
Clinical Efficacy Analysis of the Personalization of Prosthetic Abutments in Implant Supported Restorations in Comparison to Available Standard Titanium Abutments

 ,
,  , ,
, , 
Abstract
:1. Introduction
- (a)
- Prosthetic solutions used with standard and customized abutments divided by type of materials;
- (b)
- Incidence of complications;
- (c)
- The evolution of dental implants in immediate loading vs. delayed loading scenarios.
2. Materials and Methods
3. Results
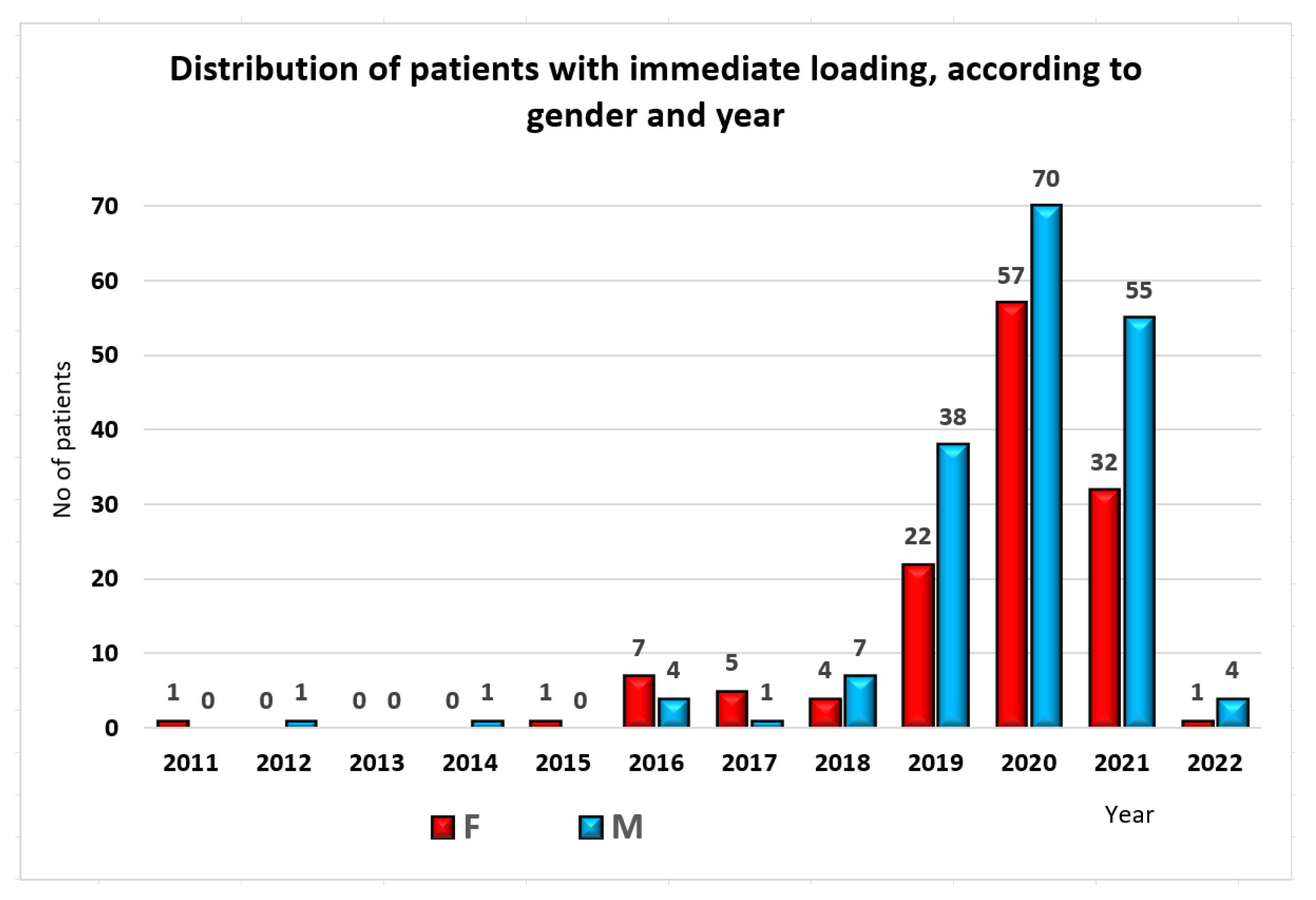
3.1. Immediate/Delayed Loading
3.2. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Linkevicius, T.; Vaitelis, J. The effect of zirconia or titanium as abutment material on soft peri-implant tissues: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2015, 26, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T. Zero Bone Loss Concepts; Quintessence Publishing Co, Inc.: Batavia, IL, USA, 2019. [Google Scholar]
- Dumbrigue, H.B.; Abanomi, A.A.; Cheng, L.L. Techniques to minimize excess luting agent in cement-retained implant restorations. J. Prosthet. Dent. 2002, 87, 112–114. [Google Scholar] [CrossRef]
- Tarnow, D.P.; Chu, S.J. The Single-Tooth Implant: A Minimally Invasive Approach for Anterior and Posterior Extraction Sockets; Quintessence Publishing Co, Inc.: Batavia, IL, USA, 2020. [Google Scholar]
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodontics Restor. Dent. 2006, 26, 9–17. [Google Scholar]
- Canullo, L.; Fedele, G.R.; Iannello, G.; Jepsen, S. Platform switching and marginal bone-level alterations: The results of a randomized-controlled trial. Clin. Oral Implant. Res. 2010, 21, 115–121. [Google Scholar] [CrossRef]
- Reda, R.; Zanza, A.; Cicconetti, A.; Bhandi, S.; Guarnieri, R.; Testarelli, L.; Di Nardo, D. A Systematic Review of Cementation Techniques to Minimize Cement Excess in Cement-Retained Implant Restorations. Methods Protoc. 2022, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Reda, R.; Zanza, A.; Bellanova, V.; Patil, S.; Bhandi, S.; Di Nardo, D.; Testarelli, L. Zinc Oxide Non-Eugenol Cement versus Resinous Cement on Single Implant Restoration: A Split-Mouth Study. J. Compos. Sci. 2023, 7, 128. [Google Scholar] [CrossRef]
- Misch, C.E. Dental Implant Prosthetics, 2nd ed.; Elsevier Mosby: St. Louis, MO, USA, 2015. [Google Scholar]
- Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95/46/EC (General Data Protection Regulation) (Text with EEA Relevance). Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016R0679 (accessed on 15 July 2023).
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Doyle, D.J.; Hendrix, J.M.; Garmon, E.H. American Society of Anesthesiologists Classification; Updated 4 December 2022; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441940/ (accessed on 15 July 2023).
- Târtea, D.A.; Ionescu, M.; Manolea, H.O.; Mercuț, V.; Obădan, E.; Amărăscu, M.O.; Mărășescu, P.C.; Dăguci, L.; Popescu, S.M. Comparative Study of Dental Custom CAD-CAM Implant Abutments and Dental Implant Stock Abutments. J. Clin. Med. 2023, 12, 2128. [Google Scholar] [CrossRef]
- Lindhe, J.; Lang, N.P.; Berglundh, T.; Giannobile, W.V.; Sanz, M. Lindhe’s Clinical Periodontology and Implant Dentistry; Wiley-Blackwell: Chichester, UK, 2021. [Google Scholar]
- Furuhashi, A.; Ayukawa, Y.; Atsuta, I.; Rakhmatia, Y.D.; Koyano, K. Soft Tissue Interface with Various Kinds of Implant Abutment Materials. J. Clin. Med. 2021, 10, 2386. [Google Scholar] [CrossRef]
- Barberi, J.; Spriano, S. Titanium and Protein Adsorption: An Overview of Mechanisms and Effects of Surface Features. Materials 2021, 14, 1590. [Google Scholar] [CrossRef]
- Marchack, C.B. A custom titanium abutment for the anterior single-tooth implant. J. Prosthet. Dent. 1996, 76, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Sailer, I.; Hämmerle, C.H.; Attin, T.; Schmidlin, P. In vitro color changes of soft tissues caused by restorative materials. Int. J. Periodontics Restor. Dent. 2007, 27, 251–257. [Google Scholar]
- Jung, R.E.; Pjetursson, B.E.; Glauser, R.; Zembic, A.; Zwahlen, M.; Lang, N.P. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin. Oral. Implant. Res. 2008, 19, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, N.D.; Senna, P.M.; Gomes, R.S.; Del Bel Cury, A.A. Influence of luting space of zirconia abutment on marginal discrepancy and tensile strength after dynamic loading. J. Prosthet. Dent. 2021, 125, 683.e1–683.e8. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, P.; Johannson, D.; Fischer, C.; Stawarczyk, B.; Beuer, F. In vitro fatigue and fracture resistance of one- and two-piece CAD/CAM zirconia implant abutments. Int. J. Oral. Maxillofac. Implant. 2015, 30, 546–554. [Google Scholar] [CrossRef]
- Nothdurft, F.P. All-Ceramic Zirconium Dioxide Implant Abutments for Single-Tooth Replacement in the Posterior Region: A 5-Year Outcome Report. Int. J. Prosthodont. 2019, 32, 177–181. [Google Scholar] [CrossRef]
- Nguyen, H.Q.; Tan, K.B.; Nicholls, J.I. Load fatigue performance of implant-ceramic abutment combinations. Int. J. Oral. Maxillofac. Implant. 2009, 24, 636–646. [Google Scholar]
- Klotz, M.W.; Taylor, T.D.; Goldberg, A.J. Wear at the titanium-zirconia implant-abutment interface: A pilot study. Int. J. Oral. Maxillofac. Implant. 2011, 26, 970–975. [Google Scholar]
- Gehrke, S.A.; Poncio da Silva, P.M.; Calvo Guirado, J.L. Mechanical behavior of zirconia and titanium abutments before and after cyclic load application. J. Prosthet. Dent. 2016, 116, 529–535. [Google Scholar] [CrossRef]
- Linkevicius, T.; Puisys, A.; Linkevicius, R.; Alkimavicius, J.; Gineviciute, E.; Linkeviciene, L. The influence of submerged healing abutment or subcrestal implant placement on soft tissue thickness and crestal bone stability. A 2-year randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2020, 22, 497–506. [Google Scholar] [CrossRef]
- de Camargos, G.V.; Sotto-Maior, B.S.; da Silva, W.J.; Lazari, P.C.; Del Bel Cury, A.A. Prosthetic abutment influences bone biomechanical behavior of immediately loaded implants. Braz. Oral. Res. 2016, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Almeida, P.J.; Silva, C.L.; Alves, J.L.; Silva, F.S.; Martins, R.C.; Sampaio Fernandes, J. Comparative analysis of the wear of titanium/titanium and titanium/zirconia interfaces in implant/abutment assemblies after thermocycling and mechanical loading. Rev. Port. Estomatol. Med. Dent. Cir. Maxilofac. 2016, 57, 207–214. [Google Scholar] [CrossRef]
- Murakami, N.; Wakabayashi, N. Finite element contact analysis as a critical technique in dental biomechanics: A review. J. Prosthodont. Res. 2014, 58, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.Y.; Pan, Y.H. Zirconia implant abutments supporting single all-ceramic crowns in anterior and premolar regions: A six-year retrospective study. Biomed. J. 2019, 42, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Ghazal-Maghras, R.; Vilaplana-Vivo, J.; Camacho-Alonso, F.; Martínez-Beneyto, Y. Properties of polyetheretheretherketone (PEEK) implant abutments: A systematic review. J. Clin. Exp. Dent. 2022, 14, e349–e358. [Google Scholar] [CrossRef]
- de Holanda Cavalcanti Pereira, A.K.; de Oliveira Limirio, J.P.J.; Cavalcanti do Egito Vasconcelos, B.; Pellizzer, E.P.; Dantas de Moraes, S.L. Mechanical behavior of titanium and zirconia abutments at the implant-abutment interface: A systematic review. J. Prosthet. Dent. 2022, 12. ahead of print. [Google Scholar] [CrossRef]
- Canullo, L.; Micarelli, C.; Lembo-Fazio, L.; Iannello, G.; Clementini, M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures. Clin. Oral. Implant. Res. 2014, 25, 328–336. [Google Scholar] [CrossRef]
- Piattelli, A.; Pontes, A.E.; Degidi, M.; Iezzi, G. Histologic studies on osseointegration: Soft tissues response to implant surfaces and components. A review. Dent. Mater. 2011, 27, 53–60. [Google Scholar] [CrossRef]
- Karl, M.; Taylor, T.D. Parameters determining micromotionat the implant-abutment interface. Int. J. Oral. Maxillofac. Implant. 2014, 29, 1338–1347. [Google Scholar] [CrossRef]
- Khraisat, A. Influence of abutment screw preload on stress distribution in marginal bone. Int. J. Oral. Maxillofac. Implant. 2012, 27, 303–307. [Google Scholar]
- Rack, T.; Zabler, S.; Rack, A.; Riesemeier, H.; Nelson, K. An in vitropilot study of abutment stability during loading in newand fatigue-loaded conical dental implants usingsynchrotron-based radiography. Int. J. Oral. Maxillofac. Implant. 2013, 28, 44–50. [Google Scholar] [CrossRef]
- Sui, X.; Wei, H.; Wang, D.; Han, Y.; Deng, J.; Wang, Y. Experimental research on the relationship between fit accuracy and fracture resistance of zirconia abutments. J. Dent. 2014, 42, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Saravi, B.; Flohr, A.; Patzelt, S.B.; Spies, B.C.; Hazard, D.; Kohal, R.J. Fatigue and Fracture Resistance Testing of Polyether Ether Ketone (PEEK) Implant Abutments in an Ex Vivo Chewing Simulator Model. Materials 2022, 15, 6927. [Google Scholar] [CrossRef] [PubMed]
- Hahnel, S.; Wieser, A.; Lang, R.; Rosentritt, M. Biofilm Formation on the Surface of Modern Implant Abutment Materials. Clin. Oral Implant. Res. 2015, 26, 1297–1301. [Google Scholar] [CrossRef]
- Santing, H.J.; Meijer, H.J.A.; Raghoebar, G.M.; Özcan, M. Fracture Strength and Failure Mode of Maxillary Implant-Supported Provisional Single Crowns: A Comparison of Composite Resin Crowns Fabricated Directly over PEEK Abutments and Solid Titanium Abutments. Clin. Implant. Dent. Relat. Res. 2012, 14, 882–889. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Age (Years Old) | Total | |||||
|---|---|---|---|---|---|---|---|
| 19−29 | 30−39 | 40−49 | 50−59 | 60−69 | 70−82 | ||
| Females | 11 | 39 | 96 | 94 | 77 | 21 | 338 |
| Males | 6 | 38 | 102 | 115 | 103 | 26 | 390 |
| Total | 17 | 77 | 198 | 209 | 180 | 47 | 728 |
| Group | n/% | Standard | P abutment | T abutment | Z Abutment | p |
|---|---|---|---|---|---|---|
| Females | 330 (100) | 126 (38.2) | 18 (5.5) | 139 (42.1) | 47 (14.2) | 0.094 * |
| Males | 377 (100) | 167 (44.3) | 30 (8.0) | 141 (37.4) | 39 (10.3) | |
| Age (mean ± SD) | 52.69 ± 11.68 | 56.54 ± 9.88 | 50.64 ± 11.34 | 51.60 ± 11.79 | 45.43 ± 12.81 | <0.0005 ** |
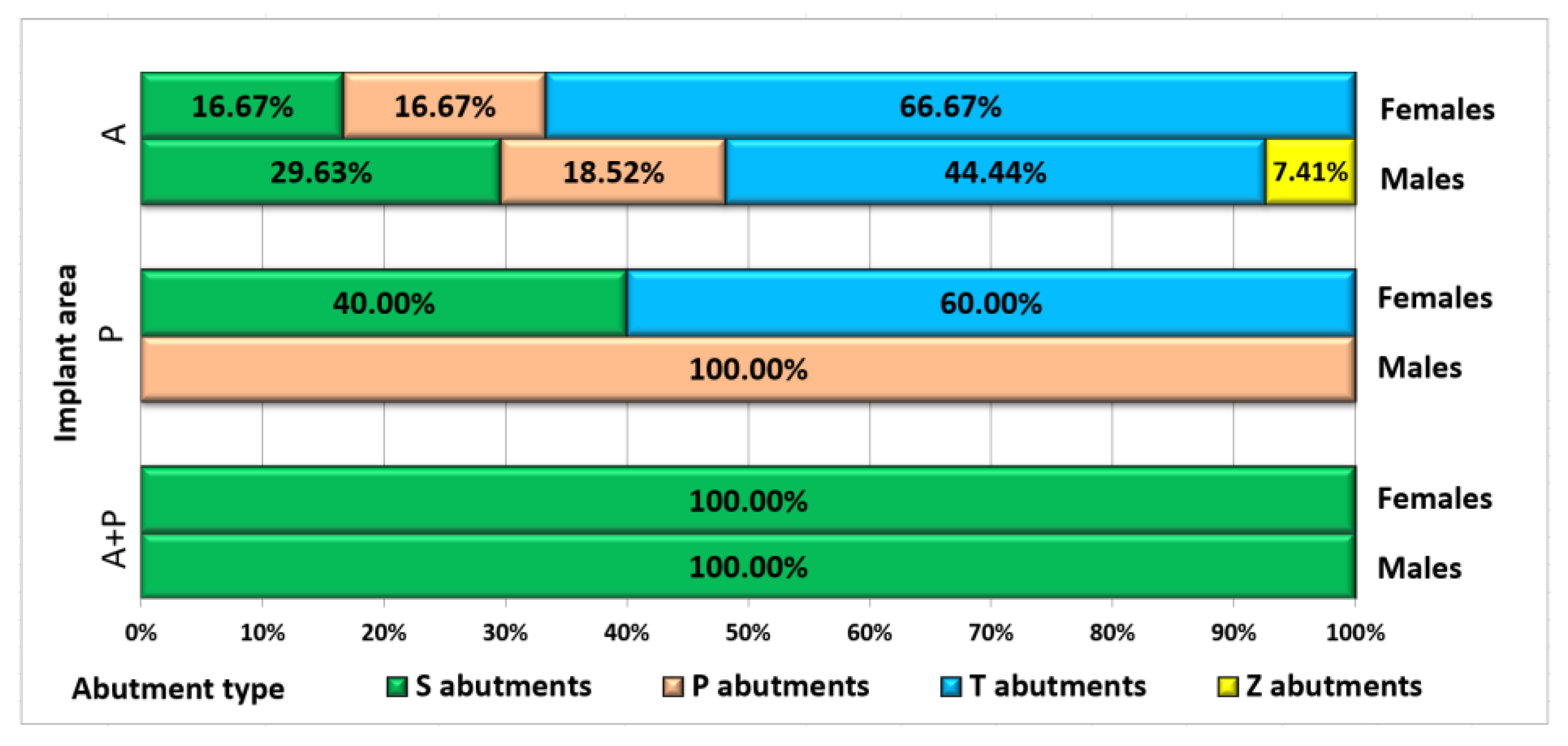
| A | 69 (100) | 9 (13.0) | 22 (31.9) | 23 (33.3) | 15 (21.7) | |
| P | 347 (100) | 6 (1.7) | 26 (7.5) | 244 (70.3) | 71 (20.5) | <0.0005 * |
| A + P | 291 (100) | 278 (95.5) | 0 (0.0) | 13 (4.5) | 1 (0.3) |
| Group | Loading | p * | ||
|---|---|---|---|---|
| Delayed | Immediate | Total | ||
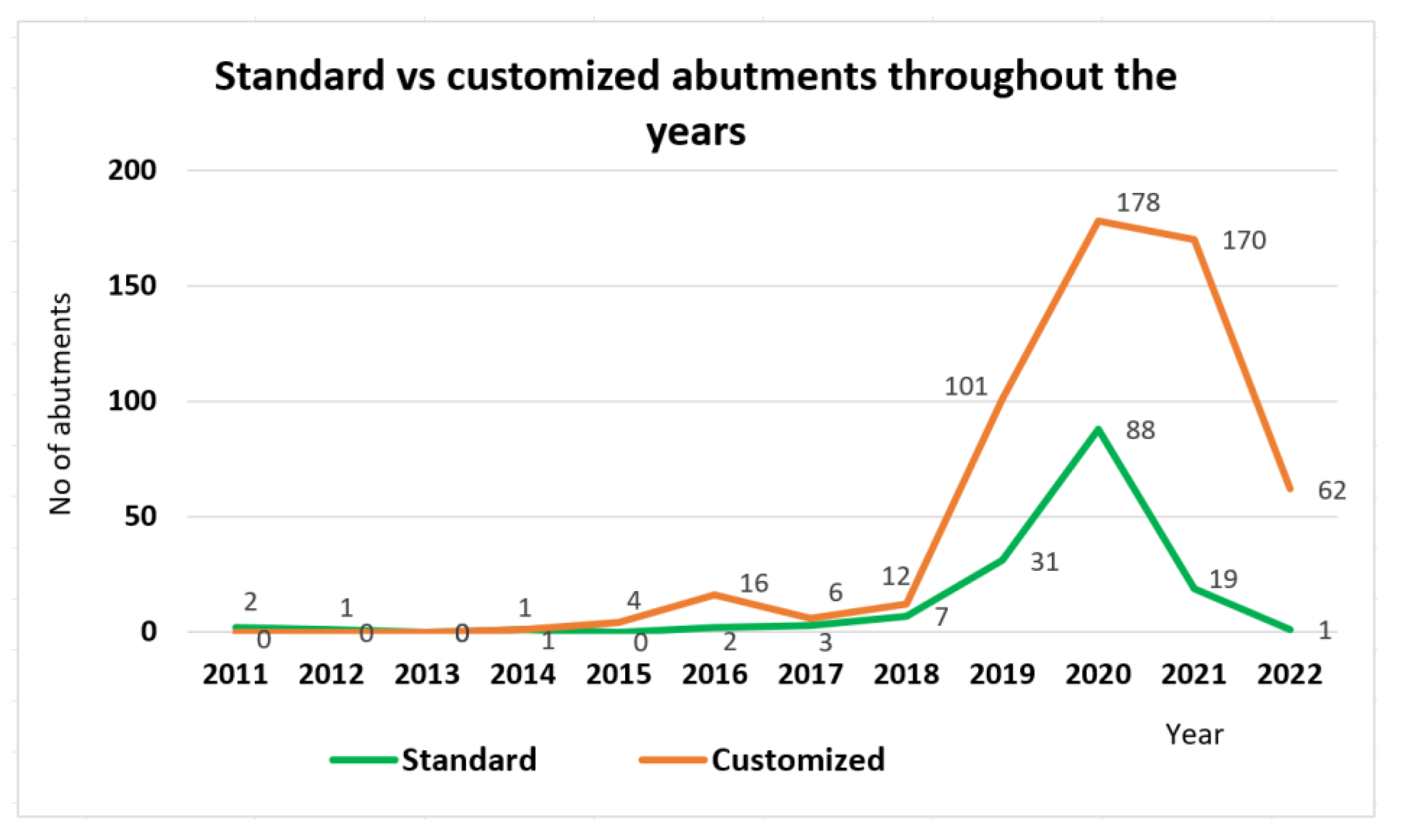
| Standard | 9 (3.1%) | 284 (96.9%) | 293 (100%) | <0.0005 |
| Customized | 386 (93.2%) | 28 (9.6%) | 414 (100%) | |
| P abutment | 41 (85.4%) | 7 (14.6%) | 48 (100%) | |
| T abutment | 261 (93.2%) | 19 (6.8%) | 280 (100%) | |
| Z abutment | 84 (97.7%) | 2 (2.3%) | 86 (100%) | |
| A | 36 (52.2%) | 33 (47.8%) | 69 (100%) | <0.0005 |
| P | 341 (98.3%) | 6 (1.7%) | 347 (100%) | |
| A + P | 18 (6.2%) | 273 (93.8%) | 291 (100%) | |
| Group | Total (N) | Total Complication (n, % from N) | Fractures | Explantation | Decementation | Loosened Screw | Fistulae | p |
|---|---|---|---|---|---|---|---|---|
| Females | 330 | 16 (4.85%) | 8 | 4 | 1 | 2 | 1 | 0.462 * |
| Males | 377 | 20 (5.31%) | 13 | 5 | 2 | - | - | |
| Age (mean ± SD) | 707 | 36 (5.09%) | 58.24 ± 9.46 | 55.55 ± 8.23 | 57.33 ± 4.72 | 55.50 ± 4.95 | - | 0.922 ** |
| Standard | 293 | 27 (9.22%) | 19 | 7 | - | 1 | - | <0.0005 * |
| Customized | 414 | 9 (2.17%) | 2 | 2 | 3 | 1 | 1 | |
| P | 48 | 2 (4.17%) | - | - | 1 | - | 1 | |
| T | 280 | 5 (1.79%) | 2 | 2 | - | 1 | - | |
| Z | 86 | 2 (2.33%) | - | - | 2 | - | - | |
| A | 69 | 5 (7.25%) | - | 3 | 1 | - | 1 | <0.0005 * |
| P | 347 | 5 (1.44%) | - | 2 | 2 | 1 | - | |
| A + P | 291 | 26 (8.93%) | 21 | 4 | - | 1 | - | |
| Delayed loading | 396 | 6 (1.52%) | 2 | 1 | 3 | - | - | <0.0005 * |
| Immediate loading | 311 | 30 (9.65%) | 19 | 8 | - | 2 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obădan, M.E.; Mitruț, I.; Ionescu, M.; Obădan, F.; Târtea, D.A.; Popescu, M.A.; Popescu, S.M.; Smarandache, A.M.; Manolea, H.O. Clinical Efficacy Analysis of the Personalization of Prosthetic Abutments in Implant Supported Restorations in Comparison to Available Standard Titanium Abutments. J. Pers. Med. 2023, 13, 1402. https://doi.org/10.3390/jpm13091402
Obădan ME, Mitruț I, Ionescu M, Obădan F, Târtea DA, Popescu MA, Popescu SM, Smarandache AM, Manolea HO. Clinical Efficacy Analysis of the Personalization of Prosthetic Abutments in Implant Supported Restorations in Comparison to Available Standard Titanium Abutments. Journal of Personalized Medicine. 2023; 13(9):1402. https://doi.org/10.3390/jpm13091402
Chicago/Turabian StyleObădan, Magdalena Eugenia, Ioana Mitruț, Mihaela Ionescu, Florian Obădan, Daniel Adrian Târtea, Marcel Adrian Popescu, Sanda Mihaela Popescu, Andreea Maria Smarandache, and Horia Octavian Manolea. 2023. "Clinical Efficacy Analysis of the Personalization of Prosthetic Abutments in Implant Supported Restorations in Comparison to Available Standard Titanium Abutments" Journal of Personalized Medicine 13, no. 9: 1402. https://doi.org/10.3390/jpm13091402
APA StyleObădan, M. E., Mitruț, I., Ionescu, M., Obădan, F., Târtea, D. A., Popescu, M. A., Popescu, S. M., Smarandache, A. M., & Manolea, H. O. (2023). Clinical Efficacy Analysis of the Personalization of Prosthetic Abutments in Implant Supported Restorations in Comparison to Available Standard Titanium Abutments. Journal of Personalized Medicine, 13(9), 1402. https://doi.org/10.3390/jpm13091402