
Characterization of Depressive Symptom Trajectories in Women between Childbirth and Diagnosis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Questionnaires
2.3. Missing Data
2.4. Parameter Overview
2.5. Methods: LCMM
2.6. Methods: MultLCMM
3. Results
3.1. Population
3.2. LCMM EPDS: Model Selection
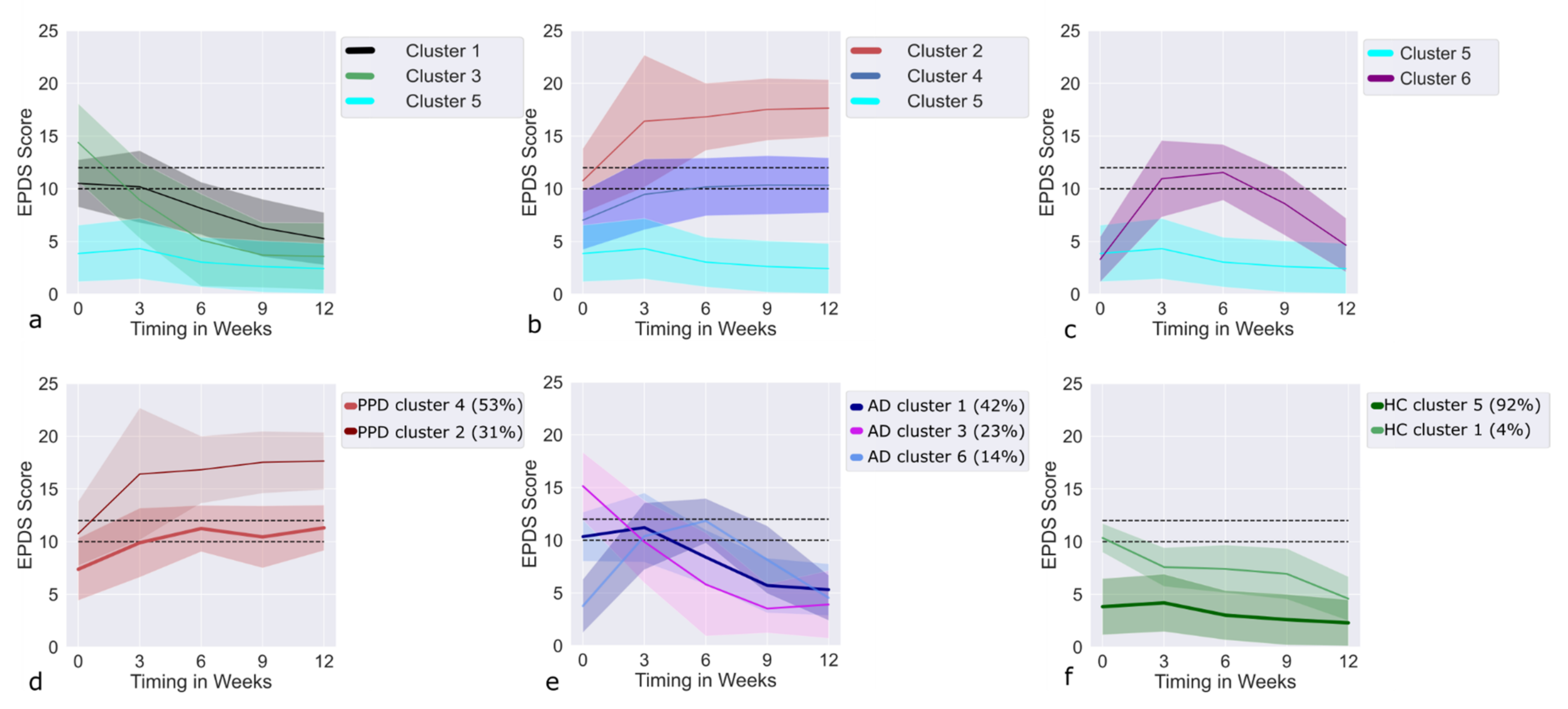
3.3. LCMM EPDS: Clusters
3.4. Recovering Clusters
3.5. Deteriorating Clusters
3.6. Trajectories of AD Cases within the Recovering Clusters
3.7. Trajectories of PPD Cases within the Deteriorating Clusters
3.8. Results MultLCMM MPAS + EPDS: Model Selection
3.9. MultLCMM MPAS/EPDS: Clusters
3.10. Trajectories of PPD Cases in the MPAS/EPDS Clusters
3.11. Trajectories of AD Cases in the MPAS/EPDS Clusters
3.12. Trajectories of HC in the MPAS/EPDS Clusters
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lindsay, J.R.; Nieman, L.K. The Hypothalamic-Pituitary-Adrenal Axis in Pregnancy: Challenges in Disease Detection and Treatment. Endocr. Rev. 2005, 26, 775–799. [Google Scholar] [CrossRef] [PubMed]
- Galea, L.A.; Frokjaer, V. Perinatal Depression: Embracing Variability toward Better Treatment and Outcomes. Neuron 2019, 102, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Hahn, L.; Eickhoff, S.B.; Habel, U.; Stickeler, E.; Schnakenberg, P.; Goecke, T.W.; Stickel, S.; Franz, M.; Dukart, J.; Chechko, N. Early identification of postpartum depression using demographic, clinical, and digital phenotyping. Transl. Psychiatry 2021, 11, 121. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Stickel, S.; Eickhoff, S.B.; Habel, U.; Stickeler, E.; Goecke, T.; Lang, J.; Chechko, N. Endocrine stress response in pregnancy and 12 weeks postpartum—Exploring risk factors for postpartum depression. Psychoneuroendocrinology 2020, 125, 105122. [Google Scholar] [CrossRef]
- Field, T. Postpartum depression effects on early interactions, parenting, and safety practices: A review. Infant Behav. Dev. 2010, 33, 1–6. [Google Scholar] [CrossRef]
- Barker, E.D.; Kirkham, N.; Ng, J.; Jensen, S.K.G. Prenatal maternal depression symptoms and nutrition, and child cognitive function. Br. J. Psychiatry 2013, 203, 417–421. [Google Scholar] [CrossRef]
- Rahman, A.; Surkan, P.J.; Cayetano, C.E.; Rwagatare, P.; Dickson, K.E. Grand Challenges: Integrating Maternal Mental Health into Maternal and Child Health Programmes. PLoS Med. 2013, 10, e1001442. [Google Scholar] [CrossRef]
- Monk, C.; Georgieff, M.K.; Osterholm, E.A. Research Review: Maternal prenatal distress and poor nutrition–mutually influencing risk factors affecting infant neurocognitive development. J. Child Psychol. Psychiatry 2013, 54, 115–130. [Google Scholar] [CrossRef]
- Pearson, R.M.; Bornstein, M.H.; Cordero, M.; Scerif, G.; Mahedy, L.; Evans, J.; Abioye, A.; Stein, A. Maternal perinatal mental health and offspring academic achievement at age 16: The mediating role of childhood executive function. J. Child Psychol. Psychiatry 2016, 57, 491–501. [Google Scholar] [CrossRef]
- Goodman, S.H.; Rouse, M.H.; Connell, A.M.; Broth, M.R.; Hall, C.M.; Heyward, D. Maternal Depression and Child Psychopathology: A Meta-Analytic Review. Clin. Child Fam. Psychol. Rev. 2011, 14, 1–27. [Google Scholar] [CrossRef]
- Murray, L.; Arteche, A.; Fearon, P.; Halligan, S.; Croudace, T.; Cooper, P. The effects of maternal postnatal depression and child sex on academic performance at age 16 years: A developmental approach: PND & child cognitive and academic outcomes. J. Child Psychol. Psychiatry 2010, 51, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Magnusson, C.; Rai, D.; Lundberg, M.; Lê-Scherban, F.; Dalman, C.; Lee, B.K. Associations of Parental Depression with Child School Performance at Age 16 Years in Sweden. JAMA Psychiatry 2016, 73, 239. [Google Scholar] [CrossRef] [PubMed]
- Weissman, M.M.; Wickramaratne, P.; Nomura, Y.; Warner, V.; Pilowsky, D.; Verdeli, H. Offspring of Depressed Parents: 20 Years Later. Am. J. Psychiatry 2006, 163, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Pearson, R.M.; Evans, J.; Kounali, D.; Lewis, G.; Heron, J.; Ramchandani, P.; O’Connor, T.G.; Stein, A. Maternal Depression During Pregnancy and the Postnatal Period: Risks and Possible Mechanisms for Offspring Depression at Age 18 Years. JAMA Psychiatry 2013, 70, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yin, P.; Wei, D.; Wang, K.; Li, Y.; Qiu, J. Effects of parental emotional warmth on the relationship between regional gray matter volume and depression-related personality traits. Soc. Neurosci. 2017, 12, 337–348. [Google Scholar] [CrossRef]
- Miller, L.J. Postpartum Depression. JAMA 2002, 287, 762–765. [Google Scholar] [CrossRef]
- O’Hara, M.W. Postpartum depression: What we know. J. Clin. Psychol. 2009, 65, 1258–1269. [Google Scholar] [CrossRef]
- O’Hara, M.W.; McCabe, J.E. Postpartum Depression: Current Status and Future Directions. Annu. Rev. Clin. Psychol. 2013, 9, 379–407. [Google Scholar] [CrossRef]
- Campbell, S.B.; Matestic, P.; Von Stauffenberg, C.; Mohan, R.; Kirchner, T. Trajectories of maternal depressive symptoms, maternal sensitivity, and children’s functioning at school entry. Dev. Psychol. 2007, 43, 1202–1215. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Qandil, S.; Jabr, S.; Wagler, S.; Collin, S.M. Postpartum depression in the Occupied Palestinian Territory: A longitudinal study in Bethlehem. BMC Pregnancy Childbirth 2016, 16, 375. [Google Scholar] [CrossRef] [PubMed]
- Denckla, C.A.; Mancini, A.D.; Consedine, N.S.; Milanovic, S.M.; Basu, A.; Seedat, S.; Spies, G.; Henderson, D.C.; Bonanno, G.A.; Koenen, K.C. Distinguishing postpartum and antepartum depressive trajectories in a large population-based cohort: The impact of exposure to adversity and offspring gender. Psychol. Med. 2018, 48, 1139–1147. [Google Scholar] [CrossRef] [PubMed]
- Munk-Olsen, T.; Laursen, T.M.; Pedersen, C.B.; Mors, O.; Mortensen, P.B. New Parents and Mental Disorders: A Population-Based Register Study. JAMA 2006, 296, 2582–2589. [Google Scholar] [CrossRef]
- Taylor, C.L.; Broadbent, M.; Khondoker, M.; Stewart, R.J.; Howard, L.M. Predictors of severe relapse in pregnant women with psychotic or bipolar disorders. J. Psychiatr. Res. 2018, 104, 100–107. [Google Scholar] [CrossRef]
- Halfin, A. Depression: The benefits of early and appropriate treatment. Am. J. Manag. Care 2007, 13, S92. [Google Scholar]
- Fisher, J.; De Mello, M.C.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: A systematic review. Bull. World Health Organ. 2012, 90, 139H–149H. [Google Scholar] [CrossRef]
- Akil, H.; Gordon, J.; Hen, R.; Javitch, J.; Mayberg, H.; McEwen, B.; Meaney, M.J.; Nestler, E.J.; Akil, H.; Gordon, J.; et al. Treatment resistant depression: A multi-scale, systems biology approach. Neurosci. Biobehav. Rev. 2018, 84, 272–288. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Bergant, A.M.; Nguyen, T.; Heim, K.; Ulmer, H.; Dapunt, O. Deutschsprachige Fassung und Validierung der »Edinburgh postnatal depression scale. DMW Dtsch. Med. Wochenschr. 2008, 123, 35–40. [Google Scholar] [CrossRef]
- Condon, J.T.; Corkindale, C.J. The assessment of parent-to-infant attachment: Development of a self-report questionnaire instrument. J. Reprod. Infant Psychol. 1998, 16, 57–76. [Google Scholar] [CrossRef]
- Kennerley, H.; Gath, D. Maternity Blues: I. Detection and Measurement by Questionnaire. Br. J. Psychiatry 1989, 155, 356–362. [Google Scholar] [CrossRef] [PubMed]
- RStudio Team. RStudio; RStudio Team: Boston, MA, USA, 2020. [Google Scholar]
- Harrison, E. Missing Data. Available online: https://cran.r-project.org/web/packages/finalfit/vignettes/missing.html (accessed on 2 February 2022).
- Van De Schoot, R.; Sijbrandij, M.; Winter, S.D.; Depaoli, S.; Vermunt, J.K. The GRoLTS-Checklist: Guidelines for Reporting on Latent Trajectory Studies. Struct. Equ. Model. Multidiscip. J. 2017, 24, 451–467. [Google Scholar] [CrossRef]
- Proust-Lima, C.; Philipps, V.; Liquet, B. Estimation of Extended Mixed Models Using Latent Classes and Latent Processes: The R Package lcmm. J. Stat. Softw. 2017, 78, 1–56. [Google Scholar] [CrossRef]
- Proust, C.; Jacqmin-Gadda, H. Estimation of linear mixed models with a mixture of distribution for the random effects. Comput. Methods Programs Biomed. 2005, 78, 165–173. [Google Scholar] [CrossRef]
- Carrière, I.; Farré, A.; Proust-Lima, C.; Ryan, J.; Ancelin, M.L.; Ritchie, K. Chronic and remitting trajectories of depressive symptoms in the elderly. Characterisation and risk factors. Epidemiol. Psychiatr. Sci. 2017, 26, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Madigan, S.; Wade, M.; Plamondon, A.; Jenkins, J.M. Trajectories of maternal depressive symptoms in the early childhood period and family-wide clustering of risk. J. Affect. Disord. 2017, 215, 49–55. [Google Scholar] [CrossRef]
- Lo, Y.; Mendell, N.R.; Rubin, D.B. Testing the number of components in a normal mixture. Biometrika 2001, 88, 767–778. [Google Scholar] [CrossRef]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Model. A Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Feder, A.; Singh, R.; Schechter, C.B.; Bromet, E.J.; Katz, C.L.; Reissman, D.B.; Ozbay, F.; Sharma, V.; Crane, M.; et al. Trajectories of PTSD risk and resilience in World Trade Center responders: An 8-year prospective cohort study. Psychol. Med. 2014, 44, 205–219. [Google Scholar] [CrossRef]
- Fleishman, A.I. A method for simulating non-normal distributions. Psychometrika 1978, 43, 521–532. [Google Scholar] [CrossRef]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.T. Predictors of Postpartum Depression: An Update. Nurs. Res. 2001, 50, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Luoma, I.; Korhonen, M.; Salmelin, R.K.; Helminen, M.; Tamminen, T. Long-term trajectories of maternal depressive symptoms and their antenatal predictors. J. Affect. Disord. 2015, 170, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Righetti-Veltema, M.; Conne-Perréard, E.; Bousquet, A.; Manzano, J. Risk factors and predictive signs of postpartum depression. J. Affect. Disord. 1998, 49, 167–180. [Google Scholar] [CrossRef]
- Sundström-Poromaa, I.; Comasco, E.; Sumners, R.; Luders, E. Progesterone–Friend or foe? Front. Neuroendocr. 2020, 59, 100856. [Google Scholar] [CrossRef] [PubMed]
- Harris, B. Biological and Hormonal Aspects of Postpartum Depressed Mood: Working Towards Strategies for Prophylaxis and Treatment. Br. J. Psychiatry 1994, 164, 288–292. [Google Scholar] [CrossRef][Green Version]
- Patel, M.; Jabeen, S.; Osiezagha, K.; Bailey, R.K.; Ali, S.; Barker, N.C. Postpartum Depression: A Review. J. Health Care Poor Underserved 2012, 23, 534–542. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Risk Factors | Cluster 1 vs. Baseline | Cluster 3 vs. Baseline | Cluster 6 vs. Baseline | Cluster 2 vs. Baseline | Cluster 4 vs. Baseline |
|---|---|---|---|---|---|
| Family psychiatric history | X | ||||
| Psychiatric diagnosis in previous pregnancy | X | X | X | ||
| Relocation to another ward | X | ||||
| Baby blues | X | X | X | X | |
| Birth-related psychological and physical traumas | X | X | |||
| Previous depression | X | X | X | X | |
| PMS Severity | X | X | X | ||
| EPDS T0 | X | X | X | X | |
| EPDS T1 | X | X | X | X | X |
| EPDS T2 | X | X | X | X | X |
| EPDS T3 | X | X | X | X | |
| EPDS T4 | X | X | X | X | |
| MPAS T1 | X | X | X | X | |
| MPAS T2 | X | X | X | ||
| MPAS T3 | X | X | X | ||
| MPAS T4 | X | X | |||
| SLE | X | X | |||
| Support at home | X | X | |||
| Family status | X | ||||
| Income | X |
| Risk Factors | Cluster 1 MPAS/EPDS vs. Baseline | Upright U-shaped vs. Baseline | Inverted U-shaped vs. Baseline |
|---|---|---|---|
| Baby blues | X | X | X |
| Previous depression | X | X | |
| PMS Severity | X | X | X |
| EPDS T0 | X | X | X |
| EPDS T1 | X | X | X |
| EPDS T2 | X | X | X |
| EPDS T3 | X | X | X |
| EPDS T4 | X | X | X |
| MPAS T1 | X | X | X |
| MPAS T2 | X | X | X |
| MPAS T3 | X | X | X |
| MPAS T4 | X | X | X |
| SLE | X | ||
| Support at home | X | X | |
| Birth-related psychological and physical traumas | X | X | |
| Psychiatric diagnosis in previous pregnancy | X | ||
| Family psychiatric history | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chechko, N.; Stickel, S.; Losse, E.; Shymanskaya, A.; Habel, U. Characterization of Depressive Symptom Trajectories in Women between Childbirth and Diagnosis. J. Pers. Med. 2022, 12, 538. https://doi.org/10.3390/jpm12040538
Chechko N, Stickel S, Losse E, Shymanskaya A, Habel U. Characterization of Depressive Symptom Trajectories in Women between Childbirth and Diagnosis. Journal of Personalized Medicine. 2022; 12(4):538. https://doi.org/10.3390/jpm12040538
Chicago/Turabian StyleChechko, Natalia, Susanne Stickel, Elena Losse, Aliaksandra Shymanskaya, and Ute Habel. 2022. "Characterization of Depressive Symptom Trajectories in Women between Childbirth and Diagnosis" Journal of Personalized Medicine 12, no. 4: 538. https://doi.org/10.3390/jpm12040538
APA StyleChechko, N., Stickel, S., Losse, E., Shymanskaya, A., & Habel, U. (2022). Characterization of Depressive Symptom Trajectories in Women between Childbirth and Diagnosis. Journal of Personalized Medicine, 12(4), 538. https://doi.org/10.3390/jpm12040538