
Novel Interdisciplinary Enhanced Recovery after Surgery Protocol Implementation in Paediatric Orthopaedics
 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
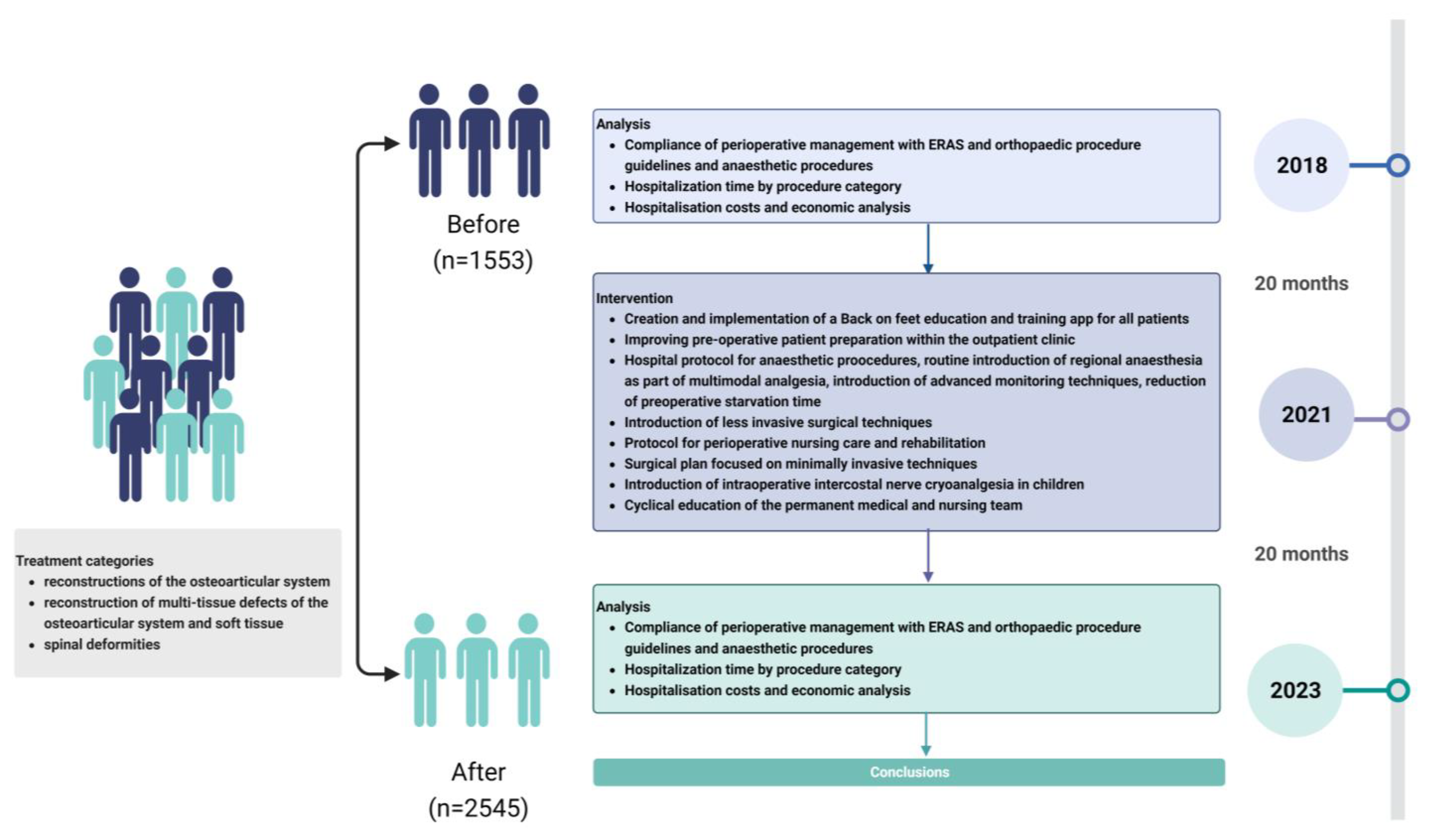
2. Materials and Methods
- Qualification and preparation for surgery and anaesthesia in the Outpatient Clinic,
- Pre-operative preparation of the patient: education via access to the proprietary educational and training app BackOnFeet, prehabilitation (physical activity, diet), and psychological consultation,
- Standardised hospital management of surgical techniques, modes of anaesthesia, options for advanced monitoring, multimodal analgesia and a plan for pain assessment and relief, including novel methods (intraoperative nerve cryoanalgesia),
- Creation of an established interdisciplinary team (orthopaedic surgeons, anaesthetists, physiotherapists, nurses, psychologists, and dieticians) with regular training to implement optimal perioperative care.
- Category 1: reconstructions of the osteoarticular system (osteotomies and long bone lengthening procedures, reconstructions of congenital and acquired bone and joint defects);
- Category 2: multi-tissue reconstructions of osteoarticular and soft tissue defects (pelvic osteotomies with hip reconstruction, multi-tissue reconstructions of peripheral joints);
- Category 3: spinal deformities (scoliosis of various aetiologies);
- Category 4: other procedures.
3. Results
- Lack of prehabilitation;
- No anaesthetic consultation in advance in the Outpatient Clinic area;
- Significantly prolonged preoperative starvation time and excessive fluid restriction (inability to consume carbohydrate-rich beverages before surgery);
- No pre-emptive analgesia;
- Incomplete use of multimodal analgesia;
- Non-routine use of regional analgesia;
- Lack of use of advanced haemodynamic monitoring techniques;
- Long-term use of opioids;
- Delayed start of post-operative rehabilitation due to pain;
- Delayed return to oral feeding.
4. Discussion
4.1. Pre-Operative Period
4.2. Surgery-Anaesthetic Team
4.3. Surgery—Orthopaedic Team
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kehlet, H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Soffin, E.M. Enhanced Recovery After Surgery (ERAS) Protocols in Orthopedic Patients. In Perioperative Care of the Orthopedic Patient, 2nd ed.; MacKenzie, C.R., Cornell, C.N., Memtsoudis, S.G., Eds.; Springer: New York, NY, USA, 2020; pp. 143–150. [Google Scholar]
- Wainwright, T.W.; Gill, M.; Mcdonald, D.A.; Middleton, R.G.; Reed, M.; Sahota, O.; Yates, P.; Ljungqvist, O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop. 2020, 91, 3–19. [Google Scholar] [CrossRef]
- Debono, B.; Wainwright, T.W.; Wang, M.Y.; Sigmundsson, F.G.; Yang, M.M.; Smid-Nanninga, H.; Bonnal, A.; Le Huec, J.C.; Fawcett, W.J.; Ljungqvist, O.; et al. Consensus statement for perioperative care in lumbar spinal fusion: Enhanced Recovery After Surgery (ERAS) Society recommendations. Spine J. 2021, 21, 729–752. [Google Scholar] [CrossRef] [PubMed]
- Feldheiser, A.; Aziz, O.; Baldini, G.; Cox, B.P.; Fearon, K.C.; Feldman, L.S.; Gan, T.J.; Kennedy, R.H.; Ljungqvist, O.; Lobo, D.N.; et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, part 2: Consensus statement for anaesthesia pratice. Acta Anaesthesiol. Scand. 2016, 60, 289–334. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.C.; He, L.J.; Chen, D.; Li, X.B.; Feng, Z.H.; Fu, C.W.; Xuan, J.W.; Ni, W.F.; Wu, A.M. An enhanced recovery after surgery programme in orthopaedic surgery: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2019, 14, 77. [Google Scholar] [CrossRef]
- Dąbrowski, M.; Kubaszewski, Ł. Enhanced recovery after surgery—Possibility of implementation in the department of orthopedics and spine surgery in Poland. Chir. Narzadow Ruchu Ortop. Pol. 2020, 85, 121–125. [Google Scholar] [CrossRef]
- Li, J.; Rai, S.; Ze, R.; Tang, X.; Liu, R.; Hong, P. Enhanced recovery care versus traditional non-ERAS care following osteotomies in developmental dysplasia of the hip in children: A retrospective case-cohort study. BMC Musculoskelet. Disord. 2020, 21, 234. [Google Scholar] [CrossRef]
- Garin, C. Enhanced recovery after surgery in pediatric orthopedics (ERAS-PO). Orthop. Traumatol. Surg. Res. 2020, 106, 101–107. [Google Scholar] [CrossRef]
- Koucheki, R.; Koyle, M.; Ibrahim, G.M.; Nallet, J.; Lebel, D.E. Comparison of interventions and outcomes of enhanced recovery after surgery: A systematic review and meta-analysis of 2456 adolescent idiopathic scoliosis cases. Eur. Spine J. 2021, 30, 3457–3472. [Google Scholar] [CrossRef]
- Rao, K.E.; Krodel, D.; Toaz, E.E.; Fanelli, J.; Hajduk, J.; Kato, K.; Rychlik, K.; King, E.; Sarwark, J.; Grayhack, J.; et al. Introduction of an enhanced recovery pathway results in decreased length of stay in patients with adolescent idiopathic scoliosis undergoing posterior spinal fusion: A description of implementation strategies and retrospective before-and-after study of outcomes. J. Clin. Anesth. 2021, 75, 110493. [Google Scholar] [CrossRef]
- Julien-Marsollier, F.; Michelet, D.; Assaker, R.; Doval, A.; Louisy, S.; Madre, C.; Simon, A.L.; Ilharreborde, B.; Brasher, C.; Dahmani, S. Enhanced recovery after surgical correction of adolescent idiopathic scoliosis. Paediatr. Anaesth. 2020, 30, 1068–1076. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Huang, X.; Gao, X.N.; Xia, B.; Gao, J.B.; Wang, C.; Zhu, X.L.; Shi, X.J.; Tao, H.R.; Luo, Z.J.; et al. An Optimized Enhanced Recovery After Surgery (ERAS) Pathway Improved Patient Care in Adolescent Idiopathic Scoliosis Surgery: A Retrospective Cohort Study. World Neurosurg. 2021, 145, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, N.D.; Murphy, J.S.; Austin, T.M.; Bruce, R.W., Jr.; Harris, H.; Bush, P.; Yu, A.; Kusumoto, H.; Schmitz, M.L.; Devito, D.P.; et al. Short term outcomes of an enhanced recovery after surgery (ERAS) pathway versus a traditional discharge pathway after posterior spinal fusion for adolescent idiopathic scoliosis. Spine Deform. 2021, 9, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Gadiya, A.D.; Koch, J.; Patel, M.; Shafafy, M.S.; Grevitt, M.; Quraishi, N. Enhanced recovery after surgery (ERAS) in adolescent idiopathic scoliosis (AIS): A meta-analysis -and systematic review. Spine Deform. 2021, 9, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Zacha, S.; Andrzejewska, A.; Jastrzębska-Ligocka, B.; Szwed, A.; Modrzejewska, E.; Zacha, W.; Skonieczna-Żydecka, K.; Miegoń, J.; Jarosz, K.; Biernawska, J. Intercostal nerve cryoanalgesia in the treatment of pain in patients operated on by the modified Nuss method with the BackOnFeet application-a new strategy to improve outcomes. Front. Pediatr. 2023, 10, 1069805. [Google Scholar] [CrossRef] [PubMed]
- Frykholm, P.; Disma, N.; Andersson, H.; Beck, C.; Bouvet, L.; Cercueil, E.; Hofman, J.; Isserman, R.; Klaucane, A.; Kuhn, F.; et al. Pre-operative fasting in children. A guideline from the European Society of Anaesthesiology and Intensive Care. Eur. J. Anaesthesiol. 2022, 39, 4–25. [Google Scholar] [CrossRef]
- Tong, J.; Gan, T.J.; Kumar, G.; Belani, K.G.; Sergio Bergese, S.; Chung, F.; Diemunsch, P.; Habib, A.S.; Jin, Z.; Kovac, A.L.; et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth. Analg. 2020, 131, 411–448. [Google Scholar] [CrossRef]
- Cettler, M.; Zielińska, M.; Rosada-Kurasińska, J.; Kubica-Cielińska, A.; Jarosz, K.; Bartkowska-Śniatkowska, A. Guidelines for treatment of acute pain in children—The consensus statement of the Section of Paediatric Anaesthesiology and Intensive Therapy of the Polish Society of Anaesthesiology and Intensive Therapy. Anaesthesiol. Intensive Ther. 2022, 54, 197–218. [Google Scholar] [CrossRef]
- Halvorsen, S.; Mehilli, J.; Cassese, S.; Hall, T.S.; Abdelhamid, M.; Barbato, E.; De Hert, S.; de Laval, I.; Geisler, T. 2022 ESC Guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery: Developed by the task force for cardiovascular assessment and management of patients undergoing non-cardiac surgery of the European Society of Cardiology (ESC) Endorsed by the European Society of Anaesthesiology and Intensive Care (ESAIC). Eur. Heart J. 2022, 43, 3826–3924. [Google Scholar] [CrossRef]
- Elsarrag, M.; Soldozy, S.; Patel, P.; Norat, P.; Sokolowski, J.D.; Park, M.S.; Tvrdik, P.; Kalani, M.Y. Enhanced recovery after spine surgery: A systematic review. Neurosurg. Focus 2019, 46, E3. [Google Scholar] [CrossRef]
- Jeandel, C.; Ikonomoff, T.; Bertoncelli, C.M.; Cunsolo, L.L.; Luna, M.V.; Monticone, M.; Clement, J.L.; Rampal, V.; Solla, F. Enhanced recovery following posterior spinal fusion for adolescent idiopathic scoliosis: A medical and economic study in a French private nonprofit pediatric hospital. Orthop. Traumatol. Surg. Res. 2023, 2023, 103626. [Google Scholar] [CrossRef] [PubMed]
- Voepel-Lewis, T.; Caird, M.S.; Tait, A.R.; Farley, F.A.; Li, Y.; Malviya, S.; Hassett, A.; Weber, M.; Currier, E.; de Sibour, T.; et al. A cluster of high psychological and somatic symptoms in children with idiopathic scoliosis predicts persistent pain and analgesic use 1 year after spine fusion. Paediatr. Anaesth. 2018, 28, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Perry, M.; Starkweather, A.; Baumbauer, K.; Young, E. Factors Leading to Persistent Postsurgical Pain in Adolescents Undergoing Spinal Fusion: An Integrative Literature Review. J. Pediatr. Nurs. 2018, 8, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Lambrechts, M.J.; Boeyer, M.E.; Tweedy, N.M.; Gupta, S.K.; Kimchi, E.T.; Hoernschemeyer, D.G. Team Integrated Enhanced Recovery (TIGER) Protocol after Adolescent Idiopathic Scoliosis Correction Lowers Direct Cost and Length of Stay While Increasing Daily Contribution Margins. Mol. Med. 2022, 119, 152–157. [Google Scholar]
- Lee, C.S.; Merchant, S.; Chidambaran, V. Postoperative Pain Management in Pediatric Spinal Fusion Surgery for Idiopathic Scoliosis. Paediatr. Drugs 2020, 22, 575–601. [Google Scholar] [CrossRef]
- Han, M.; Lee, E. Effectiveness of Mobile Health Application Use to Improve Health Behavior Changes: A Systematic Review of Randomized Controlled Trials. Healthc. Inform. Res. 2018, 24, 207–226. [Google Scholar] [CrossRef]
- Teles, A.R.; Ocay, D.D.; Bin Shebreen, A.; Tice, A.; Saran, N.; Ouellet, J.A.; Ferland, C.E. Evidence of impaired pain modulation in adolescents with idiopathic scoliosis and chronic back pain. Spine J. 2019, 19, 677–686. [Google Scholar] [CrossRef]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and Strategies in Guideline Implementation—A Scoping Review. Healthcare 2016, 4, 36. [Google Scholar] [CrossRef]
- Badge, H.M.; Churches, T.; Naylor, J.M.; Xuan, W.; Armstrong, E.; Gray, L.; Fletcher, J.; Gosbell, I.; Lin, C.; Harris, I.A. Non-compliance with clinical guidelines increases the risk of complications after primary total hip and knee joint replacement surgery. PLoS ONE 2021, 16, e0260146. [Google Scholar] [CrossRef]
- Song, S.H.; Moon, D.H.; Shim, Y.H.; Jung, H.; Lee, S. Limited cryoablation reduces hospital stay and opioid consumption compared to thoracic epidural analgesia after minimally invasive repair of pectus excavatum. Medicine 2022, 101, e29773. [Google Scholar] [CrossRef]
- Hallet, J.; Sutradhar, R.; Jerath, A.; d’Empaire, P.P.; Carrier, F.M.; Turgeon, A.F.; McIsaac, D.I.; Idestrup, C.; Lorello, G.; Flexman, A.; et al. Association Between Familiarity of the Surgeon-Anesthesiologist Dyad and Postoperative Patient Outcomes for Complex Gastrointestinal Cancer Surgery. JAMA Surg. 2023, 158, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Loganathan, A.K.; Joselyn, A.S.; Babu, M.; Jehangir, S. Implementation and outcomes of enhanced recovery protocols in pediatric surgery: A systematic review and meta-analysis. Pediatr. Surg. Int. 2022, 38, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Elias, K.; Stone, A.; McGinigle, K.; Tankou, J.; Scott, M.; Fawcett, W.; Demartines, N.; Lobo, D.; Ljungqvist, O.; Urman, R. The Reporting on ERAS Compliance, Outcomes, and Elements Research (RECOvER) Checklist: A Joint Statement by the ERAS and ERAS USA Societies. World J. Surg. 2019, 43, 1–8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ERAS | Our Project |
|---|---|
| PATIENT before surgery | |
|
|
| Before surgery TEAM | |
|
|
| ANAESTHETIST during surgery | |
|
|
| ORTHOPAEDIC during surgery | |
|
|
| After surgery TEAM | |
|
|
| BEFORE Group (n = 1553) | AFTER Group (n = 2545) | p | |
|---|---|---|---|
| Age groups n (%) | |||
| <1 year old | 23 (2) | 22 (1) | <0.001 |
| 1–6 | 193 (12) | 223 (9) | |
| 7–18 | 1337 (86) | 2300 (90) | |
| Gender n (%) | |||
| Girls | 610 (39) | 1052 (41) | 0.19 |
| Boys | 943 (61) | 1493 (59) | |
| Category n (%) | |||
| Category 1 | 261 (17) | 881 (34) | 0.005 |
| Category 2 | 44 (3) | 198 (8) | |
| Category 3 | 7 (<1) | 73 (3) | |
| Category 4 | 1241 (79) | 1393 (55) | |
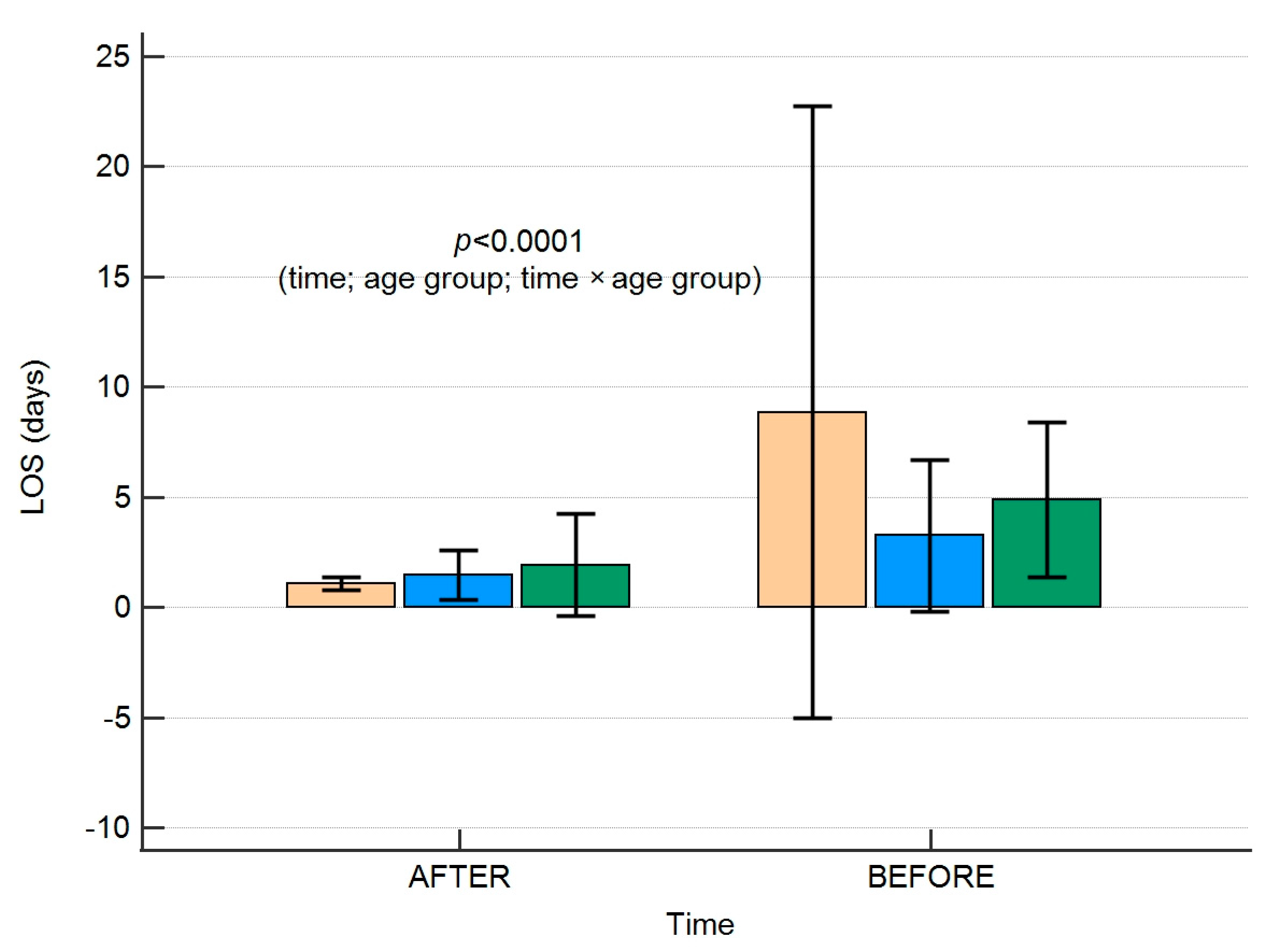
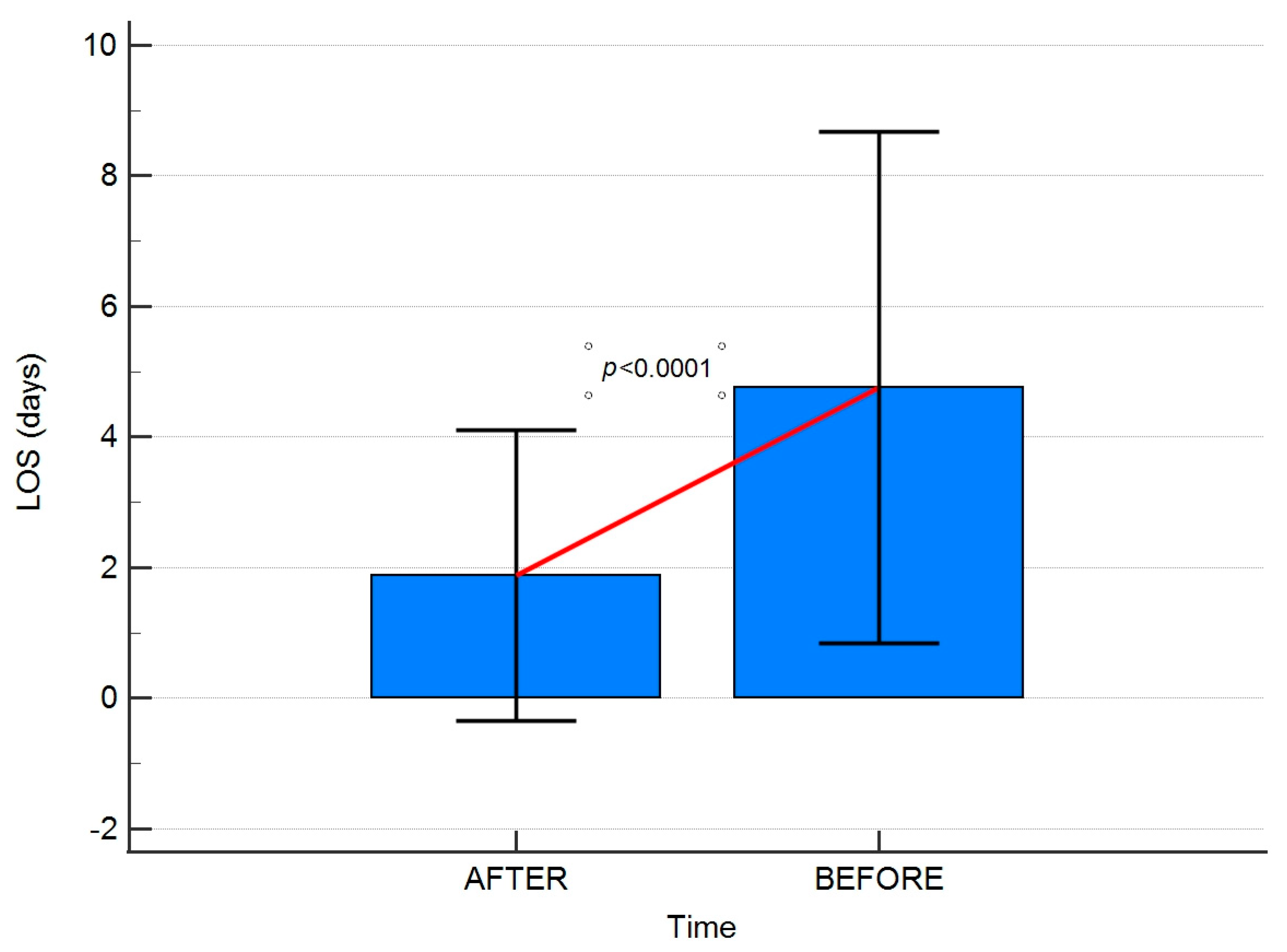
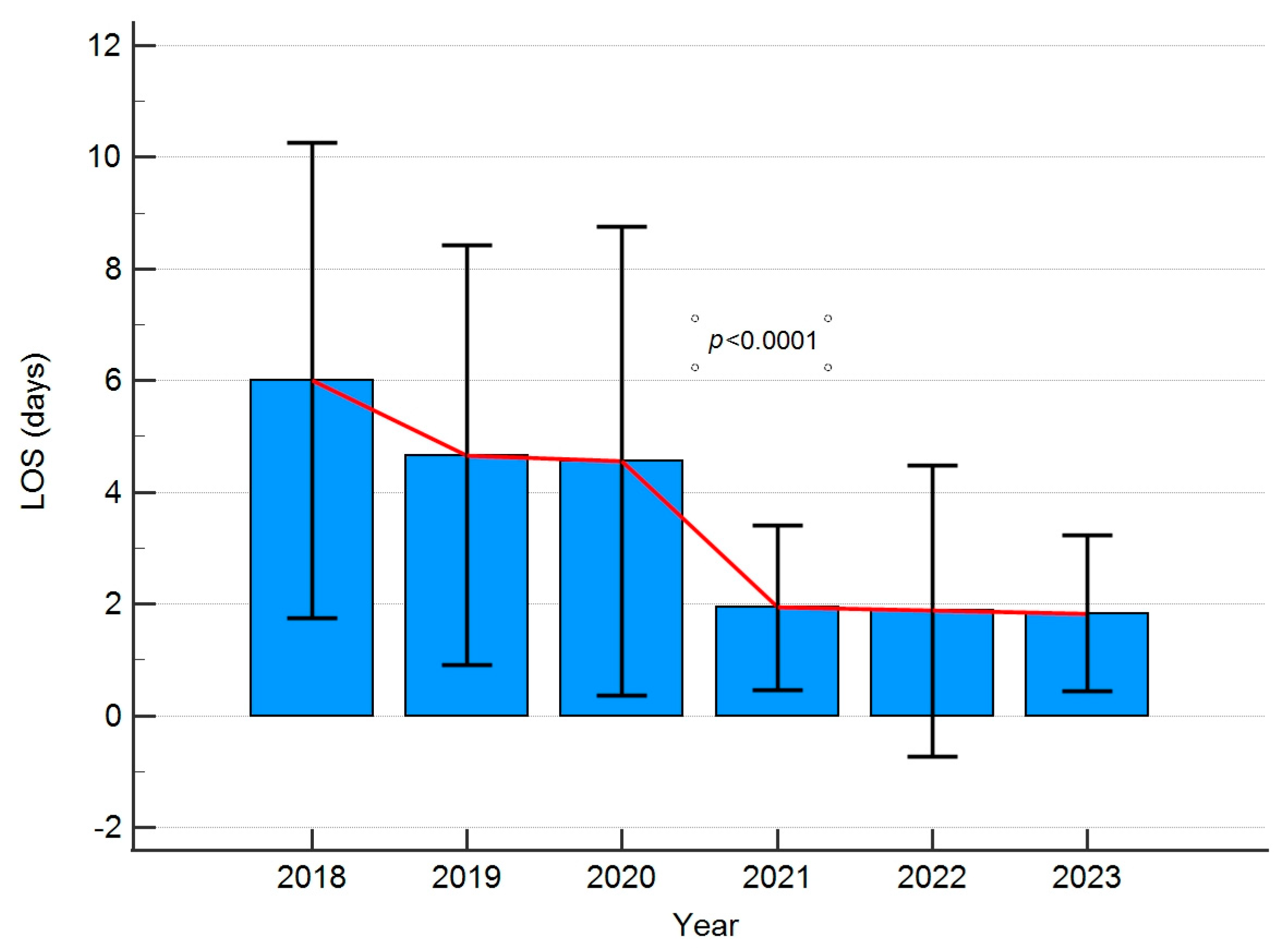
| Duration of hospitalisation (days, mean ± SD) | |||
| Whole group (n = 4098) | 4.76 ± 3.92 | 1.88 ± 2.22 | <0.001 |
| Category 1 (n = 1142) | 6.09 ± 3.60 | 1.81 ± 0.73 | <0.001 |
| Category 2 (n = 242) | 6.88 ± 2.30 | 2.25 ± 1.09 | |
| Category 3 (n = 80) | 16.86 ± 7.14 | 7.14 ± 9.84 | |
| Year | 2018 | 2019 | 2020 | 2021 | 2022 |
|---|---|---|---|---|---|
| Cost/revenue | 85.02% | 81.09% | 84.83% | 67.97% | 71.15% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zacha, S.; Szwed, A.; Miegoń, J.; Skonieczna-Żydecka, K.; Andrzejewska, A.; Modrzejewska, E.; Horecki, M.; Jarosz, K.; Biernawska, J. Novel Interdisciplinary Enhanced Recovery after Surgery Protocol Implementation in Paediatric Orthopaedics. J. Pers. Med. 2023, 13, 1417. https://doi.org/10.3390/jpm13091417
Zacha S, Szwed A, Miegoń J, Skonieczna-Żydecka K, Andrzejewska A, Modrzejewska E, Horecki M, Jarosz K, Biernawska J. Novel Interdisciplinary Enhanced Recovery after Surgery Protocol Implementation in Paediatric Orthopaedics. Journal of Personalized Medicine. 2023; 13(9):1417. https://doi.org/10.3390/jpm13091417
Chicago/Turabian StyleZacha, Sławomir, Aleksander Szwed, Jakub Miegoń, Karolina Skonieczna-Żydecka, Agata Andrzejewska, Elżbieta Modrzejewska, Marcin Horecki, Konrad Jarosz, and Jowita Biernawska. 2023. "Novel Interdisciplinary Enhanced Recovery after Surgery Protocol Implementation in Paediatric Orthopaedics" Journal of Personalized Medicine 13, no. 9: 1417. https://doi.org/10.3390/jpm13091417
APA StyleZacha, S., Szwed, A., Miegoń, J., Skonieczna-Żydecka, K., Andrzejewska, A., Modrzejewska, E., Horecki, M., Jarosz, K., & Biernawska, J. (2023). Novel Interdisciplinary Enhanced Recovery after Surgery Protocol Implementation in Paediatric Orthopaedics. Journal of Personalized Medicine, 13(9), 1417. https://doi.org/10.3390/jpm13091417