
Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study

 , and
, and 
Abstract
1. Introduction
2. Methodology
2.1. Design and Participants
2.2. Data Collection and Information Sources
2.3. Statistical Analysis
3. Results
Characteristics of Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Mental Health Aspects of Women’s Reproductive Health: A Global Review of the Literature. WHO Press, 2009. Available online: http://apps.who.int/iris/bitstream/handle/10665/43846/9789241563567_eng.pdf;jsessionid=1A812923347FE5054B9FAFCA9CCA9E96?sequence=1 (accessed on 15 October 2020).
- Flores-Ramos, M. Mental health in pregnant women. Perinatol Hum Reprod. 2013, 27, 4–143. [Google Scholar]
- Beck, C.T.; Casavant, S. Synthesis of Mixed Research on Posttraumatic Stress Related to Traumatic Birth. J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 385–397. [Google Scholar] [CrossRef]
- Cook, N.; Ayers, S.; Horsch, A. Maternal posttraumatic stress disorder during the perinatal period and child outcomes: A systematic review. J. Affect. Disord. 2018, 225, 18–31. [Google Scholar] [CrossRef]
- Grekin, R.; O’Hara, M.W. Prevalence and risk factors of postpartum posttraumatic stress disorder: A meta-analysis. Clin. Psychol. Rev. 2014, 34, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Khoramroudi, R. The prevalence of posttraumatic stress disorder during pregnancy and postpartum period. J. Fam. Med. Prim. Care 2018, 7, 220–223. [Google Scholar] [CrossRef]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Factors associated with post-traumatic stress symptoms (PTSS) 4–6 weeks and 6 months after birth: A longitudinal population-based study. J. Affect. Disord. 2017, 221, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, P.D.; Ayers, S.; Phillips, L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord. 2017, 208, 634–645. [Google Scholar] [CrossRef]
- Ayers, S. Delivery as a Traumatic Event: Prevalence, Risk Factors, and Treatment for Postnatal Posttraumatic Stress Disorder. Clin. Obstet. Gynecol. 2004, 47, 552–567. [Google Scholar] [CrossRef]
- Olde, E.; van der Hart, O.; Kleber, R.; van Son, M. Posttraumatic stress following childbirth: A review. Clin. Psychol. Rev. 2006, 26, 1–16. [Google Scholar] [CrossRef]
- Ferguson, R. Recognizing postpartum posttraumatic stress disorder. Nursery 2018, 48, 14. [Google Scholar] [CrossRef]
- Garthus-Niegel, S.; Horsch, A.; Handtke, E.; Von Soest, T.; Ayers, S.; Weidner, K.; Eberhard-Gran, M. The Impact of Postpartum Posttraumatic Stress and Depression Symptoms on Couples’ Relationship Satisfaction: A Population-Based Prospective Study. Front. Psychol. 2018, 9, 1728. [Google Scholar] [CrossRef] [PubMed]
- Nerum, H.; Halvorsen, L.; Sørlie, T.; Øian, P. Maternal Request for Cesarean Section due to Fear of Birth: Can It Be Changed Through Crisis-Oriented Counseling. Birth 2006, 33, 221–228. [Google Scholar] [CrossRef]
- Wilson, C.K.; Padron, E.; Samuelson, K.W. Trauma Type and Posttraumatic Stress Disorder as Predictors of Parenting Stress in Trau-ma-Exposed Mothers. Violence Vict. 2017, 32, 141–158. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.T. Post-traumatic stress disorder due to childbirth: The aftermath. Nurs Res. 2004, 53, 216–224. [Google Scholar] [CrossRef]
- Lev-Wiesel, R.; Daphna-Tekoah, S.; Hallak, M. Childhood sexual abuse as a predictor of birth-related posttraumatic stress and post-partum posttraumatic stress. Child Abus Negl. 2009, 33, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Muzik, M.; McGinnis, E.W.; Bocknek, E.; Morelen, D.; Rosenblum, K.L.; Liberzon, I.; Seng, J.; Abelson, J.L. PTSD Symptoms Across Pregnancy and Early Postpartum Among Women with Lifetime PTSD Diagnosis. Depress. Anxiety 2016, 33, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Martínez, A.; Rodríguez-Almagro, J.; Molina-Alarcón, M.; Infante-Torres, N.; Rubio-Álvarez, A.; Martínez-Galiano, J.M. Peri-natal factors related to post-traumatic stress disorder symptoms 1–5 years following birth. Women Birth. 2020, 33, 129–135. [Google Scholar] [CrossRef]
- Zaat, T.R.; van Steijn, M.E.; de Haan-Jebbink, J.M.; Olff, M.; Stramrood, C.A.I.; van Pampus, M.G. Posttraumatic stress disorder related to postpartum haemorrhage: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 225, 20–214. [Google Scholar] [CrossRef]
- Çapik, A.; Durmaz, H. Fear of Childbirth, Postpartum Depression, and Birth-Related Variables as Predictors of Posttraumatic Stress Disorder After Childbirth. Worldviews Evid. Based Nurs. 2018, 15, 455–463. [Google Scholar] [CrossRef]
- Angelini, C.R.; Pacagnella, R.C.; Parpinelli, M.A.; Silveira, C.; Andreucci, C.B.; Ferreira, E.C. Post-Traumatic Stress Disorder and se-vere maternal morbidity: Is there an association? Clinics 2018, 73, 309. [Google Scholar] [CrossRef]
- van Heumen, M.A.; Hollander, M.H.; van Pampus, M.G.; van Dillen, J.; Stramrood, C.A. Psychosocial Predictors of Postpartum Posttrau-matic Stress Disorder in Women with a Traumatic Childbirth Experience. Front. Psychiatry 2018, 9, 348. [Google Scholar] [CrossRef] [PubMed]
- Dekel, S.; Stuebe, C.; Dishy, G. Childbirth Induced Posttraumatic Stress Syndrome: A Systematic Review of Prevalence and Risk Factors. Front. Psychol. 2017, 8, 560. [Google Scholar] [CrossRef] [PubMed]
- Garthus-Niegel, S.; Horsch, A.; Ayers, S.; Junge-Hoffmeister, J.; Weidner, K.; Eberhard-Gran, M. The influence of postpartum PTSD on breastfeeding: A longitudinal population-based study. Birth 2018, 45, 193–201. [Google Scholar] [CrossRef]
- Thomson, G.; Downe, S. Widening the trauma discourse: The link between childbirth and experiences of abuse. J. Psychosom. Obstet. Gynecol. 2008, 29, 268–273. [Google Scholar] [CrossRef]
- Sando, D.; Abuya, T.; Asefa, A.; Banks, K.P.; Freedman, L.P.; Kujawski, S.; Markovitz, A.; Ndwiga, C.; Ramsey, K.; Ratcliffe, H.; et al. Methods used in prevalence studies of disrespect and abuse during facility based childbirth: Lessons learned. Reprod. Health 2017, 14, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Bohren, M.A.; Mehrtash, H.; Fawole, B.; Maung, T.M.; Balde, M.D.; Maya, E. How women are treated during facility-based childbirth in four countries: A cross-sectional study with labour observations and community-based surveys. Lancet 2019, 394, 1750–1763. [Google Scholar] [CrossRef]
- Siraj, A.; Teka, W.; Hebo, H. Prevalence of disrespect and abuse during facility based child birth and associated factors, Jimma University Medical Center, Southwest Ethiopia. BMC Pregnancy Childbirth 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Martínez-Galiano, J.M.; Martinez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martinez, A. The magnitude of the problem of obstetric violence and its associated factors: A cross-sectional study. Women Birth 2020, S1871-5192(20)30359-0. [Google Scholar] [CrossRef]
- World Health Organization. WHO recommendations on health promotion interventions for maternal and newborn health. Matern. Newborn Child Adolesc. Health 2015, 1, 90. [Google Scholar]
- Ayers, S.; Bond, R.; Bertullies, S.; Wijma, K. The aetiology of post-traumatic stress following childbirth: A meta-analysis and theoretical framework. Psychol. Med. 2016, 46, 1121–1134. [Google Scholar] [CrossRef]
- Andersen, L.B.; Melvaer, L.B.; Videbech, P.; Lamont, R.F.; Joergensen, J.S. Risk factors for developing post-traumatic stress disorder following childbirth: A systematic review. ACTA Obstet. Gynecol. Scand. 2012, 91, 1261–1272. [Google Scholar] [CrossRef]
- Callister, L.C. Making meaning: Women’s birth narratives. J. Obstet. Gynecol. Neonatal. Nurs. JOGNN 2004, 33, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Dekel, S.; Thiel, F.; Dishy, G.; Ashenfarb, A.L. Is childbirth-induced PTSD associated with low maternal attachment? Arch. Women. Ment. Health 2019, 22, 119–122. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Martínez, A.H.; Rodríguez-Almagro, J.; Molina-Alarcón, M.; Infante-Torres, N.; Manzanares, M.D.; Martínez-Galiano, J.M. Postpartum post-traumatic stress disorder: Associated perinatal factors and quality of life. J. Affect. Disord. 2019, 249, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Callahan, J.L.; Borja, S.E.; Hynan, M.T. Modification of the Perinatal PTSD Questionnaire to enhance clinical utility. J. Perinatol. 2006, 26, 533–539. [Google Scholar] [CrossRef]
- Kim, W.J.; Lee, E.; Kim, K.R.; Namkoong, K.; Park, E.S.; Rha, D.-W. Progress of PTSD symptoms following birth: A prospective study in mothers of high-risk infants. J. Perinatol. 2015, 35, 575–579. [Google Scholar] [CrossRef]
- Smith, T.; Gemmill, A.W.; Milgrom, J. Perinatal anxiety and depression: Awareness and attitudes in Australia. Int. J. Soc. Psychiatry 2019, 65, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Vignato, J.; Georges, J.M.; Bush, R.A.; Connelly, C.D. Post-traumatic stress disorder in the perinatal period: A concept analysis. J. Clin. Nurs. 2017, 26, 3859–3868. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, I.J.; Redshaw, M. Mode of birth and women’s psychological and physical wellbeing in the postnatal period. BMC Pregnancy Childbirth 2012, 12, 138. [Google Scholar] [CrossRef]
- Ryding, E.L.; Wijma, K.; Wijma, B. Psychological impact of emergency cesarean section in comparison with elective cesarean section, instrumental and normal vaginal delivery. J. Psychosom. Obstet. Gynaecol. 1998, 19, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodi, Z.; Dolatian, M.; Shaban, Z.; Shams, J.; Alavi-Majd, H.; Mirabzadeh, A. Correlation between Kind of Delivery and Posttrau-matic Stress Disorder. Ann. Med. Health Sci. Res. 2016, 6, 61–356. [Google Scholar]
- Olieman, R.M.; Siemonsma, F.; Bartens, M.A.; Garthus-Niegel, S.; Scheele, F.; Honig, A. The effect of an elective cesarean section on maternal request on peripartum anxiety and depression in women with childbirth fear: A systematic review. BMC Pregnancy Childbirth 2017, 17, 1–8. [Google Scholar] [CrossRef]
- Aftyka, A.; Rybojad, B.; Rozalska-Walaszek, I.; Rzoñca, P.; Humeniuk, E. Post-traumatic stress disorder in parents of children hospitalized in the neonatal intensive care unit (NICU): Medical and demographic risk factors. Psychiatr. Danub. 2014, 26, 347–352. [Google Scholar]
- Lefkowitz, D.S.; Baxt, C.; Evans, J.R. Prevalence and correlates of posttraumatic stress and postpartum depression in parents of in-fants in the Neonatal Intensive Care Unit (NICU). J. Clin. Psychol. Med. Settings 2010, 17, 7–230. [Google Scholar] [CrossRef] [PubMed]
- van Dinter-Douma, E.E.; de Vries, N.E.; Aarts-Greven, M.; Stramrood, C.A.I.; van Pampus, M.G. Screening for trauma and anxiety recognition: Knowledge, management and attitudes amongst gynecologists regarding women with fear of childbirth and postpartum post-traumatic stress disorder. J. Matern. Fetal. Neonatal. Med. 2018, 12, 1–281. [Google Scholar] [CrossRef]
- Spanish Ministry of Health. Strategy on Care for Normal Childbirth in the National Health System (Spain). Clin. Pract. Guidel. Care Norm. Childbirth. 2015. Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/InformeFinalEAPN_revision8marzo2015.pdf (accessed on 15 October 2020).
- Imširagić, A.S.; Begić, D.; Sarajlić, I.; Palavra, I.R.; Orban, M. Predictors of Exclusive Breastfeeding 6–9 Weeks After Delivery: A Pro-spective Cohort Study. Public Mental Health Perspective. Psychiatr. Danub. 2016, 28, 395–403. [Google Scholar]


{kind=link}
| Variable | n (%) | Mean (SD) |
|---|---|---|
| Maternal age | 35.2 (4.25) | |
| Weight before pregnancy (mean) | 65.8 (13.24) | |
| Weight after pregnancy (mean) | 77.3 (12.96) | |
| Months from last child | 5.4 (3.42) | |
| Pre-gestational BMI | 24.4 (4.85) | |
| Education level | ||
| Primary school | 15 (1.7) | |
| Secondary school | 61 (6.8) | |
| High school | 199 (22.1) | |
| University | 624 (69.4) | |
| Current working status | ||
| Full-time work | 277 (30.8) | |
| Part-time work | 131 (14.6) | |
| Sick leave | 189 (21.0) | |
| Unpaid leave | 103 (11.5) | |
| Unemployed | 199 (22.1) | |
| Nationality | ||
| Spanish | 868 (96.6) | |
| Other | 31 (3.4) | |
| Family monthly wage | ||
| Less than 1000 euros | 46 (5.1) | |
| Between 1000 and 2000 euros | 319 (35.5) | |
| Between 2000 and 3000 euros | 282 (31.4) | |
| Between 3000 and 4000 euros | 78 (8.7) | |
| Planned pregnancy | ||
| No | 64 (7.1) | |
| Yes | 835 (92.9) | |
| Number of pregnancies | ||
| One | 363 (40.4) | |
| Two | 329 (36.6) | |
| Three | 138 (15.4) | |
| Four | 45 (5) | |
| Five or more | 24 (2.7) | |
| Number of vaginal births | ||
| None | 170 (18.9) | |
| One | 402 (44.7) | |
| Two | 283 (31.5) | |
| Three or more | 43 (4.8) | |
| Place of birth | ||
| Public hospital | 736 (81.9) | |
| Private hospital | 152 (16.9) | |
| Midwife-led hospital | 3 (0.3) | |
| Home | 8 (0.9) | |
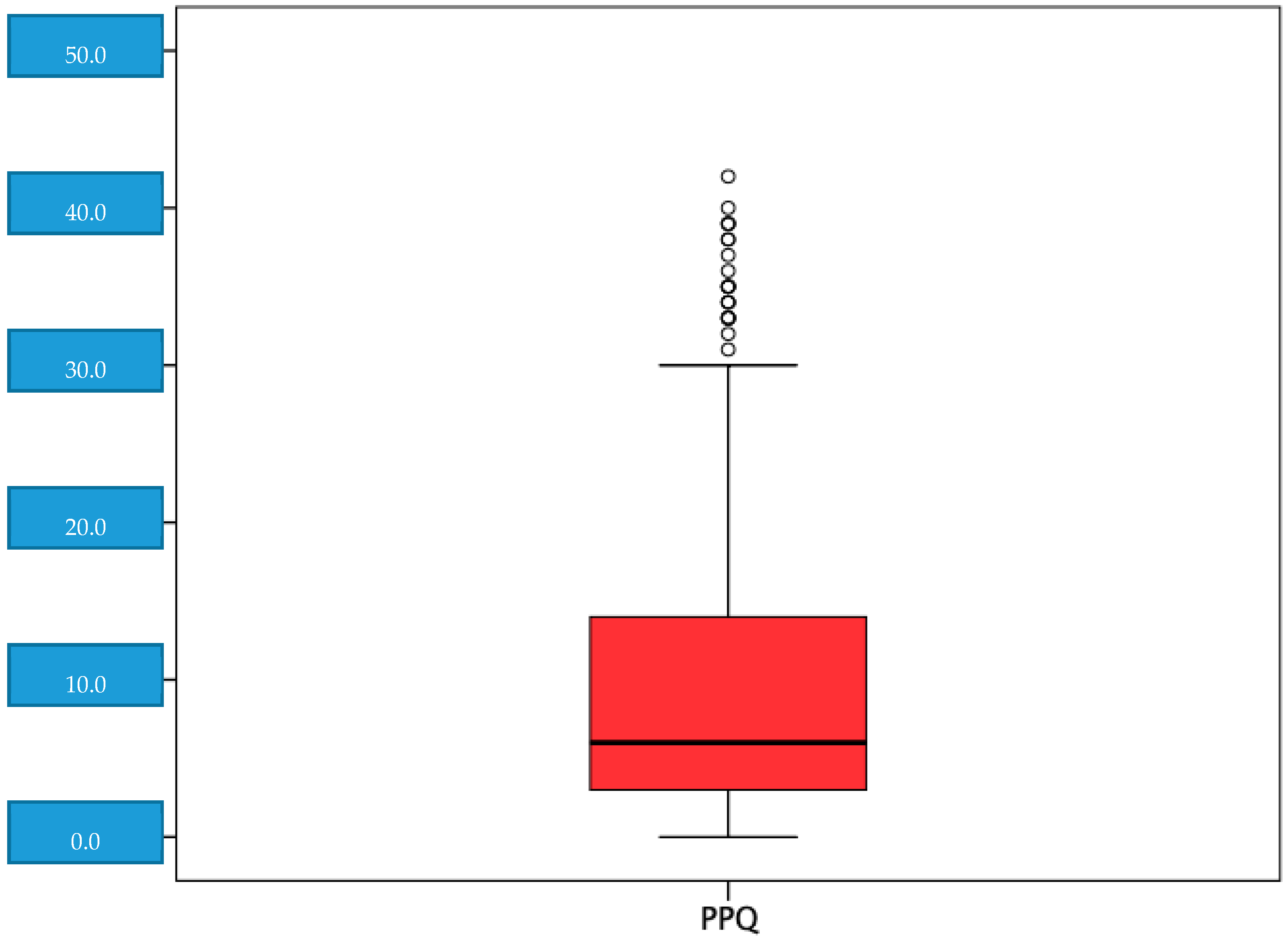
| PPQ | 9.10 (8.52) | |
| Score < 19 | 785 (87.3) | |
| Score ≥ 19 | 114 (12.7) |
| Variable | Obstetric Violence & PTSD Risk | |||
|---|---|---|---|---|
| Score < 19 | Score ≥ 19 | OR (95% CI) | aOR (95% CI) | |
| Maternal age | ||||
| ≤35 years | 404 (87.3) | 59 (12.7) | 1 (ref.) | |
| >35 years | 381 (87.4) | 55 (12.6) | 0.99 (0.67, 1.47) | |
| Academic level | ||||
| Primary school | 15 (100.0) | 0 (0.0) | ||
| Secondary school | 53 (88.3) | 7 (11.7) | NC | |
| High school | 173 (86.9) | 26 (13.1) | NC | |
| University | 544 (87.0) | 81 (13.0) | NC | |
| Current working status | ||||
| Full-time work | 242 (87.4) | 35 (12.6) | 1 (ref.) | |
| Part-time work | 113 (86.3) | 18 (13.7) | 1.10 (0.60, 2.02) | |
| Sick leave | 167 (88.4) | 22 (11.6) | 0.91 (0.52, 1.61) | |
| Unpaid leave | 88 (85.4) | 15 (14.6) | 1.18 (0.61, 2.26) | |
| Unemployed | 175 (87.9) | 24 (12.1) | 0.95 (0.55, 1.65) | |
| Nationality | ||||
| Spanish | 760 (87.6) | 108 (12.4) | 1 (ref.) | |
| Other | 25 (80.6) | 6 (19.4) | 1.69 (0.68, 4.21) | |
| Family monthly wage | ||||
| Less than 1000 euros | 40 (87.0) | 6 (13.0) | 1 (ref.) | |
| Between 1000 and 2000 euros | 271 (85.0) | 48 (15.0) | 1.18 (0.48, 2.94) | |
| Between 2000 and 3000 euros | 251 (89.0) | 31 (11.0) | 0.82 (0.32, 2.10) | |
| Between 3000 and 4000 euros | 154 (88.5) | 20 (11.5) | 0.87 (0.33, 2.30) | |
| More than 4000 euros | 69 (88.5) | 9 (11.5) | 0.87 (0.29, 2.62) | |
| Planned pregnancy | ||||
| No | 56 (87.5) | 8 (12.5) | 1 (ref.) | |
| Yes | 729 (87.3) | 106 (12.7) | 1.02 (0.47, 2.20) | |
| Maternal antenatal classes | ||||
| No | 161 (89.0) | 20 (11.0) | 1 (ref.) | |
| Yes (less than 5 classes) | 113 (85.6) | 19 (14.4) | 1.35 (0.69, 2.65) | |
| Yes (more than 5 classes) | 511 (87.2) | 75 (12.8) | 1.18 (0.70, 2.00) | |
| Birth plan | ||||
| No | 436 (89.7) | 50 (10.3) | 1 (ref.) | 1 (ref.) |
| Yes, but not respected | 59 (60.8) | 38 (39.2) | 5.62 (3.40, 9.28) | 2.85 (1.56, 5.21) |
| Yes, and was respected | 290 (91.8) | 26 (8.2) | 0.78 (0.48, 1.29) | 1.49 (0.82, 2.70) |
| Twin pregnancy | ||||
| No | 769 (87.3) | 112 (12.7) | 1 (ref.) | |
| Yes | 16 (88.9) | 2 (11.1) | 0.86 (0.20, 3.78) | |
| Live newborn | ||||
| No | 3 (50.0) | 3 (50.0) | 1 (ref.) | |
| Yes | 782 (87.6) | 111 (12.4) | 0.14 (0.03, 0.71) | |
| Parity | ||||
| Primiparous | 1 (ref.) | |||
| Multiparous | 0.40 (0.25, 0.65) | |||
| Induction of labour | ||||
| No | 491 (89.8) | 56 (10.2) | 1 (ref.) | |
| Yes | 294 (83.5) | 58 (16.5) | 1.73 (1.17, 2.57) | |
| Natural analgesia | ||||
| No | 631 (86.7) | 97 (13.3) | 1 (ref.) | |
| Yes | 154 (90.1) | 17 (9.9) | 0.72 (0.42, 1.24) | |
| Regional analgesia | ||||
| No | 232 (91.0) | 23 (9.0) | 1 (ref.) | |
| Yes | 553 (85.9) | 91 (14.1) | 1.66 (1.03, 2.69) | |
| General anaesthesia | ||||
| No | 763 (87.8) | 106 (12.2) | 1 (ref.) | |
| Yes | 22 (73.3) | 8 (26.7) | 2.62 (1.14, 6.03) | |
| Type of birth | ||||
| Normal vaginal delivery | 500 (92.8) | 39 (7.2) | 1 (ref.) | 1 (ref.) |
| Instrumental | 150 (88.2) | 20 (11.8) | 1.39 (0.92, 2.09) | 1.08 (0.56, 2.11) |
| Elective C/S | 48 (80.0) | 12 (20.0) | 1.08 (0.56, 2.08) | 2.53 (1.02, 2.26) |
| Emergency C/S | 87 (66.9) | 43 (33.1) | 2.09 (1.35, 3.23) | 3.58 (1.83, 6.99) |
| Episiotomy | ||||
| No | 567 (86.2) | 91 (13.8) | 1 (ref.) | |
| Yes | 218 (90.5) | 23 (9.5) | 0.66 (0.41, 1.07) | |
| Perineal tear | ||||
| No | 453 (84.5) | 83 (15.5) | 1 (ref.) | |
| Mild | 306 (92.2) | 26 (7.8) | 0.46 (0.29, 0.74) | |
| Severe | 26 (83.9) | 5 (16.1) | 1.05 (0.39, 2.81) | |
| Skin-to-skin | ||||
| No | 135 (71.4) | 54 (28.6) | 1 (ref.) | |
| Yes | 650 (91.5) | 60 (8.5) | 0.23 (0.15, 0.35) | |
| Breastfeeding 1 h after childbirth | ||||
| No | 171 (78.1) | 48 (21.9) | 1 (ref.) | 1 (ref.) |
| Yes | 614 (90.3) | 66 (9.7) | 0.38 (0.25, 0.58) | 0.48 (0.26, 0.87) |
| Admission of the new born to care unit | ||||
| No | 699 (89.8) | 79 (10.2) | 1 (ref.) | 1 (ref.) |
| Intermediate care | 38 (64.4) | 21 (35.6) | 4.89 (2.73, 8.75) | 4.95 (2.36, 10.36) |
| NICU | 48 (77.4) | 14 (22.6) | 2.58 (1.36, 4.89) | 2.25 (1.02, 4.97) |
| Place of birth | ||||
| Public hospital | 646 (87.8) | 90 (12.2) | 1 (ref.) | |
| Private hospital | 128 (84.2) | 24 (15.8) | 1.35 (0.83, 2.19) | |
| Midwife-led hospital | 3 (100.0) | 0 (0.0) | 0.00 (0.00, 0.00) | |
| Home | 8 (100.0) | 0 (0.0) | 0.00 (0.00, 0.00) | |
| Hospital length of stay | ||||
| 1 day | 66 (94.3) | 4 (5.7) | 1 (ref.) | |
| 2 day | 412 (93.2) | 30 (6.8) | 1.20 (0.41, 3.52) | |
| 3 day | 203 (83.9) | 39 (16.1) | 3.17 (1.09, 9.20) | |
| 4 days or more | 104 (71.7) | 41 (28.3) | 6.51 (2.23, 19.00) | |
| Partner support during childbirth | ||||
| None | 8 (44.4) | 10 (55.6) | 1 (ref.) | 1 (ref.) |
| Little | 19 (54.3) | 16 (45.7) | 0.67 (0.22, 2.11) | 0.74 (0.19, 2.86) |
| Something | 47 (83.9) | 9 (16.1) | 0.15 (0.05, 0.49) | 0.16 (0.04, 0.63) |
| Quite | 198 (88.0) | 27 (12.0) | 0.11 (0.04, 0.30) | 0.17 (0.05, 0.57) |
| A lot | 513 (90.8) | 52 (9.2) | 0.08 (0.03, 0.21) | 0.17 (0.06, 0.53) |
| Infant feeding on discharge | ||||
| Maternal | 362 (90.0) | 70 (10.0) | 1 (ref.) | 1 (ref.) |
| Mixed | 126 (78.3) | 35 (21.7) | 2.51 (1.60, 3.91) | 1.42 (0.81, 2.49) |
| Artificial | 27 (75.0) | 9 (25.0) | 3.01 (1.36, 6.66) | 3.57 (1.32, 9.69) |
| Postpartum surgical intervention | ||||
| No | 759 (88.1) | 103 (11.9) | 1 (ref.) | |
| Yes | 26 (70.3) | 11 (29.7) | 3.12 (1.50, 6.50) | |
| Maternal ITU admission | ||||
| No | 785 (87.3) | 114 (12.7) | NC | |
| Yes | 0 (0.0) | 0 (0.0) | ||
| Hospital readmission | ||||
| No | 764 (87.6) | 108 (12.4) | 1 (ref.) | |
| Yes | 21 (77.8) | 6 (22.2) | 2.02 (0.80, 5.12) | |
| Verbal violence | ||||
| No | 632 (93.9) | 41 (6.1) | 1 (ref.) | 1 (ref.) |
| Yes | 153 (67.7) | 73 (32.3) | 7.36 (4.83, 11.21) | 5.07 (2.98, 8.63) |
| Physical violence | ||||
| No | 381 (93.2) | 28 (6.8) | 1 (ref.) | |
| Yes | 404 (82.4) | 86 (17.6) | 2.90 (1.85, 5.54) | |
| Psych-affective violence | ||||
| No | 544 (95.6) | 25 (4.4) | 1 (ref.) | 1 (ref.) |
| Yes | 241 (83.0) | 89 (27.0) | 8.04 (5.03, 12.84) | 2.61 (1.45, 4.67) |
| Violence (dichotomous) | ||||
| No | 283 (96.6) | 10 (3.4) | 1 (ref.) | |
| Yes | 502 (82.8) | 104 (17.2) | 5.86 (3.02, 11.40) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Vázquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Martínez-Galiano, J.M. Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study. J. Pers. Med. 2021, 11, 338. https://doi.org/10.3390/jpm11050338
Martinez-Vázquez S, Rodríguez-Almagro J, Hernández-Martínez A, Martínez-Galiano JM. Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study. Journal of Personalized Medicine. 2021; 11(5):338. https://doi.org/10.3390/jpm11050338
Chicago/Turabian StyleMartinez-Vázquez, Sergio, Julián Rodríguez-Almagro, Antonio Hernández-Martínez, and Juan Miguel Martínez-Galiano. 2021. "Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study" Journal of Personalized Medicine 11, no. 5: 338. https://doi.org/10.3390/jpm11050338
APA StyleMartinez-Vázquez, S., Rodríguez-Almagro, J., Hernández-Martínez, A., & Martínez-Galiano, J. M. (2021). Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study. Journal of Personalized Medicine, 11(5), 338. https://doi.org/10.3390/jpm11050338