

No Association of Angiotensin-Converting Enzyme Insertion/Deletion (ACE I/D) Gene Polymorphism in the Susceptibility to Diabetic Retinopathy in Type 2 Diabetes Mellitus Patients: An Updated Meta-Analysis
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Selection of Articles and Evaluation of Methodological Quality
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
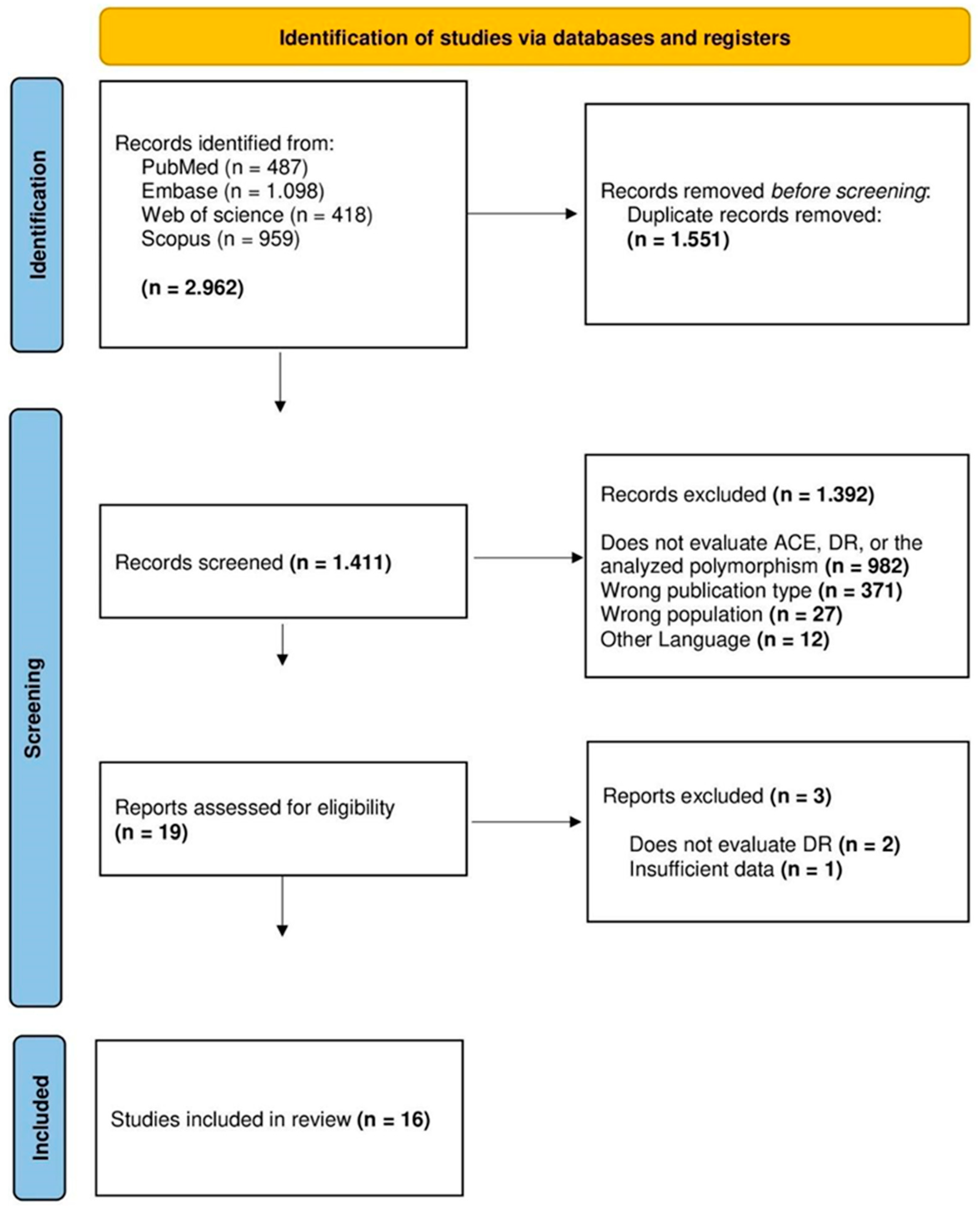
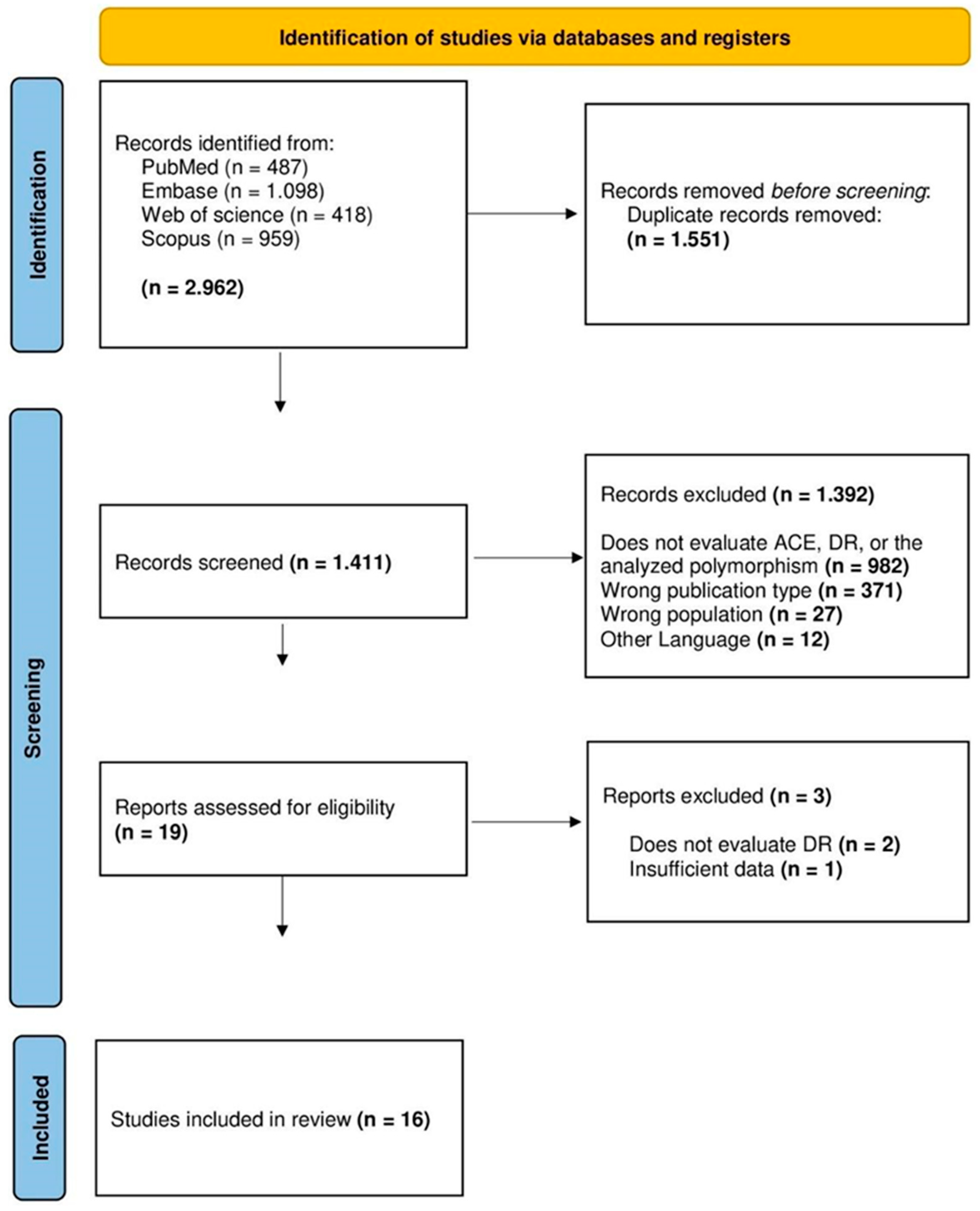
3.1. Selection and Individual Results of Studies
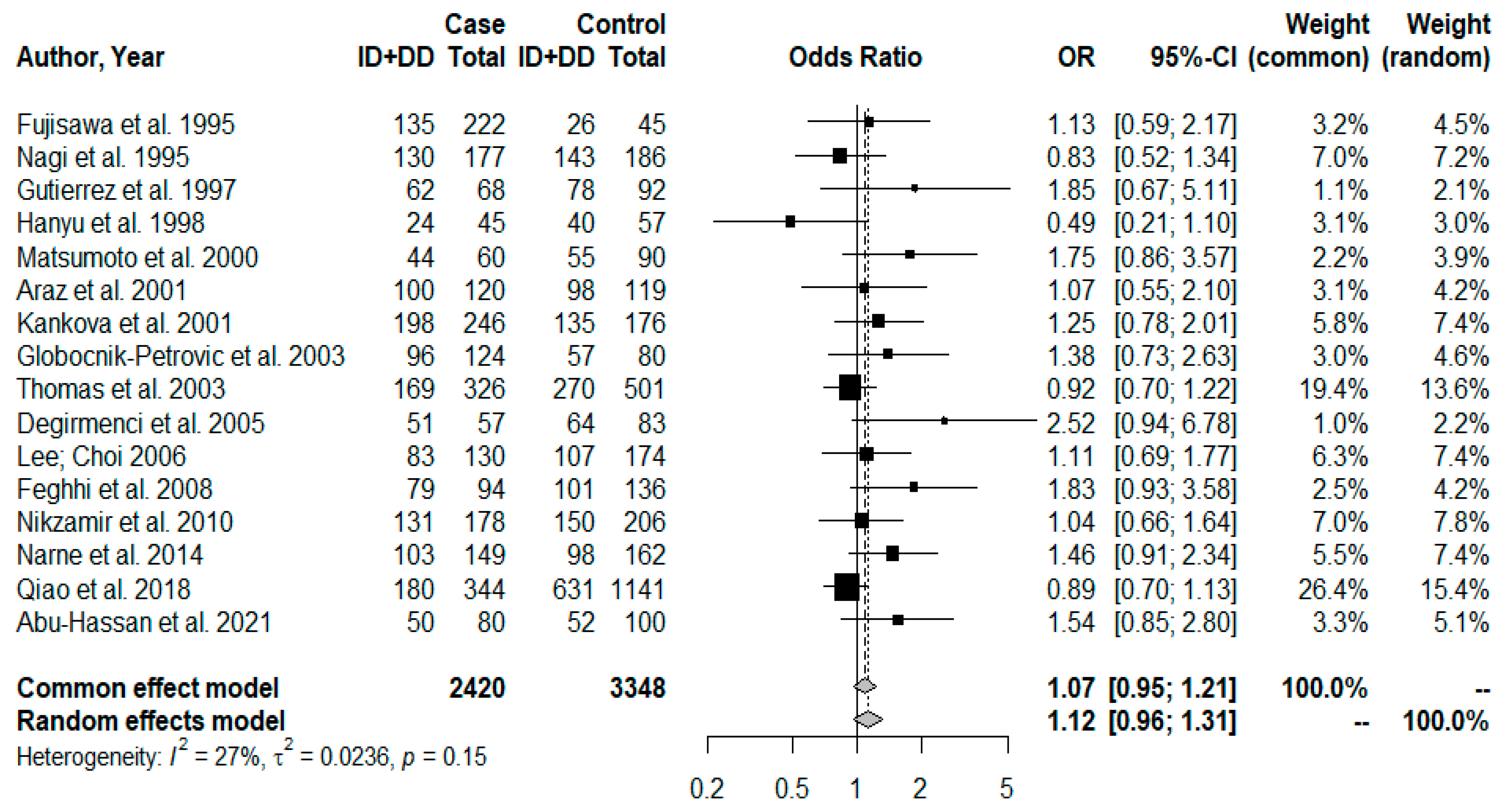
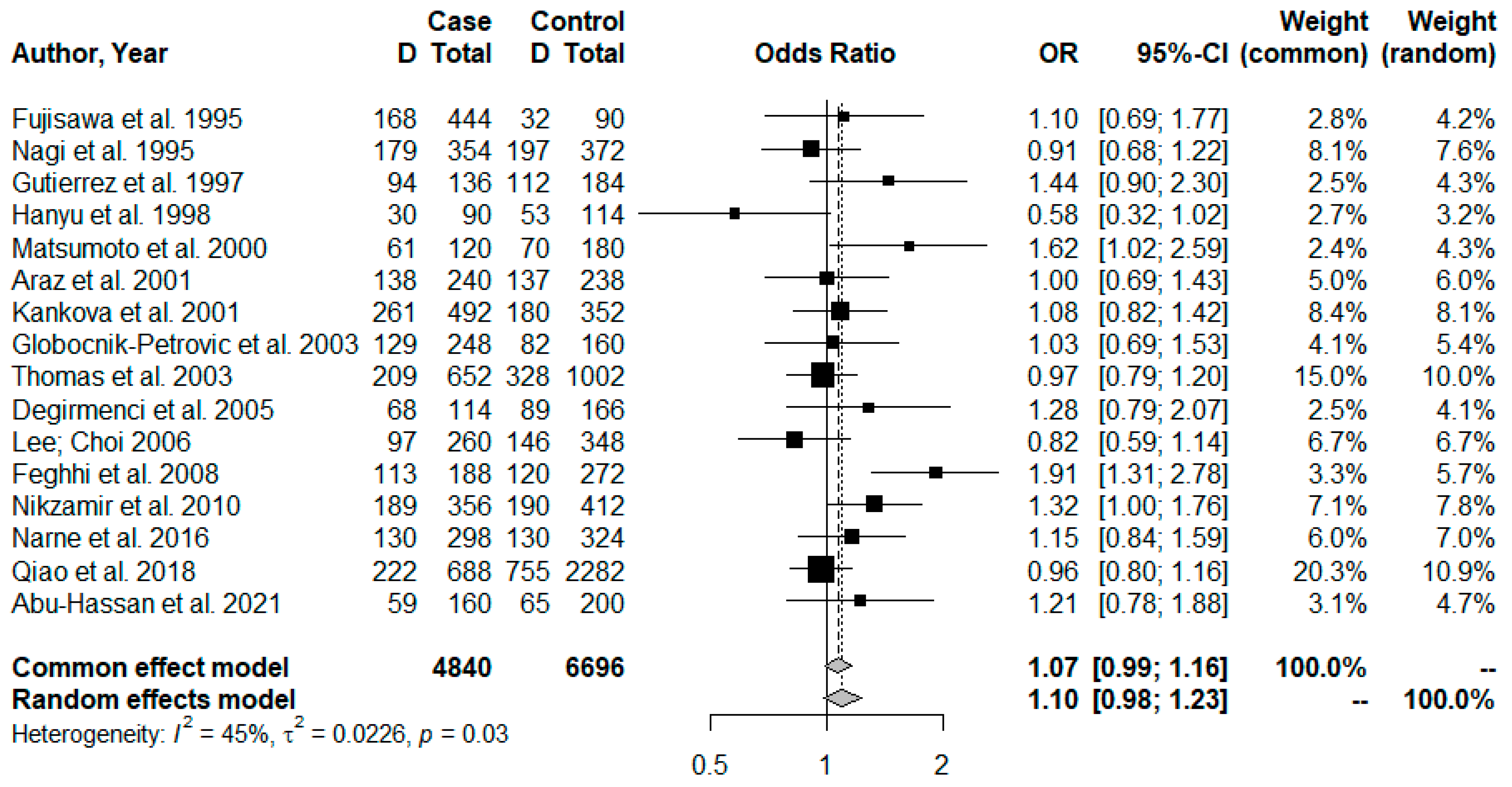
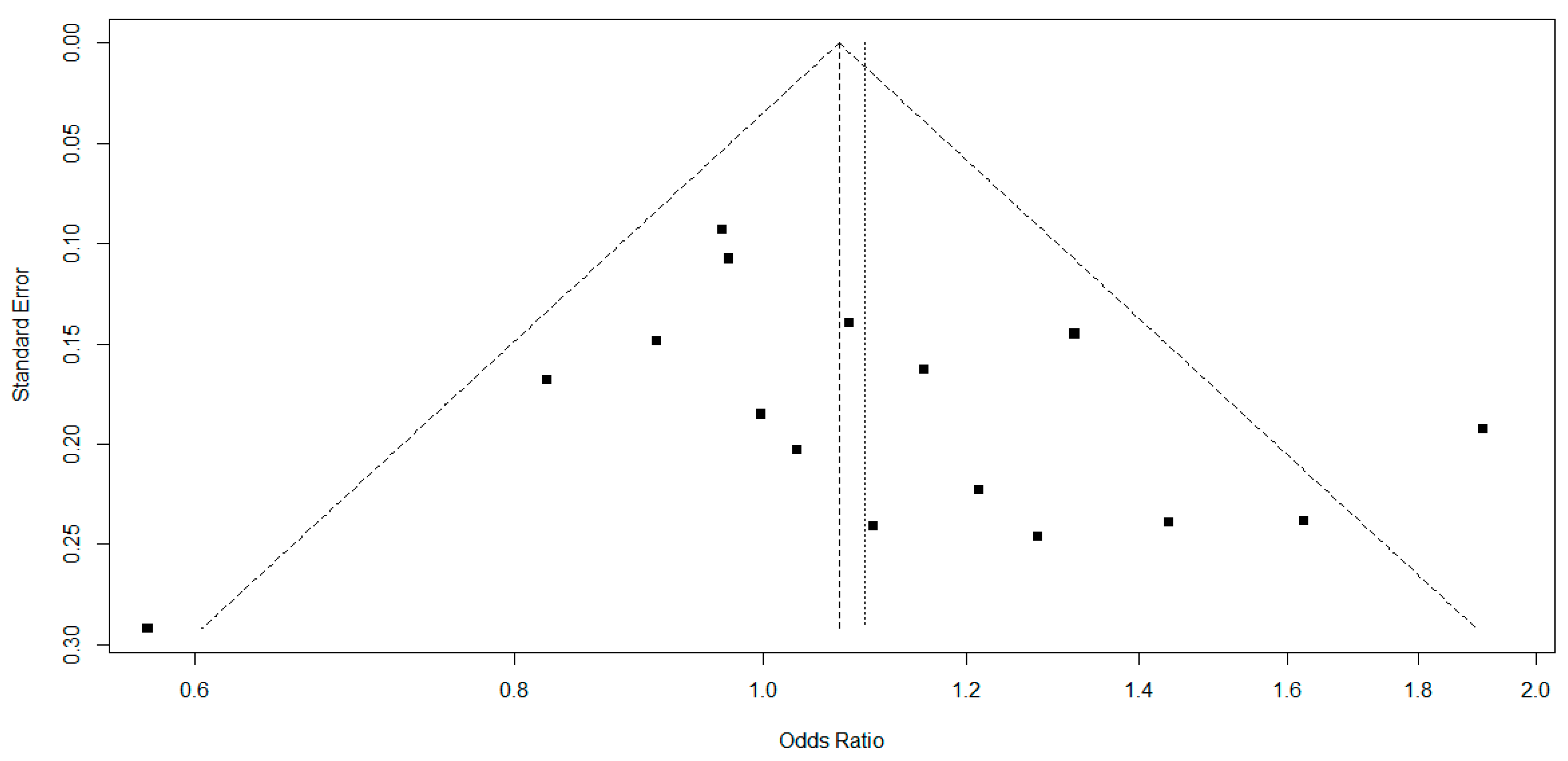
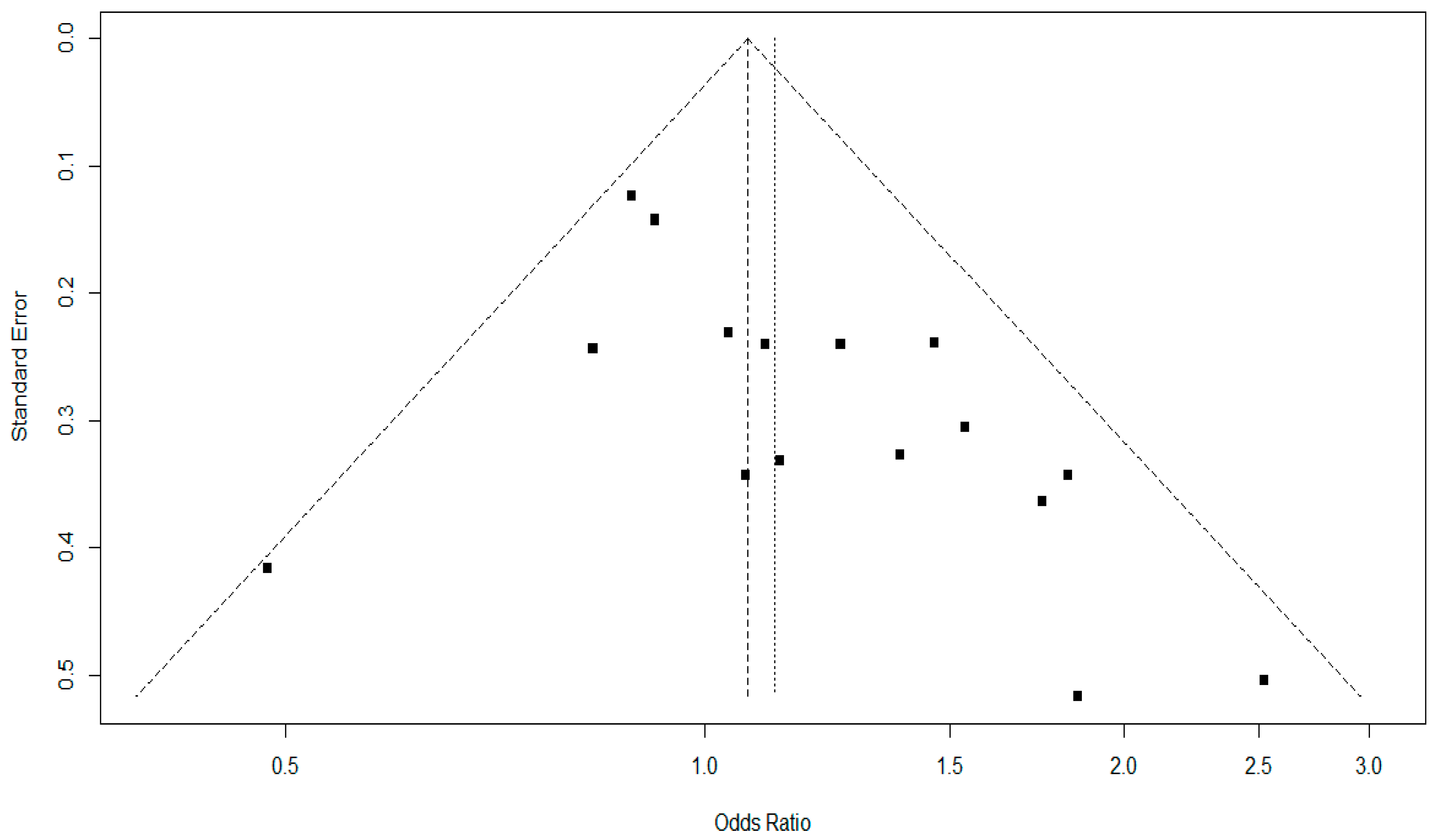
3.2. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bourne, R.R.; Stevens, G.A.; White, R.A.; Smith, J.L.; Flaxman, S.R.; Price, H.; Taylor, H.R. Causes of vision loss worldwide, 1990–2010: A systematic analysis. Lancet Glob. Health 2013, 1, e339–e349. [Google Scholar] [CrossRef] [PubMed]
- Lechner, J.; O’Leary, O.E.; Stitt, A.W. The pathology associated with diabetic retinopathy. Vis. Res. 2017, 139, 7–14. [Google Scholar] [CrossRef]
- Wong, T.Y.; Cheung, C.M.G.; Larsen, M.; Sharma, S.; Simó, R. Diabetic retinopathy. Nat. Rev. Dis. Prim. 2016, 2, 16012. [Google Scholar] [CrossRef]
- Luo, S.; Shi, C.; Wang, F.; Wu, Z. Association between the Angiotensin-Converting Enzyme (ACE) Genetic Polymorphism and Diabetic Retinopathy—A Meta-Analysis Comprising 10,168 Subjects. Int. J. Environ. Res. Public Health 2016, 13, 1142. [Google Scholar] [CrossRef] [PubMed]
- Abu-Hassan, D.W.; Al-Bdour, M.D.; El-Khateeb, M. Lack of relationship between Alu repetitive elements in angiotensin converting enzyme and the severity of diabetic retinopathy. J. Med. Biochem. 2021, 40, 302–309. [Google Scholar]
- Rahimi, Z.; Moradi, M.; Nasri, H. A systematic review of the role of renin angiotensin aldosterone system genes in diabetes mellitus, diabetic retinopathy and diabetic neuropathy. J. Res. Med. Sci. 2014, 19, 1090–1098. [Google Scholar]
- Sayed-Tabatabaei, F.A.; Oostra, B.A.; Isaacs, A.; van Duijn, C.M.; Witteman, J.C.M. ACE Polymorphisms. Circ. Res. 2006, 98, 1123–1133. [Google Scholar] [CrossRef]
- Rigat, B.; Hubert, C.; Alhenc-Gelas, F.; Cambien, F.; Corvol, P.; Soubrier, F. An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J. Clin. Investig. 1990, 86, 1343–1346. [Google Scholar] [CrossRef]
- Rahimi, Z.; Hasanvand, A.; Felehgari, V. Interaction of MTHFR 1298C with ACE D allele augments the risk of diabetic nephropathy in Western Iran. DNA Cell Biol. 2012, 31, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.M.; Nawaz, A.; Evans, M. Diabetes and Novel Coronavirus Infection: Implications for Treatment. Diabetes Ther. 2020, 11, 1915–1924. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan–a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Institute, TJB. JBI Reviewer’s Manual. Joanna Briggs Inst. 32. The Joanna Briggs Institute. 2022. Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 20 March 2023).
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, T.; Ikegami, H.; Shen, G.-Q.; Yamato, E.; Takekawa, K.; Nakagawa, Y.; Ogihara, T. Angiotensin I-converting enzyme gene polymorphism is associated with myocardial infarction, but not with retinopathy or nephropathy, in NIDDM. Diabetes Care 1995, 18, 983–985. [Google Scholar] [CrossRef]
- Nagi, D.K.; Mansfield, M.W.; Stickland, M.H.; Grant, P.J. Angiotensin converting enzyme (ACE) insertion/deletion (I/D) polymorphism, and diabetic retinopathy in subjects with IDDM and NIDDM. Diabet. Med. 1995, 12, 997–1001. [Google Scholar] [CrossRef]
- Gutiérrez, C.; Vendrell, J.; Pastor, R.; Llor, C.; Aguilar, C.; Broch, M.; Richart, C. Angiotensin I-converting enzyme and angiotensinogen gene polymorphisms in non-insulin-dependent diabetes mellitus. Lack of relationship with diabetic nephropathy and retinopathy in a Caucasian Mediterranean population. Metabolism 1997, 46, 976–980. [Google Scholar] [CrossRef]
- Hanyu, O.; Hanawa, H.; Nakagawa, O.; Tani, N.; Andou, N.; Aizawa, Y.; Shibata, A. Polymorphism of the angiotensin I-converting enzyme gene in diabetic nephropathy in type II diabetic patients with proliferative retinopathy. Ren. Fail. 1998, 20, 125–133. [Google Scholar] [CrossRef]
- Matsumoto, A.; Iwashima, Y.; Abiko, A.; Morikawa, A.; Sekiguchi, M.; Eto, M.; Makino, I. Detection of the association between a deletion polymorphism in the gene encoding angiotensin I-converting enzyme and advanced diabetic retinopathy. Diabetes Res. Clin. Pract. 2000, 50, 195–202. [Google Scholar] [CrossRef]
- Araz, M.; Yilmaz, N.; Güngör, K.; Okan, V.; Kepekci, Y.; Sükrü Aynacioglu, A. Angiontensin-converting enzyme gene polymorphism and microvascular complications in Turkish type 2 diabetic patients. Diabetes Res. Clin. Pract. 2001, 54, 95–104. [Google Scholar] [CrossRef]
- Kanková, K.; Muzík, J.; Karásková, J.; Beránek, M.; Hájek, D.; Znojil, V.; Vácha, J. Duration of non-insulin-dependent diabetes mellitus and the TNF-beta NcoI genotype as predictive factors in proliferative diabetic retinopathy. Ophthalmologica 2001, 215, 294–298. [Google Scholar] [CrossRef]
- Globocnik-Petrovic, M.; Hawlina, M.; Peterlin, B.; Petrovic, D. Insertion/deletion plasminogen activator inhibitor 1 and insertion/deletion angiotensin-converting enzyme gene polymorphisms in diabetic retinopathy in type 2 diabetes. Ophthalmologica 2003, 217, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.N.; Critchley, J.A.J.H.; Tomlinson, B.; Yeung, V.T.F.; Lam, D.; Cockram, C.S. Renin-angiotensin system gene polymorphisms and retinopathy in Chinese patients with type 2 diabetes. Diabetes Care 2003, 26, 1643–1644. [Google Scholar] [CrossRef]
- Degirmenci, I.; Kebapci, N.; Basaran, A.; Efe, B.; Gunes, H.V.; Akalin, A.; Demirustu, C. Frequency of angiotensin-converting enzyme gene polymorphism in Turkish type 2 diabetic patients. Int. J. Clin. Pract. 2005, 59, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Choi, M.G. Association of manganese superoxide dismutase gene polymorphism (V16A) with diabetic macular edema in Korean type 2 diabetic patients. Metabolism 2006, 55, 1681–1688. [Google Scholar] [CrossRef]
- Feghhi, M.; Nikzamir, A.; Esteghamati, A.; Farahi, F.; Nakhjavani, M.; Rashidi, A. The relationship between angiotensin-converting enzyme insertion/deletion polymorphism and proliferative retinopathy in type 2 diabetes. Diabetes Res. Clin. Pract. 2008, 81, e1–e4. [Google Scholar] [CrossRef]
- Nikzamir, A.; Rashidi, A.; Esteghamati, A.; Nakhjavani, M.; Golmohammadi, T.; Khalilzadeh, O. The relationship between ACE gene insertion/deletion polymorphism and diabetic retinopathy in Iranian patients with type 2 diabetes. Ophthalmic Genet. 2010, 31, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Narne, P.; Ponnaluri, K.C.; Siraj, M.; Ishaq, M. Association analysis of polymorphisms in genes related to oxidative stress in South Indian type 2 diabetic patients with retinopathy. Ophthalmic Genet. 2016, 37, 1–8. [Google Scholar] [CrossRef]
- Qiao, Y.-C.; Wang, M.; Pan, Y.-H.; Zhang, X.-X.; Tian, F.; Chen, Y.-L.; Zhao, H.L. The relationship between ACE/AGT gene polymorphisms and the risk of diabetic retinopathy in Chinese patients with type 2 diabetes. J. Renin-Angiotensin-Aldosterone Syst. 2018, 19, 1470320317752955. [Google Scholar] [CrossRef]
- IDF. International Diabetes Federation. Diabetes. In Atlas of Diabetes, 10a ed.; Boyko, E.J., Magliano, D.J., Eds.; Science & Business Media: Brussels, Belgium, 2021. [Google Scholar]
- Hampton, B.M.; Schwartz, S.G.; Brantley, M.A.; Flynn, H.W. Update on genetics and diabetic retinopathy. Clin. Ophthalmol. 2015, 9, 2175–2193. [Google Scholar]
- Suzuki, Y.; Kiyosawa, M. Relationship between Diabetic Nephropathy and Development of Diabetic Macular Edema in Addition to Diabetic Retinopathy. Biomedicines 2023, 11, 1502. [Google Scholar] [CrossRef]
- Vofo, B.N.; Chowers, I. Suppressing Inflammation for the Treatment of Diabetic Retinopathy and Age-Related Macular Degeneration: Dazdotuftide as a Potential New Multitarget Therapeutic Candidate. Biomedicines 2023, 11, 1562. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Fang, Q.; Yu, N.; Zhao, D.; Zhang, Y.; Wang, J.; Fan, X. Association between genetic polymorphism of the angiotensin-converting enzyme and diabetic nephropathy: A meta-analysis comprising 26,580 subjects. J. Renin-Angiotensin-Aldosterone Syst. 2012, 13, 161–174. [Google Scholar] [CrossRef]
- Silveira, L.C.; da Silva, E.G.; Azevedo, R.M.; dos Anjos, L.R.B.; Chagas, R.F.; Alcântara, E.C.; Reis, A.A.S. ACE insertion/deletion polymorphism and diabetic nephropathy: An evidence-based meta-analysis. Genet. Mol. Res. 2019, 18, GMR18378. [Google Scholar] [CrossRef]
- Zhou, M.S.; Schulman, I.H. Prevention of diabetes in hypertensive patients: Results and implications from the VALUE trial. Vasc. Health Risk Manag. 2009, 5, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, Z.; Mansouri, Z.O.; Rahimi, Z.; Abbasi, A. AT2R -1332 G: A polymorphism and diabetic nephropathy in type 2 diabetes mellitus patients. J. Ren. Inj. Prev. 2013, 2, 97–101. [Google Scholar]
- Cordonnier, D.J.; Zaoui, P.; Halimi, S. Role of ACE inhibitors in patients with diabetes mellitus. Drugs 2001, 61, 1883–1892. [Google Scholar] [CrossRef]
- Gilbert, R.E.; Krum, H.; Wilkinson-Berka, J.; Kelly, D.J. The renin-angiotensin system and the long-term complications of diabetes: Pathophysiological and therapeutic considerations. Diabet. Med. 2003, 20, 607–621. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, M.; Karkucak, M.; Yakut, T.; Gorukmez, O.; Ozmen, A. Lack of association of genetic polymorphisms of angiotensin-converting enzyme gene I/D and glutathione-S-transferase enzyme T1 and M1 with retinopathy of prematures. Genet. Mol. Res. 2010, 9, 2131–2139. [Google Scholar] [CrossRef]
- Cheema, B.S.; Kohli, H.S.; Sharma, R.; Shah, V.N.; Bhansali, A.; Khullar, M. Angiotensin-converting enzyme gene variants interact with the renin-angiotensin system pathway to confer risk and protection against type 2 diabetic retinopathy. J. Diabetes Investig. 2013, 4, 103–104. [Google Scholar] [CrossRef]
- Saleem, S.; Azam, A.; Maqsood, S.I.; Muslim, I.; Bashir, S.; Fazal, N.; Azam, M. Role of ACE and PAI-1 Polymorphisms in the Development and Progression of Diabetic Retinopathy. PLoS ONE 2015, 10, e0144557. [Google Scholar] [CrossRef]
- Schmidt, S.; Strojek, K.; Grzeszczak, W.; Bergis, K.; Ritz, E. Excess of DD homozygotes in haemodialysed patients with type II diabetes. The diabetic nephropathy study group. Nephrol. Dial. Transpl. 1997, 12, 427–429. [Google Scholar] [CrossRef] [PubMed]
- Shaker, O.G.; Ismail, M.F.; Ashour, E.; Yousif, H.M.; Afify, M.; Gouda, W. ACE gene polymorphism and serum ACE level with Progression of Nephropathy in Type 2 Diabetic Patients. J. Adv. Chem. 2014, 9, 2023–2032. [Google Scholar] [CrossRef]
- Alharbi, A.M.D.; Alhazmi, A.M.S. Prevalence, Risk Factors, and Patient Awareness of Diabetic Retinopathy in Saudi Arabia: A Review of the Literature. Cureus 2020, 12, e11991. [Google Scholar] [CrossRef] [PubMed]
- Abhary, S.; Hewitt, A.W.; Burdon, K.P.; Craig, J.E. A systematic meta-analysis of genetic association studies for diabetic retinopathy. Diabetes 2009, 58, 2137–2147. [Google Scholar] [CrossRef]
- Salem, A.H.; Batzer, M.A. High frequency of the D allele of the angiotensin converting enzyme gene in Arabic populations. BMC Res. Notes 2009, 2, 99. [Google Scholar] [CrossRef]
- Zhou, J.B.; Yang, J.K. Angiotensin-converting enzyme gene polymorphism is associated with proliferative diabetic retinopathy: A meta-analysis. Acta Diabetol. 2010, 47 (Suppl. 10), 187–193. [Google Scholar] [CrossRef]
- Zhou, D.; Ruiter, R.; Zhang, J.; Zhou, M.; Liu, H.; Liu, W.; Wang, S. Angiotensin-converting enzyme I/D polymorphism is not associated with type 2 diabetes in a Chinese population. JRAAS–J. Renin-Angiotensin-Aldosterone Syst. 2012, 13, 372–378. [Google Scholar] [CrossRef]
- Catalogue of Bias Collaboration; Spencer, E.A.; Brassey, J.; Mahtani, K.; Heneghan, C. Wrong sample size bias. In Catalogue of Bias; 2017; Available online: https://catalogofbias.org/biases/wrong-sample-size-bias/ (accessed on 20 March 2023).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | Search Strategy |
|---|---|
| PubMed/MEDLINE | ((“Diabetes Mellitus”[Mesh] OR “Diabetes Mellitus, Type 2”[Mesh]) AND (“Polymorphism, Genetic”[Mesh] OR “Amplified Fragment Length Polymorphism Analysis”[Mesh])) AND (“Diabetic Retinopathy/complications”[Mesh] OR “Diabetic Retinopathy/genetics”[Mesh]) |
| Embase | ‘((‘diabetes mellitus’/exp OR ‘non insulin dependent diabetes mellitus’/exp) AND ‘genetic polymorphism’/exp OR ‘amplified fragment length polymorphism’/exp) AND ‘diabetic retinopathy’/exp AND [1992–2022]/py |
| Web of Science | ((((ALL=(diabetes)) OR ALL=(type 2 diabetes mellitus)) AND ALL=(genetic polymorphism)) OR ALL=(amplified fragment length polymorphism analysis)) AND ALL=(diabetic retinopathy) |
| Scopus | (TITLE-ABS-KEY (diabetes) OR TITLE-ABS-KEY (type 2 diabetes AND mellitus) AND TITLE-ABS-KEY (genetic AND polymorphism) OR TITLE-ABS-KEY (amplified AND fragment AND length AND polymorphism AND analysis) AND TITLE-ABS-KEY (diabetic AND retinopathy)) AND (LIMIT-TO (PUBYEAR, 2022) OR LIMIT-TO (PUBYEAR, 2021) OR LIMIT-TO (PUBYEAR, 2020) OR LIMIT-TO (PUBYEAR, 2019) OR LIMIT-TO (PUBYEAR, 2018) OR LIMIT-TO (PUBYEAR, 2017) OR LIMIT-TO (PUBYEAR, 2016) OR LIMIT-TO (PUBYEAR, 2015) OR LIMIT-TO (PUBYEAR, 2014) OR LIMIT-TO (PUBYEAR, 2013) OR LIMIT-TO (PUBYEAR, 2012) OR LIMIT-TO (PUBYEAR, 2011) OR LIMIT-TO (PUBYEAR, 2010) OR LIMIT-TO (PUBYEAR, 2009) OR LIMIT-TO (PUBYEAR, 2008) OR LIMIT-TO (PUBYEAR, 2007) OR LIMIT-TO (PUBYEAR, 2006) OR LIMIT-TO (PUBYEAR, 2005) OR LIMIT-TO (PUBYEAR, 2004) OR LIMIT-TO (PUBYEAR, 2003) OR LIMIT-TO (PUBYEAR, 2002) OR LIMIT-TO (PUBYEAR, 2001) OR LIMIT-TO (PUBYEAR, 2000) OR LIMIT-TO (PUBYEAR, 1999) OR LIMIT-TO (PUBYEAR, 1998) OR LIMIT-TO (PUBYEAR, 1997) OR LIMIT-TO (PUBYEAR, 1996) OR LIMIT-TO (PUBYEAR, 1995) OR LIMIT-TO (PUBYEAR, 1994) OR LIMIT-TO (PUBYEAR, 1993) OR LIMIT-TO (PUBYEAR, 1992)) |
| Reference | Country | Design | Case | Control | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | Sex (M/F) | Age (Year) | DM Duration (Year) | Definition | Sample Size | Sex (M/F) | Age (Year) | DM Duration (Year) | Definition | |||
| Abu-Hassan et al. [5] | Jordan | Cross-sectional | 80 | 41/41 | 62 ± 8 | 10.8 ± 4.1 | DR (T2DM) | 100 | 39/61 | 60 ± 8 | 7.0 ± 4.3 | NDR (T2DM) |
| Fujisawa et al. [16] | Japan | Case-control | 222 | NA | NA | NA | DR (T2DM) | 45 | NA | NA | NA | NDR (T2DM) |
| Nagi et al. [17] | United Kingdom | Cross-sectional | 177 | 55/45 | 66.8 ± 10.4 | 11 (1–36) | DR (T2DM) | 186 | 52/48 | 69.5 ± 11.1 | 7 (1–45) | NDR (T2DM) |
| Gutiérrez et al. [18] | Spain | Case-control | 68 | 29/39 | 61.90 ± 9.1 | 14.8 ± 5.7 | DR (T2DM) | 92 | 45/47 | 59.6 ± 10.3 | 12.1 ± 6.3 | NDR (T2DM) |
| Hanyu et al. [19] | Japan | Case-control | 45 | 15/30 | 58.0 ± 8.8 | 18.2 ± 5.7 | DR (T2DM) | 57 | 31/26 | 56.4 ± 5.1 | NA | Healthy |
| Matsumoto et al. [20] | Japan | Case-control | 60 | 27/37 | 56.8±11.90 | 16.2 ± 9.1 | DR (T2DM) | 90 | 50/40 | 58.9 ± 12.1 | 15.0 ± 6.6 | NDR (T2DM) |
| Araz et al. [21] | Turkey | Cross-sectional | 120 | 49/71 | 55 ± 8 | 11.2 ± 6.5 | DR (T2DM) | 119 | 37/82 | 51 ± 9 | 5.2 ± 5.1 | NDR (T2DM) |
| Kanková et al. [22] | Czech Republic | Cohort | 246 | 118/128 | 64.1 ± 11.1 | 10.2 ± 9.2 | DR (T2DM) | 176 | 67/109 | 63.60 ± 13.4 | NA | Healthy |
| Globocnik-Petrovic et al. [23] | Slovenia | Case-control | 124 | 59/65 | 65.6 ± 9.7 | 18.7 ± 9.1 | DR (T2DM) | 80 | 40/40 | 71.3 ± 7.0 | 16.8 ± 6.8 | NDR (T2DM) |
| Thomas et al. [24] | China | Case-control | 326 | 128/198 | 59.8 ± 11.4 | 6.3 (5.6–7.0) | DR (T2DM) | 501 | 197/304 | 60.4 ± 9.3 | 6.0 (5.6–6.3) | NDR (T2DM) |
| Degirmenci et al. [25] | Turkey | Case-control | 57 | 95/48 | 57.66 ± 0.85 | 10.64 ± 0.22 | DR (T2DM) | 83 | 83/50 | 46.39 ± 1.52 | NA | NDR (T2DM) |
| Lee; Choi [26] | South Korea | Cross-sectional | 130 | 77/53 | 53.1 ± 12.3 | 11.4 ± 3.7 | DR (T2DM) | 174 | 102/72 | 53.7 ± 12.9 | 9.4.± 2.8 | NDR (T2DM) |
| Feghhi et al. [27] | Iran | Case-control | 94 | 56/38 | 60.55 ± 8.15 | 14.01 ± 4.38 | PDR (T2DM) | 136 | 87/49 | 60.46 ± 7.85 | 13.40 ± 5.0 | NPDR (T2DM) |
| Nikzamir et al. [28] | Iran | Case-control | 178 | 92/86 | 59.0 ± 8.7 | 13 (4–30) | DR (T2DM) | 206 | 114/92 | 59.5 ± 8.2 | 11 (1–30) | NDR (T2DM) |
| Narne et al. [29] | India | Case-control | 149 | 47/102 | 52.7 ± 7.3 | 14.7 ± 4.7 | DR (T2DM) | 162 | 49/113 | 53.4 ± 5.4 | 15.9 ± 5.6 | NDR (T2DM) |
| Qiao et al. [30] | China | Cross-sectional | 344 | 148/197 | 60.08 ±11.34 | 8.97 ±7.13 | DR (T2DM) | 1141 | 455/691 | 51.42 ±13.59 | 4.45 ±4.62 | NDR (T2DM) |
| Reference | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abu-Hassan et al. [5] 2 | Y | Y | N | Y | Y | U | Y | Y | NA | NA | NA |
| Fujisawa et al. [15] 1 | Y | Y | Y | Y | Y | N | N | Y | Y | Y | NA |
| Nagi et al. [17] 2 | Y | Y | Y | Y | Y | U | Y | Y | NA | NA | NA |
| Gutiérrez et al. [18] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Hanyu et al. [19] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Matsumoto et al. [20] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Araz et al. [21] 2 | Y | Y | Y | Y | Y | Y | Y | Y | NA | NA | NA |
| Kanková et al. [22] 3 | Y | Y | Y | Y | Y | U | Y | Y | Y | NA | Y |
| Globocnik-Petrovic et al. [23] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Thomas et al. [24] 1 | Y | Y | U | Y | Y | Y | N | Y | Y | Y | NA |
| Degirmenci et al. [25] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Lee; Choi [26] 2 | Y | Y | Y | Y | Y | Y | Y | Y | NA | NA | NA |
| Feghhi et al. [27] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Nikzamir et al. [28] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Narne et al. [29] 1 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA |
| Qiao et al. [30] 2 | Y | Y | Y | Y | Y | Y | Y | Y | NA | NA | NA |
| Reference | Genotype Frequency | Allele Frequency | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| I/I | I/D | D/D | I | D | ||||||
| Case | Control | Case | Control | Case | Control | Case | Control | Case | Control | |
| Abu-Hassan et al. [5] | 30 | 48 | 41 | 39 | 9 | 13 | 101 | 135 | 59 | 65 |
| Fujisawa et al. [16] | 87 | 19 | 102 | 20 | 33 | 6 | 276 | 58 | 168 | 32 |
| Nagi et al. [17] | 47 | 43 | 81 | 89 | 49 | 54 | 175 | 175 | 179 | 197 |
| Gutiérrez et al. [18] | 6 | 14 | 30 | 44 | 32 | 34 | 42 | 72 | 94 | 112 |
| Hanyu et al. [19] | 21 | 17 | 18 | 27 | 6 | 13 | 60 | 61 | 30 | 53 |
| Matsumoto et al. [20] | 16 | 35 | 27 | 40 | 17 | 15 | 59 | 110 | 61 | 70 |
| Araz et al. [21] | 20 | 21 | 62 | 59 | 38 | 39 | 102 | 101 | 138 | 137 |
| Kanková et al. [22] | 48 | 41 | 135 | 90 | 63 | 45 | 231 | 172 | 261 | 180 |
| Globocnik-Petrovic et al. [23] | 28 | 23 | 63 | 32 | 33 | 25 | 119 | 78 | 129 | 82 |
| Thomas et al. [24] | 157 | 231 | 129 | 212 | 40 | 58 | 443 | 674 | 209 | 328 |
| Degirmenci et al. [25] | 6 | 19 | 34 | 39 | 17 | 25 | 46 | 73 | 68 | 89 |
| Lee; Choi [26] | 47 | 67 | 69 | 68 | 14 | 39 | 163 | 202 | 97 | 146 |
| Feghhi et al. [27] | 15 | 35 | 45 | 82 | 34 | 19 | 75 | 152 | 113 | 120 |
| Nikzamir et al. [28] | 47 | 56 | 73 | 110 | 58 | 40 | 167 | 222 | 189 | 190 |
| Narne et al. [29] | 46 | 64 | 76 | 66 | 27 | 32 | 168 | 194 | 130 | 130 |
| Qiao et al. [30] | 164 | 510 | 138 | 507 | 42 | 124 | 466 | 1527 | 222 | 755 |
| Total | 785 | 1243 | 1123 | 1524 | 512 | 581 | 2693 | 4006 | 2147 | 2686 |
| Analyzes Performed | Egger’s Test | Begg’s Test |
|---|---|---|
| Genotypic | 0.01 | 0.05 |
| Allelic | 0.25 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, A.R.d.P.; Silveira, L.C.; Santos, K.d.F.; Santos, R.d.S.; Reis, A.A.d.S. No Association of Angiotensin-Converting Enzyme Insertion/Deletion (ACE I/D) Gene Polymorphism in the Susceptibility to Diabetic Retinopathy in Type 2 Diabetes Mellitus Patients: An Updated Meta-Analysis. J. Pers. Med. 2023, 13, 1308. https://doi.org/10.3390/jpm13091308
Coelho ARdP, Silveira LC, Santos KdF, Santos RdS, Reis AAdS. No Association of Angiotensin-Converting Enzyme Insertion/Deletion (ACE I/D) Gene Polymorphism in the Susceptibility to Diabetic Retinopathy in Type 2 Diabetes Mellitus Patients: An Updated Meta-Analysis. Journal of Personalized Medicine. 2023; 13(9):1308. https://doi.org/10.3390/jpm13091308
Chicago/Turabian StyleCoelho, Aline Ruilowa de Pinho, Luciana Carvalho Silveira, Kamilla de Faria Santos, Rodrigo da Silva Santos, and Angela Adamski da Silva Reis. 2023. "No Association of Angiotensin-Converting Enzyme Insertion/Deletion (ACE I/D) Gene Polymorphism in the Susceptibility to Diabetic Retinopathy in Type 2 Diabetes Mellitus Patients: An Updated Meta-Analysis" Journal of Personalized Medicine 13, no. 9: 1308. https://doi.org/10.3390/jpm13091308
APA StyleCoelho, A. R. d. P., Silveira, L. C., Santos, K. d. F., Santos, R. d. S., & Reis, A. A. d. S. (2023). No Association of Angiotensin-Converting Enzyme Insertion/Deletion (ACE I/D) Gene Polymorphism in the Susceptibility to Diabetic Retinopathy in Type 2 Diabetes Mellitus Patients: An Updated Meta-Analysis. Journal of Personalized Medicine, 13(9), 1308. https://doi.org/10.3390/jpm13091308