
Endotyping of Cholesteatoma: Which Molecular Biomarkers? A Systematic Review

 ,
, 
 ,
,
Abstract
1. Introduction
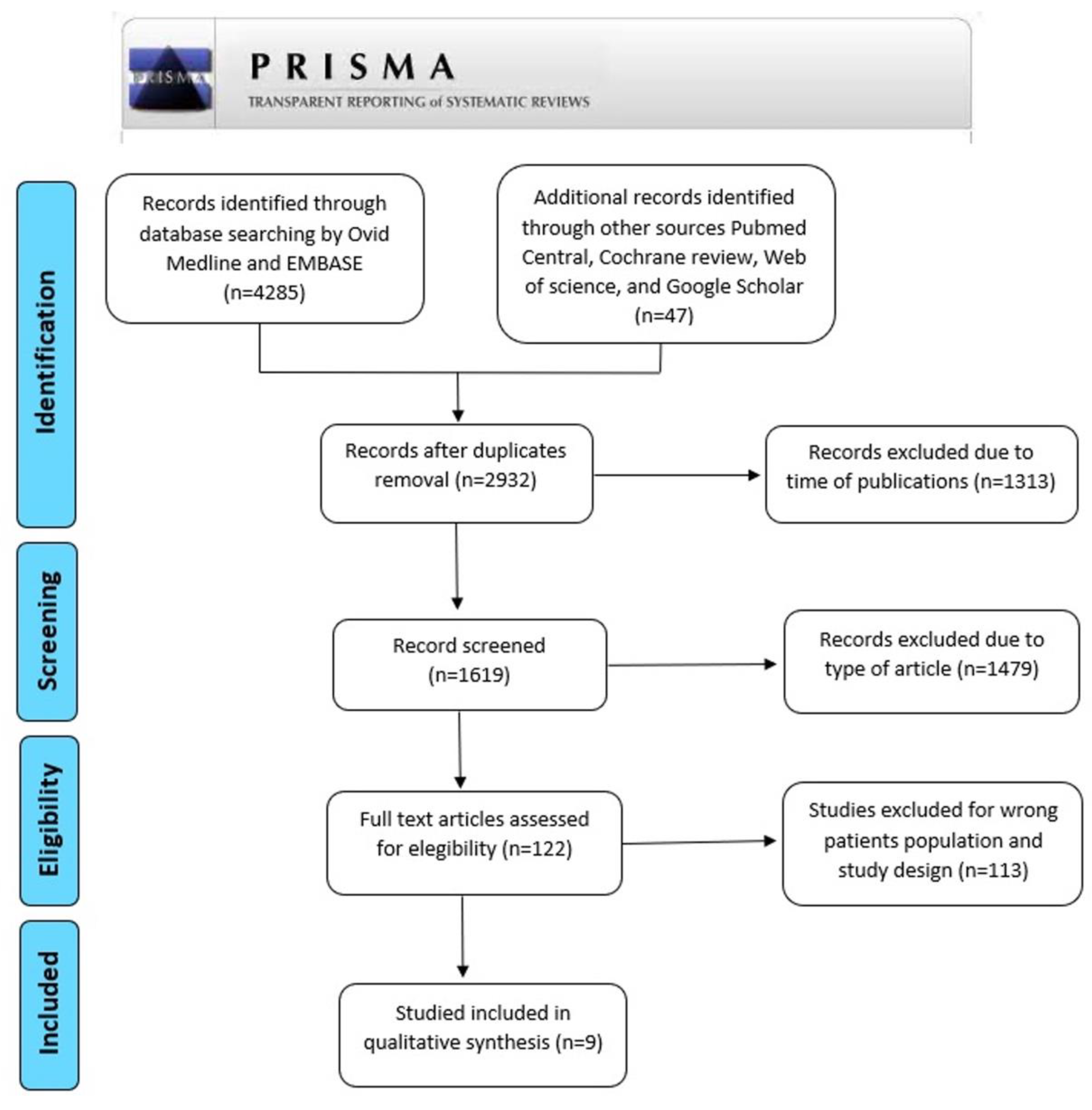
2. Materials and Methods
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sade, J. Treatment of cholesteatoma and retraction pockets. Eur. Arch. Otorhinol. 1993, 250, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Skoloudik, L.; Simakova, E.; Kalfert, D.; Chrobok, V. Histological changes of the middle ear ossicles harvested during cholesteatoma surgery. Acta Med. 2015, 58, 119–122. [Google Scholar]
- Kuo, C.L.; Shiao, A.S.; Yung, M.; Sakagami, M.; Sudhoff, H.; Wang, C.H.; Hsu, C.H.; Lien, C.F. Updates and knowledge gaps in cholesteatoma research. BioMed Res. Int. 2015, 2015, 854024. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, K.L.; Singh, A.K. Middle Ear Cholesteatoma; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Eggink, M.C.; de Wolf, M.J.F.; Ebbens, F.A.; Dikkers, F.G.; van Spronsen, E. Evaluation of Long-term Cholesteatoma Recidivism: Using the JOS, EAONO-JOS, and STAMCO Cholesteatoma Staging Systems. Otol. Neurotol. 2021, 42, 1031–1038. [Google Scholar] [CrossRef]
- Jennings, B.A.; Prinsley, P.; Philpott, C.; Willis, G.; Bhutta, M.F. The genetics of cholesteatoma. A systematic review using narrative synthesis. Clin. Otolaryngol. 2018, 43, 55–67. [Google Scholar] [CrossRef]
- Kaya, I.; Avcı, B.; Şahin, F.F.; Özateş, N.P.; Sezgin, B.; Kurt, C.; Bilgen, C.; Kirazlı, T. Evaluation of significant gene expression changes in congenital and acquired cholesteatoma. Mol. Biol. Rep. 2020, 47, 6127–6133. [Google Scholar] [CrossRef]
- Kan, T.; Ueda, H.; Takahara, H.; Tsuchiya, Y.; Kishimoto, M.; Uchida, Y.; Ogawa, T.; Ohashi, W.; Tsuzuki, T.; Fujimoto, Y. Association of Matrix Metalloproteinase-2 mRNA Expression with Subtypes of Pediatric Cholesteatoma. BioMed Res. Int. 2021, 2021, 6644897. [Google Scholar] [CrossRef]
- Maniu, A.; Harabagiu, O.; Perde Schrepler, M.; Cătană, A.; Fănuţă, B.; Mogoantă, C.A. Molecular biology of cholesteatoma. Rom. J. Morphol. Embryol. 2014, 55, 7–13. [Google Scholar]
- Aimi, K. Role of the tympanic ring in the pathogenesis of congenital cholesteatoma. Laryngoscope 1983, 93, 1140–1146. [Google Scholar] [CrossRef]
- Michaels, L. An epidermoid formation in the developing middle ear: Possible source of cholesteatoma. J. Otolaryngol. 1986, 15, 169–174. [Google Scholar]
- Michaels, L. Origin of congenital cholesteatoma from a normally occurring epidermoid rest in the developing middle ear. Int. J. Pediatr. Otorhinolaryngol. 1988, 15, 51–65. [Google Scholar] [CrossRef]
- Kodama, K.; Hara, M.; Hasegawa, M.; Matsuzawa, S.; Shinnabe, M.; Kanazawa, H.; Yoshida, N.; Iino, Y. Two cases of spontaneous regression of congenital cholesteatomas. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto-Fukuda, T.; Aoki, D.; Hishikawa, Y.; Kobayashi, T.; Takahashi, H.; Koji, T. Possible involvement of keratinocyte growth factor and its receptor in enhanced epithelial-cell proliferation and acquired recurrence of middle-ear cholesteatoma. Lab. Investig. 2003, 83, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Araz Server, E.; Kalaycık Ertugay, Ç.; Baykal Koca, S.; Longur, E.S.; Yiğit, Ö.; Demirhan, H.; Çakır, Y. Predictive Role of Ki-67 and Proliferative-Cell Nuclear Antigen (PCNA) in Recurrent Cholesteatoma. J. Int. Adv. Otol. 2019, 15, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Palkó, E.; Póliska, S.; Sziklai, I.; Penyige, A. Analysis of KRT1, KRT10, KRT19, TP53 and MMP9 expression in pediatric and adult cholesteatoma. PLoS ONE 2018, 13, e0200840. [Google Scholar] [CrossRef] [PubMed]
- Si, Y.; Chen, Y.B.; Chen, S.J.; Zheng, Y.Q.; Liu, X.; Liu, Y.; Jiang, H.L.; Xu, G.; Li, Z.H.; Huang, Q.H.; et al. TLR4 drives the pathogenesis of acquired cholesteatoma by promoting local inflammation and bone destruction. Sci. Rep. 2015, 5, 16683. [Google Scholar] [CrossRef]
- Imai, R.; Sato, T.; Iwamoto, Y.; Hanada, Y.; Terao, M.; Ohta, Y.; Osaki, Y.; Imai, T.; Morihana, T.; Okazaki, S.; et al. Osteoclasts Modulate Bone Erosion in Cholesteatoma via RANKL Signaling. J. Assoc. Res. Otolaryngol. 2019, 20, 449–459. [Google Scholar] [CrossRef]
- Wu, Y.; Tang, X.; Shao, W.; Lu, Y. Effect of CT manifestations of cholesteatoma on MMP-2, MMP-9 and IL-6 in the serum of patients. Exp. Ther. Med. 2019, 17, 4441–4446. [Google Scholar] [CrossRef]
- Haruyama, T.; Furukawa, M.; Kusunoki, T.; Onoda, J.; Ikeda, K. Expression of IL-17 and its role in bone destruction in human middle ear cholesteatoma. ORL J. Otorhinolaryngol. Relat. Spec. 2010, 72, 325–331. [Google Scholar] [CrossRef]
- Artono; Surarto, B.; Purnami, N.; Hutahaen, F.; Mahardhika, M.R. The Association of IL-1 Alpha Level and TNF Alpha Expressions on Bone Destruction in Chronic Suppurative Otitis Media and Cholesteatoma. Indian J. Otolaryngol. Head Neck Surg. 2020, 72, 1–7. [Google Scholar] [CrossRef]
- Choufani, G.; Ghanooni, R.; Decaestecker, C.; Delbrouck, K.; Simon, P.; Schüring, M.P.; Zick, Y.; Hassid, S.; Gabius, H.J.; Kiss, R. Detection of macrophage migration inhibitory factor (MIF) in human cholesteatomas and functional implications of correlations to recurrence status and to expression of matrix metalloproteinases-3/9, retinoic acid receptor-beta, and anti-apoptotic galectin-3. Laryngoscope 2001, 111, 1656–1662. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Perlikos, F.; Hillas, G.; Loukides, S. Phenotyping and Endotyping Asthma Based on Biomarkers. Curr. Top. Med. Chem. 2016, 16, 1582–1586. [Google Scholar] [CrossRef] [PubMed]
- Teitelbaum, S.L.; Ross, F.P. Genetic regulation of osteoclast development and function. Nat. Rev. Genet. 2003, 4, 638–649. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.W.; Cho, M.L.; Lee, S.H.; Oh, H.J.; Kang, C.M.; Ju, J.H.; Min, S.Y.; Cho, Y.G.; Park, S.H.; Kim, H.Y. Human rheumatoid synovial fibroblasts promote osteoclastogenic activity by activating RANKL via TLR-2 and TLR-4 activation. Immunol. Lett. 2007, 110, 54–64. [Google Scholar] [CrossRef]
- Lundy, S.K.; Sarkar, S.; Tesmer, L.A.; Fox, D.A. Cells of the synovium in rheumatoid arthritis. T lymphocytes. Arthritis Res. Ther. 2007, 9, 202. [Google Scholar] [CrossRef][Green Version]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J. Executive summary of EPOS 2020 including integrated care pathways. Rhinology 2020, 58, 82–111. [Google Scholar] [CrossRef]
- Suchozebrska-Jesionek, D.; Szymański, M.; Kurzepa, J.; Gołabek, W.; Stryjecka-Zimmer, M. Gelatinolytic activity of matrix metalloproteinases 2 and 9 in middle ear cholesteatoma. J. Otolaryngol. Head Neck Surg. 2008, 37, 628–632. [Google Scholar]
- Wang, L.F.; Chien, C.Y.; Tai, C.F.; Kuo, W.R.; His, E.; Juo, S.H. Matrix metalloproteinase-9 gene polymorphisms in nasal polyposis. BMC Med. Genet. 2010, 11, 85. [Google Scholar] [CrossRef]
- Rysz, J.; Banach, M.; Stolarek, R.A.; Pasnik, J.; Cialkowska-Rysz, A.; Koktysz, R.; Piechota, M.; Baj, Z. Serum matrix metalloproteinases MMP-2 and MMP-9 and metalloproteinase tissue inhibitors TIMP-1 and TIMP-2 in diabetic nephropathy. J. Nephrol. 2007, 20, 444–452. [Google Scholar]
- Yamamoto-Fukuda, T.; Akiyama, N.; Tatsumi, N.; Okabe, M.; Kojima, H. Menin-MLL inhibitor blocks progression of middle ear cholesteatoma in vivo. Int. J. Pediatr. Otorhinolaryngol. 2021, 140, 110545. [Google Scholar] [CrossRef]
- Agache, I.; Akdis, C.A. Endotypes of allergic diseases and asthma: An important step in building blocks for the future of precision medicine. Allergol. Int. 2016, 65, 243–252. [Google Scholar] [CrossRef] [PubMed]
- De Corso, E.; Montuori, C.; Settimi, S.; Mele, D.A.; Cantiani, A.; Corbò, M.; Cantone, E.; Paludetti, G.; Galli, J. Efficacy of Biologics on Refractory Eosinophilic Otitis Media Associated with Bronchial Asthma or Severe Uncontrolled CRSwNP. J. Clin. Med. 2022, 11, 926. [Google Scholar] [CrossRef] [PubMed]
- Lou, H.; Wang, C.; Zhang, L. Endotype-driven precision medicine in chronic rhinosinusitis. Expert Rev. Clin. Immunol. 2019, 15, 1171–1183. [Google Scholar] [CrossRef] [PubMed]
- Passalacqua, G.; Ciprandi, G.; Canonica, G.W. The nose-lung interaction in allergic rhinitis and asthma: United airways disease. Curr. Opin. Allergy Clin. Immunol. 2001, 1, 7–13. [Google Scholar] [CrossRef]
- Kuo, C.L.; Yen, Y.C.; Chang, W.P.; Shiao, A.S. Association Between Middle Ear Cholesteatoma and Chronic Rhinosinusitis. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 757–763. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Manoukian, J.J.; Sobol, S.E.; Tewfik, T.L.; Mazer, B.D.; Schloss, M.D.; Taha, R.; Hamid, Q.A. Similar allergic inflammation in the middle ear and the upper airway: Evidence linking otitis media with effusion to the united airways concept. J. Allergy Clin. Immunol. 2004, 114, 1110–1115. [Google Scholar] [CrossRef]


{kind=link}
| Author Year Ref. | N. of Cases (Sex; Mean Age) | Methods | Sample Type | Analytical Technique | Relevant Results | Recurrence | Bone Erosion |
|---|---|---|---|---|---|---|---|
| Yamamoto-Fukuda et al. 2003 [14] | A total of 56 cases (32 M, 24 F; mean age:35) | Expression of KGF, KGFR, Ki-67 | Soft tissue | Immunohistochemical analysis and electroporatically transfection to the mice ears | KGF were detected in 80% of C, KGFR in 72%. Higher Ki-67 labeling index (66%) in KGF+/KGFR+ cases than other cases. Correlation between KGF+/KGFR+ expression and recurrence. | Y | |
| Araz Server et al. 2019 [15] | A total of 43 cases (29 M, 14 F; mean age: 33) | Two groups: recurrent (21 patients) and non-recurrent within 2 years (22 patients). Ki-67 and the percentages of stained cells were calculated. | Bone tissue | Immunohistochemical analysis | A significant relationship between Ki-67 staining and malleus involvement | Y | |
| Palkó et al. 2018 [16] | A total of 26, 15 children and 11 adult (16 M, 11 F; mean age 23,4) | The expression of three cytokeratin genes (KRT1, KRT10 and KRT19), the matrix metalloproteinase 9 gene (MMP9) and the tumor suppressor TP53 gene was measured by qRT-PCR in surgical samples of cholesteatoma (C) cases and their expression level was compared to that of normal skin samples | Soft tissue | mRNA expression | Results showed identical expression pattern for KRT1 and KRT10, their expression was higher in pediatric cases than in adults, especially in pediatric recurrent samples. The expression level of KRT19 was lower in the more invasive recurrent cases both in our pediatric and adult groups. expression of MMP9 was highest in adult recurrent cases | Y | |
| Si et al. 2015 [17] | A total of 187 specimens of acquired cholesteatoma (137 F and 51 M, mean age: 45) | Immunohistochemical analysis of TLR4 expression was performed in cholesteatoma specimen. | Congenital cholesteatomas and acquired cholesteatomas samples | Real-timePCR, Western blotting, and immunohistochemistry. Animal models | The number of TLR4-positive cells increased with an increased degree of cholesteatoma invasion, bone destruction, and hearing loss | Y | |
| Imai et al. 2019 [18] | A total of 24 cholesteatoma specimens from patients who underwent tympanomastoidectomy. | Osteoclasts were stained using tartrate-resistant acid phosphatase (TRAP)-hematoxylin counterstaining. The expression of RANKL mRNA was performed with the droplet digital polymerase chain reaction (ddPCR) system. | Bone-soft tissues | Immunohistochemistry, RNA Sequencing and ELISA | The number of osteoclasts on the bone surface adjacent to C was significantly larger than on the surface of control bone. The expression of RANKL mRNA was significantly higher in cholesteatomas than in control skin. RANKL was expressed in fibroblasts in the cholesteatoma perimatrix. | Y | |
| Wu et al. 2019 [19] | A total of 176 patients (91 M and 85 F, mean age 49, 65 ± 5, 27 with cholesteatomatous otitis media | The expression levels of MMP-2, MMP-9 and IL-6 in the serum of the selected patients were detected by ELISA | Serum | ELISA | MMP-2, MMP-9 and IL-6 were higly expressed in the serum of patients with C compared to the control group and were positively correlated with CT manifestations of the patients and the injury degree of ossicle, which may be a sign of poor prognosis of cholesteatomatous otitis media (COM). | Y | |
| Haruyama et al. 2010 [20] | Tissue specimens collected from 24 patients with cholesteatomas (16 M and 8 F, mean age: 44); congenital in 8 patients and acquired in 16 patients. | The expression and localization of IL17 and RANKL were examined by immunohistochemistry in tissue specimens. The cellular sources of IL-17 were assessed by double immunofluorescent staining with CD4. The level of IL-17 protein was determined using an enzyme-linked immunosorbent assay. The degree of bone destruction was compared with the IL-17 immunoreactivity | Cholesteatoma tissue | Immunohistochemistry | IL-17-positive inflammatory cells were seen in the subepithelial granulation tissue but not in the epithelium of the C. The localization of IL-17 expression coincided with CD4-positive lymphocytes. The subepithelial granulation had RANKL positive infiltrating cells and a significant correlation between IL-17- and RANKL-positive cells in the same specimens was recognized. The degree of bone destruction was dependent on the number of IL-17-positive cells that infiltrated the cholesteatoma. | Y | |
| Artono et al. 2019 [21] | A total of 46 patients (26 M and 20 F, age range of 21–30 years) with chronic suppurative otitis media (CSOM) with cholesteatoma | Pathological tissue in the form of cholesteatoma tissue and external acustic meatus skin during surgery was assessed. IL-1a expression was assessed by using ELISA. TNF-a expression was determined by immunohistochemical staining. | Cholesteatoma tissue | ELISA | There is a significant association between expression of TNF-a and IL-1a level on the severity of bone destruction in CSOM and C patients | Y | |
| Choufani et al. 2001 [22] | A total of 56 C specimens (33 M and 23 F), and 5 congenital and 51 acquired cases. | The immunohistochemical levels of expression of macrophage migration inhibitory factor (MIF) was statistically correlated to parameters of the other markers (galectin 1, -3, and -8, retinoid acid receptors (RAR) binding sites for sarcolectin, and invasion markers (cathepsins -B and -D, and matrix metalloproteinases [MMP]-2, -3, and -9) | Cholesteatoma tissue | Immunohistochemistry | MIF expression is higher in recurrent than in nonrecurrent cholesteatomas. MIF expression in infected ones it is correlated to MMP-3 and galectin-3 expression. | Y |
| Molecular Biomarkers | |
|---|---|
| KGF-KGFR | Yamamoto et al. 2003 [14] |
| MMP-9 | Palkó et al. 2018 [16] |
| KRT-1 | Palkó et al. 2018 [16] |
| KRT-10 | Palkó et al. 2018 [16] |
| MIF | Choufani et al. 2001 [22] |
| Molecular Biomarkers | |
|---|---|
| Ki-67 | Araz-Server et al. 2019 [15] |
| TLR-4 | Si et al. 2015 [17] |
| RANKL | Imai et al. 2019 [18] |
| IL-17 | Haruyama et al. 2010 [20] |
| MMP-2 (serum) | Wu et al. 2019 [19] |
| MMP-9 (serum) | Wu et al. 2019 [19] |
| IL-6 (serum) | Wu et al. 2019 [19] |
| TNF-α | Artono et al. 2019 [21] |
| IL-1α | Artono et al. 2019 [21] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantone, E.; Di Nola, C.; De Corso, E.; Cavaliere, M.; Grimaldi, G.; Fetoni, A.R.; Motta, G. Endotyping of Cholesteatoma: Which Molecular Biomarkers? A Systematic Review. J. Pers. Med. 2022, 12, 1347. https://doi.org/10.3390/jpm12081347
Cantone E, Di Nola C, De Corso E, Cavaliere M, Grimaldi G, Fetoni AR, Motta G. Endotyping of Cholesteatoma: Which Molecular Biomarkers? A Systematic Review. Journal of Personalized Medicine. 2022; 12(8):1347. https://doi.org/10.3390/jpm12081347
Chicago/Turabian StyleCantone, Elena, Claudio Di Nola, Eugenio De Corso, Michele Cavaliere, Giusi Grimaldi, Anna Rita Fetoni, and Gaetano Motta. 2022. "Endotyping of Cholesteatoma: Which Molecular Biomarkers? A Systematic Review" Journal of Personalized Medicine 12, no. 8: 1347. https://doi.org/10.3390/jpm12081347
APA StyleCantone, E., Di Nola, C., De Corso, E., Cavaliere, M., Grimaldi, G., Fetoni, A. R., & Motta, G. (2022). Endotyping of Cholesteatoma: Which Molecular Biomarkers? A Systematic Review. Journal of Personalized Medicine, 12(8), 1347. https://doi.org/10.3390/jpm12081347