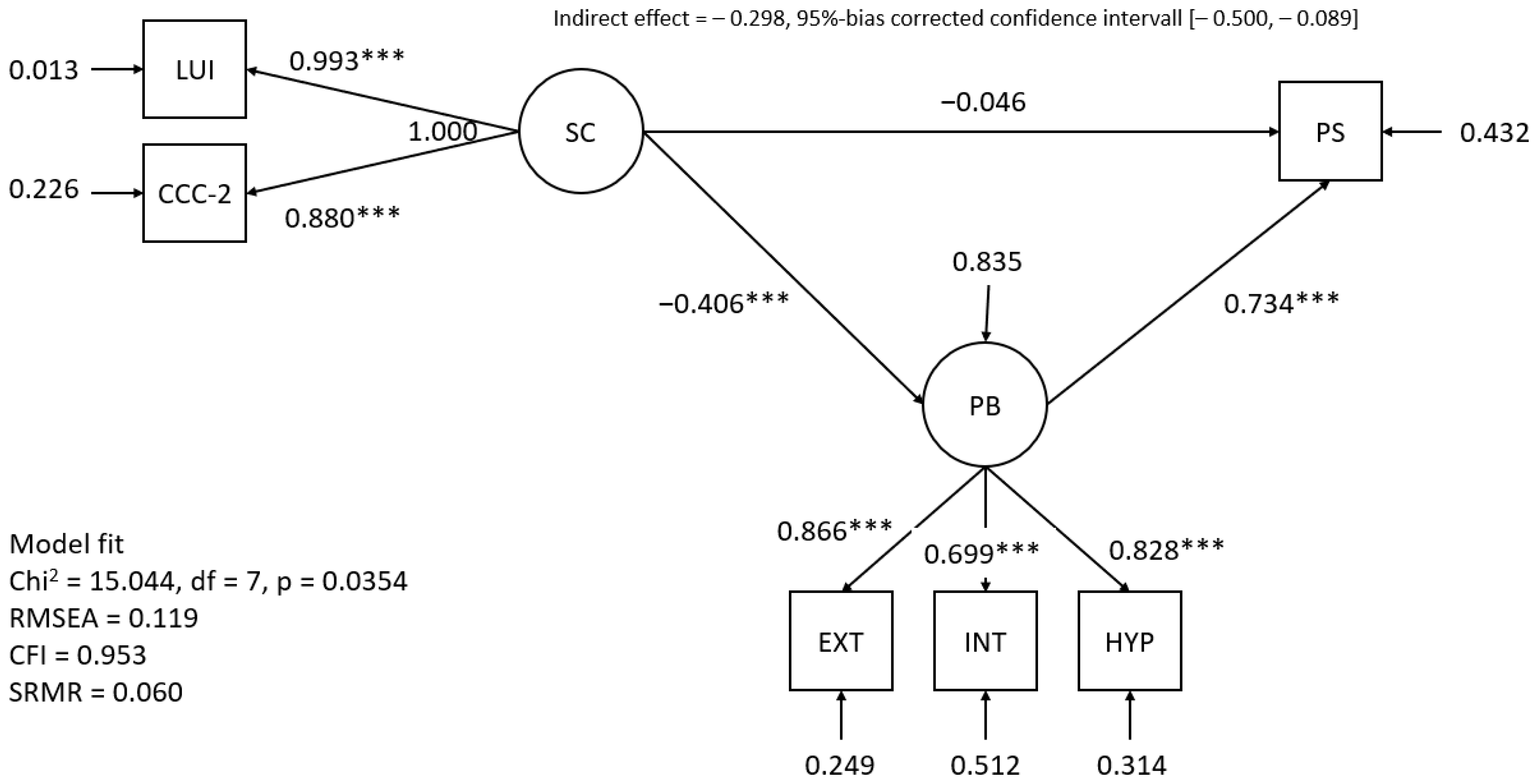
3.7. Problem Behavior as Mediator of Social Communication Effects
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Selye, H. The Stress of Life, Revised ed.; McGraw-Hill: New York, NY, USA, 1984; ISBN 0070562121. [Google Scholar]
- Lazarus, R.S. Stress and Emotion: A New Synthesis; Springer: New York, NY, USA, 2006; ISBN 9780826102614. [Google Scholar]
- Abidin, R.R. Parenting Stress Index (PSI); Pediatric Psychology Press: Charlottesville, VA, USA, 1990. [Google Scholar]
- Quittner, A.L.; Glueckauf, R.L.; Jackson, D.N. Chronic parenting stress: Moderating versus mediating effects of social support. J. Pers. Soc. Psychol. 1990, 59, 1266–1278. [Google Scholar] [CrossRef]
- Blank, A.; Frush Holt, R.; Pisoni, D.B.; Kronenberger, W.G. Associations Between Parenting Stress, Language Comprehension, and Inhibitory Control in Children With Hearing Loss. J. Speech Lang. Hear. Res. 2020, 63, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Topol, D.; Girard, N.; St Pierre, L.; Tucker, R.; Vohr, B. The effects of maternal stress and child language ability on behavioral outcomes of children with congenital hearing loss at 18–24 months. Early Hum. Dev. 2011, 87, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Stika, C.J.; Eisenberg, L.S.; Carter, A.S.; Johnson, K.C.; Hammes Ganguly, D.M.; Henning, S.C.; DesJardin, J.L. Developmental Outcomes in Early-Identified Children Who Are Hard of Hearing at 2 to 3 Years of Age. Ear Hear. 2021, 42, 1238–1252. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, E.M.; Jiawen, W.; Janet, O.; JoAnne, W.; Flora, N.; Isabelle, G.; Andrée, D.-S.; Doug, C. Parent-Reported Stress and Child Behavior for 4-Year-Old Children with Unilateral or Mild Bilateral Hearing Loss. J. Deaf Stud. Deaf Educ. 2022, 27, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Dirks, E.; Uilenburg, N.; Rieffe, C. Parental stress among parents of toddlers with moderate hearing loss. Res. Dev. Disabil. 2016, 55, 27–36. [Google Scholar] [CrossRef]
- Quittner, A.L.; Barker, D.H.; Cruz, I.; Snell, C.; Grimley, M.E.; Botteri, M.; Team, C.I. Parenting Stress Among Parents of Deaf and Hearing Children: Associations with Language Delays and Behavior Problems. Parenting 2010, 10, 136–155. [Google Scholar] [CrossRef]
- Cejas, I.; Mitchell, C.M.; Barker, D.H.; Sarangoulis, C.; Eisenberg, L.S.; Quittner, A.L. Parenting Stress, Self-Efficacy, and Involvement: Effects on Spoken Language Ability Three Years after Cochlear Implantation. Otol. Neurotol. 2021, 42, S11–S18. [Google Scholar] [CrossRef]
- Continisio, G.I.; D’Errico, D.; Toscano, S.; Maldonato, N.M.; de Falco, R.; Nunziata, F.; Rodio, A.; Casarella, A.; Del Vecchio, V.; Fetoni, A.R.; et al. Parenting Stress in Mothers of Children with Permanent Hearing Impairment. Children 2023, 10, 517. [Google Scholar] [CrossRef]
- Gunjawate, D.R.; Ravi, R.; Driscoll, C. Stress among Parents of Children with Hearing Loss and How They Deal with It: A Systematic Review. Int. Arch. Otorhinolaryngol. 2023, 27, e166–e177. [Google Scholar] [CrossRef]
- Barroso, N.E.; Mendez, L.; Graziano, P.A.; Bagner, D.M. Parenting Stress through the Lens of Different Clinical Groups: A Systematic Review & Meta-Analysis. J. Abnorm. Child Psychol. 2018, 46, 449–461. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, J.; Kreppner, J.; Pimperton, H.; Worsfold, S.; Kennedy, C. Emotional and behavioural difficulties in children and adolescents with hearing impairment: A systematic review and meta-analysis. Eur. Child Adolesc. Psychiatry 2015, 24, 477–496. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.Y.C.; Cupples, L.; Leigh, G.; Hou, S.; Wong, A. Predicting Quality of Life and Behavior and Emotion from Functional Auditory and Pragmatic Language Abilities in 9-Year-Old Deaf and Hard-of-Hearing Children. J. Clin. Med. 2021, 10, 5357. [Google Scholar] [CrossRef] [PubMed]
- Sarant, J.; Garrard, P. Parenting stress in parents of children with cochlear implants: Relationships among parent stress, child language, and unilateral versus bilateral implants. J. Deaf Stud. Deaf Educ. 2014, 19, 85–106. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.; Curtin, M.; Botting, N. The interplay between early social interaction, language and executive function development in deaf and hearing infants. Infant Behav. Dev. 2021, 64, 101591. [Google Scholar] [CrossRef] [PubMed]
- Carlson, S.M.; Mandell, D.J.; Williams, L. Executive function and theory of mind: Stability and prediction from ages 2 to 3. Dev. Psychol. 2004, 40, 1105–1122. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.H.; Ensor, R.A. How do families help or hinder the emergence of early executive function? New Dir. Child Adolesc. Dev. 2009, 2009, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.; Atkinson, J.; Marshall, C.; Botting, N.; St Clair, M.C.; Morgan, G. Expressive Vocabulary Predicts Nonverbal Executive Function: A 2-year Longitudinal Study of Deaf and Hearing Children. Child Dev. 2020, 91, e400–e414. [Google Scholar] [CrossRef]
- Austin, G.; Bondü, R.; Elsner, B. Executive Function, Theory of Mind, and Conduct-Problem Symptoms in Middle Childhood. Front. Psychol. 2020, 11, 539. [Google Scholar] [CrossRef]
- Dall, M.; Fellinger, J.; Holzinger, D. The link between social communication and mental health from childhood to young adulthood: A systematic review. Front. Psychiatry 2022, 13, 944815. [Google Scholar] [CrossRef]
- Zaidman-Zait, A.; Most, T. Pragmatics and Peer Relationships Among Deaf, Hard of Hearing, and Hearing Adolescents. Pediatrics 2020, 146, S298–S303. [Google Scholar] [CrossRef] [PubMed]
- Haukedal, C.L.; Wie, O.B.; Schauber, S.K.; Lyxell, B.; Fitzpatrick, E.M.; Koss Torkildsen, J. von. Social communication and quality of life in children using hearing aids. Int. J. Pediatr. Otorhinolaryngol. 2022, 152, 111000. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, D.; Fellinger, J. Conversation difficulties rather than language deficits are linked to emotional problems in school children with hearing loss. Front. Educ. 2022, 7, 944814. [Google Scholar] [CrossRef]
- Dall, M.; Kiblböck, S.; Müllegger, D.; Fellinger, J.; Hofer, J.; Kapplmüller, R.; Breitwieser, S.; Schossleitner, K.; Weber, C.; Zöhrer, R.; et al. Understanding the Impact of Child, Intervention, and Family Factors on Developmental Trajectories of Children with Hearing Loss at Preschool Age: Design of the AChild Study. J. Clin. Med. 2022, 11, 1508. [Google Scholar] [CrossRef] [PubMed]
- Tröster, H. Eltern-Belastungs-Inventar: Deutsche Version des Parenting Stress Index (PSI) von R. R. Abidin, 1st ed.; Hogrefe: Göttingen, Germany, 2010. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child. Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Achenbach, T.M. Child Behavior Checklist 1½-5 Deutsche Fassung: Elternfragebogen für Klein- und Vorschulkinder, 1st ed.; Hogrefe: Göttingen, Germany, 2000. [Google Scholar]
- Daseking, M.; Petermann, F. Verhaltensinventar zur Beurteilung exekutiver Funktionen für das Kindergartenalter: Deutschsprachige Adaptation des Behavior Rating Inventory of Executive Function®—Preschool Version (BRIEF®-P) von Gerard A. Gioia, Kimberly Andrews Espy und Peter K. Isquith; Huber: Göttingen, Germany, 2013. [Google Scholar]
- O’Neill, D. LUI Manual Language Use Inventory: An Assessment of Young Children’s Pragmatic Language Development; Knowledge in Development: Waterloo, ON, Canada, 2009. [Google Scholar]
- Bishop, D. Children’s Communication Checklist-2: CCC-2; Pearson: London, UK, 2006. [Google Scholar]
- Tellegen, P.J.; Laros, J.A.; Petermann, F. SON-R 2½-7 Non-Verbaler Intelligenztest; Hogrefe: Göttingen, Germany, 2007. [Google Scholar]
- World Health Organization. Childhood Hearing Loss: Strategies for Prevention and Care. Available online: https://www.who.int/publications/i/item/childhood-hearing-loss-strategies-for-prevention-and-care (accessed on 24 October 2023).
- Ferrando, P.J.; Lorenzo-Seva, U. Assessing the Quality and Appropriateness of Factor Solutions and Factor Score Estimates in Exploratory Item Factor Analysis. Educ. Psychol. Meas. 2018, 78, 762–780. [Google Scholar] [CrossRef] [PubMed]
- Tonidandel, S.; LeBreton, J.M. Relative Importance Analysis: A Useful Supplement to Regression Analysis. J. Bus. Psychol. 2011, 26, 1–9. [Google Scholar] [CrossRef]
- Preacher, K. A Primer on Interaction Effects in Multiple Linear Regression. Available online: https://www.quantpsy.org/interact/interactions.htm (accessed on 25 December 2023).
- Gonzalez, O.; Valente, M.; Cheong, J.; MacKinnon, D. Mediation/Indirect Effects in Structural Equation Modeling. In Handbook of Structural Equation Modeling; Hoyle, R.H., Ed.; Guilford Press: New York, NY, USA, 2022; pp. 409–426. ISBN 9781462550715. [Google Scholar]
- West, S.; Wei, W.; McNeish, D.; Savord, A. Chapter 10: Model Fit in Structural Equation Modeling. In Handbook of Structural Equation Modeling; Hoyle, R.H., Ed.; Guilford Press: New York, NY, USA, 2022; pp. 184–205. ISBN 9781462550715. [Google Scholar]
- Tonidandel, S.; LeBreton, J.M. RWA Web: A Free, Comprehensive, Web-Based, and User-Friendly Tool for Relative Weight Analyses. J. Bus. Psychol. 2015, 30, 207–216. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. User’s Guide. In Mplus; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The Performance of RMSEA in Models with Small Degrees of Freedom. Sociol. Methods Res. 2015, 44, 486–507. [Google Scholar] [CrossRef]
- Soleimani, R.; Jalali, M.M.; Faghih, H.A. Comparing the prevalence of attention deficit hyperactivity disorder in hearing-impaired children with normal-hearing peers. Arch. Pediatr. 2020, 27, 432–435. [Google Scholar] [CrossRef]
- Daza González, M.T.; Phillips-Silver, J.; López Liria, R.; Gioiosa Maurno, N.; Fernández García, L.; Ruiz-Castañeda, P. Inattention, Impulsivity, and Hyperactivity in Deaf Children Are Not Due to Deficits in Inhibitory Control, but May Reflect an Adaptive Strategy. Front. Psychol. 2021, 12, 629032. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, E.S.; Mangal, L.; Macdonald, K. Referential communication in children with ADHD: Challenges in the role of a listener. J. Speech Lang. Hear. Res. 2013, 56, 590–603. [Google Scholar] [CrossRef] [PubMed]
- Parke, E.M.; Becker, M.L.; Graves, S.J.; Baily, A.R.; Paul, M.G.; Freeman, A.J.; Allen, D.N. Social Cognition in Children With ADHD. J. Atten. Disord. 2021, 25, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, S.; Taylor, L.; Sadiq, H.; Tripp, G. The profile of pragmatic language impairments in children with ADHD: A systematic review. Dev. Psychopathol. 2022, 34, 1938–1960. [Google Scholar] [CrossRef] [PubMed]
- Roos, C.; Cramér-Wolrath, E.; Falkman, K.W. Intersubjective Interaction Between Deaf Parents/Deaf Infants during the Infant’s First 18 Months. J. Deaf Stud. Deaf Educ. 2016, 21, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R. Parent-infant synchrony: A biobehavioral model of mutual influences in the formation of affiliative bonds. Monogr. Soc. Res. Child 2012, 77, 42–51. [Google Scholar] [CrossRef]
- Thoemmes, F.; MacKinnon, D.P.; Reiser, M.R. Power Analysis for Complex Mediational Designs Using Monte Carlo Methods. Struct. Equ. Model. 2010, 17, 510–534. [Google Scholar] [CrossRef]
- Quach, N.E.; Yang, K.; Chen, R.; Tu, J.; Xu, M.; Tu, X.M.; Zhang, X. Post-hoc power analysis: A conceptually valid approach for power based on observed study data. Gen. Psychiatr. 2022, 35, e100764. [Google Scholar] [CrossRef]
- Perugini, M.; Gallucci, M.; Costantini, G. Safeguard Power as a Protection Against Imprecise Power Estimates. Perspect. Psychol. Sci. 2014, 9, 319–332. [Google Scholar] [CrossRef]

{kind=link}
| 36 Months | 66 Months | Total | Min–Max b | |
|---|---|---|---|---|
| Number of children | 40 | 41 | 81 | |
| Age a (months)—m (SD) | 38.13 (2.2) * | 66.3 (5.7) * | 52.4 (14.8) * | 35–73 |
| Sex, male—n (%) | 23 (57.5) | 25 (61.0) | 48 (59.3) | |
| Intellectual functioning, mean (SD) | 103.4 (15.3) * | 96.4 (14.4) * | 99.9 (15.2) | 56–135 |
| Bayley | 103.6 (20.7) | 97.4 (14.5) | 101.5 (18.9) | 65–145 |
| SON | 101.5 (14.5) | 96.7 (14.9) | 98.9 (14.8) | 55–131 |
| Number of siblings—n (%) | ||||
| 0 | 17 (42.5) | 18 (45.0) | 35 (43.8) | |
| 1 | 14(35.0) | 16 (40.0) | 30 (37.5) | |
| 2 | 5 (12.5) | 5 (12.5) | 10 (12.5) | |
| 3 or more | 4 (10.0) | 1 (2.5) | 5 (6.3) | |
| Primary language spoken at home—n (%) | ||||
| German | 29 (72.5) | 33 (80.5) | 62 (76.5) | |
| Bilingual (two or more spoken languages) | 11 (27.5) | 8 (19.5) | 19 (23.5) | |
| Degree of HL bilateral (in the better ear)—n (%) | ||||
| Mild | 6 (15.4) | 6 (15.0) | 12 (15.2) | |
| Moderate | 16 (41.0) | 18 (45.0) | 34 (43.0) | |
| Severe | 0 (0.0) | 5 (12.5) | 5 (6.3) | |
| Profound | 4 (10.3) | 4 (10.0) | 8 (10.1) | |
| Fletcher Index—mean (SD) | 44.7 (26.5) | 53.7 (26.8) | 49.2 (26.9) | 5–115 |
| Laterality—n (%) | ||||
| Bilateral | 26 (66.7) | 33 (80.5) | 59 (73.8) | |
| Unilateral | 13 (33.3) | 8 (19.5) | 21 (26.2) | |
| HA supply | ||||
| CI bilateral | 7 (17.5) | 10 (24.4) | 17 (21.0) | |
| CI unilateral | 1 (2.5) | 0 (0.0) | 1 (1.2) | |
| CI unilateral and HA unilateral | 1 (2.5) | 0 (0.0) | 1 (1.2) | |
| HA aid unilateral | 11 (27.5) | 7 (17.1) | 18 (22.2) | |
| HA bilateral | 20 (50.0) | 24 (58.5) | 44 (54.3) | |
| Age at diagnosis (months)—mean (SD) | 8.7 (10.1) * | 16.0 (17.2) * | 12.2 (14.3) * | 0–73 |
| Age at start of family intervention (months)—mean (SD) | 11.6 (11.8) * | 25.8 (24.1) * | 18.8 (20.2) * | 0–64 |
| Age at amplification of hearing aid (months)—mean (SD) | 11.7 (11.4) * | 26.5 (22.5) * | 18.5 (18.7) * | 0–63 |
| 36 Months | 66 Months | Total | Min–Max a | |
|---|---|---|---|---|
| Externalizing problem behavior | ||||
| Externalizing factor score, mean (SD) | 0.02 (0.91) | −0.02 (0.89) | 0.00 (0.90) | −1.28–3.32 |
| SDQ conduct problems, mean (SD) | 2.5 (2.1) | 2.2 (1.7) | 2.4 (1.9) | 0–10 |
| Borderline n (%) | 5 (13.5) | 4 (10.8) | 9 (12.2) | |
| Abnormal n (%) | 6 (16.2) | 9 (24.3) | 15 (20.3) | |
| CBCL aggressive behavior, raw score, mean (SD) | - | 8.1 (6.8) | 8.1 (6.8) | 0–29 |
| Internalizing problem behavior | ||||
| Internalizing factor score, mean (SD) | −0.14 (0.73) | 0.14 (0.93) | 0.00 (0.84) | −1.12–2.61 |
| SDQ emotional symptoms | 1.1 (1.3) | 1.7 (1.6) | 1.4 (1.5) | 0–6 |
| Borderline n (%) | 0 (0.0) | 1 (2.7) | 1 (1.4) | |
| Abnormal n (%) | 2 (5.4) | 3 (8.1) | 5 (6.8) | |
| CBCL internalizing problems T-score, mean (SD) | - | 49.4 (10.5) | 49.4 (10.5) | 29–72 |
| Hyperactivity | ||||
| Hyperactivity factor score, mean (SD) | −0.09 (0.94) | 0.09 (0.97) | 0.00 (0.95) | −1.50–2.82 |
| SDQ hyperactivity/inattention mean (SD) | 3.1 (2.1) | 3.9 (2.6) | 3.5 (2.4) | 0–10 |
| Borderline n (%) | 1 (2.7) | 1 (2.7) | 2 (2.7) | |
| Abnormal (%) | 2 (5.4) | 7 (18.9) | 9 (12.2) | |
| CBCL attention problems, raw scores, mean (SD) | - | 2.0 (1.9) | 2.0 (1.9) | 0–6 |
| PSI hyperactivity, mean stanine score (SD) | 5.1 (2.0) | 5.3 (1.6) | 5.2 (1.8) | 2–9 |
| BRIEF-P hyperactivity, T-score, mean (SD) | 44.8 (11.2) | 47.6 (10.9) | 46.3 (11.0) | 31–85 |
| Social Communication (pragmatics) | ||||
| LUI total percentile score mean (SD) | 17.9 (21.6) | 0–70 | ||
| CCC-2 total percentile score mean (SD) | 18.9 (21.8) | 0–72 | ||
| Parenting stress | ||||
| PSI Parenting stress, mean T-score | 51.3 (11.9) | 51.6 (10.9) | 51.4 (11.3) | 30–70 |
| Elevated T-score ≥ 60, n (%) | 8 (20.0) | 7 (16.9) | 15 (18.4) | |
| Highly elevated T-score ≥ 70, n (%) | 4 (10.0) | 2 (4.9) | 6 (7.4) |
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) | (15) | (16) | (17) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parental stress | (1) | 1 | ||||||||||||||||
| Externalizing problems | (2) | 0.643 *** | 1 | |||||||||||||||
| Internalizing problems | (3) | 0.582 *** | 0.620 *** | 1 | ||||||||||||||
| Hyperactivity | (4) | 0.606 *** | 0.730 *** | 0.528 *** | 1 | |||||||||||||
| LUI | (5) | −0.443 ** | −0.251 | −0.333 * | −0.498 *** | 1 | ||||||||||||
| CCC-2 | (6) | −0.250 | −0.282 | −0.211 | −0.483 ** | 0.829 * | 1 | |||||||||||
| Age | (7) | −0.007 | −0.011 | 0.173 | 0.116 | −0.189 | 0.054 | 1 | ||||||||||
| Male | (8) | 0.130 | 0.163 | 0.074 | 0.172 | −0.186 | −0.141 | 0.045 | 1 | |||||||||
| IQ | (9) | −0.063 | −0.093 | −0.006 | −0.295 ** | 0.470 ** | 0.482 ** | −0.232 * | −0.221 | 1 | ||||||||
| Number siblings | (10) | −0.105 | −0.087 | −0.098 | −0.016 | −0.007 | −0.258 | −0.103 | 0.087 | −0.076 | 1 | |||||||
| Multilingual | (11) | −0.113 | −0.086 | −0.052 | −0.048 | 0.001 | −0.07 | −0.112 | −0.193 | −0.077 | 0.149 | 1 | ||||||
| Bilateral | (12) | 0.022 | −0.056 | 0.038 | 0.039 | −0.248 | −0.118 | 0.141 | 0.093 | −0.039 | 0.065 | −0.134 | 1 | |||||
| Fletcher index | (13) | 0.021 | −0.103 | −0.008 | −0.064 | −0.164 | −0.089 | 0.101 | −0.017 | −0.038 | −0.345 ** | 0.047 | 0.473 *** | 1 | ||||
| Cochlear implant | (14) | 0.019 | −0.115 | −0.031 | −0.006 | −0.257 | −0.039 | −0.047 | −0.075 | −0.081 | −0.259 | 0.175 | 0.266 | 0.658 *** | 1 | |||
| Hearing aid | (15) | −0.045 | 0.095 | 0.003 | −0.003 | 0.311 | 0.039 | 0.021 | 0.101 | 0.083 | 0.271 | −0.125 | −0.253 | −0.667 *** | −0.966 | 1 | ||
| Age at amplification HA | (16) | 0.003 | 0.033 | 0.088 | 0.062 | −0.394 | −0.206 | 0.441 | −0.016 | −0.16 | 0.159 | −0.033 | 0.157 | −0.143 | −0.25 | 0.25 | 1 | |
| Age at diagnosis | (17) | 0.036 | 0.074 | 0.068 | 0.202 | −0.55 | −0.471 | 0.267 | −0.014 | −0.15 | 0.163 | 0.012 | 0.098 | 0.109 | 0.005 | −0.03 | 0.651 | 1 |
| Age at intervention start | (18) | 0.11 | 0.001 | 0.125 | 0.209 | −0.601 | −0.41 | 0.387 | 0.131 | −0.317 | 0.207 | 0.023 | 0.231 | 0.067 | −0.128 | 0.104 | 0.701 | 0.723 |
| OLS Regression | Relative Weight Analysis | |||||
|---|---|---|---|---|---|---|
| B (SE) | Β | Raw Weights | Relative Weights | |||
| Estimate | 95% Confidence Interval LL | 95% Confidence Interval UL | ||||
| Intercept | 65.345 (1.758) | |||||
| Externalizing problems | 7.197 * (3.153) | 0.295 | 0.179 | 0.097 | 0.281 | 36.11% |
| Internalizing problems | 6.932 * (2.706) | 0.267 | 0.157 | 0.058 | 0.272 | 31.54% |
| Hyperactivity | 5.752 * (2.746) | 0.250 | 0.161 | 0.062 | 0.267 | 32.35% |
| R2 | 0.497 | 100% | ||||
| Predictors | |||||
|---|---|---|---|---|---|
| Externalizing Problems | Internalizing Problems | Hyperactivity | Social Communication (LUI) | Social Communication (CCC-2) | |
| B (SE) | B (SE) | B (SE) | B (SE) | B (SE) | |
| Intercept | 0.000 (0.111) | 0.000 (0.111) | 0.000 (0.111) | 0.000 (0.111) | 0.000 (0.111) |
| Predictor | 0.663 *** (0.077) | 0.584 *** (0.101) | 0.614 (0.084) | −0.399 ** (0.148) | −0.312 * (0.145) |
| Fletcher Index (Degree of Hearing Loss) | 0.048 (0.082) | 0.017 (0.092) | 0.077 (0.106) | −0.025 (0.102) | −0.029 (0.116) |
| Predictor × Fletcher Index | −0.090 (0.092) | −0.037 (0.110) | 0.050 (0.132) | 0.145 (0.144) | 0.010 (0.177) |
| R2 | 0.424 | 0.340 | 0.373 | 0.209 | 0.096 |
| Effects of Social Communication on PS | ||||
|---|---|---|---|---|
| Total Effect | Direct Effect | Indirect Effect | Bc Bootstrap 95% Confidence Interval | |
| Mediators | B (SE) | B (SE) | B (SE) | |
| Externalizing problems | −0.352 ** (0.124) | −0.207 (*) 0.108 | −0.145 * (0.069) | [−0.299, −0.012] |
| Internalizing problems | −0.352 ** (0.122) | −0.221 (0.123) | −0.132 (*) (0.077) | [−0.301, 0.009] |
| Hyperactivity | −0.343 (0.121) | −0.042 (0.128) | −0.301 *** (0.078) | [−0.475, −0.166] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dall, M.; Weber, C.; Holzinger, D.; Binder, D.; Hofer, J.; Horvarth, S.; Müllegger, D.; Rosenthaler, C.; Zöhrer, R.; Fellinger, J. Preschool Children with Hearing Loss: Social Communication and Parenting Stress. J. Pers. Med. 2024, 14, 47. https://doi.org/10.3390/jpm14010047
Dall M, Weber C, Holzinger D, Binder D, Hofer J, Horvarth S, Müllegger D, Rosenthaler C, Zöhrer R, Fellinger J. Preschool Children with Hearing Loss: Social Communication and Parenting Stress. Journal of Personalized Medicine. 2024; 14(1):47. https://doi.org/10.3390/jpm14010047
Chicago/Turabian StyleDall, Magdalena, Christoph Weber, Daniel Holzinger, Doris Binder, Johannes Hofer, Sonja Horvarth, Daiva Müllegger, Christoph Rosenthaler, Ruth Zöhrer, and Johannes Fellinger. 2024. "Preschool Children with Hearing Loss: Social Communication and Parenting Stress" Journal of Personalized Medicine 14, no. 1: 47. https://doi.org/10.3390/jpm14010047
APA StyleDall, M., Weber, C., Holzinger, D., Binder, D., Hofer, J., Horvarth, S., Müllegger, D., Rosenthaler, C., Zöhrer, R., & Fellinger, J. (2024). Preschool Children with Hearing Loss: Social Communication and Parenting Stress. Journal of Personalized Medicine, 14(1), 47. https://doi.org/10.3390/jpm14010047