
Development of Metabolic Syndrome Decreases Bone Mineral Density T-Score of Calcaneus in Foot in a Large Taiwanese Population Follow-Up Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. TWB
2.3. Collection of Demographic, Medical, and Laboratory Data
2.4. Definition of MetS
2.5. Assessment of BMD
2.6. Statistical Analysis
3. Results
3.1. Associations among MetS and Its Five Components with Baseline BMD T-Score
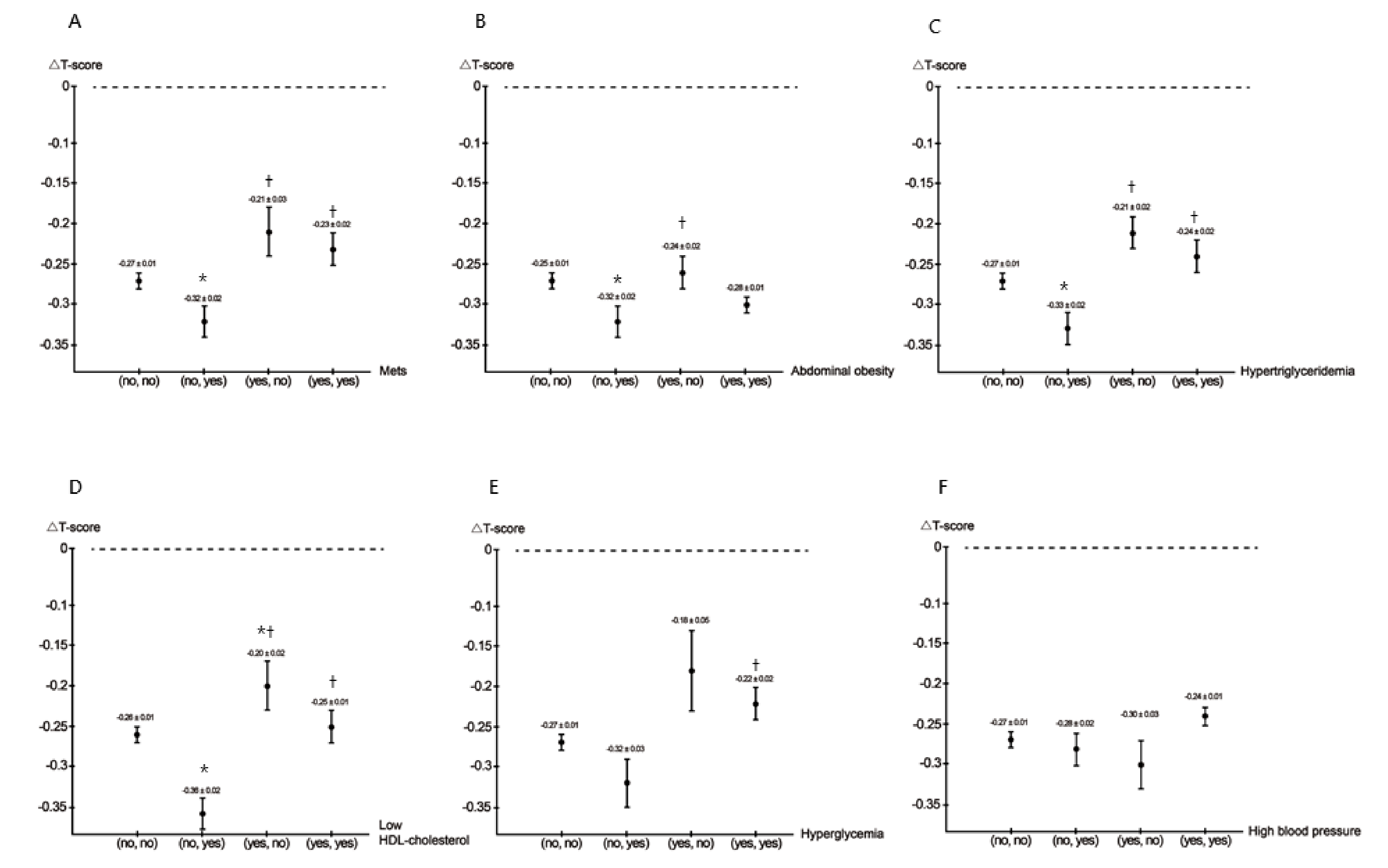
- MetSCompared to the (no, no), (yes, no), and (yes, yes) MetS groups, the (no, yes) MetS group had the lowest ΔT-score.
- Abdominal obesityCompared to the (no, no) and (yes, no) abdominal obesity groups, the (no, yes) abdominal obesity group had the lowest ΔT-score.
- HypertriglyceridemiaCompared to the (no, no), (yes, no), and (yes, yes) hypertriglyceridemia groups, the (no, yes) hypertriglyceridemia group had the lowest ΔT-score.
- Low HDL cholesterolCompared to the (no, no), (yes, no), and (yes, yes) low HDL cholesterol groups, the (no, yes) low HDL cholesterol group had the lowest ΔT-score.
- HyperglycemiaCompared to the (yes, yes) hyperglycemia group, the (no, yes) hyperglycemia group had a lower ΔT-score.
- High blood pressure
- MetSCompared to the (no, yes) MetS group, the (no, no) MetS group (unstandardized coefficient β, 0.043; p = 0.048), (yes, no) MetS group (unstandardized coefficient β, 0.101; p = 0.004), and (yes, yes) MetS group (unstandardized coefficient β, 0.091; p = 0.001) were significantly associated with high ΔT-score.
- Abdominal obesityCompared to the (no, yes) abdominal obesity group, the other three abdominal obesity groups were not significantly associated with ΔT-score.
- HypertriglyceridemiaCompared to the (no, yes) hypertriglyceridemia group, the (no, no) hypertriglyceridemia group (unstandardized coefficient β, 0.085; p < 0.001), (yes, no) hypertriglyceridemia group (unstandardized coefficient β, 0.144; p < 0.001), and (yes, yes) hypertriglyceridemia group (unstandardized coefficient β, 0.088; p = 0.001) were significantly associated with high ΔT-score.
- Low HDL cholesterolCompared to the (no, yes) low HDL cholesterol group, the (no, no) low HDL cholesterol group (unstandardized coefficient β, 0.081; p < 0.001), (yes, no) low HDL cholesterol group (unstandardized coefficient β, 0.135; p < 0.001), and (yes, yes) low HDL cholesterol group (unstandardized coefficient β, 0.112; p < 0.001) were significantly associated with high ΔT-score.
- HyperglycemiaCompared to the (no, yes) hyperglycemia group, the (yes, no) hyperglycemia group (unstandardized coefficient β, 0.118; p = 0.033) and (yes, yes) hyperglycemia group (unstandardized coefficient β, 0.106; p = 0.002) were significantly associated with high ΔT-score.
- High blood pressureCompared to the (yes, no) high blood pressure group, the (yes, yes) high blood pressure group (unstandardized coefficient β, 0.076; p = 0.025) was significantly associated with high ΔT-score.
3.2. Associations among ΔMetS Components with BMD ΔT-Score Using Multivariable Linear Regression Analysis in the (No, Yes) MetS Group
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zimmet, P.; Alberti, K.; Shaw, J. International Diabetes Federation: The IDF consensus worldwide definition of the metabolic syndrome. Diabetes Voice 2005, 50, 31–33. Available online: https://www.idf.org/component/attachments/attachments.html?id=705&task=download (accessed on 19 May 2021).
- Ranasinghe, P.; Mathangasinghe, Y.; Jayawardena, R.; Hills, A.P.; Misra, A. Prevalence and trends of metabolic syndrome among adults in the Asia-Pacific region: A systematic review. BMC Public Health 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.C.; Conell, C.; Ren, X.; Banki, N.M.; Chan, S.L.; Rao, V.A.; Melles, R.B.; Bhatt, D.L. Effect of Systolic and Diastolic Blood Pressure on Cardiovascular Outcomes. N. Engl. J. Med. 2019, 381, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Cornier, M.-A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.; Wang, H.; Eckel, R.H. The Metabolic Syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar] [CrossRef]
- Alberti, K.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Kaur, J. A Comprehensive Review on Metabolic Syndrome. Cardiol. Res. Pract. 2014, 2014, 1–21. [Google Scholar] [CrossRef]
- Consensus development conference: Diagnosis, prophylaxis, and treatment of osteoporosis. Am. J. Med. 1993, 94, 646–650. [CrossRef]
- Edwards, M.; Dennison, E.; Sayer, A.A.; Fielding, R.; Cooper, C. Osteoporosis and sarcopenia in older age. Bone 2015, 80, 126–130. [Google Scholar] [CrossRef]
- Fink, H.A.; Ewing, S.K.; Ensrud, K.; Barrett-Connor, E.; Taylor, B.C.; Cauley, J.A.; Orwoll, E.S. Association of Testosterone and Estradiol Deficiency with Osteoporosis and Rapid Bone Loss in Older Men. J. Clin. Endocrinol. Metab. 2006, 91, 3908–3915. [Google Scholar] [CrossRef]
- Almeida, M.; Han, L.; Martin-Millan, M.; Plotkin, L.I.; Stewart, S.A.; Roberson, P.K.; Kousteni, S.; O’Brien, C.A.; Bellido, T.; Parfitt, A.M.; et al. Skeletal Involution by Age-associated Oxidative Stress and Its Acceleration by Loss of Sex Steroids. J. Biol. Chem. 2007, 282, 27285–27297. [Google Scholar] [CrossRef]
- Ding, C.; Parameswaran, V.; Udayan, R.; Burgess, J.; Jones, G. Circulating Levels of Inflammatory Markers Predict Change in Bone Mineral Density and Resorption in Older Adults: A Longitudinal Study. J. Clin. Endocrinol. Metab. 2008, 93, 1952–1958. [Google Scholar] [CrossRef]
- Von Muhlen, D.; Safii, S.; Jassal, S.K.; Svartberg, J.; Barrett-Connor, E. Associations between the metabolic syndrome and bone health in older men and women: The Rancho Bernardo Study. Osteoporos. Int. 2007, 18, 1337–1344. [Google Scholar] [CrossRef]
- Jeon, Y.K.; Lee, J.G.; Kim, S.S.; Kim, B.H.; Kim, S.-J.; Kim, Y.K.; Kim, I.J. Association between bone mineral density and metabolic syndrome in pre- and postmenopausal women. Endocr. J. 2011, 58, 87–93. [Google Scholar] [CrossRef]
- Wong, S.K.; Chin, K.-Y.; Suhaimi, F.H.; Ahmad, F.; Ima-Nirwana, S. The Relationship between Metabolic Syndrome and Osteoporosis: A Review. Nutrients 2016, 8, 347. [Google Scholar] [CrossRef]
- Zhou, J.; Zhang, Q.; Yuan, X.; Wang, J.; Li, C.; Sheng, H.; Qu, S.; Li, H. Association between metabolic syndrome and osteoporosis: A meta-analysis. Bone 2013, 57, 30–35. [Google Scholar] [CrossRef]
- Muka, T.; Trajanoska, K.; Jong, J.C.K.-D.; Oei, L.; Uitterlinden, A.G.; Hofman, A.; Dehghan, A.; Zillikens, M.C.; Franco, O.H.; Rivadeneira, F. The Association between Metabolic Syndrome, Bone Mineral Density, Hip Bone Geometry and Fracture Risk: The Rotterdam Study. PLoS ONE 2015, 10, e0129116. [Google Scholar] [CrossRef]
- Loke, S.-S.; Chang, H.-W.; Li, W.-C. Association between metabolic syndrome and bone mineral density in a Taiwanese elderly population. J. Bone Miner. Metab. 2017, 36, 200–208. [Google Scholar] [CrossRef]
- Jones, D.H.; Kong, Y.-Y.; Penninger, J.M. Role of RANKL and RANK in bone loss and arthritis. Ann. Rheum. Dis. 2002, 61, ii32–ii39. [Google Scholar] [CrossRef] [PubMed]
- Hofbauer, L.C. Clinical Implications of the Osteoprotegerin/RANKL/RANK System for Bone and Vascular Diseases. JAMA 2004, 292, 490–495. [Google Scholar] [CrossRef]
- Caudarella, R.; Vescini, F.; Rizzoli, E.; Francucci, C.M. Salt intake, hypertension, and osteoporosis. J. Endocrinol. Investig. 2009, 32, 15–20. [Google Scholar]
- Tanaka, K.-I.; Yamaguchi, T.; Kanazawa, I.; Sugimoto, T. Effects of high glucose and advanced glycation end products on the expressions of sclerostin and RANKL as well as apoptosis in osteocyte-like MLO-Y4-A2 cells. Biochem. Biophys. Res. Commun. 2015, 461, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, C.; Zhou, Y.; Chen, W.; Luo, G.; Zhang, Z.; Wang, H.; Zhang, Y.; Xu, D.; Sheng, P. Advanced glycation end products biphasically modulate bone resorption in osteoclast-like cells. Am. J. Physiol. Metab. 2016, 310, E355–E366. [Google Scholar] [CrossRef] [PubMed]
- Hannan, M.T.; Felson, D.T.; Anderson, J.J. Bone mineral density in elderly men and women: Results from the framingham osteoporosis study. J. Bone Miner. Res. 2009, 7, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Edelstein, S.L.; Barrett-Connor, E. Relation between Body Size and Bone Mineral Density in Elderly Men and Women. Am. J. Epidemiology 1993, 138, 160–169. [Google Scholar] [CrossRef]
- Chen, C.-H.; Yang, J.-H.; Chiang, C.W.; Hsiung, C.-N.; Wu, P.-E.; Chang, L.-C.; Chu, H.-W.; Chang, J.; Yuan-Tsong, C.; Yang, S.-L.; et al. Population structure of Han Chinese in the modern Taiwanese population based on 10,000 participants in the Taiwan Biobank project. Hum. Mol. Genet. 2016, 25, 5321–5331. [Google Scholar] [CrossRef]
- Fan, C.-T.; Hung, T.-H.; Yeh, C.-K. Taiwan Regulation of Biobanks. J. Law Med. Ethics 2015, 43, 816–826. [Google Scholar] [CrossRef]
- SOCIAL INDICATORS 2010. Directorate General of Budget, Accounting and Statistics, Executive Yuan, Republic of China ed.; 2011. Available online: https://ebook.dgbas.gov.tw/public/Data/331311351353.pdf (accessed on 19 May 2021).
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D.R. A More Accurate Method to Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Isomaa, B.; Henricsson, M.; Almgren, P.; Tuomi, T.; Taskinen, M.-R.; Groop, L. The metabolic syndrome influences the risk of chronic complications in patients with Type II diabetes. Diabetologia 2001, 44, 1148–1154. [Google Scholar] [CrossRef]
- Tan, C.-E.; Ma, S.; Wai, D.; Chew, S.-K.; Tai, E.-S. Can We Apply the National Cholesterol Education Program Adult Treatment Panel Definition of the Metabolic Syndrome to Asians? Diabetes Care 2004, 27, 1182–1186. [Google Scholar] [CrossRef]
- Xue, P.; Gao, P.; Li, Y. The association between metabolic syndrome and bone mineral density: A meta-analysis. Endocrine 2012, 42, 546–554. [Google Scholar] [CrossRef]
- Sugimoto, T.; Sato, M.; Dehle, F.C.; Brnabic, A.J.; Weston, A.; Burge, R. Lifestyle-Related Metabolic Disorders, Osteoporosis, and Fracture Risk in Asia: A Systematic Review. Value Health Reg. Issues 2016, 9, 49–56. [Google Scholar] [CrossRef]
- Darroudi, S.; Fereydouni, N.; Tayefi, M.; Ahmadnezhad, M.; Zamani, P.; Tayefi, B.; Kharazmi, J.; Tavalaie, S.; Heidari-Bakavoli, A.; Azarpajouh, M.R.; et al. Oxidative stress and inflammation, two features associated with a high percentage body fat, and that may lead to diabetes mellitus and metabolic syndrome. BioFactors 2019, 45, 35–42. [Google Scholar] [CrossRef]
- Singh, A.; Mehdi, A.A.; Srivastava, R.N.; Verma, N.S. Immunoregulation of bone remodelling. Int. J. Crit. Illn. Inj. Sci. 2012, 2, 75–81. [Google Scholar] [CrossRef]
- Wang, X.; Chen, B.; Sun, J.; Jiang, Y.; Zhang, H.; Zhang, P.; Fei, B.; Xu, Y. Iron-induced oxidative stress stimulates osteoclast differentiation via NF-κB signaling pathway in mouse model. Metabolism 2018, 83, 167–176. [Google Scholar] [CrossRef]
- Redlich, K.; Smolen, J.S. Inflammatory bone loss: Pathogenesis and therapeutic intervention. Nat. Rev. Drug Discov. 2012, 11, 234–250. [Google Scholar] [CrossRef]
- Domazetovic, V. Oxidative stress in bone remodeling: Role of antioxidants. Clin. Cases Miner. Bone Metab. 2017, 14, 209–216. [Google Scholar] [CrossRef]
- Kim, T.; Park, S.; Pak, Y.-S.; Lee, S.; Lee, E.-H. Association between metabolic syndrome and bone mineral density in Korea: The Fourth Korea National Health and Nutrition Examination Survey (KNHANES IV), 2008. J. Bone Miner. Metab. 2013, 31, 652–662. [Google Scholar] [CrossRef]
- Rendina, D.; D’Elia, L.; Evangelista, M.; De Filippo, G.; Giaquinto, A.; Abate, V.; Barone, B.; Piccinocchi, G.; Prezioso, D.; Strazzullo, P. Metabolic syndrome is associated to an increased risk of low bone mineral density in free-living women with suspected osteoporosis. J. Endocrinol. Investig. 2021, 44, 1321–1326. [Google Scholar] [CrossRef]
- Kinjo, M.; Setoguchi, S.; Solomon, D.H. Bone Mineral Density in Adults with the Metabolic Syndrome: Analysis in a Population-Based, U.S. Sample. J. Clin. Endocrinol. Metab. 2007, 92, 4161–4164. [Google Scholar] [CrossRef][Green Version]
- Wani, K.; Yakout, S.M.; Ansari, M.G.A.; Sabico, S.; Hussain, S.D.; Alokail, M.S.; Sheshah, E.; Aljohani, N.J.; Al-Saleh, Y.; Reginster, J.-Y.; et al. Metabolic Syndrome in Arab Adults with Low Bone Mineral Density. Nutrients 2019, 11, 1405. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.-Y.; Chan, C.Y.; Subramaniam, S.; Muhammad, N.; Fairus, A.; Ng, P.Y.; Jamil, N.A.; Aziz, N.A.; Ima-Nirwana, S.; Mohamed, N. Positive association between metabolic syndrome and bone mineral density among Malaysians. Int. J. Med. Sci. 2020, 17, 2585–2593. [Google Scholar] [CrossRef] [PubMed]
- Society, N.A.M. Management of osteoporosis in postmenopausal women. Menopause 2006, 13, 340–367. [Google Scholar] [CrossRef]
- Anandacoomarasamy, A.; Caterson, I.; Sambrook, P.; Fransen, M.; March, L. The impact of obesity on the musculoskeletal system. Int. J. Obes. 2007, 32, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; Rogucka, E.; Mędraś, M. Are general obesity and visceral adiposity in men linked to reduced bone mineral content resulting from normal ageing? A population-based study. Andrologia 2001, 33, 384–389. [Google Scholar] [CrossRef]
- Greco, E.; Fornari, R.; Rossi, F.; Santiemma, V.; Prossomariti, G.; Annoscia, C.; Aversa, A.; Brama, M.; Marini, M.; Donini, L.M.; et al. Is obesity protective for osteoporosis? Evaluation of bone mineral density in individuals with high body mass index. Int. J. Clin. Pract. 2010, 64, 817–820. [Google Scholar] [CrossRef]
- Moon, S.-S.; Lee, Y.-S.; Kim, S.W. Association of nonalcoholic fatty liver disease with low bone mass in postmenopausal women. Endocrine 2012, 42, 423–429. [Google Scholar] [CrossRef]
- Cao, J.J. Effects of obesity on bone metabolism. J. Orthop. Surg. Res. 2011, 6, 30. [Google Scholar] [CrossRef]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jö Nsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity commissioned by the ILSI Europe Metabolic Syndrome and Diabetes Task Force. Br. J. Nutr. 2011, 106, S1–S78. [Google Scholar] [CrossRef]
- Lecka-Czernik, B.; Moerman, E.J.; Grant, D.F.; Lehmann, J.M.; Manolagas, S.C.; Jilka, R.L. Divergent Effects of Selective Peroxisome Proliferator-Activated Receptor-γ2 Ligands on Adipocyte Versus Osteoblast Differentiation. Endocrinology 2002, 143, 2376–2384. [Google Scholar] [CrossRef]
- Kim, B.-J.; Ahn, S.H.; Bae, S.J.; Kim, E.H.; Kim, T.-H.; Lee, S.H.; Kim, H.-K.; Choe, J.W.; Kim, S.-Y.; Koh, J.-M.; et al. Association between metabolic syndrome and bone loss at various skeletal sites in postmenopausal women: A 3-year retrospective longitudinal study. Osteoporos. Int. 2013, 24, 2243–2252. [Google Scholar] [CrossRef]
- Adami, S.; Braga, V.; Zamboni, M.; Gatti, D.; Rossini, M.; Bakri, J.; Battaglia, E. Relationship Between Lipids and Bone Mass in 2 Cohorts of Healthy Women and Men. Calcif. Tissue Int. 2004, 74, 136–142. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Sugimoto, T.; Yano, S.; Yamauchi, M.; Sowa, H.; Chen, Q.; Chihara, K. Plasma Lipids and Osteoporosis in Postmenopausal Women. Endocr. J. 2002, 49, 211–217. [Google Scholar] [CrossRef]
- Brodeur, M.R.; Brissette, L.; Falstrault, L.; Moreau, R. HDL3reduces the association and modulates the metabolism of oxidized LDL by osteoblastic cells: A protection against cell death. J. Cell. Biochem. 2008, 105, 1374–1385. [Google Scholar] [CrossRef]
- Eren, E.; Ellidag, H.Y.; Aydin, O.; Yılmaz, N. HDL-Associated Paraoxonase 1 as a Bridge between Postmenopausal Osteoporosis and Cardiovascular Disease. Chonnam Med. J. 2014, 50, 75–81. [Google Scholar] [CrossRef][Green Version]
- Inoue, M.; Niki, M.; Ozeki, Y.; Nagi, S.; Chadeka, E.A.; Yamaguchi, T.; Osada-Oka, M.; Ono, K.; Oda, T.; Mwende, F.; et al. High-density lipoprotein suppresses tumor necrosis factor alpha production by mycobacteria-infected human macrophages. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef]
- Vestergaard, P.; Rejnmark, L.; Mosekilde, L. Hypertension Is a Risk Factor for Fractures. Calcif. Tissue Int. 2008, 84, 103–111. [Google Scholar] [CrossRef]
- Ilic, K.; Obradović, N.; Vujasinović-Stupar, N. The Relationship Among Hypertension, Antihypertensive Medications, and Osteoporosis: A Narrative Review. Calcif. Tissue Int. 2012, 92, 217–227. [Google Scholar] [CrossRef]
- Hanley, D.A.; Brown, J.P.; Tenenhouse, A.; Olszynski, W.P.; Ioannidis, G.; Berger, C.; Prior, J.C.; Pickard, L.; Murray, T.M.; Anastassiades, T.; et al. Associations Among Disease Conditions, Bone Mineral Density, and Prevalent Vertebral Deformities in Men and Women 50 Years of Age and Older: Cross-Sectional Results from the Canadian Multicentre Osteoporosis Study. J. Bone Miner. Res. 2003, 18, 784–790. [Google Scholar] [CrossRef]
- Tseng, Y.-H.; Huang, K.-C.; Liu, M.-L.; Shu, W.-T.; Sheu, W.H.-H. Association between metabolic syndrome (MS) and bone mineral loss: A cross-sectional study in Puli Township in Taiwan. Arch. Gerontol. Geriatr. 2009, 49, S37–S40. [Google Scholar] [CrossRef]
- Yang, S.; Nguyen, N.D.; Center, J.R.; Eisman, J.A.; Nguyen, T.V. Association between hypertension and fragility fracture: A longitudinal study. Osteoporos. Int. 2014, 25, 97–103. [Google Scholar] [CrossRef]
- Thrailkill, K.M.; Lumpkin, C.K.; Bunn, R.C.; Kemp, S.F.; Fowlkes, J.L. Is insulin an anabolic agent in bone? Dissecting the diabetic bone for clues. Am. J. Physiol. Metab. 2005, 289, E735–E745. [Google Scholar] [CrossRef] [PubMed]
- Dragsbæk, K.; Neergaard, J.; Laursen, J.M.; Hansen, H.B.; Christiansen, C.; Beck-Nielsen, H.; Karsdal, M.A.; Brix, S.; Henriksen, K. Metabolic syndrome and subsequent risk of type 2 diabetes and cardiovascular disease in elderly women. Medicine 2016, 95, e4806. [Google Scholar] [CrossRef]
- Yaturu, S.; Humphrey, S.; Landry, C.; Jain, S.K. Decreased bone mineral density in men with metabolic syndrome alone and with type 2 diabetes. Med Sci. Monit. 2009, 15, CR5–CR9. [Google Scholar] [PubMed]
- Schwartz, A.V.; Sellmeyer, D.E.; Ensrud, K.E.; Cauley, J.A.; Tabor, H.K.; Schreiner, P.J.; Jamal, S.A.; Black, D.M.; Cummings, S.R. Older Women with Diabetes Have an Increased Risk of Fracture: A Prospective Study. J. Clin. Endocrinol. Metab. 2001, 86, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, A.H.; Nilsson, P.M.; Nilsson, J.-Å.; Åkesson, K. The Association between Hyperglycemia and Fracture Risk in Middle Age. A Prospective, Population-Based Study of 22,444 Men and 10,902 Women. J. Clin. Endocrinol. Metab. 2008, 93, 815–822. [Google Scholar] [CrossRef]
- Nowotny, K.; Jung, T.; Höhn, A.; Weber, D.; Grune, T. Advanced Glycation End Products and Oxidative Stress in Type 2 Diabetes Mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef]
- Suzuki, R.; Fujiwara, Y.; Saito, M.; Arakawa, S.; Shirakawa, J.; Yamanaka, M.; Komohara, Y.; Marumo, K.; Nagai, R. Intracellular Accumulation of Advanced Glycation End Products Induces Osteoblast Apoptosis Via Endoplasmic Reticulum Stress. J. Bone Miner. Res. 2020, 35, 1992–2003. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Lu, H.; Liu, P. Association between essential hypertension and bone mineral density: A systematic review and meta-analysis. Oncotarget 2017, 8, 68916–68927. [Google Scholar] [CrossRef]
- Evans, J.M.; Wang, S.; Greb, C.; Kostas, V.; Knapp, C.F.; Zhang, Q.; Roemmele, E.S.; Stenger, M.B.; Randall, D.C. Body Size Predicts Cardiac and Vascular Resistance Effects on Men’s and Women’s Blood Pressure. Front. Physiol. 2017, 8, 561. [Google Scholar] [CrossRef]
- Jin, N.; Lin, S.; Zhang, Y.; Chen, F. Assess the discrimination of Achilles InSight calcaneus quantitative ultrasound device for osteoporosis in Chinese women: Compared with dual energy X-ray absorptiometry measurements. Eur. J. Radiol. 2010, 76, 265–268. [Google Scholar] [CrossRef]
- Trimpou, P.; Bosaeus, I.; Bengtsson, B.-Å.; Landin-Wilhelmsen, K. High correlation between quantitative ultrasound and DXA during 7 years of follow-up. Eur. J. Radiol. 2010, 73, 360–364. [Google Scholar] [CrossRef]
- Damilakis, J.; Papadokostakis, G.; Perisinakis, K.; Maris, T.G.; Karantanas, A.H. Hip fracture discrimination by the Achilles Insight QUS imaging device. Eur. J. Radiol. 2007, 63, 59–62. [Google Scholar] [CrossRef]
- Stewart, A.; Kumar, V.; Reid, D.M. Long-Term Fracture Prediction by DXA and QUS: A 10-Year Prospective Study. J. Bone Miner. Res. 2005, 21, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Moayyeri, A.; Kaptoge, S.; Dalzell, N.; Bingham, S.; Luben, R.N.; Wareham, N.J.; Reeve, J.; Khaw, K.T. Is QUS or DXA Better for Predicting the 10-Year Absolute Risk of Fracture? J. Bone Miner. Res. 2009, 24, 1319–1325. [Google Scholar] [CrossRef]
- Hans, D.; Baim, S. Quantitative Ultrasound (QUS) in the Management of Osteoporosis and Assessment of Fracture Risk. J. Clin. Densitom. 2017, 20, 322–333. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | MetS (No, No) (n = 19,986) | MetS (No, Yes) (n = 2525) | MetS (Yes, No) (n = 1316) | MetS (Yes, Yes) (n = 3206) |
|---|---|---|---|---|
| Age (year, baseline) | 50.2 ± 10.4 | 52.7 ± 9.9 * | 54.5 ± 9.4 *,† | 54.9 ± 9.3 *,† |
| Age (year, follow-up) | 54.0 ± 10.4 | 56.7 ± 9.8 * | 58.2 ± 9.4 *,† | 58.7 ± 9.3 *,† |
| Male sex (%) | 33.8 | 37.9 * | 42.2 *,† | 40.0 *,†,# |
| Smoking (%) | 23.8 | 29.4 * | 30.9 * | 31.7 * |
| Alcohol (%) | 2.6 | 3.9 * | 3.3 | 4.0 * |
| Regular exercise habits (%) | 48.3 | 46.8 | 54.4 *,† | 46.8 # |
| Diabetes mellitus (%) | 1.9 | 6.3 * | 10.2 *,† | 23.6 *,†,# |
| Hypertension (%) | 7.2 | 17.3 * | 25.2 *,† | 41.7 *,†,# |
| SBP (mmHg, baseline) | 114.0 ± 16.3 | 122.8 ± 16.2 * | 128.3 ± 17.7 *,† | 131.0 ± 17.4 *,†,# |
| SBP (mmHg, follow-up) | 120.4 ± 17.6 | 134.2 ± 17.3 * | 130.8 ± 17.8 *,† | 136.7 ± 18.2 *,†,# |
| DBP (mmHg, baseline) | 70.7 ± 10.2 | 75.3 ± 10.2 * | 78.5 ± 11.0 *,† | 79.2 ± 11.1 *,† |
| DBP (mmHg, follow-up) | 72.0 ± 10.3 | 79.4 ± 10.6 * | 76.9 ± 10.8 *,† | 79.5 ± 11.3 *,† |
| BMI (kg/m2, baseline) | 23.2 ± 3.1 | 25.8 ± 3.3 * | 26.2 ± 3.4 *,† | 27.6 ± 3.7 *,†,# |
| BMI (kg/m2, follow-up) | 23.4 ± 3.2 | 26.5 ± 3.5 * | 25.8 ± 3.3 *,† | 27.7 ± 3.8 *,†,# |
| WC (cm, baseline) | 80.6 ± 8.7 | 87.4 ± 8.8 * | 89.8 ± 8.1 *,† | 92.9 ± 9.0 *,†,# |
| WC (cm, follow-up) | 81.4 ± 8.9 | 90.5 ± 8.6 * | 87.6 ± 8.6 *,† | 89.3 ± 9.1 *,†,# |
| Laboratory parameters | ||||
| Fasting glucose (mg/dL, baseline) | 92.5 ± 12.8 | 99.0 ± 21.5 * | 103.9 ± 25.4 *,† | 113.8 ± 37.7 *,†,# |
| Fasting glucose (mg/dL, follow-up) | 93.1 ± 13.3 | 104.3 ± 27.7 * | 101.8 ± 25.4 *,† | 116.7 ± 38.3 *,†,# |
| Triglyceride (mg/dL, baseline) | 92.2 ± 53.3 | 130.9 ± 71.9 * | 180.7 ± 83.4 *,† | 209.3 ± 139.7 *,†,# |
| Triglyceride (mg/dL, follow-up) | 95.6 ± 53.3 | 187.4 ± 106.0 * | 128.3 ± 67.3 *,† | 216.4 ± 186.3 *,†,# |
| Total cholesterol (mg/dL, baseline) | 194.5 ± 34.5 | 198.4 ± 35.8 * | 200.5 ± 36.3 * | 196.7 ± 39.4 *,# |
| Total cholesterol (mg/dL, follow-up) | 196.9 ± 35.3 | 198.3 ± 37.5 | 194.9 ± 37.0 † | 190.6 ± 40.1 *,†,# |
| HDL cholesterol (mg/dL, baseline) | 57.5 ±12.8 | 48.8 ± 9.8 * | 44.6 ± 8.8 *,† | 42.1 ± 8.3 *,†,# |
| HDL cholesterol (mg/dL, follow-up) | 58.0 ± 13.0 | 44.7 ± 9.0 * | 49.4 ± 9.8 *,† | 42.3 ± 8.6 *,†,# |
| LDL cholesterol (mg/dL, baseline) | 120.7 ± 30.9 | 128.5 ± 32.6 * | 125.8 ± 32.1 * | 120.5 ± 34.1 †,# |
| LDL cholesterol (mg/dL, follow-up) | 120.7 ± 31.0 | 122.7 ± 33.2 * | 122.9 ± 34.0 | 113.7 ± 34.5 *,†,# |
| Hemoglobin (g/dL, baseline) | 13.6 ± 1.5 | 13.9 ± 1.6 * | 14.1 ± 1.6 *,† | 14.2 ± 1.6 *,† |
| Hemoglobin (g/dL, follow-up) | 13.6 ± 1.5 | 14.0 ± 1.5 * | 14.0 ± 1.5 * | 14.1 ± 1.6 * |
| eGFR (mL/min/1.73 m2, baseline) | 110.4 ± 24.8 | 106.6 ± 25.9 * | 104.8 ± 25.2 * | 105.1 ± 28.0 * |
| eGFR (mL/min/1.73 m2, follow-up) | 108.1 ± 24.4 | 103.6 ± 25.7 * | 103.0 ± 25.9 * | 100.9 ± 29.7 *,† |
| Uric acid (mg/dL, baseline) | 5.3 ± 1.3 | 5.9 ± 1.4 * | 6.0 ± 1.4 *,† | 6.3 ± 1.5 *,†,# |
| Uric acid (mg/dL, follow-up) | 5.2 ± 1.3 | 6.0 ± 1.4 * | 5.8 ± 1.4 *,† | 6.1 ± 1.5 *,†,# |
| BMD T-score (baseline) | −0.44 ± 0.01 | −0.50 ± 0.03 | −0.63 ± 0.04 * | −0.65 ± 0.03 *,† |
| BMD T-score (follow-up) | −0.71 ± 0.01 | −0.82 ± 0.03 * | −0.84 ± 0.04 * | −0.88 ± 0.03 * |
| Parameter | Multivariable | |
|---|---|---|
| Unstandardized Coefficient β (95% CI) | p | |
| MetS | −0.126 (−0.179, −0.074) | <0.001 |
| MetS component | ||
| Abdominal obesity | −0.131 (−0.178, −0.084) | <0.001 |
| Hypertriglyceridemia | −0.121 (−0.170, −0.072) | <0.001 |
| Low HDL cholesterol | −0.087 (−0.130, −0.044) | <0.001 |
| Hyperglycemia | 0.038 (−0.022, 0.098) | 0.214 |
| High blood pressure | −0.054 (−0.098, −0.010) | 0.016 |
| MetS and Its Component | Multivariable | |
|---|---|---|
| Unstandardized Coefficient β (95% CI) | p | |
| MetS (no, no) | 0.043 (0, 0.085) | 0.048 |
| MetS (no, yes) | Reference | |
| MetS (yes, no) | 0.101 (0.033, 0.169) | 0.004 |
| MetS (yes, yes) | 0.091 (0.038, 0.144) | 0.001 |
| Abdominal obesity (no, no) | 0.023 (−0.017, 0.063) | 0.268 |
| Abdominal obesity (no, yes) | Reference | |
| Abdominal obesity (yes, no) | 0.048 (−0.009, 0.105) | 0.097 |
| Abdominal obesity (yes, yes) | 0.040 (0, 0.082) | 0.053 |
| Hypertriglyceridemia (no, no) | 0.085 (0.044, 0.126) | <0.001 |
| Hypertriglyceridemia (no, yes) | Reference | |
| Hypertriglyceridemia (yes, no) | 0.144 (0.084, 0.205) | <0.001 |
| Hypertriglyceridemia (yes, yes) | 0.088 (0.037, 0.139) | 0.001 |
| Low HDL cholesterol (no, no) | 0.081 (0.037, 0.125) | <0.001 |
| Low HDL cholesterol (no, yes) | Reference | |
| Low HDL cholesterol (yes, no) | 0.135 (0.076, 0.194) | <0.001 |
| Low HDL cholesterol (yes, yes) | 0.112 (0.062, 0.162) | <0.001 |
| Hyperglycemia (no, no) | 0.053 (−0.004, 0.110) | 0.070 |
| Hyperglycemia (no, yes) | Reference | |
| Hyperglycemia (yes, no) | 0.118 (0.010, 0.227) | 0.033 |
| Hyperglycemia (yes, yes) | 0.106 (0.038, 0.174) | 0.002 |
| High blood pressure (no, no) | 0.036 (−0.028, 0.100) | 0.267 |
| High blood pressure (no, yes) | 0.042 (−0.028, 0.111) | 0.241 |
| High blood pressure (yes, no) | Reference | |
| High blood pressure (yes, yes) | 0.076 (0.009, 0.142) | 0.025 |
| Parameter | Multivariable | |
|---|---|---|
| Unstandardized Coefficient β (95% CI) | p | |
| ΔWC (per 1 cm) | −0.009 (−0.016, −0.002) | 0.009 |
| ΔTG (per 10 mg/dL) | −0.008 (−0.014, −0.003) | 0.004 |
| ΔHDL cholesterol (per 1 mg/dL) | 0.006 (0, 0.012) | 0.034 |
| Δfasting glucose (per 1 mg/dL) | −0.002 (−0.003, 0) | 0.051 |
| ΔSBP (per 1 mmHg) | 0.003 (0, 0.005) | 0.020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, H.; Lee, M.-Y.; Wu, P.-Y.; Huang, J.-C.; Chen, S.-C. Development of Metabolic Syndrome Decreases Bone Mineral Density T-Score of Calcaneus in Foot in a Large Taiwanese Population Follow-Up Study. J. Pers. Med. 2021, 11, 439. https://doi.org/10.3390/jpm11050439
Chiu H, Lee M-Y, Wu P-Y, Huang J-C, Chen S-C. Development of Metabolic Syndrome Decreases Bone Mineral Density T-Score of Calcaneus in Foot in a Large Taiwanese Population Follow-Up Study. Journal of Personalized Medicine. 2021; 11(5):439. https://doi.org/10.3390/jpm11050439
Chicago/Turabian StyleChiu, Hsuan, Mei-Yueh Lee, Pei-Yu Wu, Jiun-Chi Huang, and Szu-Chia Chen. 2021. "Development of Metabolic Syndrome Decreases Bone Mineral Density T-Score of Calcaneus in Foot in a Large Taiwanese Population Follow-Up Study" Journal of Personalized Medicine 11, no. 5: 439. https://doi.org/10.3390/jpm11050439
APA StyleChiu, H., Lee, M.-Y., Wu, P.-Y., Huang, J.-C., & Chen, S.-C. (2021). Development of Metabolic Syndrome Decreases Bone Mineral Density T-Score of Calcaneus in Foot in a Large Taiwanese Population Follow-Up Study. Journal of Personalized Medicine, 11(5), 439. https://doi.org/10.3390/jpm11050439