
H-Wave® Device Stimulation: A Critical Review

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of This Study
Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items
2.7. Risk of Bias and Methodological Weaknesses
2.8. Data Synthesis
3. Results
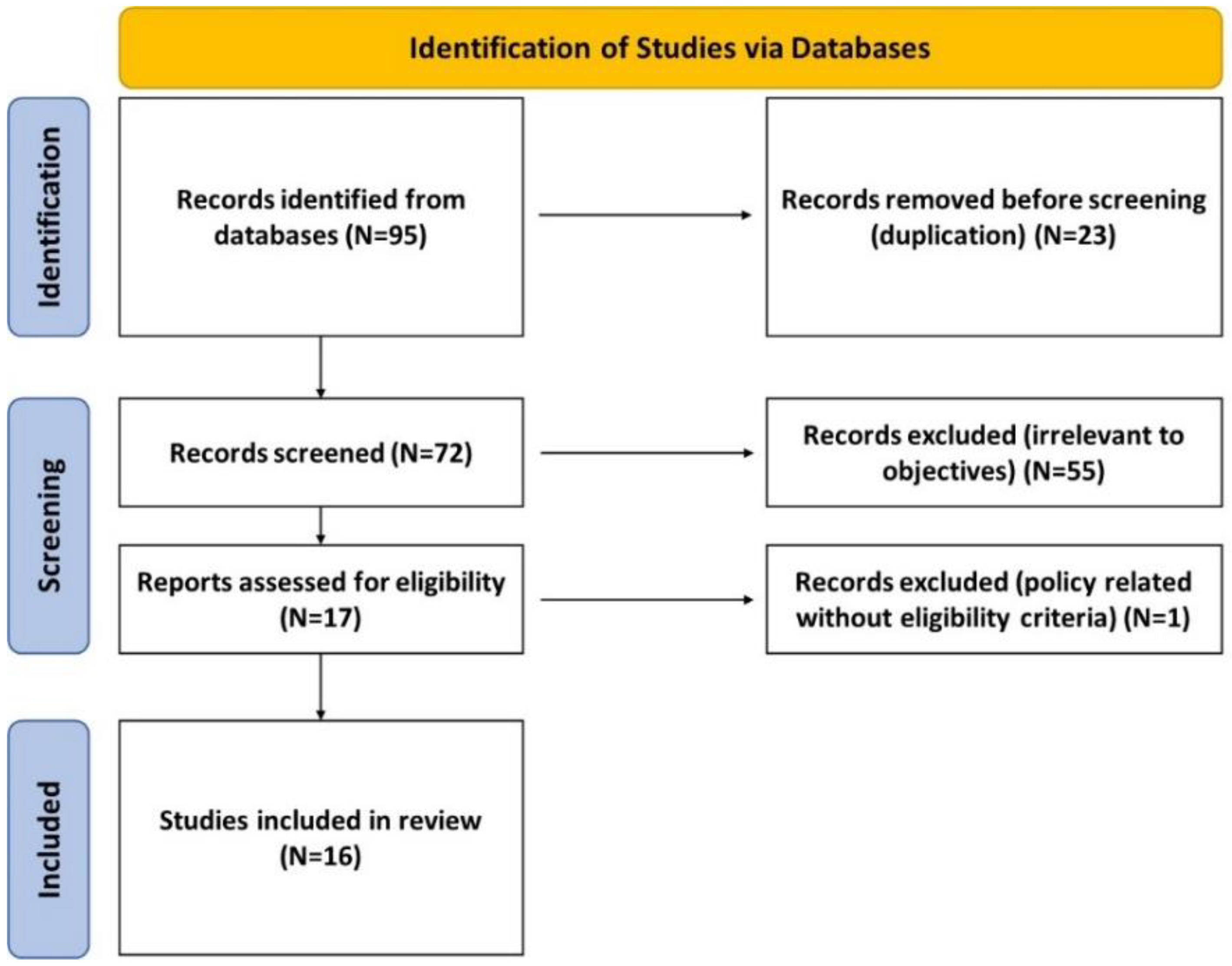
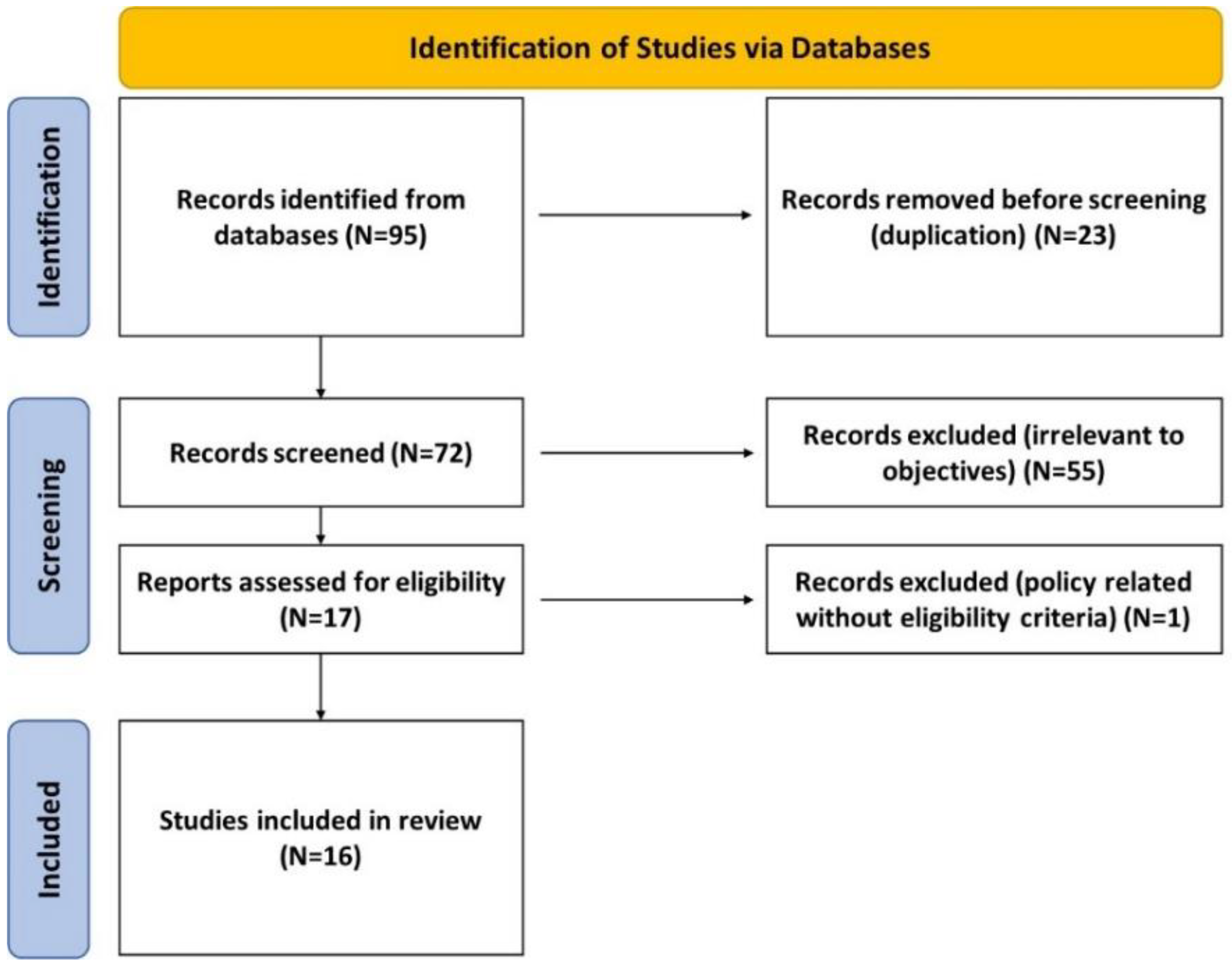
3.1. Search Results
3.2. Pre-Clinical Studies
3.2.1. H-Wave Technology
3.2.2. Blood Flow Effects
3.2.3. Muscle Contraction Effects
3.2.4. Nerve Action Potential Effects
3.2.5. Lymphatic Function Effects
3.3. Clinical Studies
3.3.1. Pain
3.3.2. Functionality
3.3.3. Pain Medication Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nahin, R.L. Estimates of pain prevalence and severity in adults: United States, 2012. J. Pain 2015, 16, 769–780. [Google Scholar] [CrossRef] [Green Version]
- Alford, D.P.; Krebs, E.E.; Chen, I.A.; Nicolaidis, C.; Bair, M.J.; Liebschutz, J. Update in pain medicine. J. Gen. Intern. Med. 2010, 25, 1222–1226. [Google Scholar] [CrossRef]
- Pizzo, P.A.; Clark, N.M. Alleviating suffering 101—Pain relief in the United States. N. Engl. J. Med. 2012, 366, 197–199. [Google Scholar] [CrossRef] [Green Version]
- Torrance, N.; Ferguson, J.A.; Afolabi, E.; Bennett, M.I.; Serpell, M.G.; Dunn, K.M.; Smith, B.H. Neuropathic pain in the community: More under-treated than refractory? PAIN® 2013, 154, 690–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bovill, J.G. Mechanisms of actions of opioids and non-steroidal anti-inflammatory drugs. Eur. J. Anaesthesiol. Suppl. 1997, 15, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.; Oscar-Berman, M.; Dinubile, N.; Giordano, J.; Braverman, E.R.; Truesdell, C.E.; Barh, D.; Badgaiyan, R. Coupling Genetic Addiction Risk Score (GARS) with Electrotherapy: Fighting Iatrogenic Opioid Dependence. J. Addict. Res. Ther. 2013, 4, 1000163. [Google Scholar]
- Smith, H.S. Potential analgesic mechanisms of acetaminophen. Pain Phys. 2009, 12, 269–280. [Google Scholar] [CrossRef]
- Lee, W.M. Acetaminophen (APAP) hepatotoxicity-Isn’t it time for APAP to go away? J. Hepatol. 2017, 67, 1324–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeki, S. Side Effects of Acetaminophen and their Management. Masui 2016, 65, 701–708. [Google Scholar] [PubMed]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- McGrane, N.; Galvin, R.; Cusack, T.; Stokes, E. Addition of motivational interventions to exercise and traditional physiotherapy: A review and meta-analysis. Physiotherapy 2015, 101, 1–12. [Google Scholar] [CrossRef]
- Flynn, D.M. Chronic Musculoskeletal Pain: Nonpharmacologic, Noninvasive Treatments. Am. Fam. Phys. 2020, 102, 465–477. [Google Scholar]
- Attal, N.; Lanteri-Minet, M.; Laurent, B.; Fermanian, J.; Bouhassira, D. The specific disease burden of neuropathic pain: Results of a French nationwide survey. Pain 2011, 152, 2836–2843. [Google Scholar] [CrossRef]
- Smith, T.L.; Blum, K.; Callahan, M.F.; DiNubile, N.; Chen, T.J.; Waite, R.L. H-Wave induces arteriolar vasodilation in rat striated muscle via nitric oxide-mediated mechanisms. J. Orthop. Res. Off. Publ. Orthop. Res. Society. 2009, 27, 1248–1251. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.L.; Callahan, M.F.; Blum, K.; Dinubile, N.A.; Chen, T.J.; Waite, R.L. H-Wave effects on blood flow and angiogenesis in longitudinal studies in rats. J. Surg. Orthop. Adv. 2011, 20, 255–259. [Google Scholar]
- Blum, K.; Chen, A.L.; Chen, T.J.; Prihoda, T.J.; Schoolfield, J.; DiNubile, N.; Waite, R.L.; Arcuri, V.; Kerner, M.; Braverman, E.R.; et al. The H-Wave device is an effective and safe non-pharmacological analgesic for chronic pain: A meta-analysis. Adv. Ther. 2008, 25, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.; Ho, C.K.; Chen, A.L.; Fulton, M.; Fulton, B.; Westcott, W.L.; Reinl, G.; Braverman, E.R.; DiNubile, N.; Chen, T.J.H.; et al. The H-Wave Device Induces NO-Dependent Augmented Microcirculation and Angiogenesis, Providing Both Analgesia and Tissue Healing in Sports Injuries. Phys. Sportsmed. 2008, 36, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Julka, I.S.; Alvaro, M.; Kumar, D. Beneficial effects of electrical stimulation on neuropathic symptoms in diabetes patients. J. Foot Ankle Surg. 1998, 37, 191–194. [Google Scholar] [CrossRef]
- O’Connor, D.; Green, S.; Higgins, J.P. Defining the Review Question and Developing Criteria for Including Studies. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P., Green, S., Eds.; John Wiley and Sons: Chichester, UK, 2008. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Paige, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2 a Revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, I4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, K.; DiNubile, N.A.; Chen, T.J.H.; Waite, R.L.; Schoolfield, J.; Martinez-Pons, M.; Callahan, M.F.; Smith, T.L.; Mengucci, J.; Blum, S.H.; et al. H-Wave, a nonpharmacologic alternative for the treatment of patients with chronic soft tissue inflammation and neuropathic pain: A preliminary statistical outcome study. Adv Ther. 2006, 23, 446–455. [Google Scholar] [CrossRef]
- Blum, K.; Chen, T.J.H.; Ross, B.D. Innate properties of H-Wave device, a small fiber stimulator provides the basis for a paradigm shift of electro-therapeutic treatment of pain with increased functional restoration associated with human neuropathies by affecting tissue circulation: A hypothesis. Med. Hypotheses 2005, 64, 1066–1067. [Google Scholar] [PubMed]
- Blum, K.; Chen, A.L.; Chen, T.J.; Downs, B.W.; Braverman, E.R.; Kerner, M.; Savarimuthu, S.; Bajaj, A.; Madigan, M.; Blum, S.H.; et al. Healing enhancement of chronic venous stasis ulcers utilizing H-WAVE device therapy: A case series. Cases J. 2010, 3, 54. [Google Scholar] [CrossRef] [Green Version]
- Tsang, B.K.; Takaishi, K.; Eichhorn, J.H. Electrical stimulation reduces symptoms of thermal hypersensitivity from injury of sciatic partial ligation in rats. Anesth. Analg. 1998, 86, 324S. [Google Scholar] [CrossRef]
- Blum, K.; Chen, A.L.C.; Chen, T.J.H.; Waite, R.L.; Downs, B.W.; Braverman, E.R.; Kerner, M.M.; Savarimuthu, S.M.; DiNubile, N. Repetitive H-Wave device stimulation and program induces significant increases in the range of motion of post operative rotator cuff reconstruction in a double-blinded randomized placebo controlled human study. BMC Musculoskelet. Disord. 2009, 10, 132. [Google Scholar] [CrossRef] [Green Version]
- Hutchins, P.M.; Marshburn, T.H.; Maultsby, S.J.; Lynch, C.D.; Smith, T.L.; Dusseau, J.W. Long term microvascular response to hydralazine in spontaneously hypertensive rats. Hypertension 1988, 12, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Blum, K.; DiNubile, N.A.; Chen, T.J.H.; Waite, R.L.; Schoolfield, J.; Martinez-Pons, M.; Callahan, M.F.; Smith, T.L.; Mengucci, J.; Blum, S.H.; et al. The H-Wave small muscle fiber stimulator, a nonpharmacologic alternative for the treatment of chronic soft-tissue injury and neuropathic pain: An extended population observational study. Adv Ther. 2006, 23, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Alvaro, M.S.; Julka, I.S.; Marshall, H.J. Diabetic peripheral neuropathy. Effectiveness of electrotherapy and amitriptyline for symptomatic relief. Diabetes Care 1998, 21, 1322–1325. [Google Scholar] [CrossRef]
- Kumar, D.; Marshall, H.J. Diabetic peripheral neuropathy: Amelioration of pain with transcutaneous electrostimulation. Diabetes Care 1997, 20, 1702–1705. [Google Scholar] [CrossRef]
- Flatt, D.W. Resolution of a double Crush syndrome. J. Manip. Physiol. Ther. 1994, 17, 395–397. [Google Scholar]
- Almeida, T.F.; Roizenblatt, S.; Tufik, S. Afferent pain pathways: A neuroanatomical review. Brain Res. 2004, 1000, 40–56. [Google Scholar] [CrossRef]
- Basbaum, A.I.; Bautista, D.M.; Scherrer, G.; Julius, D. Cellular and molecular mechanisms of pain. Cell 2009, 139, 267–284. [Google Scholar] [CrossRef] [Green Version]
- Ding, Y.H.; Luan, X.D.; Li, J.; Rafols, J.A.; Guthinkonda, M.; Diaz, F.G.; Ding, Y. Exercise-induced overexpression of angiogenic factors and reduction of ischemia/reperfusion injury in stroke. Curr. Neurovasc. Res. 2004, 1, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Spanos, K.; Saleptsis, V.; Athanasoulas, A.; Karathanos, C.; Bargiota, A.; Chan, P.; Giannoukas, A.D. Factors Associated with Ulcer Healing and Quality of Life in Patients With Diabetic Foot Ulcer. Angiology 2017, 68, 242–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lépine, J.P.; Briley, M. The epidemiology of pain in depression. Hum. Psychopharmacol. 2004, 19, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Ji, R.R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef]
- Blum, K.; Jacobs, W.; Modestino, E.J.; DiNubile, N.; Baron, D.; McLaughlin, T.; Siwicki, D.; Elman, I.; Moran, M.; Braverman, E.R.; et al. Insurance Companies Fighting the Peer Review Empire without any Validity: The Case for Addiction and Pain Modalities in the face of an American Drug Epidemic. SEJ Surg. Pain 2018, 1, 1–11. [Google Scholar]
- Moran, M.; Blum, K.; Ponce, J.V.; Lott, L.; Gondre-Lewis, M.C.; Badgaiyan, S.; Brewer, R.; Downs, B.W.; Fynman, P.; Weingarten, A.; et al. High Genetic Addiction Risk Score (GARS) in Chronically Prescribed Severe Chronic Opioid Probands Attending Multi-pain Clinics: An Open Clinical Pilot Trial. Mol. Neurobiol. 2021, 58, 3335–3346. [Google Scholar] [CrossRef]

{kind=link}
| Title | Author/Year | Study Type | HWDS Patient Numbers | Summary | Relevance | H-Wave® Outcomes | Clinical Evidence Certainty |
|---|---|---|---|---|---|---|---|
| Coupling Genetic Addiction Risk Score (GARS) with Electrotherapy: Fighting Iatrogenic Opioid Dependence | Blum 2013 [6] | Policy Paper/ Pre-Clinical Study | _ | Strategies to prevent opioid overdose deaths and attenuation of prescription abuse | _ | Identifying patients with specific genes leading to opioid dependence in order to initiate non-pharmacologic H-Wave instead | _ |
| Sciatic Ligation in Rats | Tsang, Tajkaishi 1998 [23] | Pre-Clinical Study | _ | Electrotherapy effect on thermal hypersensitivity in rats after surgical ligation of sciatic nerve | Electrotherapy performed on 10 rats vs. control; withdrawal latency after heat application tested | Electrotherapy rats recovered latency to a greater extent | _ |
| Innate Properties of H-Wave on Pain: A Hypothesis | Blum 2005 [24] | Pre-Clinical Study | _ | Hypothesis behind H-Wave to limit inflammation by stimulating lymphatic smooth muscle | _ | _ | _ |
| Innate Properties of H-Wave on Pain with Increased Functional Restoration: A Hypothesis | Blum 2005 [14] | Pre-clinical Study | _ | Hypothesis behind H-Wave to limit inflammation by stimulating lymphatic smooth muscle | _ | _ | _ |
| H-Wave device induces NO-dependent augmented microcirculation and angiogenesis | Blum 2008 [17] | Pre-Clinical Study | _ | Hypothesis regarding H-Wave effects on NO production and angiogenesis | _ | Deactivates sodium pumps within nerve fibers, leading to long-lasting analgesic effect | _ |
| H-Wave induces arteriolar vasodilation in rat striated muscle | Smith 2009 [15] | Pre-Clinical Study | _ | Measured H-Wave vasodilatory effects on rat arterioles in cremaster muscle | 57 male rats, blocked with L-NAME, received HW at both 1 and 2 Hz | HW resulted increased blood flow between 26 and 62% | _ |
| H-Wave Effects on Blood Flow and Angiogenesis in Longitudinal Studies in Rats | Smith 2011 [25] | Pre-Clinical Study | _ | HW effect on hind limb blood flow | 60 min daily of 2 Hz for 3 weeks | 247% increase in blood flow above resting conditions; biopsy showed increased formation of new blood vessels in biceps femoris | _ |
| Healing enhancement of chronic venous stasis ulcers utilizing H-Wave device therapy: a case series | Blum 2010 [26] | Case Series | 3 | Effect of HW on venous stasis ulcer healing | 3 patients, different duration of ulcers, 30–60 min treatments at ultra-low; p1 twice daily; p2 once weekly; p3 once weekly until 9 months, then once daily | p1: healed after 3 months, p2: healed after 1 month, p3: healed after 9 months | Low |
| Resolution of a Double Crush Syndrome | Flatt 1994 [27] | Case Study | 1 | 63 y/o patient slipped on ice, did the splits, and herniated L4-S1 | 2.25 min of ultra-low; 5 min of high 2x/wk for 6wks | 36 months after reported injury, began treatment schedule; loss of pinprick, deep pressure, pain, and temperature sensation in RLE resolved after four weeks of HW and lumbar flexion/distraction | Low |
| Repetitive H-Wave device stimulation and program induces significant increases in the range of motion of post-operative rotator cuff reconstruction | Blum 2009 [28] | Double-Blind RCT | 11 | Range of motion and strength testing after HW therapy in post-op rotator cuff patients | 22 patients, 11 sham; HW 1 h twice daily for 90 days post-op; evaluated on flexion, ER at side, ER at 90 degrees abduction, IR at side, IR at 90 degrees abduction | Significant improvement in both active ER and IR, no difference in strength testing; HW advanced more quickly through PT | Low |
| H-Wave meta-analysis | Blum 2008 [16] | Meta-Analysis | 6535 | Meta-analysis of H-Wave effect on pain, pain med use, increased functionality | HWDS twice daily for 90 days | Biggest improvement in functionality; moderate to strong effect in all | Moderate |
| H-Wave, a non-pharmacologic alternative to treatment of chronic soft tissue inflammation and neuropathic pain | Blum 2006 [29] | Observational Study | 1291 | Clinical study of H-Wave effect on pain, functionality, pain med usage in chronic inflammation | 1291 patients used H-Wave on either LE, UE, or back for 2 to 6 weeks; previous moderate degree of pain 6–10/10 | More than 60% reported over 25% pain reduction; functional improvement in over 50%; 40% reduced or completely eliminated pain meds | Moderate |
| H-Wave, a non-pharmacologic alternative to treatment of chronic soft tissue inflammation and neuropathic pain: Extended Study | Blum 2006 [30] | Observational Study | 6774 | Clinical study of H-Wave | 6774 patients twice daily for 90 days | 65% decreased need for pain med; 79% increased functionality; 78% symptomatic improvement | Moderate |
| Diabetic Peripheral Neuropathy: Amelioration of Pain with Transcutaneous Electrostimulation | Kumar, Marshall 1998 [31] | RCT | 18 | H-Wave electrotherapy on diabetic neuropathic pain vs. placebo | 25–35 mA above 2 Hz as patient could tolerate | Symptomatic improvement in 15/18 patients; most pain relief was achieved by the third week; no side effects reported; one month f/u after stopping treatment yielded tendency for recurrence of symptoms | Moderate |
| Beneficial Effects of Electrical Stimulation on Neuropathic Symptoms in Diabetes Patients | Julka, Alvaro, Kumar 1998 [18] | RCT | 54 | H-Wave electrotherapy for diabetic neuropathic pain surveyed | Average twice daily for 35 min per treatment for 1.7 years | Over 34 +/− 4% reduction in pain; 2 point reduction on pain scale; 12/19 had reduction in LE swelling | Low |
| Diabetic Peripheral Neuropathy: Effectiveness of Electrotherapy and Amitriptyline for Symptomatic Relief | Kumar, Alvaro, Julka, Marshall 1998 [32] | RCT | 14 | Compared amitriptyline, amitriptyline + sham, amitriptyline + H-Wave on symptomatic relief of diabetic neuropathy | Amitriptyline 50 mg for all, 12 weeks of electrotherapy | 12/14 patients had symptomatic improvement with H-Wave; 5 /14 with complete relief | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williamson, T.K.; Rodriguez, H.C.; Gonzaba, A.; Poddar, N.; Norwood, S.M.; Gupta, A. H-Wave® Device Stimulation: A Critical Review. J. Pers. Med. 2021, 11, 1134. https://doi.org/10.3390/jpm11111134
Williamson TK, Rodriguez HC, Gonzaba A, Poddar N, Norwood SM, Gupta A. H-Wave® Device Stimulation: A Critical Review. Journal of Personalized Medicine. 2021; 11(11):1134. https://doi.org/10.3390/jpm11111134
Chicago/Turabian StyleWilliamson, Tyler K., Hugo C. Rodriguez, Andrew Gonzaba, Neil Poddar, Stephen M. Norwood, and Ashim Gupta. 2021. "H-Wave® Device Stimulation: A Critical Review" Journal of Personalized Medicine 11, no. 11: 1134. https://doi.org/10.3390/jpm11111134
APA StyleWilliamson, T. K., Rodriguez, H. C., Gonzaba, A., Poddar, N., Norwood, S. M., & Gupta, A. (2021). H-Wave® Device Stimulation: A Critical Review. Journal of Personalized Medicine, 11(11), 1134. https://doi.org/10.3390/jpm11111134