
What’s in a Name? Parents’ and Healthcare Professionals’ Preferred Terminology for Pathogenic Variants in Childhood Cancer Predisposition Genes

 ,
,  , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
- What term do parents with a child with cancer prefer to describe P/LP variants in cancer predisposition genes in children, and why?
- What term do genetics health professionals prefer within the childhood cancer setting, and why?
- What term do pediatric oncologists prefer, and why?
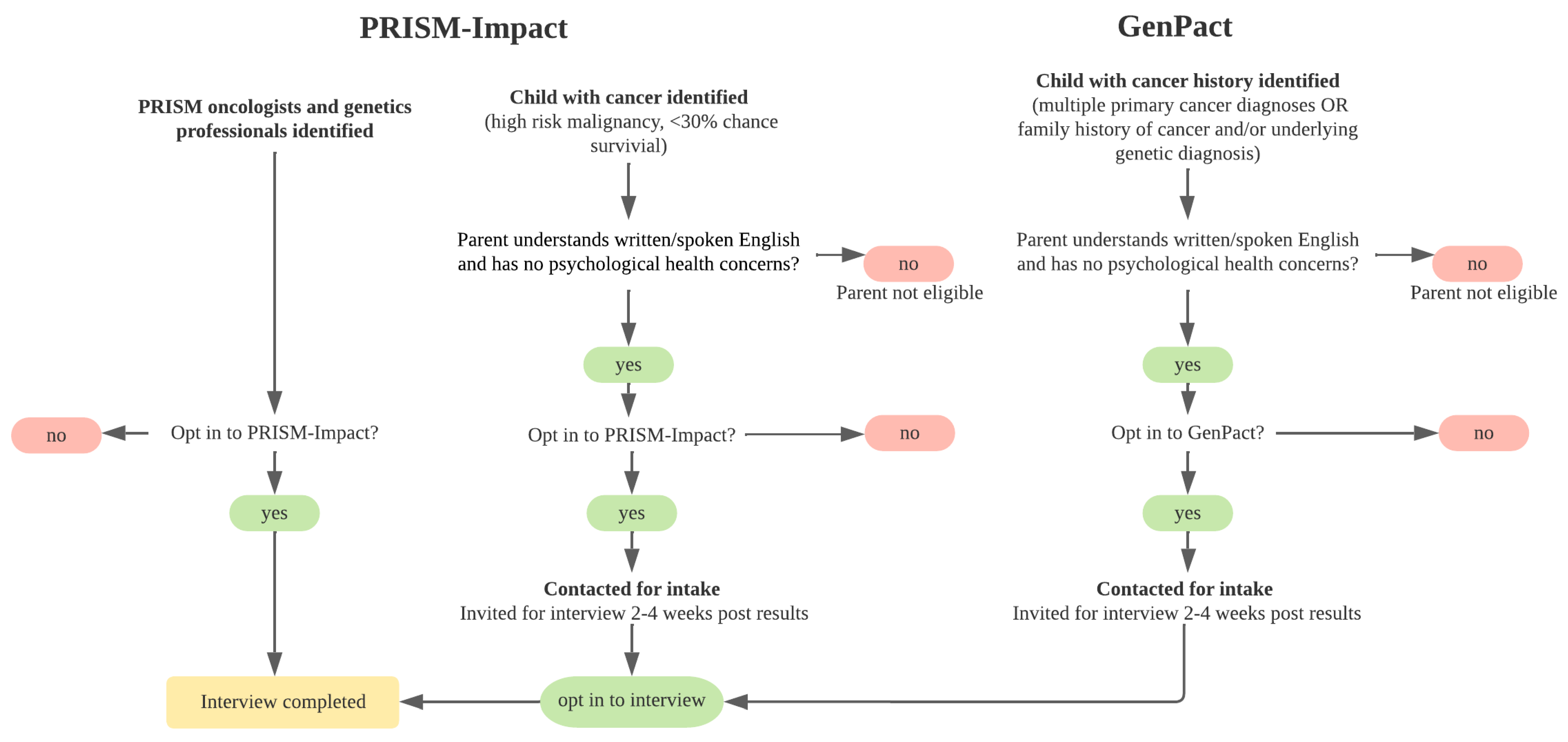
2. Materials and Methods
3. Results
3.1. Participants
3.2. Parents’ Naming Preferences
“I think that’s probably the easiest to understand. Plus, probably not as traumatic sounding.”(mother aged 42, child with central nervous system tumor)
“(Genetic variant) sounds like it’s OK like it’s not …as harsh.”(mother aged 45, child with central nervous system tumor)
“Not faulty. I must have spent one whole month not sleeping properly thinking how and why [my child got cancer]… so fault would probably just add another pile of extra stuff to the plate.”(father aged 49, child with sarcoma)
“They were very explicit when talking to [child’s name] that…you haven’t done anything bad. They never wanted him to think he had done anything wrong to cause this happening…that sat with me… I don’t like the use of a word that would imply that the person themselves caused that problem to occur.”(mother aged 44, child with retinoblastoma)
“[Genetic variant]… I know what it means, but I’ve also come across lots of families in wards that are ESL [English as a second language], such as my husband…those terms are too scientific for him to really grasp what you mean.”(mother aged 35, child with Wilms tumor)
3.3. Genetics Professionals’ Naming Preferences
“If you want to make it very clear that it’s a pathogenic variant, a disease-causing variant rather than a change, a fault indicates that it’s incorrect.”(genetic counselor, years practice unknown)
“You just have to take it on an individual basis because by the time he got to us he knew there was a gene fault in the family.”(clinical geneticist, 25 years practice)
“I will tend to adapt my language with what I hear the patients saying back to me.”(genetic counselor, 12 years practice)
3.4. Pediatric Oncologists’ Naming Preferences
“I think the most broadly encompassing term would be a genetic variant, one because it describes change in itself, and not necessarily what its implications might be.”(pediatric oncologist, 9 years practice)
“I use the word altered. Because I don’t see it as faulty. It’s faulty from the point of view of what it may cause, but it may protect you against something else which I don’t understand.”(pediatric oncologist, 10 years practice)
“It sounds very negative…without proper explanation and genetic counseling…it could cause a lot of anxiety, until they are explained what it actually means.”(pediatric oncologist, 14 years practice)
“Telling somebody to their face that you’ve got a faulty gene puts a whole heap of guilt on them…one of the things that comes up particularly when you start talking about hereditary cancer is that I think a lot of parents will take on the guilt that I did this. It’s my fault.”(pediatric oncologist, 21 years practice)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gröbner, S.N.; Worst, B.C.; Weischenfeldt, J.; Buchhalter, I.; Kleinheinz, K.; Rudneva, V.A.; Johann, P.D.; Balasubramanian, G.P.; Segura-Wang, M.; Brabetz, S.; et al. The landscape of genomic alterations across childhood cancers. Nature 2018, 555, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.; Mayoh, C.; Lau, L.M.S.; Khuong-Quang, D.-A.; Pinese, M.; Kumar, A.; Barahona, P.; Wilkie, E.E.; Sullivan, P.; Bowen-James, R.; et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat. Med. 2020, 26, 1742–1753. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Walsh, M.F.; Wu, G.; Edmonson, M.N.; Gruber, T.A.; Easton, J.; Hedges, D.; Ma, X.; Zhou, X.; Yergeau, D.A.; et al. Germline mutations in predisposition genes in pediatric cancer. N. Engl. J. Med. 2015, 373, 2336–2346. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. Genome sequencing of children promises a new era in oncology. Br. Med. J. (Clin. Res. Ed.) 2019, 364, l105. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.A.; Vundamati, D.S.; Farooqi, M.S.; Guest, E. Precision medicine in pediatric cancer: Current applications and future prospects. High-Throughput 2018, 7, 39. [Google Scholar] [CrossRef]
- Freedman, A.N.; Klabunde, C.N.; Wiant, K.; Enewold, L.; Gray, S.W.; Filipski, K.K.; Keating, N.L.; Leonard, D.G.B.; Lively, T.; McNeel, T.S.; et al. Use of next-generation sequencing tests to guide cancer treatment: Results from a nationally representative survey of oncologists in the united states. JCO Precis. Oncol. 2018, 2, 1–13. [Google Scholar] [CrossRef]
- Rahner, N.; Steinke, V. Hereditary cancer syndromes. Dtsch. Arztebl. Int. 2008, 105, 706–714. [Google Scholar] [CrossRef]
- Thiele, C.J.; Cohn, S.L. Genetically informed therapies—A “gift” for children with cancer. Clin. Cancer Res. 2012, 18, 2735–2739. [Google Scholar] [CrossRef]
- Villani, A.; Shore, A.; Wasserman, J.D.; Stephens, D.; Kim, R.H.; Druker, H.; Gallinger, B.; Naumer, A.; Kohlmann, W.; Novokmet, A.; et al. Biochemical and imaging surveillance in germline tp53 mutation carriers with li-fraumeni syndrome: 11 year follow-up of a prospective observational study. Lancet Oncol. 2016, 17, 1295–1305. [Google Scholar] [CrossRef]
- Joseph, L.; Cankovic, M.; Caughron, S.; Chandra, P.; Emmadi, R.; Hagenkord, J.; Hallam, S.; Jewell, K.E.; Klein, R.D.; Pratt, V.M.; et al. The spectrum of clinical utilities in molecular pathology testing procedures for inherited conditions and cancer: A report of the association for molecular pathology. J. Mol. Diagn. 2016, 18, 605–619. [Google Scholar] [CrossRef]
- Oberg, J.A.; Glade Bender, J.L.; Sulis, M.L.; Pendrick, D.; Sireci, A.N.; Hsiao, S.J.; Turk, A.T.; Dela Cruz, F.S.; Hibshoosh, H.; Remotti, H.; et al. Implementation of next generation sequencing into pediatric hematology-oncology practice: Moving beyond actionable alterations. Genome Med. 2016, 8, 133. [Google Scholar] [CrossRef] [PubMed]
- Cotton, R.; Scriver, C. Proof of “disease causing” mutation. Hum. Mutat. 1998, 12, 1–3. [Google Scholar] [CrossRef]
- Condit, C.M.; Achter, P.J.; Lauer, I.; Sefcovic, E. The changing meanings of “mutation:” A contextualized study of public discourse. Hum. Mutat. 2002, 19, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Jarvik, G.P.; Evans, J.P. Mastering genomic terminology. Genet. Med. 2017, 19, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Cutting, G.R. Annotating DNA variants is the next major goal for human genetics. Am. J. Hum. Genet. 2014, 94, 5–10. [Google Scholar] [CrossRef]
- Marshall, J.H. On the changing meanings of “mutation”. Hum. Mutat. 2002, 19, 76–78. [Google Scholar] [CrossRef]
- Abramsky, L.; Fletcher, O. Interpreting information: What is said, what is heard—A questionnaire study of health professionals and members of the public. Prenat. Diagn. 2002, 22, 1188–1194. [Google Scholar] [CrossRef]
- Ando, N.; Iwamitsu, Y.; Takemura, K.; Saito, Y.; Takada, F. Perceptions of the concept of mutation among family members of patients receiving outpatient genetic services and university students. J. Genet. Couns. 2009, 18, 567. [Google Scholar] [CrossRef]
- Ando, N.; Saito, Y.; Takemura, K.; Takada, F.; Iwamitsu, Y. Knowledge and impressions regarding the concept of mutation among japanese university students. Clin. Genet. 2008, 74, 75–81. [Google Scholar] [CrossRef]
- Condit, C.M.; Dubriwny, T.; Lynch, J.; Parrott, R. Lay people’s understanding of and preference against the word “mutation”. Am. J. Med. Genet. A 2004, 130, 245–250. [Google Scholar] [CrossRef]
- Hodgson, J.; Hughes, E.; Lambert, C. “Slang”—Sensitive language and the new genetics—An exploratory study. J. Genet. Couns. 2005, 14, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Melas, P.A.; Georgsson Öhman, S.; Juth, N.; Bui, T.-H. Information related to prenatal genetic counseling: Interpretation by adolescents, effects on risk perception and ethical implications. J. Genet. Couns. 2012, 21, 536–546. [Google Scholar] [CrossRef] [PubMed]
- Marron, J.M.; Dizon, D.S.; Symington, B.; Thompson, M.A.; Rosenberg, A.R. Waging war on war metaphors in cancer and covid-19. JCO Oncol. Pract. 2020, 16, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.A.; Sharp, R.R.; Aufox, S.A.; Bland, S.T.; Blout, C.; Bowen, D.J.; Buchanan, A.H.; Halverson, C.; Harr, M.; Hebbring, S.J.; et al. Understanding the return of genomic sequencing results process: Content review of participant summary letters in the emerge research network. J. Pers. Med. 2020, 10, 38. [Google Scholar] [CrossRef]
- Wakefield, C.; Juan, A.; Kasparian, N. Men at increased risk of developing breast cancer: Language preferences for naming a cancer-related mutation. Genet. Test. Mol. Biomark. 2009, 13, 395–398. [Google Scholar] [CrossRef]
- Wakefield, C.; Meiser, B.; Homewood, J.; Barlow-Stewart, K.; Tucker, K. A comparison of community, clinician, and patient preferences for naming a cancer-related mutation. Clin. Genet. 2007, 71, 140–147. [Google Scholar] [CrossRef]
- Cotton, R.G.H. Communicating “mutation:” modern meanings and connotations. Hum. Mutat. 2002, 19, 2–3. [Google Scholar] [CrossRef]
- Den Dunnen, J.T.; Dalgleish, R.; Maglott, D.R.; Hart, R.K.; Greenblatt, M.S.; McGowan-Jordan, J.; Roux, A.-F.; Smith, T.; Antonarakis, S.E.; Taschner, P.E.M. Hgvs recommendations for the description of sequence variants: 2016 update. Hum. Mutat. 2016, 37, 564–569. [Google Scholar] [CrossRef]
- Plon, S.E.; Eccles, D.M.; Easton, D.; Foulkes, W.D.; Genuardi, M.; Greenblatt, M.S.; Hogervorst, F.B.; Hoogerbrugge, N.; Spurdle, A.B.; Tavtigian, S.V. Sequence variant classification and reporting: Recommendations for improving the interpretation of cancer susceptibility genetic test results. Hum. Mutat. 2008, 29, 1282–1291. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the american college of medical genetics and genomics and the association for molecular pathology. Genet. Med. Off. J. Am. Coll. Med. Genet. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Spurdle, A.B.; Greville-Heygate, S.; Antoniou, A.C.; Brown, M.; Burke, L.; de la Hoya, M.; Domchek, S.; Dörk, T.; Firth, H.V.; Monteiro, A.N.; et al. Towards controlled terminology for reporting germline cancer susceptibility variants: An enigma report. J. Med. Genet. 2019, 56, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Jamal, L.; Schupmann, W.; Berkman, B.E. An ethical framework for genetic counseling in the genomic era. J. Genet. Couns. 2020, 29, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Assarroudi, A.; Heshmati Nabavi, F.; Armat, M.R.; Ebadi, A.; Vaismoradi, M. Directed qualitative content analysis: The description and elaboration of its underpinning methods and data analysis process. J. Res. Nurs. 2018, 23, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Gibbins, J.; Steinhardt, K.; Beinart, H. A systematic review of qualitative studies exploring the experience of parents whose child is diagnosed and treated for cancer. J. Pediatric Oncol. Nurs. 2012, 29, 253–271. [Google Scholar] [CrossRef] [PubMed]
- Hallowell, N.; Arden-Jones, A.; Eeles, R.; Foster, C.; Lucassen, A.; Moynihan, C.; Watson, M. Guilt, blame and responsibility: Men’s understanding of their role in the transmission of brca1/2 mutations within their family. Sociol. Health Illn. 2006, 28, 969–988. [Google Scholar] [CrossRef]
- Kasparian, N.A.; Rutstein, A.; Sansom-Daly, U.M.; Mireskandari, S.; Tyler, J.; Duffy, J.; Tucker, K.M. Through the looking glass: An exploratory study of the lived experiences and unmet needs of families affected by von hippel-lindau disease. Eur. J. Hum. Genet. EJHG 2015, 23, 34–40. [Google Scholar] [CrossRef]
- Cohen, B.; Roth, M.; Marron, J.M.; Gray, S.W.; Geller, D.S.; Hoang, B.; Gorlick, R.; Janeway, K.A.; Gill, J. Pediatric oncology provider views on performing a biopsy of solid tumors in children with relapsed or refractory disease for the purpose of genomic profiling. Ann. Surg. Oncol. 2016, 23, 990–997. [Google Scholar] [CrossRef]
- Johnson, L.M.; Valdez, J.M.; Quinn, E.A.; Sykes, A.D.; McGee, R.B.; Nuccio, R.; Hines-Dowell, S.J.; Baker, J.N.; Kesserwan, C.; Nichols, K.E.; et al. Integrating next-generation sequencing into pediatric oncology practice: An assessment of physician confidence and understanding of clinical genomics. Cancer 2017, 123, 2352–2359. [Google Scholar] [CrossRef]
- McGill, B.C.; Wakefield, C.E.; Hetherington, K.; Munro, L.J.; Warby, M.; Lau, L.; Tyrrell, V.; Ziegler, D.S.; O’Brien, T.A.; Marshall, G.M.; et al. “Balancing expectations with actual realities”: Conversations with clinicians and scientists in the first year of a high-risk childhood cancer precision medicine trial. J. Pers. Med. 2020, 10, 9. [Google Scholar] [CrossRef]
- Fennell, A.P.; Hunter, M.F.; Corboy, G.P. The changing face of clinical genetics service delivery in the era of genomics: A framework for monitoring service delivery and data from a comprehensive metropolitan general genetics service. Genet. Med. 2020, 22, 210–218. [Google Scholar] [CrossRef]
- Hoskovec, J.M.; Bennett, R.L.; Carey, M.E.; DaVanzo, J.E.; Dougherty, M.; Hahn, S.E.; LeRoy, B.S.; O’Neal, S.; Richardson, J.G.; Wicklund, C.A. Projecting the supply and demand for certified genetic counselors: A workforce study. J. Genet. Couns. 2018, 27, 16–20. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | Data |
|---|---|
| Parents | |
| Age, mean (SD), range | 43.5 (4.9), 35–56 |
| Sex, no. (%) | |
| Female | 22 (88.0) |
| Education, no. (%) | |
| Year 12 or below | 2 (8.0) |
| Certificate/Diploma | 8 (32.0) |
| Higher Education | 15 (60.0) |
| Previous genetics education, no. (%) | |
| Yes | 9 (36.0) |
| No | 15 (60.0) |
| Unsure | 1 (4.0) |
| Self-reported perceived genetic knowledge, no. (%) | |
| Below average | 8 (32.0) |
| About average | 12 (48.0) |
| Better than average | 5 (20.0) |
| Religion type, no. (%) | |
| Christian | 13 (52.0) |
| Other religion | 4 (16.0) |
| No religion | 8 (32.0) |
| Cultural background, no. (%) | |
| Western/European | 18 (72.0) |
| Other | 6 (24.0) |
| Missing | 1 (4.0) |
| Research study child enrolled in, no. (%) | |
| PRISM | 21 (84.0) |
| GenSeq | 4 (16.0) |
| Patients | |
| Age at study enrolment, mean (SD), range | 10.4 (4.8), 1–17 |
| Age at diagnosis, mean (SD), range | 9.0 (4.9), 1–16 |
| Time (years) since diagnosis and enrolment, mean (SD), range | 1.4 (2.6), 0–10 |
| Sex, no. (%) | |
| Female | 11 (44.0) |
| Cancer type, no. (%) | |
| Central nervous system | 6 (24.0) |
| Sarcoma | 9 (36.0) |
| Leukemia/Lymphoma | 2 (8.0) |
| Thyroid | 2 (98.0) |
| Other | 6 (24.0) |
| Reportable germline finding identified via research testing, no (%) | |
| No | 22 (88.0) |
| Yes | 3 (12.0) |
| Characteristic | Data |
|---|---|
| Profession, no. (%) | |
| Genetic counselor | 5 (83.3) |
| Clinical geneticist | 1 (16.7) |
| Sex, no. (%) | |
| Female | 6 (100) |
| Age, mean (SD), range (n = 5) | 45.8 (9.9), 38–63 |
| Years of practice in genetics, mean (SD), range (n = 5) | 14.4 (6.3), 10–25 |
| Percentage time dedicated to research, mean (SD), range (n = 5) | 14% (22.7), 2–60 |
| Self-reported formal genetics training, no. (%) | |
| As part of compulsory genetics training only | 5 (83.3) |
| Missing | 1 (16.7) |
| Characteristic | Data |
|---|---|
| Profession, no. (%) | |
| Pediatric oncologist | 29 (100) |
| Sex, no. (%) | |
| Female | 12 (41.4) |
| Age, mean (SD), range | 50.7 (10.5), 25–76 |
| Years of practice in pediatric oncology, mean (SD), range | 19.4 (9.5), 6–40 |
| Percentage time dedicated to research, mean (SD), range | 33.6 (20.6), 5–80 |
| Self-reported formal genetics training, no. (%) | |
| Very little/none | 11 (37.9) |
| As part of compulsory medical training only | 11 (37.9) |
| Additional training (e.g., PhD in genetics) | 7 (24.1) |
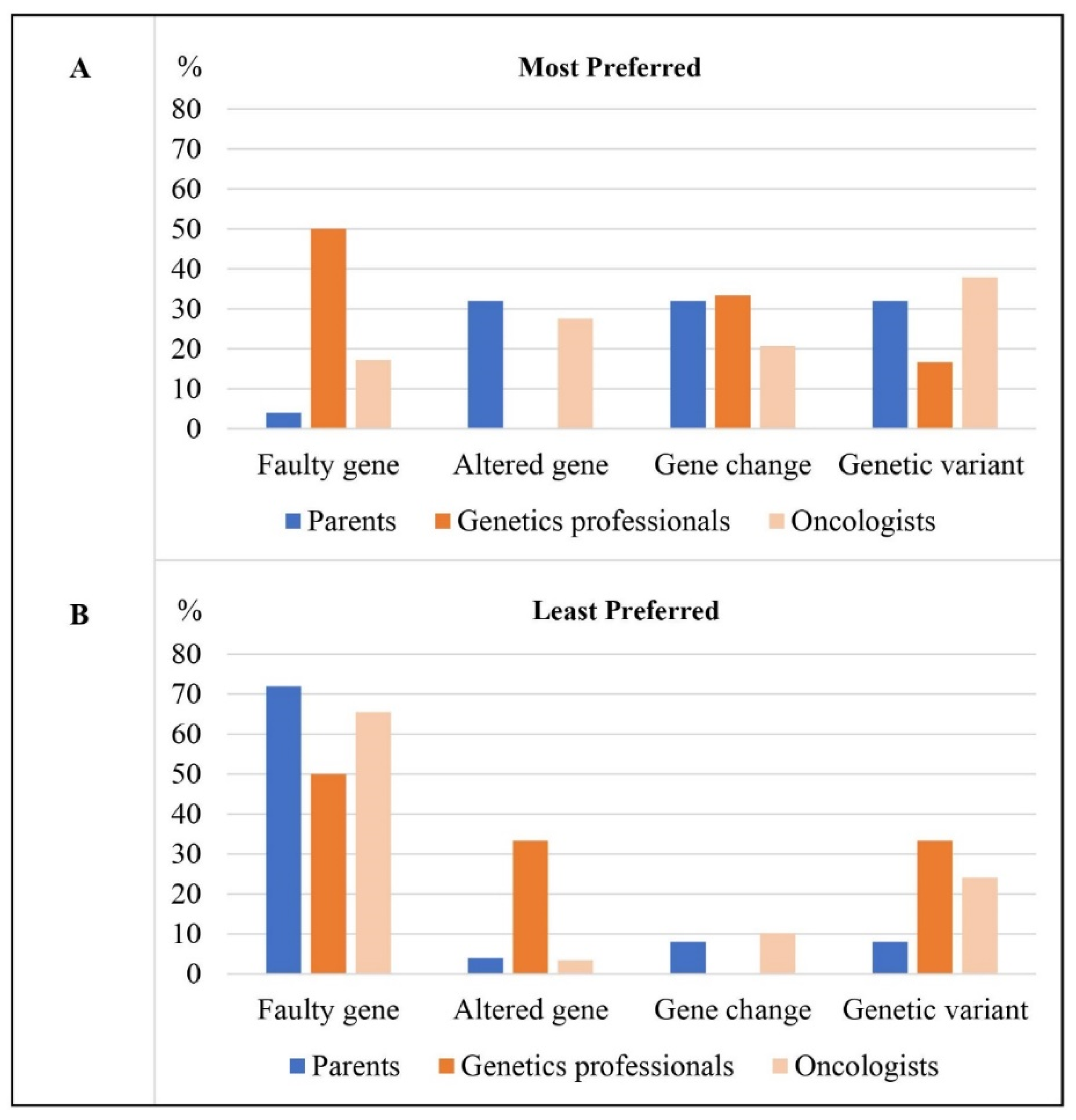
| Term | Preference | Participant Group ** | Pros | Cons | ||
|---|---|---|---|---|---|---|
| Parents | Genetics Professionals | Oncologists | ||||
| Faulty | Most prefer | 1/25 | 3/6 | 5/29 |
|
|
| Least prefer | 18/25 | 3/6 | 19/29 | |||
| Altered gene | Most prefer | 8/25 | 0/6 | 8/29 |
|
|
| Least prefer | 1/25 | 2/6 | 1/29 | |||
| Gene change | Most prefer | 8/25 | 2/6 | 6/29 |
|
|
| Least prefer | 2/25 | 0/6 | 3/29 | |||
| Genetic variant | Most prefer | 8/25 | 1/6 | 11/29 |
|
|
| Least prefer | 2/25 | 2/6 | 7/29 | |||
| None of the above | Most prefer | 2/25 | 0/6 | 0/21 | N/A | N/A |
| Least prefer | 2/25 | 1/6 * | 0/29 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hunter, J.D.; Robertson, E.G.; Hetherington, K.; Ziegler, D.S.; Marshall, G.M.; Kirk, J.; Marron, J.M.; Denburg, A.E.; Barlow-Stewart, K.; Warby, M.; et al. What’s in a Name? Parents’ and Healthcare Professionals’ Preferred Terminology for Pathogenic Variants in Childhood Cancer Predisposition Genes. J. Pers. Med. 2022, 12, 1327. https://doi.org/10.3390/jpm12081327
Hunter JD, Robertson EG, Hetherington K, Ziegler DS, Marshall GM, Kirk J, Marron JM, Denburg AE, Barlow-Stewart K, Warby M, et al. What’s in a Name? Parents’ and Healthcare Professionals’ Preferred Terminology for Pathogenic Variants in Childhood Cancer Predisposition Genes. Journal of Personalized Medicine. 2022; 12(8):1327. https://doi.org/10.3390/jpm12081327
Chicago/Turabian StyleHunter, Jacqueline D., Eden G. Robertson, Kate Hetherington, David S. Ziegler, Glenn M. Marshall, Judy Kirk, Jonathan M. Marron, Avram E. Denburg, Kristine Barlow-Stewart, Meera Warby, and et al. 2022. "What’s in a Name? Parents’ and Healthcare Professionals’ Preferred Terminology for Pathogenic Variants in Childhood Cancer Predisposition Genes" Journal of Personalized Medicine 12, no. 8: 1327. https://doi.org/10.3390/jpm12081327
APA StyleHunter, J. D., Robertson, E. G., Hetherington, K., Ziegler, D. S., Marshall, G. M., Kirk, J., Marron, J. M., Denburg, A. E., Barlow-Stewart, K., Warby, M., Tucker, K. M., Lee, B. M., O’Brien, T. A., & Wakefield, C. E. (2022). What’s in a Name? Parents’ and Healthcare Professionals’ Preferred Terminology for Pathogenic Variants in Childhood Cancer Predisposition Genes. Journal of Personalized Medicine, 12(8), 1327. https://doi.org/10.3390/jpm12081327