
Machine Learning for Prediction of Recurrence in Parasagittal and Parafalcine Meningiomas: Combined Clinical and MRI Texture Features

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Patient Selection
2.3. Clinical Data
2.4. Evaluation of Progression/Recurrence (P/R)
2.5. Image Acquisition
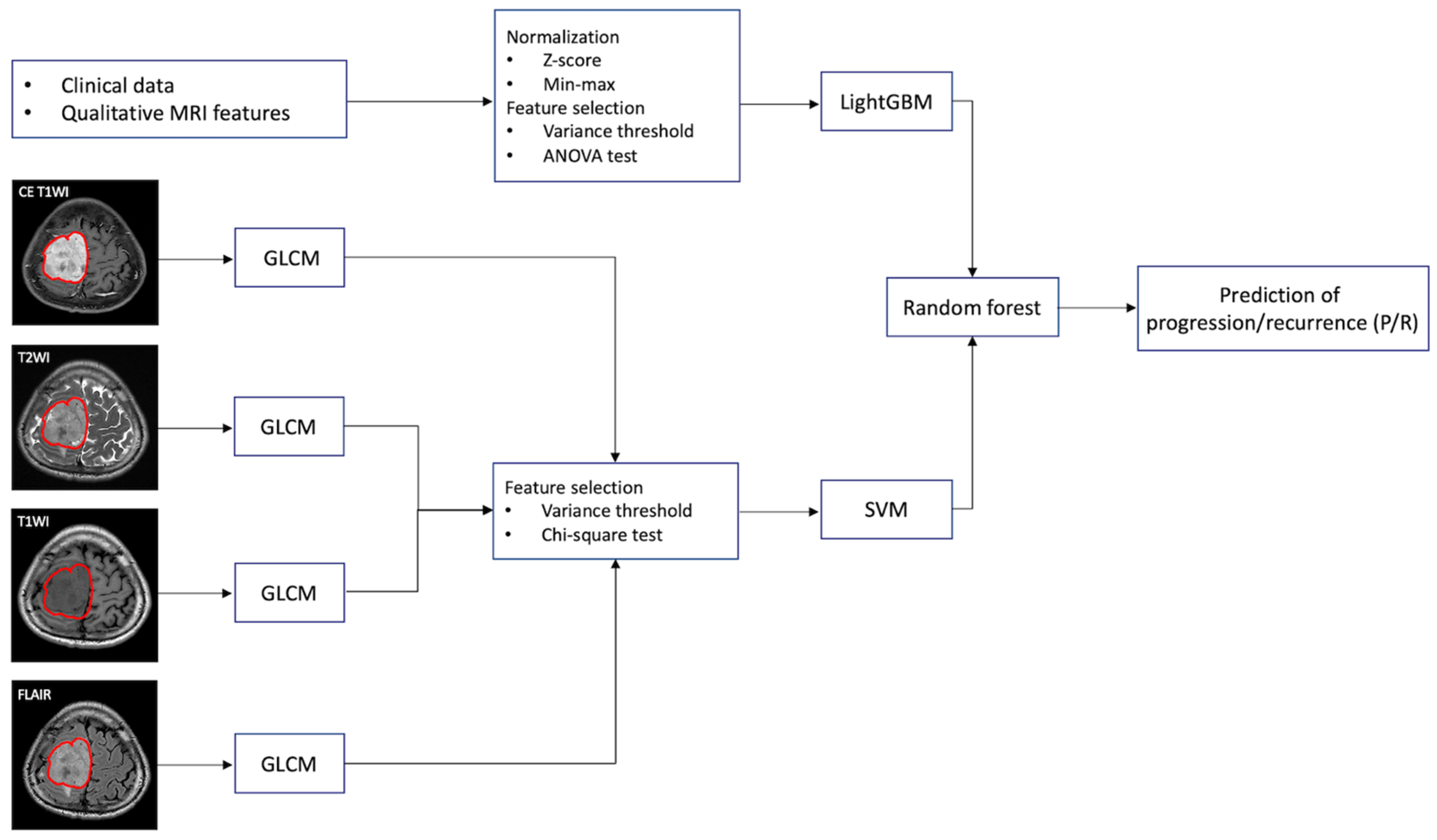
2.6. Machine Learning and Classification Methods
2.7. Feature Extraction in Clinical Data
2.8. Tumor Segmentation and Texture Feature Extraction
2.9. Combination of Clinical and Texture Classifiers
2.10. Statistical Analysis
3. Results
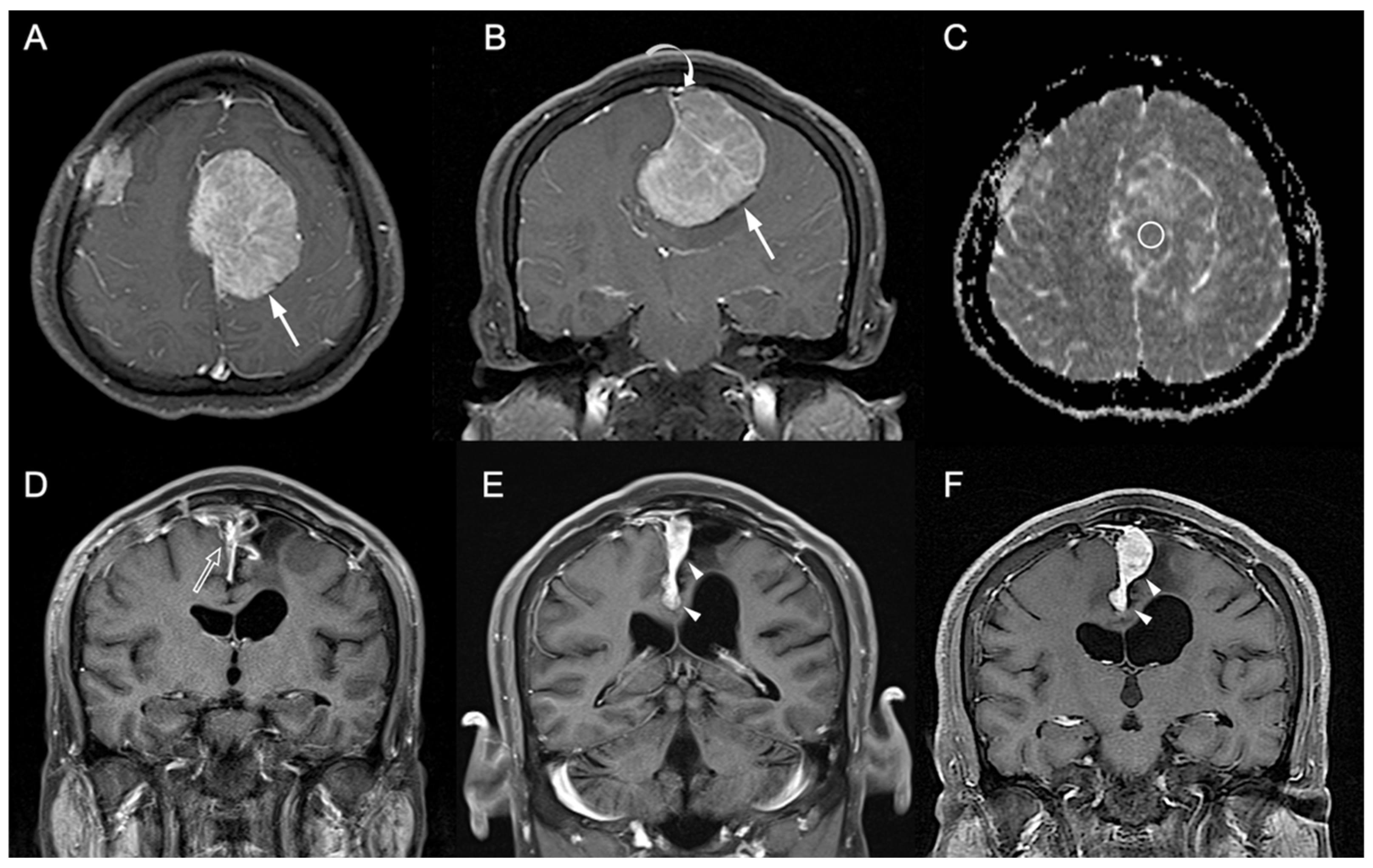
3.1. Clinical and Imaging Findings
3.2. Machine Learning for the Prediction of P/R
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiemels, J.; Wrensch, M.; Claus, E.B. Epidemiology and etiology of meningioma. J. Neurooncol. 2010, 99, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Pettersson-Segerlind, J.; Orrego, A.; Lönn, S.; Mathiesen, T. Long-term 25-year follow-up of surgically treated parasagittal meningiomas. World Neurosurg. 2011, 76, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Maillo, A.; Orfao, A.; Espinosa, A.B.; Sayagues, J.M.; Merino, M.; Sousa, P.; Lara, M.; Tabernero, M.D. Early recurrences in histologically benign/grade I meningiomas are associated with large tumors and coexistence of monosomy 14 and del(1p36) in the ancestral tumor cell clone. Neuro-Oncology 2007, 9, 438–446. [Google Scholar] [CrossRef]
- Ildan, F.; Erman, T.; Gocer, A.I.; Tuna, M.; Bagdatoglu, H.; Cetinalp, E.; Burgut, R. Predicting the probability of meningioma recurrence in the preoperative and early postoperative period: A multivariate analysis in the midterm follow-up. Skull Base Off. J. North Am. Skull Base Soc. 2007, 17, 157–171. [Google Scholar] [CrossRef]
- Ko, C.C.; Zhang, Y.; Chen, J.H.; Chang, K.T.; Chen, T.Y.; Lim, S.W.; Wu, T.C.; Su, M.Y. Pre-operative MRI Radiomics for the Prediction of Progression and Recurrence in Meningiomas. Front. Neurol. 2021, 12, 636235. [Google Scholar] [CrossRef]
- Ding, D.; Xu, Z.; McNeill, I.T.; Yen, C.P.; Sheehan, J.P. Radiosurgery for parasagittal and parafalcine meningiomas. J. Neurosurg. 2013, 119, 871–877. [Google Scholar] [CrossRef]
- Ko, C.C.; Chen, T.Y.; Lim, S.W.; Kuo, Y.T.; Wu, T.C.; Chen, J.H. Prediction of Recurrence in Parasagittal and Parafalcine Meningiomas: Added Value of Diffusion-Weighted Magnetic Resonance Imaging. World Neurosurg. 2019, 124, e470–e479. [Google Scholar] [CrossRef]
- Huo, W.Y.; Li, L.; Zhang, Y.F. Resection of recurrent parasagittal meningiomas with complete obstructed superior sagittal sinus. Int. Congr. Ser. 2004, 1259, 53–57. [Google Scholar] [CrossRef]
- Raza, S.M.; Gallia, G.L.; Brem, H.; Weingart, J.D.; Long, D.M.; Olivi, A. Perioperative and long-term outcomes from the management of parasagittal meningiomas invading the superior sagittal sinus. Neurosurgery 2010, 67, 885–893. [Google Scholar] [CrossRef]
- Oyama, H.; Kito, A.; Maki, H.; Hattori, K.; Noda, T.; Wada, K. Surgical results of parasagittal and falx meningioma. Nagoya J. Med. Sci. 2012, 74, 211–216. [Google Scholar] [PubMed]
- Skudas, G.; Tamasauskas, A. Prognosis of the surgical treatment of parasagittal meningioma. Medicina 2002, 38, 1089–1096. [Google Scholar] [PubMed]
- Sughrue, M.E.; Rutkowski, M.J.; Shangari, G.; Parsa, A.T.; Berger, M.S.; McDermott, M.W. Results with judicious modern neurosurgical management of parasagittal and falcine meningiomas. J. Neurosurg. 2011, 114, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Ottenhausen, M.; Rumalla, K.; Younus, I.; Minkowitz, S.; Tsiouris, A.J.; Schwartz, T.H. Predictors of postoperative motor function in rolandic meningiomas. J. Neurosurg. 2018, 1, 1–6. [Google Scholar] [CrossRef]
- Tahta, K.; Cirak, B.; Pakdemirli, E.; Suzer, T.; Tahta, F. Postoperative mutism after removal of an anterior falcine meningioma. J. Clin. Neurosci. 2007, 14, 793–796. [Google Scholar] [CrossRef]
- Conti, A.; Pontoriero, A.; Siddi, F.; Iati, G.; Cardali, S.; Angileri, F.F.; Granata, F.; Pergolizzi, S.; Germano, A.; Tomasello, F. Post-Treatment Edema after Meningioma Radiosurgery is a Predictable Complication. Cureus 2016, 8, e605. [Google Scholar] [CrossRef]
- Kalapurakal, J.A.; Silverman, C.L.; Akhtar, N.; Laske, D.W.; Braitman, L.E.; Boyko, O.B.; Thomas, P.R. Intracranial meningiomas: Factors that influence the development of cerebral edema after stereotactic radiosurgery and radiation therapy. Radiology 1997, 204, 461–465. [Google Scholar] [CrossRef]
- Koçak, B.; Durmaz, E.; Ateş, E.; Kılıçkesmez, Ö. Radiomics with artificial intelligence: A practical guide for beginners. Diagn Interv. Radiol. 2019, 25, 485–495. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, C.; Tian, Z.; Feng, R.; Cheng, Y.; Xu, J. The Diagnostic Value of MRI-Based Texture Analysis in Discrimination of Tumors Located in Posterior Fossa: A Preliminary Study. Front. Neurosci. 2019, 13, 1113. [Google Scholar] [CrossRef]
- Ion-Mărgineanu, A.; Van Cauter, S.; Sima, D.M.; Maes, F.; Sunaert, S.; Himmelreich, U.; Van Huffel, S. Classifying Glioblastoma Multiforme Follow-Up Progressive vs. Responsive Forms Using Multi-Parametric MRI Features. Front. Neurosci. 2016, 10, 615. [Google Scholar] [CrossRef][Green Version]
- Chaddad, A.; Daniel, P.; Desrosiers, C.; Toews, M.; Abdulkarim, B. Novel Radiomic Features Based on Joint Intensity Matrices for Predicting Glioblastoma Patient Survival Time. IEEE J. Biomed. Health Inf. 2019, 23, 795–804. [Google Scholar] [CrossRef]
- Zhu, Y.; Man, C.; Gong, L.; Dong, D.; Yu, X.; Wang, S.; Fang, M.; Wang, S.; Fang, X.; Chen, X.; et al. A deep learning radiomics model for preoperative grading in meningioma. Eur. J. Radiol. 2019, 116, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Hamerla, G.; Meyer, H.J.; Schob, S.; Ginat, D.T.; Altman, A.; Lim, T.; Gihr, G.A.; Horvath-Rizea, D.; Hoffmann, K.T.; Surov, A. Comparison of machine learning classifiers for differentiation of grade 1 from higher gradings in meningioma: A multicenter radiomics study. Magn. Reson. Imaging 2019, 63, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [PubMed]
- Sindou, M.; Hallacq, P. Venous reconstruction in surgery of meningiomas invading the sagittal and transverse sinuses. Skull Base Surg. 1998, 8, 57–64. [Google Scholar] [CrossRef]
- Chung, S.B.; Kim, C.Y.; Park, C.K.; Kim, D.G.; Jung, H.W. Falx meningiomas: Surgical results and lessons learned from 68 cases. J. Korean Neurosurg. Soc. 2007, 42, 276–280. [Google Scholar] [CrossRef]
- Ko, C.C.; Lim, S.W.; Chen, T.Y.; Chen, J.H.; Li, C.F.; Shiue, Y.L. Prediction of progression in skull base meningiomas: Additional benefits of apparent diffusion coefficient value. J. Neurooncol. 2018, 138, 63–71. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, J.H.; Chen, T.Y.; Lim, S.W.; Wu, T.C.; Kuo, Y.T.; Ko, C.C.; Su, M.Y. Radiomics approach for prediction of recurrence in skull base meningiomas. Neuroradiology 2019, 61, 1355–1364. [Google Scholar] [CrossRef]
- Walker, A.J.; Ruzevick, J.; Malayeri, A.A.; Rigamonti, D.; Lim, M.; Redmond, K.J.; Kleinberg, L. Postradiation imaging changes in the CNS: How can we differentiate between treatment effect and disease progression? Future Oncol. 2014, 10, 1277–1297. [Google Scholar] [CrossRef]
- Morin, O.; Chen, W.C.; Nassiri, F.; Susko, M.; Magill, S.T.; Vasudevan, H.N.; Wu, A.; Vallieres, M.; Gennatas, E.D.; Valdes, G.; et al. Integrated models incorporating radiologic and radiomic features predict meningioma grade, local failure, and overall survival. Neuro-Oncology 2019, 1, vdz011. [Google Scholar] [CrossRef]
- Laukamp, K.R.; Shakirin, G.; Baeßler, B.; Thiele, F.; Zopfs, D.; Große Hokamp, N.; Timmer, M.; Kabbasch, C.; Perkuhn, M.; Borggrefe, J. Accuracy of Radiomics-Based Feature Analysis on Multiparametric Magnetic Resonance Images for Noninvasive Meningioma Grading. World Neurosurg. 2019, 132, e366–e390. [Google Scholar] [CrossRef] [PubMed]
- GuolinKe, Q.M.; Finley, T.; Wang, T.; Chen, W.; Ma, W.; Ye, Q.; Liu, T.-Y. LightGBM: A Highly Efficient Gradient Boosting Decision Tree. Adv. Neural Inf. Process. Syst. 2017, 30, 52. [Google Scholar]
- Mohanaiah, P.; Sathyanarayana, P.; GuruKumar, L. Image texture feature extraction using GLCM approach. Int. J. Sci. Res. Publ. 2013, 3, 1–5. [Google Scholar]
- Guyon, I.; Elisseeff, A. An introduction to variable and feature selection. J. Mach. Learn. Res. 2003, 3, 1157–1182. [Google Scholar]
- Tong, S.; Chang, E. Support vector machine active learning for image retrieval. In Proceedings of the Ninth ACM International Conference on Multimedia, Ottawa, ON, Canada, 30 September–5 October 2001; pp. 107–118. [Google Scholar]
- Segal, M.R. Machine learning benchmarks and random forest regression. Biostatistics 2004, 10, 1–14. [Google Scholar]
- Paul, J.; Verleysen, M.; Dupont, P. Identification of Statistically Significant Features from Random Forests. In Proceedings of the ECML Workshop on Solving Complex Machine Learning Problems with Ensemble Methods, Prague, Czech Republic, 27 September 2013. [Google Scholar]
- Franklin, J. The elements of statistical learning: Data mining, inference and prediction. Math. Intell. 2005, 27, 83–85. [Google Scholar]
- Kohavi, R.; John, G.H. Automatic parameter selection by minimizing estimated error. In Machine Learning Proceedings 1995; Elsevier: Amsterdam, The Netherlands, 1995; pp. 304–312. [Google Scholar]
- Fida, M.A.F.A.; Ahmad, T.; Ntahobari, M. Variance Threshold as Early Screening to Boruta Feature Selection for Intrusion Detection System. In Proceedings of the 2021 13th International Conference on Information & Communication Technology and System (ICTS), Surabaya, Indonesia, 20–21 October 2021; pp. 46–50. [Google Scholar]
- Patro, S.; Sahu, K.K. Normalization: A preprocessing stage. arXiv preprint 2015, arXiv:1503.06462. [Google Scholar]
- Kopitar, L.; Kocbek, P.; Cilar, L.; Sheikh, A.; Stiglic, G. Early detection of type 2 diabetes mellitus using machine learning-based prediction models. Sci. Rep. 2020, 10, 11981. [Google Scholar] [CrossRef]
- Song, Y.; Jiao, X.; Qiao, Y.; Liu, X.; Qiang, Y.; Liu, Z.; Zhang, L. Prediction of double-high biochemical indicators based on LightGBM and XGBoost. In Proceedings of the 2019 International Conference on Artificial Intelligence and Computer Science, Wuhan, China, 12–13 July 2019; pp. 189–193. [Google Scholar]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Cham, Switzerlands, 2015; pp. 234–241. [Google Scholar]
- Jain, S. Brain cancer classification using GLCM based feature extraction in artificial neural network. Int. J. Comput. Sci. Eng. Technol. 2013, 4, 966–970. [Google Scholar]
- Usha, R.; Perumal, K. SVM classification of brain images from MRI scans using morphological transformation and GLCM texture features. Int. J. Comput. Syst. Eng. 2019, 5, 18–23. [Google Scholar]
- Joshi, J.; Phadke, M. Feature extraction and texture classification in MRI. Energy 2010, 1, 0. [Google Scholar]
- Platt, J. Probabilistic outputs for SVMs and comparisons to regularized likelihood methods. Adv. Large Margin Classif. 2004, 24, 61–74. [Google Scholar]
- Drucker, H.; Burges, C.J.; Kaufman, L.; Smola, A.; Vapnik, V. Support vector regression machines. Adv. Neural Inf. Processing Syst. 1997, 9, 155–161. [Google Scholar]
- Nasrabadi, N.M. Pattern recognition and machine learning. J. Electron. Imaging 2007, 16, 049901. [Google Scholar]
- Abuella, M.; Chowdhury, B. Random forest ensemble of support vector regression models for solar power forecasting. In Proceedings of the 2017 IEEE Power & Energy Society Innovative Smart Grid Technologies Conference (ISGT at the Crystal Gateway Marriott, Arlington, VA, USA), Washington, DC, USA, 23–26 April 2017; pp. 1–5. [Google Scholar]
- Dimitriadis, S.I.; Liparas, D.; Tsolaki, M.N.; Initiative, A.s.D.N. Random forest feature selection, fusion and ensemble strategy: Combining multiple morphological MRI measures to discriminate among healhy elderly, MCI, cMCI and alzheimer’s disease patients: From the alzheimer’s disease neuroimaging initiative (ADNI) database. J. Neurosci. Methods 2018, 302, 14–23. [Google Scholar]
- Louppe, G.; Wehenkel, L.; Sutera, A.; Geurts, P. Understanding variable importances in forests of randomized trees. Adv. Neural Inf. Process. Syst. 2013, 26. [Google Scholar]
- van Alkemade, H.; de Leau, M.; Dieleman, E.M.; Kardaun, J.W.; van Os, R.; Vandertop, W.P.; van Furth, W.R.; Stalpers, L.J. Impaired survival and long-term neurological problems in benign meningioma. Neuro-Oncology 2012, 14, 658–666. [Google Scholar] [CrossRef]
- Park, Y.W.; Oh, J.; You, S.C.; Han, K.; Ahn, S.S.; Choi, Y.S.; Chang, J.H.; Kim, S.H.; Lee, S.K. Radiomics and machine learning may accurately predict the grade and histological subtype in meningiomas using conventional and diffusion tensor imaging. Eur. Radiol. 2019, 29, 4068–4076. [Google Scholar] [CrossRef]
- Yang, L.; Xu, P.; Zhang, Y.; Cui, N.; Wang, M.; Peng, M.; Gao, C.; Wang, T. A deep learning radiomics model may help to improve the prediction performance of preoperative grading in meningioma. Neuroradiology 2022, 1–10. [Google Scholar] [CrossRef]
- Chen, C.; Guo, X.; Wang, J.; Guo, W.; Ma, X.; Xu, J. The Diagnostic Value of Radiomics-Based Machine Learning in Predicting the Grade of Meningiomas Using Conventional Magnetic Resonance Imaging: A Preliminary Study. Front. Oncol. 2019, 9, 1338. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhang, X.Y.; Shi, Y.J.; Wang, L.; Zhu, H.T.; Tang, Z.; Wang, S.; Li, X.T.; Tian, J.; Sun, Y.S. Radiomics Analysis for Evaluation of Pathological Complete Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. Clin. Cancer Res. 2017, 23, 7253–7262. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Yang, P.; Liang, W.; Liu, W.; Wang, W.; Luo, C.; Wang, J.; Peng, Z.; Xing, L.; Huang, M.; et al. A radiomics approach based on support vector machine using MR images for preoperative lymph node status evaluation in intrahepatic cholangiocarcinoma. Theranostics 2019, 9, 5374–5385. [Google Scholar] [CrossRef]
- Fan, Y.; Jiang, S.; Hua, M.; Feng, S.; Feng, M.; Wang, R. Machine Learning-Based Radiomics Predicts Radiotherapeutic Response in Patients with Acromegaly. Front. Endocrinol. 2019, 588. [Google Scholar] [CrossRef]
- Ming, X.; Oei, R.W.; Zhai, R.; Kong, F.; Du, C.; Hu, C.; Hu, W.; Zhang, Z.; Ying, H.; Wang, J. MRI-based radiomics signature is a quantitative prognostic biomarker for nasopharyngeal carcinoma. Sci. Rep. 2019, 9, 10412. [Google Scholar] [CrossRef] [PubMed]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and Reproducibility of Radiomic Features: A Systematic Review. Int. J. Radiat Oncol. Biol. Phys. 2018, 102, 1143–1158. [Google Scholar] [CrossRef]
- Shur, J.; Blackledge, M.; D’Arcy, J.; Collins, D.J.; Bali, M.; O’Leach, M.; Koh, D.-M. MRI texture feature repeatability and image acquisition factor robustness, a phantom study and in silico study. Eur. Radiol Exp. 2021, 5, 2. [Google Scholar] [CrossRef]
- Shiri, I.; Abdollahi, H.; Shaysteh, S.; Mahdavi, S.R. Test-retest reproducibility and robustness analysis of recurrent glioblastoma MRI radiomics texture features. Iran. J. Radiol. 2017, 5. [Google Scholar]
- Baeßler, B.; Weiss, K.; Pinto Dos Santos, D. Robustness and Reproducibility of Radiomics in Magnetic Resonance Imaging: A Phantom Study. Investig. Radiol 2019, 54, 221–228. [Google Scholar] [CrossRef]
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of deep learning: Concepts, CNN architectures, challenges, applications, future directions. J. Big Data 2021, 8, 53. [Google Scholar] [CrossRef]
- Preethi, G.; Sornagopal, V. MRI image classification using GLCM texture features. In Proceedings of the 2014 International Conference on Green Computing Communication and Electrical Engineering (ICGCCEE), Coimbatore, India, 6–8 March 2014; 1–6. [Google Scholar]
- Mall, P.K.; Singh, P.K.; Yadav, D. GLCM Based Feature Extraction and Medical X-RAY Image Classification using Machine Learning Techniques. In Proceedings of the 2019 IEEE Conference on Information and Communication Technology, Allahabad, India, 6–8 December 2019; pp. 1–6. [Google Scholar]
- Ahn, S.J.; Shin, H.J.; Chang, J.H.; Lee, S.K. Differentiation between primary cerebral lymphoma and glioblastoma using the apparent diffusion coefficient: Comparison of three different ROI methods. PLoS ONE 2014, 9, e112948. [Google Scholar] [CrossRef]
- Nanda, A.; Bir, S.C.; Maiti, T.K.; Konar, S.K.; Missios, S.; Guthikonda, B. Relevance of Simpson grading system and recurrence-free survival after surgery for World Health Organization Grade I meningioma. J. Neurosurg. 2017, 126, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Sayegh, E.T.; Larson, A.; Bloch, O.; Madden, M.; Sun, M.Z.; Barani, I.J.; James, C.D.; Parsa, A.T. Adjuvant radiotherapy for atypical and malignant meningiomas: A systematic review. Neuro-Oncology 2014, 16, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Maclean, J.; Fersht, N.; Short, S. Controversies in radiotherapy for meningioma. Clin. Oncol. 2014, 26, 51–64. [Google Scholar] [CrossRef]
- Savardekar, A.R.; Patra, D.P.; Bir, S.; Thakur, J.D.; Mohammed, N.; Bollam, P.; Georgescu, M.M.; Nanda, A. Differential Tumor Progression Patterns in Skull Base Versus Non-Skull Base Meningiomas: A Critical Analysis from a Long-Term Follow-Up Study and Review of Literature. World Neurosurg. 2018, 112, e74–e83. [Google Scholar] [CrossRef]
- Hwang, W.L.; Marciscano, A.E.; Niemierko, A.; Kim, D.W.; Stemmer-Rachamimov, A.O.; Curry, W.T.; Barker, F.G., 2nd; Martuza, R.L.; Loeffler, J.S.; Oh, K.S.; et al. Imaging and extent of surgical resection predict risk of meningioma recurrence better than WHO histopathological grade. Neuro-Oncology 2016, 18, 863–872. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P/R | Non-P/R | p Value | |
|---|---|---|---|
| Number of patients | 13 | 44 | |
| Sex | 0.053 | ||
| Male | 8 (61.5%) | 14 (31.8%) | |
| Female | 5 (38.5%) | 30 (68.2%) | |
| Age (y) | 57 (48, 66) | 56 (47.5, 64.5) | 0.909 |
| Histological subtypes | 0.928 | ||
| Meningothelial (syncytial) | 11 (84.6%) | 36 (81.8%) | |
| Transitional (mixed) | 1 (7.7%) | 3 (6.8%) | |
| Fibroblastic (fibrous) | 1 (7.7%) | 5 (11.4%) | |
| Parasagittal or parafalcine | 0.466 | ||
| Parasagittal | 9 (69.2%) | 35 (79.5%) | |
| Parafalcine | 4 (30.8%) | 9 (20.5%) | |
| Degree of superior sagittal sinus invasion (Sindou classification) | 0.592 | ||
| None | 3 (23.1%) | 15 (34.1%) | |
| Type 1–3 | 5 (38.5%) | 18 (40.9%) | |
| Type 4–6 | 5 (38.5%) | 11 (25%) | |
| Tumor location | 0.627 | ||
| Anterior | 5 (38.5%) | 11 (25%) | |
| Middle | 7 (53.8%) | 28 (63.6%) | |
| Posterior | 1 (7.7%) | 5 (11.4%) | |
| Simpson grade resection | 0.015 * | ||
| Grades I, II, and III (gross-total resection) | 5 (38.5%) | 34 (77.3%) | |
| Grade IV and V (subtotal resection) | 8 (61.5%) | 10 (22.7%) | |
| Postoperative adjuvant radiotherapy | 0.713 | ||
| Yes | 2 (15.4%) | 10 (22.7%) | |
| No | 11 (84.6%) | 34 (77.3%) | |
| Peritumoral edema | 7 (53.8%) | 26 (59.1%) | 0.736 |
| Calcification | 2 (15.4%) | 15 (34.1%) | 0.304 |
| Heterogeneous enhancement | 4 (30.8%) | 20 (45.5%) | 0.346 |
| Cystic change or necrosis | 3 (23.1%) | 8 (18.2%) | 0.700 |
| Dural tail sign | 7 (53.8%) | 21 (47.7%) | 0.698 |
| Skull bone invasion | 5 (38.5%) | 6 (13.6%) | 0.102 |
| Reactive hyperostosis | 1 (7.7%) | 7 (15.9%) | 0.667 |
| Multiplicity | 2 (15.4%) | 1 (2.3%) | 0.127 |
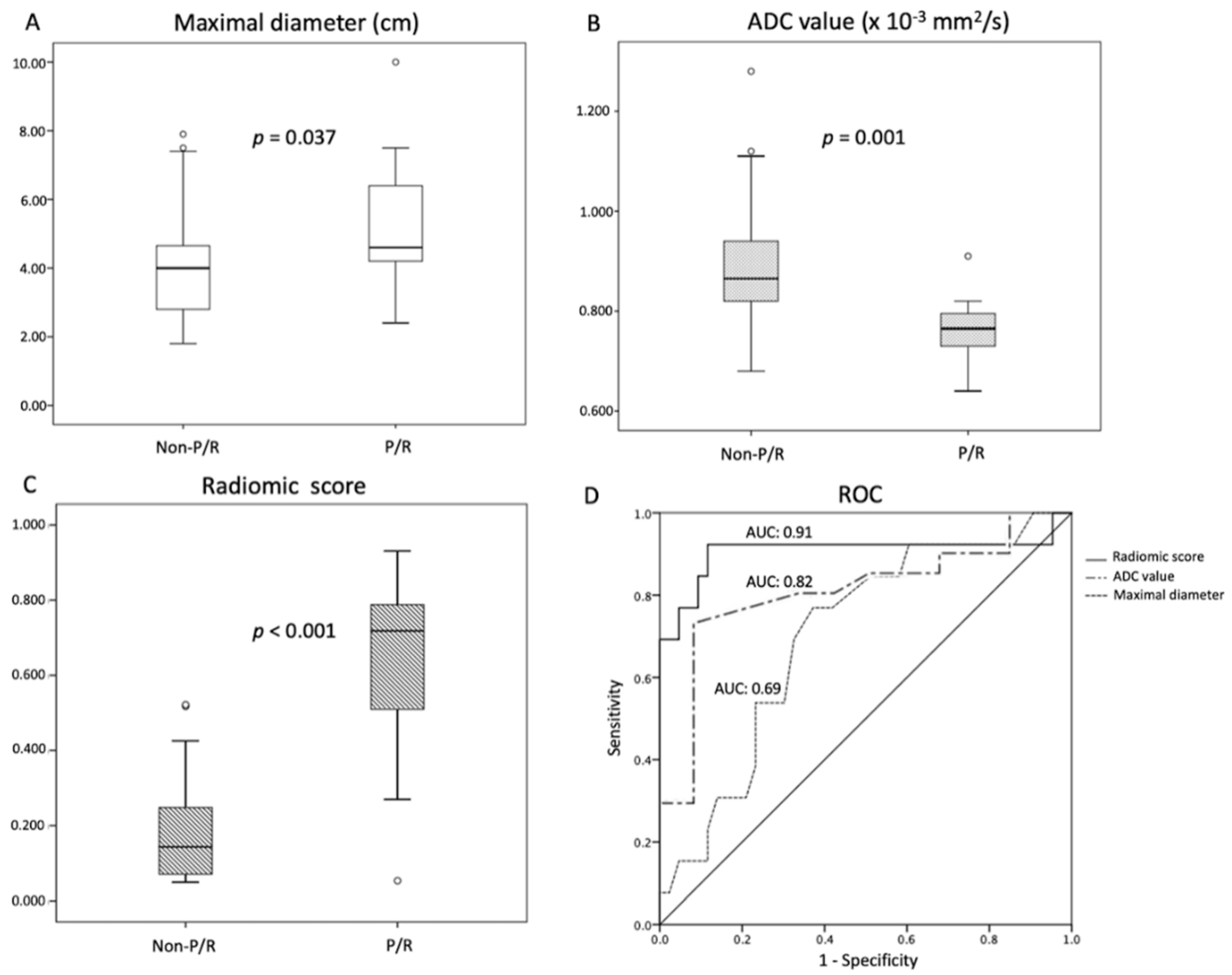
| Maximal diameter (cm) | 4.6 (3.3, 5.9) | 4 (3.1, 4.9) | 0.037 * |
| Tumor volume (cm3) | 26.5 (13.8, 120) | 20.3 (4.3 36.3) | 0.224 |
| ADC value (×10−3 mm2/s) | 0.765 (0.729, 0.802) | 0.865 (0.799, 0.932) | 0.001 * |
| Radiomic score | 0.718 (0.518, 0.918) | 0.143 (0.051, 0.236) | <0.001* |
| Follow-up time (months) | 77 (49.5, 104.5) | 54 (27, 81) | 0.083 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR (95 % CI) for P/R | p | HR (95 % CI) for P/R | p | |
| Sex (fraction male) | 2.165 (0.659, 7.110) | 0.203 | ||
| Superior sagittal sinus invasion (Sindou types 4–6) | 1.851 (0.563, 6.082) | 0.311 | ||
| Location (middle) | 1.006 (0.293, 3.455) | 0.993 | ||
| Subtotal resection | 4.407 (1.284, 15.126) | 0.018 * | 2.063 (0.524, 8.125) | 0.301 |
| Postoperative adjuvant radiotherapy | 0.612 (0.131, 2.855) | 0.523 | ||
| Peritumoral edema | 0.624 (0.190, 2.056) | 0.439 | ||
| Calcification | 0.556 (0.119, 2.590) | 0.455 | ||
| Heterogeneous enhancement | 0.506 (0.134, 1.911) | 0.315 | ||
| Cystic change or necrosis | 1.221 (0.263, 5.676) | 0.799 | ||
| Dural tail sign | 1.964 (0.588, 6.556) | 0.273 | ||
| Adjacent bone invasion | 3.246 (0.941, 11.194) | 0.062 | ||
| Reactive hyperostosis | 0.698 (0.089, 5.468) | 0.732 | ||
| Multiplicity | 3.051 (0.656, 14.186) | 0.155 | ||
| Maximal diameter > 4.2 cm (cut-off value) | 3.223 (0.852, 12.187) | 0.085 | ||
| Tumor volume (cm3) | 1.005 (0.995, 1.015) | 0.364 | ||
| ADC < 0.825 × 10−3 mm2/s (cut-off value) | 17.183 (2.171, 135.986) | 0.007 * | 4.130 (0.414, 41.161) | 0.227 |
| Radiomic score > 0.269 (cut-off value) | 28.701 (3.660, 225.068) | 0.001 * | 15.729 (1.751, 141.292) | 0.014 * |
| 5-Fold Cross Validation | Data | Accuracy | Precision | Recall | AUC |
|---|---|---|---|---|---|
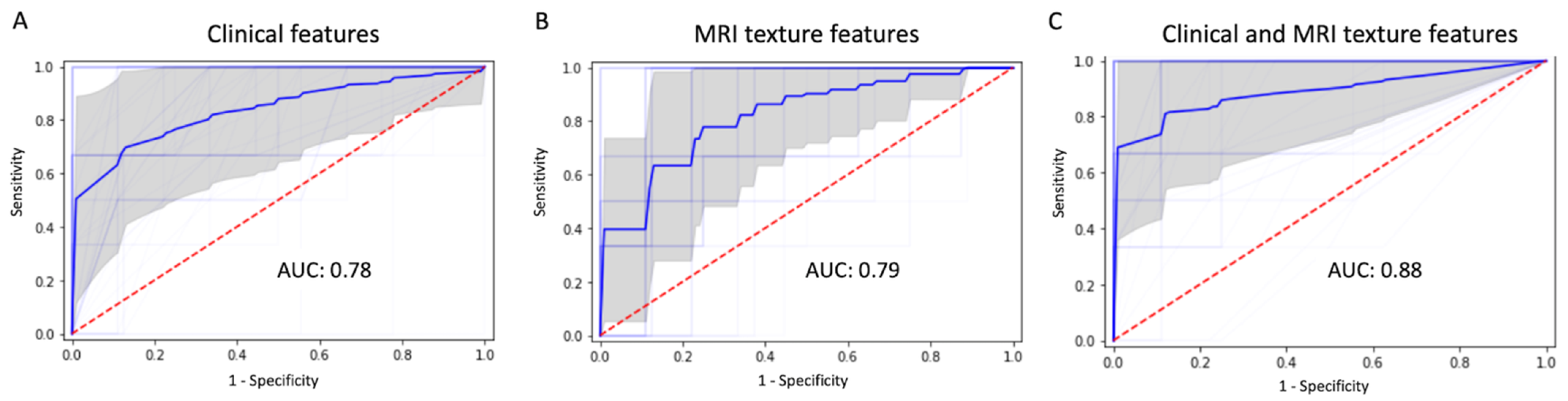
| Average over 15 trials | Clinical data | 0.86 | 0.83 | 0.67 | 0.78 |
| T1WI | 0.77 | 0.53 | 0.23 | 0.58 | |
| T2WI | 0.68 | 0.52 | 0.37 | 0.57 | |
| T2 FLAIR | 0.72 | 0.43 | 0.23 | 0.55 | |
| Contrast enhanced (CE) T1WI | 0.77 | 0.69 | 0.37 | 0.63 | |
| Combination of four MRI sequences | 0.88 | 0.83 | 0.63 | 0.79 | |
| Combination of clinical and MRI | 0.91 | 0.85 | 0.83 | 0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, H.-P.; Wu, D.-Y.; Hung, K.-C.; Lim, S.-W.; Chen, T.-Y.; Fan-Chiang, Y.; Ko, C.-C. Machine Learning for Prediction of Recurrence in Parasagittal and Parafalcine Meningiomas: Combined Clinical and MRI Texture Features. J. Pers. Med. 2022, 12, 522. https://doi.org/10.3390/jpm12040522
Hsieh H-P, Wu D-Y, Hung K-C, Lim S-W, Chen T-Y, Fan-Chiang Y, Ko C-C. Machine Learning for Prediction of Recurrence in Parasagittal and Parafalcine Meningiomas: Combined Clinical and MRI Texture Features. Journal of Personalized Medicine. 2022; 12(4):522. https://doi.org/10.3390/jpm12040522
Chicago/Turabian StyleHsieh, Hsun-Ping, Ding-You Wu, Kuo-Chuan Hung, Sher-Wei Lim, Tai-Yuan Chen, Yang Fan-Chiang, and Ching-Chung Ko. 2022. "Machine Learning for Prediction of Recurrence in Parasagittal and Parafalcine Meningiomas: Combined Clinical and MRI Texture Features" Journal of Personalized Medicine 12, no. 4: 522. https://doi.org/10.3390/jpm12040522
APA StyleHsieh, H.-P., Wu, D.-Y., Hung, K.-C., Lim, S.-W., Chen, T.-Y., Fan-Chiang, Y., & Ko, C.-C. (2022). Machine Learning for Prediction of Recurrence in Parasagittal and Parafalcine Meningiomas: Combined Clinical and MRI Texture Features. Journal of Personalized Medicine, 12(4), 522. https://doi.org/10.3390/jpm12040522