
Standardized Rehabilitation or Individual Approach?—A Retrospective Analysis of Early Rehabilitation Protocols after Isolated Posterior Cruciate Ligament Reconstruction

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Algorithm of Evaluation
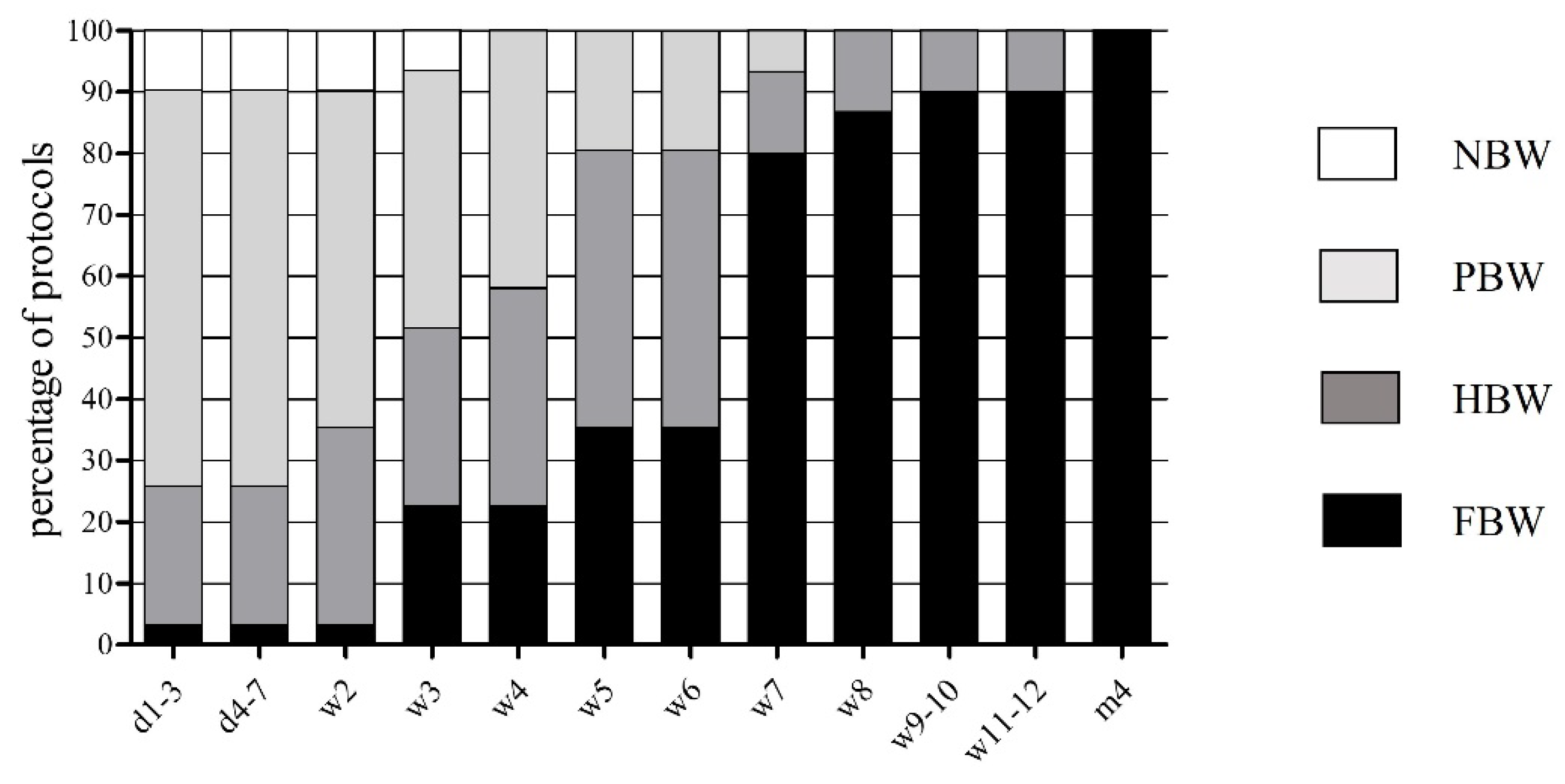
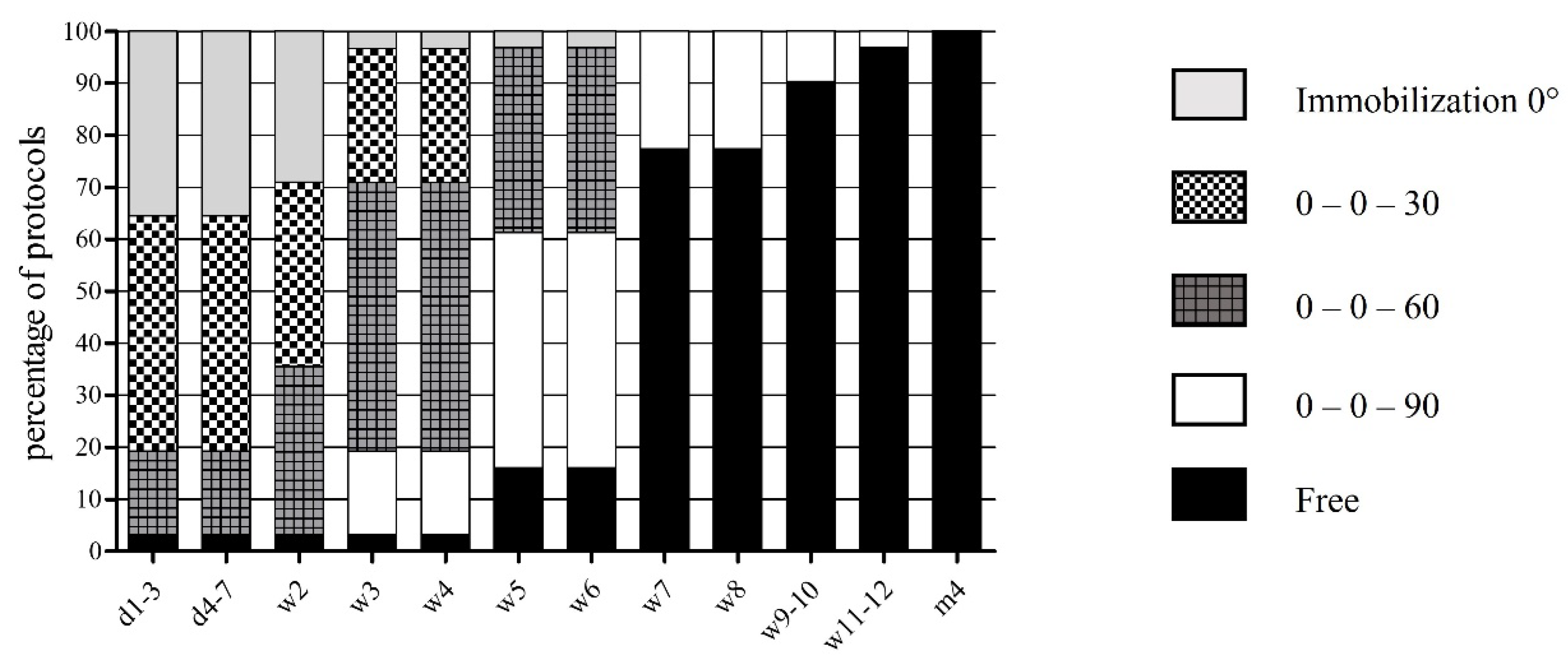
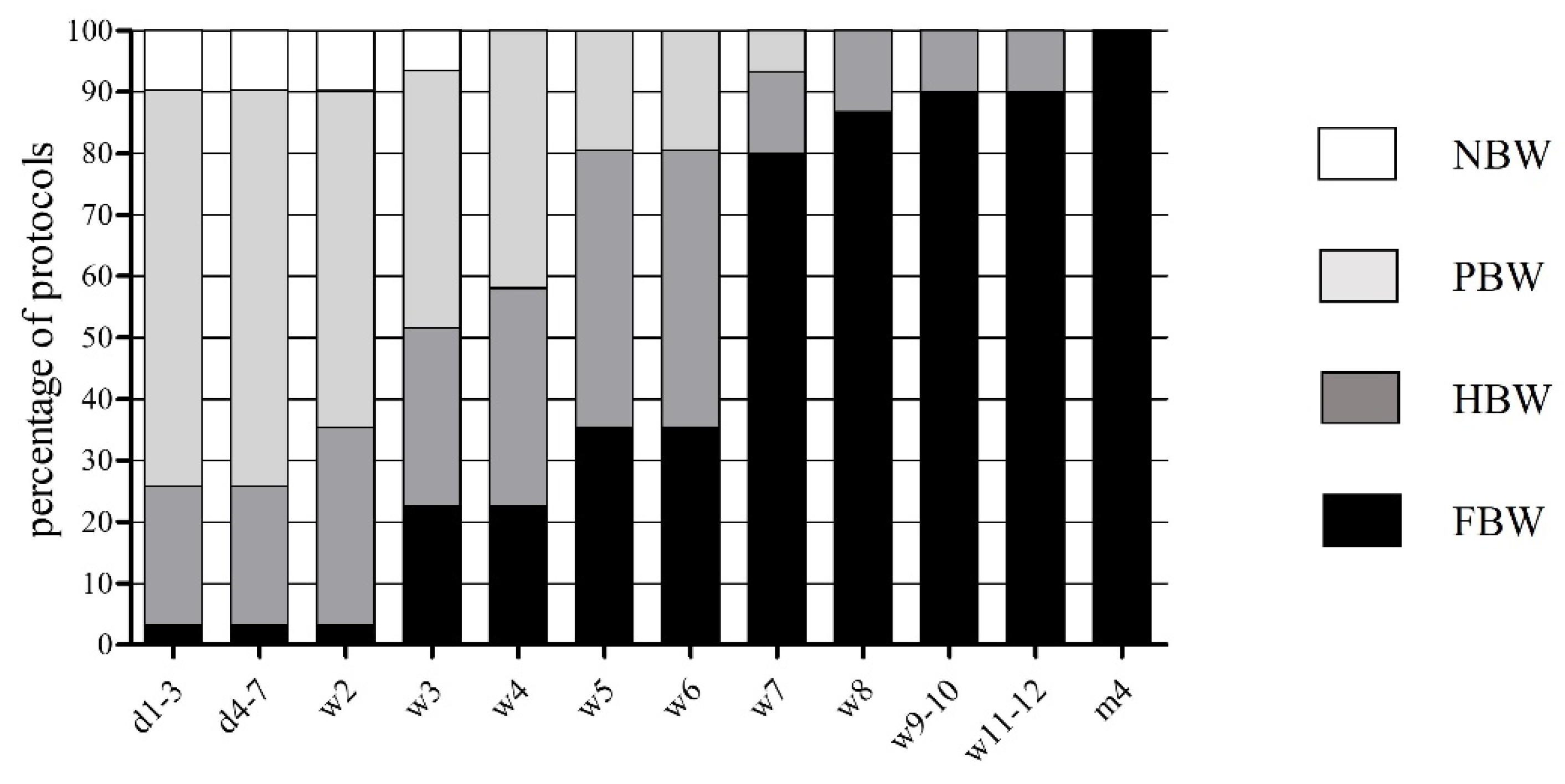
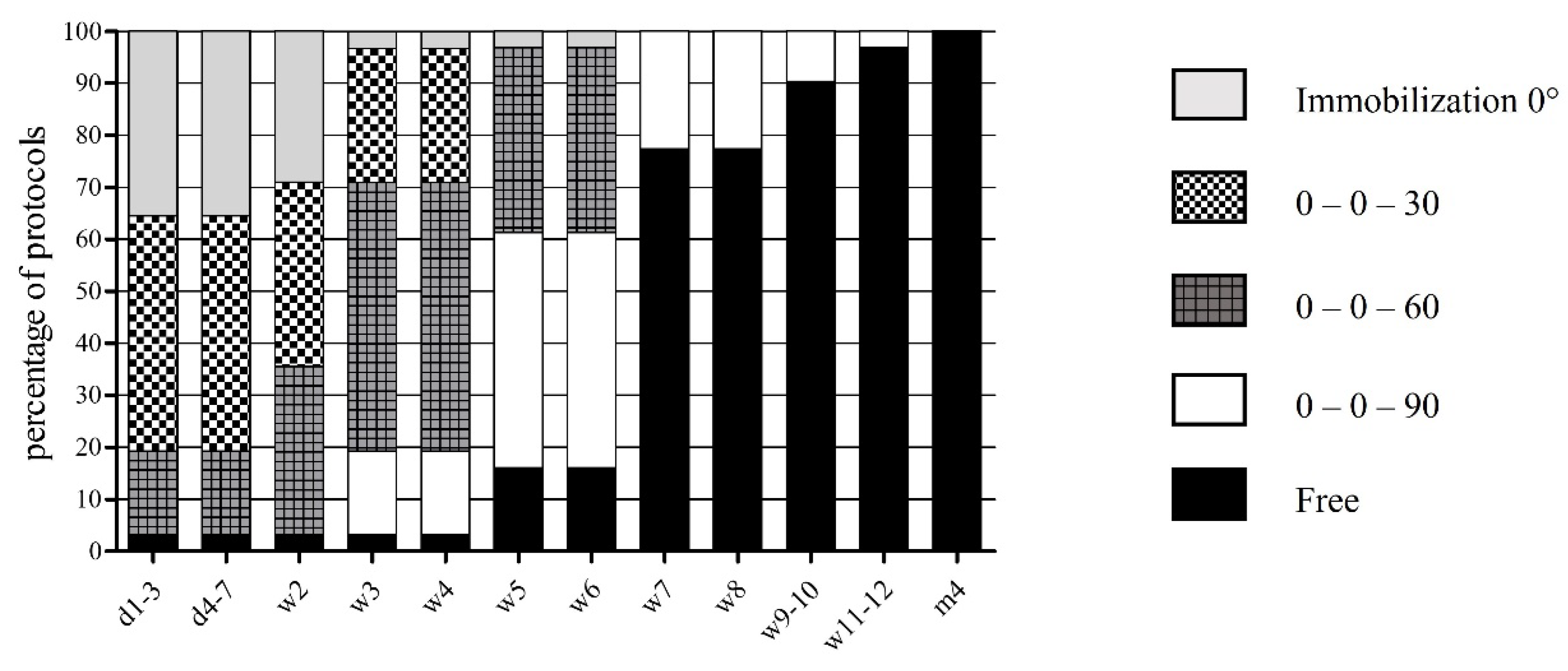
3.2. Progression of Weight Bearing and Range of Motion
3.3. Use of Knee Braces
3.4. Rehabilitation and Specific Training
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amis, A.A.; Bull, A.M.J.; Gupte, C.M.; Hijazi, I.; Race, A.; Robinson, J.R. Biomechanics of the PCL and related structures: Posterolateral, posteromedial and meniscofemoral ligaments. Knee Surgery, Sports Traumatol. Arthrosc. 2003, 11, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Bowman, K.F.; Sekiya, J.K. Anatomy and Biomechanics of the Posterior Cruciate Ligament, Medial and Lateral Sides of the Knee. Sports Med. Arthrosc. Rev. 2010, 18, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Matava, M.J.; Ellis, E.; Gruber, B. Surgical Treatment of Posterior Cruciate Ligament Tears: An Evolving Technique. J. Am. Acad. Orthop. Surg. 2009, 17, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Bedi, A.; Musahl, V.; Cowan, J.B. Management of Posterior Cruciate Ligament Injuries: An Evidence-Based Review. J. Am. Acad. Orthop. Surg. 2016, 24, 277–289. [Google Scholar] [CrossRef]
- Kennedy, N.I.; Wijdicks, C.A.; Goldsmith, M.T.; Michalski, M.P.; Devitt, B.M.; Årøen, A.; Engebretsen, L.; LaPrade, R.F. Kinematic analysis of the posterior cruciate ligament, part 1: The individual and collective function of the anterolateral and posteromedial bundles. Am. J. Sports Med. 2013, 41, 2828. [Google Scholar] [CrossRef]
- Dürselen, L.; Claes, L.; Kiefer, H. The Influence of Muscle Forces and External Loads on Cruciate Ligament Strain. Am. J. Sports Med. 1995, 23, 129–136. [Google Scholar] [CrossRef]
- Goyal, K.; Tashman, S.; Wang, J.H.; Li, K.; Zhang, X.; Harner, C. In Vivo Analysis of the Isolated Posterior Cruciate Ligament–Deficient Knee During Functional Activities. Am. J. Sports Med. 2012, 40, 777–785. [Google Scholar] [CrossRef]
- Sanders, T.L.; Pareek, A.; Barrett, I.J.; Kremers, H.M.; Bryan, A.J.; Stuart, M.J.; Levy, B.A.; Krych, A.J. Incidence and long-term follow-up of isolated posterior cruciate ligament tears. Knee Surgery, Sports Traumatol. Arthrosc. 2017, 25, 3017–3023. [Google Scholar] [CrossRef]
- Fanelli, G.C. Posterior cruciate ligament injuries in trauma patients. Arthrosc. J. Arthrosc. Relat. Surg. 1993, 9, 291–294. [Google Scholar] [CrossRef]
- Senese, M.; Greenberg, E.; Todd Lawrence, J.; Ganley, T. Rehabilitation following isolated posterior cruciate ligament reconstruction: A literature review of published protocols. Int. J. Sports Phys. Ther. 2018, 13, 737–751. [Google Scholar] [CrossRef] [Green Version]
- Zsidai, B.; Horvath, A.; Winkler, P.W.; Narup, E.; Kaarre, J.; Svantesson, E.; Musahl, V.; Hamrin Senorski, E.; Samuelsson, K. Different injury patterns exist among patients undergoing operative treatment of isolated PCL, combined PCL/ACL, and isolated ACL injuries: A study from the Swedish National Knee Ligament Registry. Knee Surg., Sports Traumatol. Arthrosc. 2022. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, K.; Takayama, Y.; Osaki, K.; Matsuo, Y.; Mizu-Uchi, H.; Hamai, S.; Honda, H.; Iwamoto, Y. Subclinical cartilage degeneration in young athletes with posterior cruciate ligament injuries detected with T1ρ magnetic resonance imaging mapping. Knee Surg. Sports Traumatol. Arthrosc. 2014, 23, 3094–3100. [Google Scholar] [CrossRef] [PubMed]
- Schüttler, K.F.; Ziring, E.; Ruchholtz, S.; Efe, T. Posterior cruciate ligament injuries. Unfallchirurg 2017, 120, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Skyhar, M.J.; Warren, R.F.; Ortiz, G.J.; Schwartz, E.; Otis, J.C. The effects of sectioning of the posterior cruciate ligament and the posterolateral complex on the articular contact pressures within the knee. J. Bone Jt. Surg. Am 1993, 75, 694–699. [Google Scholar] [CrossRef]
- Fowler, P.J.; Messieh, S.S. Isolated posterior cruciate ligament injuries in athletes. Am. J. Sports Med. 1987, 15, 553–557. [Google Scholar] [CrossRef]
- Jacobi, M.; Reischl, N.; Wahl, P.; Gautier, E.; Jakob, R.P. Acute isolated injury of the posterior cruciate ligament treated by a dynamic anterior drawer brace: A preliminary report. J. Bone Jt. Surg. Br. 2010, 92, 1381–1384. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Clark, M.; Gray, T. Minimum 10-Year Follow-up of Patients After an Acute, Isolated Posterior Cruciate Ligament Injury Treated Nonoperatively. Am. J. Sports Med. 2013, 41, 1526–1533. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Muthukaruppan, Y. Subjective results of nonoperatively treated, acute, isolated posterior cruciate ligament injuries. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 457–461. [Google Scholar] [CrossRef]
- Ahn, S.; Lee, Y.S.; Song, Y.D.; Chang, C.B.; Kang, S.B.; Choi, Y.S. Does surgical reconstruction produce better stability than conservative treatment in the isolated PCL injuries? Arch. Orthop. Trauma. Surg. 2016, 136, 811–819. [Google Scholar] [CrossRef]
- Vaquero-Picado, A.; Rodríguez-Merchán, E.C. Isolated posterior cruciate ligament tears: An update of management. EFORT Open Rev. 2017, 2, 89–96. [Google Scholar] [CrossRef]
- Johnson, P.; Mitchell, S.M.; Görtz, S. Graft Considerations in Posterior Cruciate Ligament Reconstruction. Curr. Rev. Musculoskelet. Med. 2018, 11, 521–527. [Google Scholar] [CrossRef]
- Montgomery, S.R.; Johnson, J.S.; McAllister, D.R.; Petrigliano, F.A. Surgical management of PCL injuries: Indications, techniques, and outcomes. Curr. Rev. Musculoskelet. Med. 2013, 6, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memmel, C.; Krutsch, W.; Szymski, D.; Pfeifer, C.; Henssler, L.; Frankewycz, B.; Angele, P.; Alt, V.; Koch, M. Current Standards of Early Rehabilitation after Anterior Cruciate Ligament Reconstruction in German Speaking Countries—Differentiation Based on Tendon Graft and Concomitant Injuries. Int. J. Environ. Res. Public Health 2022, 19, 4060. [Google Scholar] [CrossRef] [PubMed]
- Memmel, C.; Krutsch, W.; Koch, M.; Riedl, M.; Henssler, L.; Zeman, F.; Knorr, C.; Alt, V.; Pfeifer, C. The Conformity of Rehabilitation Protocols Used for Different Cartilage Repairs of the Knee Joint—A Review on Rehabilitation Standards in German Speaking Countries. Appl. Sci. 2021, 11, 8873. [Google Scholar] [CrossRef]
- Pierce, C.M.; O’Brien, L.; Griffin, L.W.; LaPrade, R.F. Posterior cruciate ligament tears: Functional and postoperative rehabilitation. Knee Surgery, Sports Traumatol. Arthrosc. 2012, 21, 1071–1084. [Google Scholar] [CrossRef] [PubMed]
- de Paula Leite Cury, R.; Kiyomoto, H.D.; Rosal, G.F.; Bryk, F.F.; de Oliveira, V.M.; de Camargo, O.P.A. Rehabilitation protocol after isolated posterior cruciate ligament reconstruction. Rev. Bras. Ortop. 2012, 47, 421–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, M.; Memmel, C.; Zeman, F.; Pfeifer, C.G.; Zellner, J.; Angele, P.; Weber-Spickschen, S.; Alt, V.; Krutsch, W. Early Functional Rehabilitation after Meniscus Surgery: Are Currently Used Orthopedic Rehabilitation Standards Up to Date? Rehabil. Res. Pr. 2020, 2020, 3989535. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, K.; Freedman, K.B.; Tjoumakaris, F.P. Rehabilitation Protocols After Isolated Meniscal Repair: A Systematic Review. Am. J. Sports Med. 2016, 45, 1687–1697. [Google Scholar] [CrossRef]
- Valle, C.; Hirschmüller, A.; Schmitt-Sody, M.; Haller, B.; Keller, M.; Schoch, W.; Hoffman, H.; Minzlaff, P. Standards in rehabilitation following anterior cruciate ligament reconstruction in the German-speaking world. Sportverletz. Sportschaden 2018, 32, 103–110. [Google Scholar]
- Fisher, B.; Nyland, J.; Brand, E.; Curtin, B. Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocation: A Systematic Review Including Rehabilitation and Return-to-Sports Efficacy. Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 1384–1394. [Google Scholar] [CrossRef]
- Hilber, F.; Pfeifer, C.; Memmel, C.; Zellner, J.; Angele, P.; Nerlich, M.; Kerschbaum, M.; Popp, D.; Baumann, F.; Krutsch, W. Early functional rehabilitation after patellar dislocation—What procedures are daily routine in orthopedic surgery? Injury 2019, 50, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, J.T.; Powers, M. ACL Rehabilitation Progression: Where Are We Now? Curr. Rev. Musculoskelet Med. 2017, 10, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, J.T.; Killian, S.E. Rehabilitation following meniscal repair. Curr. Rev. Musculoskelet Med. 2012, 5, 46–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Criteria of Early Rehabilitation | |
|---|---|
| Weight bearing | No body weight (NBW) |
| Partial body weight (PBW; loading up to 20 kg) | |
| Half body weight (HBW; loading more than 20 kg) | |
| Full body weight (FBW; unlimited loading) | |
| Range of motion (extension/flexion) | Immobilization 0° |
| 0–0–30° | |
| 0–0–60° | |
| 0–0–90° | |
| Free | |
| Use of braces | Yes/No |
| Recommended wearing time (weeks) | |
| Continuous passive/active motion | No CPM/CAM recommended |
| CPM recommended | |
| CAM recommended | |
| Start of rehabilitation training | Weeks after surgery |
| Start of specific training | Weeks after surgery |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Memmel, C.; Koch, M.; Szymski, D.; Huber, L.; Pfeifer, C.; Knorr, C.; Alt, V.; Krutsch, W. Standardized Rehabilitation or Individual Approach?—A Retrospective Analysis of Early Rehabilitation Protocols after Isolated Posterior Cruciate Ligament Reconstruction. J. Pers. Med. 2022, 12, 1299. https://doi.org/10.3390/jpm12081299
Memmel C, Koch M, Szymski D, Huber L, Pfeifer C, Knorr C, Alt V, Krutsch W. Standardized Rehabilitation or Individual Approach?—A Retrospective Analysis of Early Rehabilitation Protocols after Isolated Posterior Cruciate Ligament Reconstruction. Journal of Personalized Medicine. 2022; 12(8):1299. https://doi.org/10.3390/jpm12081299
Chicago/Turabian StyleMemmel, Clemens, Matthias Koch, Dominik Szymski, Lorenz Huber, Christian Pfeifer, Christian Knorr, Volker Alt, and Werner Krutsch. 2022. "Standardized Rehabilitation or Individual Approach?—A Retrospective Analysis of Early Rehabilitation Protocols after Isolated Posterior Cruciate Ligament Reconstruction" Journal of Personalized Medicine 12, no. 8: 1299. https://doi.org/10.3390/jpm12081299
APA StyleMemmel, C., Koch, M., Szymski, D., Huber, L., Pfeifer, C., Knorr, C., Alt, V., & Krutsch, W. (2022). Standardized Rehabilitation or Individual Approach?—A Retrospective Analysis of Early Rehabilitation Protocols after Isolated Posterior Cruciate Ligament Reconstruction. Journal of Personalized Medicine, 12(8), 1299. https://doi.org/10.3390/jpm12081299