
Influence of Catheter–Incision Congruency in Epidural Analgesia on Postcesarean Pain Management: A Single-Blinded Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Preoperative Evaluation
2.2. Epidural Catheterization and Spinal Anesthesia
2.3. Primary Outcome: Pain Intensity Assessment
2.4. Rescue and Adjuvant Analgesics
2.5. Secondary Outcome: Adverse Effects of Epidural Analgesia
2.6. Statistical Analysis
3. Results
3.1. Intraoperative Profiles
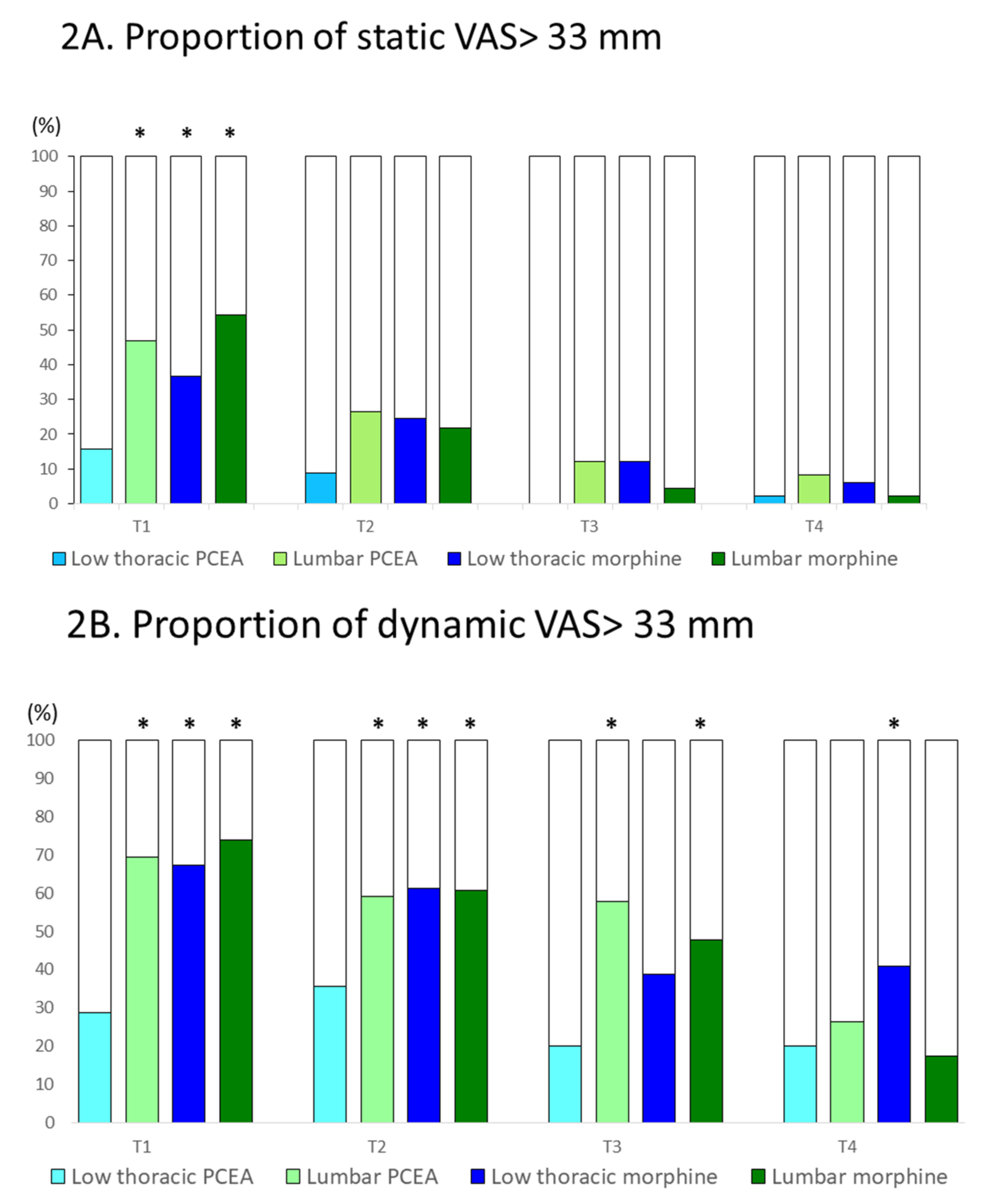
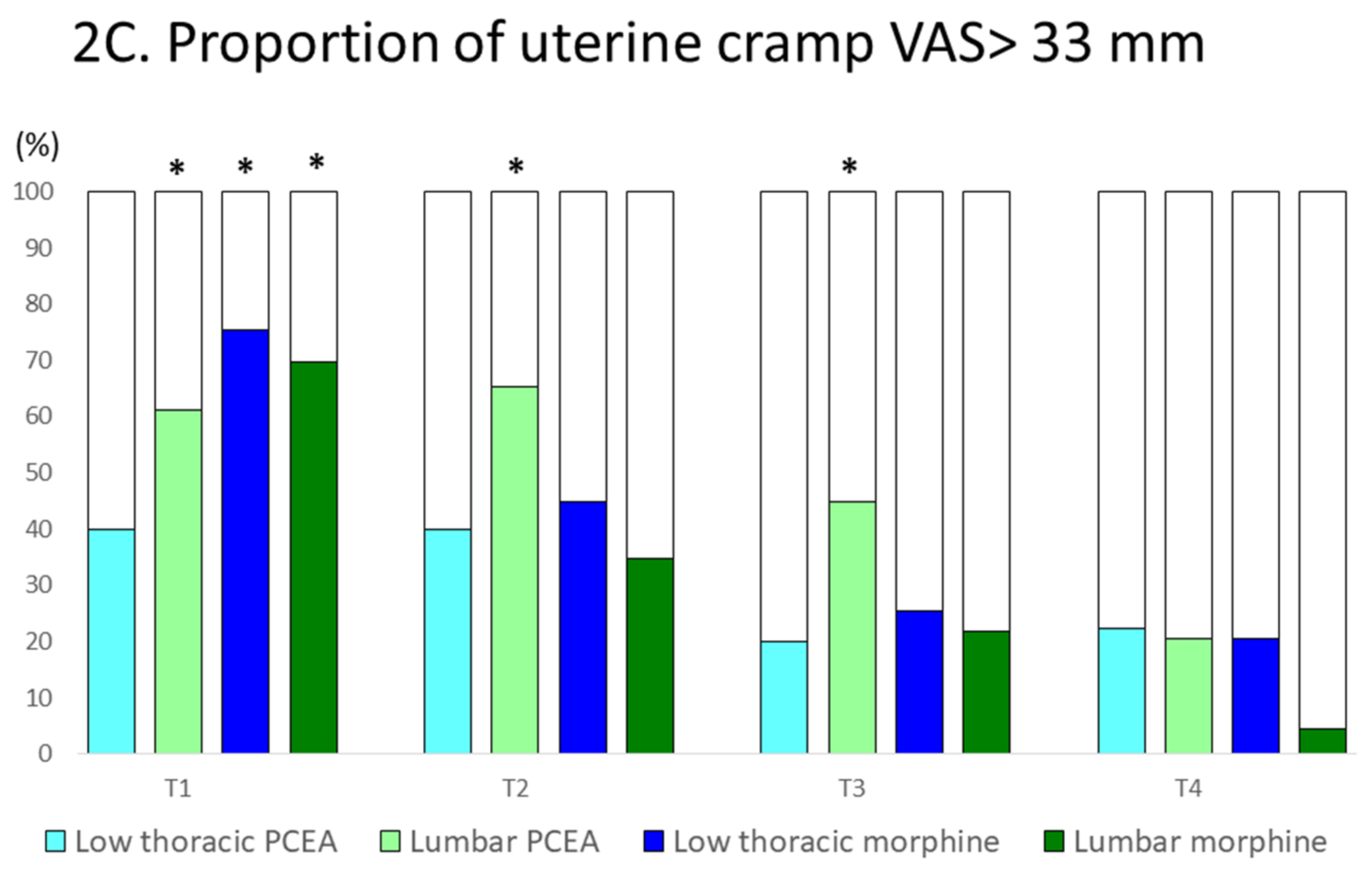
3.2. Postcesarean Pain: Proportion of Participants with a VAS Score of >33 mm
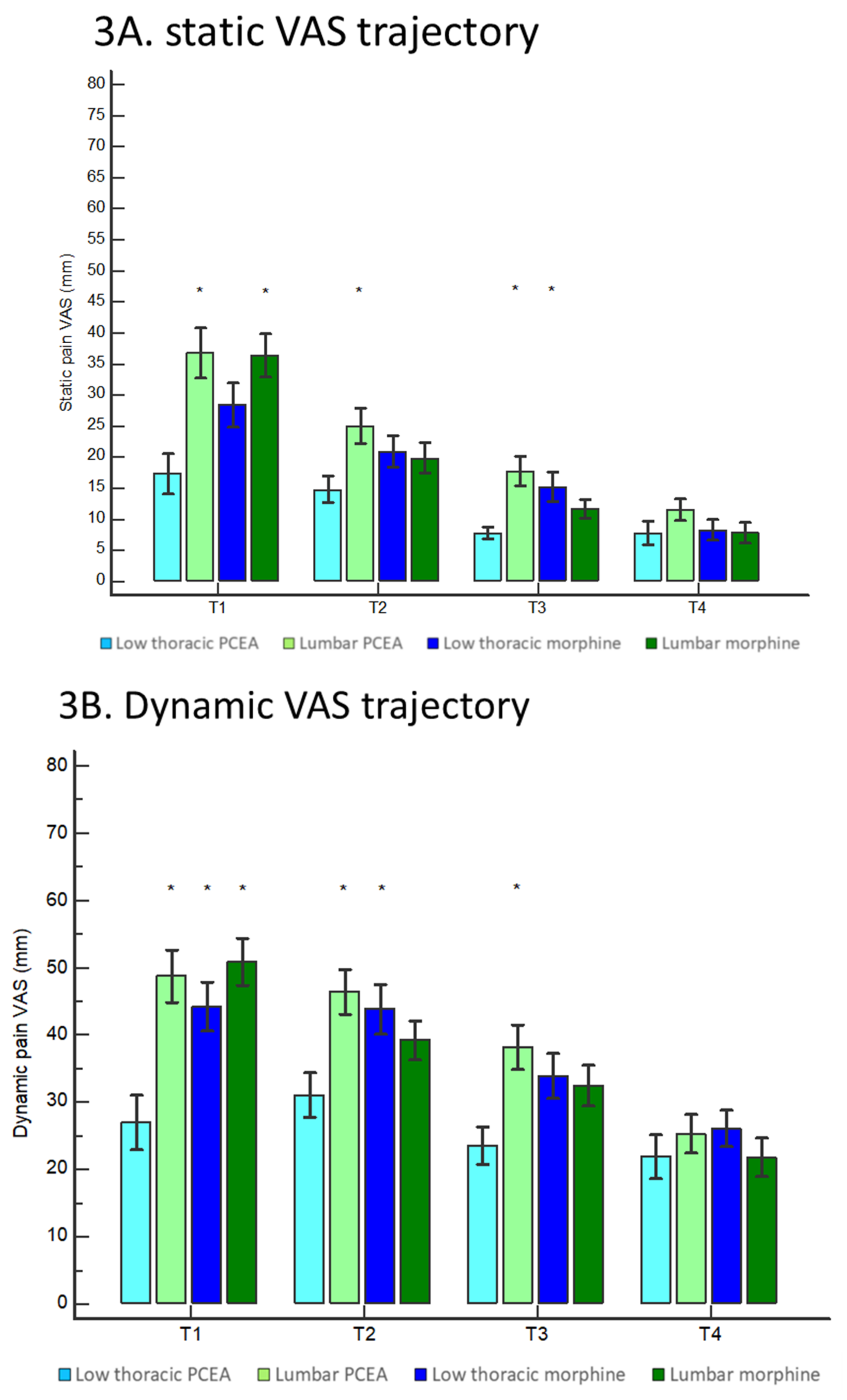
3.3. Postcesarean Pain: Comparison of VAS Scores
3.4. Adverse Effect Profiles
3.5. Analgesic Requirement
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Clinical Trial Registration
Acknowledgments
Conflicts of Interest
References
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.; Peelen, L.M.; Kalkman, C.J.; Meissner, W. Pain intensity on the first day after surgery: A prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef] [Green Version]
- Marcus, H.; Gerbershagen, H.J.; Peelen, L.M.; Aduckathil, S.; Kappen, T.H.; Kalkman, C.J.; Meissner, W.; Stamer, U.M. Quality of pain treatment after caesarean section: Results of a multicentre cohort study. Eur. J. Pain 2015, 19, 929–939. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Martin, R.; Chan, B.; Gofeld, M.; Geary, M.P.; Laffey, J.G.; Abdallah, F.W. Using activity trackers to quantify postpartum ambulation: A prospective observational study of ambulation after regional anesthesia and analgesia interventions. Anesthesiology 2018, 128, 598–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komatsu, R.; Carvalho, B.; Flood, P.D. Recovery after nulliparous birth: A detailed analysis of pain analgesia and recovery of function. Anesthesiology 2017, 127, 684–694. [Google Scholar] [CrossRef]
- Wen, L.; Hilton, G.; Carvalho, B. The impact of breastfeeding on postpartum pain after vaginal and cesarean delivery. J. Clin. Anesth. 2015, 27, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Weibel, S.; Neubert, K.; Jelting, Y.; Meissner, W.; Wockel, A.; Roewer, N.; Kranke, P. Incidence and severity of chronic pain after caesarean section: A systematic review with meta-analysis. Eur. J. Anaesthesiol. 2016, 33, 853–865. [Google Scholar] [CrossRef]
- Block, B.M.; Liu, S.S.; Rowlingson, A.J.; Cowan, A.R.; Cowan, J.A., Jr.; Wu, C.L. Efficacy of postoperative epidural analgesia: A meta-analysis. JAMA 2003, 290, 2455–2463. [Google Scholar] [CrossRef]
- Guasch, E.; Brogly, N.; Gilsanz, F. Combined spinal epidural for labour analgesia and caesarean section: Indications and recommendations. Curr. Opin. Anaesthesiol. 2020, 33, 284–290. [Google Scholar] [CrossRef]
- Simmons, S.W.; Dennis, A.T.; Cyna, A.M.; Richardson, M.G.; Bright, M.R. Combined spinal-epidural versus spinal anaesthesia for caesarean section. Cochrane Database Syst. Rev. 2019, 10, CD004908. [Google Scholar] [CrossRef]
- Kehlet, H.; Holte, K. Effect of postoperative analgesia on surgical outcome. Br. J. Anaesth. 2001, 87, 62–72. [Google Scholar] [CrossRef] [Green Version]
- Gizzo, S.; Noventa, M.; Fagherazzi, S.; Lamparelli, L.; Ancona, E.; Di Gangi, S.; Saccardi, C.; D'Antona, D.; Nardelli, G.B. Update on best available options in obstetrics anaesthesia: Perinatal outcomes, side effects and maternal satisfaction. Fifteen years systematic literature review. Arch Gynecol. Obs. 2014, 290, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.L. Epidural analgesia for labor and delivery. N. Engl. J. Med. 2010, 362, 1503–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rollins, M.; Lucero, J. Overview of anesthetic considerations for Cesarean delivery. Br. Med. Bull. 2012, 101, 105–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kara, H.; Sahin, N.; Ulusan, V.; Aydogdu, T. Magnesium infusion reduces perioperative pain. Eur. J. Anaesthesiol. 2002, 19, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Pan, P.H.; Tonidandel, A.M.; Aschenbrenner, C.A.; Houle, T.T.; Harris, L.C.; Eisenach, J.C. Predicting acute pain after cesarean delivery using three simple questions. Anesthesiology 2013, 118, 1170–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backe, S.K.; Sheikh, Z.; Wilson, R.; Lyons, G.R. Combined epidural/spinal anaesthesia: Needle-through-needle or separate spaces? Eur. J. Anaesthesiol. 2004, 21, 854–857. [Google Scholar] [CrossRef]
- Lee, A.J.; Ranasinghe, J.S.; Chehade, J.M.; Arheart, K.; Saltzman, B.S.; Penning, D.H.; Birnbach, D.J. Ultrasound assessment of the vertebral level of the intercristal line in pregnancy. Anesth. Analg. 2011, 113, 559–564. [Google Scholar] [CrossRef]
- Ousley, R.; Egan, C.; Dowling, K.; Cyna, A.M. Assessment of block height for satisfactory spinal anaesthesia for caesarean section. Anaesthesia 2012, 67, 1356–1363. [Google Scholar] [CrossRef]
- Onishi, E.; Murakami, M.; Hashimoto, K.; Kaneko, M. Optimal intrathecal hyperbaric bupivacaine dose with opioids for cesarean delivery: A prospective double-blinded randomized trial. Int. J. Obs. Anesth. 2017, 31, 68–73. [Google Scholar] [CrossRef]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Hals, E.K.; Kvarstein, G.; Stubhaug, A. Assessment of pain. Br. J. Anaesth. 2008, 101, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S.; European Palliative Care Research, C. Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: A systematic literature review. J. Pain Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Myles, D.B.; Galagher, W.; Boyd, D.; Chew, C.; MacDonald, N.; Dennis, A. Measuring acute postoperative pain using the visual analog scale: The minimal clinically important difference and patient acceptable symptom state. Br. J. Anaesth. 2017, 118, 424–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufner, L.; Heimann, S.; Zander, D.; Weizsacker, K.; Correns, I.; Sander, M.; Spies, C.; Schuster, M.; Feldheiser, A.; Henkelmann, A.; et al. Neuraxial anesthesia for pain control after cesarean section: A prospective randomized trial comparing three different neuraxial techniques in clinical practice. Minerva Anestesiol. 2016, 82, 514–524. [Google Scholar] [PubMed]
- Chestnut, D.H.; Wong, C.A.; Tsen, L.C.; Kee, W.D.N.; Beilin, Y.; Mhyre, J.; Bateman, B.T.; Msc, M.; Nathan, N. Chestnut's Obstetric Anesthesia: Principles and Practice 6th Edition Práctica; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Hoyle, J.; Yentis, S.M. Assessing the height of block for caesarean section over the past three decades: Trends from the literature. Anaesth. 2015, 70, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, K.; Singh, S.I. Neuraxial opioid-induced pruritus: An update. J. Anaesthesiol. Clin. Pharm. 2013, 29, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Heidrich, F.M.; Jukar-Rao, S.; Jalota, L.; Hornuss, C.; Whelan, R.P.; Zhang, K.; Cakmakkaya, O.S. Evidence-based analysis of risk factors for postoperative nausea and vomiting. Br. J. Anaesth. 2012, 109, 742–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nie, Y.; Liu, Y.; Luo, Q.; Huang, S. Effect of dexmedetomidine combined with sufentanil for post-caesarean section intravenous analgesia: A randomised, placebo-controlled study. Eur. J. Anaesthesiol. 2014, 31, 197–203. [Google Scholar] [CrossRef]
- Ciechanowicz, S.; Setty, T.; Robson, E.; Sathasivam, C.; Chazapis, M.; Dick, J.; Carvalho, B.; Sultan, P. Development and evaluation of an obstetric quality-of-recovery score (ObsQoR-11) after elective Caesarean delivery. Br. J. Anaesth. 2019, 122, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Stark, P.A.; Myles, P.S.; Burke, J.A. Development and psychometric evaluation of a postoperative quality of recovery score: The QoR-15. Anesthesiology 2013, 118, 1332–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borges, N.C.; Pereira, L.V.; de Moura, L.A.; Silva, T.C.; Pedroso, C.F. Predictors for moderate to severe acute postoperative pain after cesarean section. Pain Res. Manag. 2016, 2016, 5783817. [Google Scholar] [CrossRef] [Green Version]
- Chooi, C.S.; White, A.M.; Tan, S.G.; Dowling, K.; Cyna, A.M. Pain vs comfort scores after caesarean section: A randomized trial. Br. J. Anaesth. 2013, 110, 780–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dafna, L.; Herman, H.G.; Ben-Zvi, M.; Bustan, M.; Sasson, L.; Bar, J.; Kovo, M. Comparison of 3 protocols for analgesia control after cesarean delivery: A randomized controlled trial. Am. J. Obs. Gynecol. MFM 2019, 1, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Matsota, P.; Batistaki, C.; Apostolaki, S.; Kostopanagiotou, G. Patient-controlled epidural analgesia after Caesarean section: Levobupivacaine 0.15% versus ropivacaine 0.15% alone or combined with fentany l 2 microg/mL: A comparative study. Arch Med. Sci. 2011, 7, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Maged, A.M.; Deeb, W.S.; Elbaradie, S.; Elzayat, A.R.; Metwally, A.A.; Hamed, M.; Shaker, A. Comparison of local and intra venous dexamethasone on post operative pain and recovery after caeseream section. A randomized controlled trial. Taiwan J Obs. Gynecol. 2018, 57, 346–350. [Google Scholar] [CrossRef]
- Sun, S.; Guo, Y.; Wang, T.; Huang, S. Analgesic effect comparison between nalbuphine and sufentanil for patient-controlled intravenous analgesia after cesarean section. Front. Pharm. 2020, 11, 574493. [Google Scholar] [CrossRef]
- Carvalho, B.; Cohen, S.E.; Lipman, S.S.; Fuller, A.; Mathusamy, A.D.; Macario, A. Patient preferences for anesthesia outcomes associated with cesarean delivery. Anesth. Analg. 2005, 101, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Lu, J.; Shu, C.; Chen, Y.; Guo, T.; Wu, Q.P.; Yao, S.L.; Yin, P. A comparision of nalbuphine with morphine for analgesic effects and safety: Meta-analysis of randomized controlled trials. Sci. Rep. 2015, 5, 10927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jannuzzi, R.G. Nalbuphine for treatment of opioid-induced pruritus: A systematic review of literature. Clin. J. Pain 2016, 32, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Tsai, S.K.; Huang, C.H.; Wang, M.H.; Lin, P.L.; Chen, L.K.; Lin, C.J.; Sun, W.Z. Intravenous tenoxicam reduces uterine cramps after cesarean delivery. Can. J. Anaesth. 2002, 49, 384–387. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.W.; McPhee, R.W.; Stringer, M.D. An evidence-based approach to human dermatomes. Clin. Anat. 2008, 21, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Chestnut, D.H.; Wong, C.A.; Tsen, L.C.; Kee, W.D.N.; Beilin, Y.; Mhyre, J.; Nathan, N.; Bateman, B.T. Chestnut's Obstetric Anesthesia: Principles and Practice; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Sultan, P.; Halpern, S.H.; Pushpanathan, E.; Patel, S.; Carvalho, B. The effect of intrathecal morphine dose on outcomes after elective cesarean delivery: A meta-analysis. Anesth. Analg. 2016, 123, 154–164. [Google Scholar] [CrossRef]
- Konstantatos, A.H.; Imberger, G.; Angliss, M.; Cheng, C.H.; Meng, A.Z.; Chan, M.T. A prospective cohort study comparing early opioid requirement between Chinese from Hong Kong and Caucasian Australians after major abdominal surgery. Br. J. Anaesth. 2012, 109, 797–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duale, C.; Frey, C.; Bolandard, F.; Barriere, A.; Schoeffler, P. Epidural versus intrathecal morphine for postoperative analgesia after caesarean section. Br. J. Anaesth. 2003, 91, 690–694. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.; Jha, S.; Sia, A.T.; Rawal, N. Morphine for post-caesarean section analgesia: Intrathecal, epidural or intravenous? Singap. Med. J. 2005, 46, 392–396. [Google Scholar]
- Sarvela, J.; Halonen, P.; Soikkeli, A.; Korttila, K. A double-blinded, randomized comparison of intrathecal and epidural morphine for elective cesarean delivery. Anesth. Analg. 2002, 95, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Bujedo, B.M. Spinal opioid bioavailability in postoperative pain. Pain Pr. 2014, 14, 350–364. [Google Scholar] [CrossRef]
- Angst, M.S.; Ramaswamy, B.; Riley, E.T.; Stanski, D.R. Lumbar epidural morphine in humans and supraspinal analgesia to experimental heat pain. Anesthesiology 2000, 92, 312–324. [Google Scholar] [CrossRef]
- Sutton, C.D.; Carvalho, B. Optimal pain management after cesarean delivery. Anesth. Clin. 2017, 35, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Murata, Y.; Yamada, K.; Hamaguchi, Y.; Yamashita, S.; Tanaka, M. An optimal epidural catheter placement site for post-cesarean section analgesia with double-space technique combined spinal-epidural anesthesia: A retrospective study. JA Clin. Rep. 2021, 7, 3. [Google Scholar] [CrossRef]
- Guay, J.; Nishimori, M.; Kopp, S.L. Epidural local anesthetics versus opioid-based analgesic regimens for postoperative gastrointestinal paralysis, vomiting, and pain after abdominal surgery: A cochrane review. Anesth. Analg. 2016, 123, 1591–1602. [Google Scholar] [CrossRef]
- Tan, S.H.; Teo, E.C.; Chua, H.C. Quantitative three-dimensional anatomy of cervical, thoracic and lumbar vertebrae of Chinese Singaporeans. Eur. Spine J. 2004, 13, 137–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, K.J.; Karmakar, M.K.; Peng, P. Ultrasonography of the adult thoracic and lumbar spine for central neuraxial blockade. Anesthesiology 2011, 114, 1459–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLeod, G.; Cumming, C. Thoracic epidural anaesthesia and analgesia. Contin. Educ. Anaesth. Crit. Care Pain 2004, 4, 16–19. [Google Scholar] [CrossRef] [Green Version]
- Mowat, I.; Tang, R.; Vaghadia, H.; Krebs, C.; Henderson, W.R.; Sawka, A. Epidural distribution of dye administered via an epidural catheter in a porcine model. Br. J. Anaesth. 2016, 116, 277–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Thoracic PCEA | Lumbar PCEA | Low Thoracic Morphine | Lumbar Morphine | p Value | |
|---|---|---|---|---|---|
| (n = 45) | (n = 49) | (n = 49) | (n = 46) | ||
| Age (yr) | 36.1 ± 4.5 | 35.0 ± 4.5 | 36.4 ± 4.2 | 36.7 ± 4.2 | p = 0.225 |
| Height (cm) | 159.3 ± 6.1 | 159.1 ± 5.1 | 161.3 ± 5.5 | 159.5 ± 5.6 | p = 0.204 |
| Weight (kg) | 69.5 ± 11.1 | 67.6 ± 10.3 | 71.9 ± 11.0 | 69.8 ± 10.4 | p = 0.285 |
| Nulliparous (n; %) | 27 (60.0%) | 27 (55.1%) | 32 (65.3%) | 27 (58.7%) | p = 0.779 |
| Indication (n; %) | p = 0.585 | ||||
| Previous uterine surgery | 14 (31.1%) | 22 (44.9%) | 19 (38.8%) | 17 (37.0%) | |
| Twin | 14 (31.1%) | 6 (12.2%) | 6 (12.2%) | 5 (10.9%) | |
| Breech | 5 (11.1%) | 8 (16.3%) | 11 (22.5%) | 9 (19.6%) | |
| Fetal abnormality | 4 (8.9%) | 4 (8.2%) | 3 (6.1%) | 3 (6.5%) | |
| Maternal request | 3 (6.7%) | 4 (8.2%) | 3 (6.1%) | 3 (6.5%) | |
| Other | 5 (11.1%) | 5 (10.2%) | 7 (14.3%) | 9 (19.5%) | |
| Preoperative questionnaire | p = 0.342 | ||||
| Preoperative anxiety (0–100) | 54 ± 27 | 62 ± 24 | 55 ± 25 | 56 ± 26 | |
| Anticipated pain (0–100) | 70 ± 20 | 76 ± 17 | 66 ± 19 | 68 ± 22 | p = 0.081 |
| Anticipated medication (0–5) | 4 (3–4) | 4 (3–4) | 3 (3–4) | 4 (3–4) | p = 0.208 |
| Low Thoracic PCEA | Lumbar PCEA | Low Thoracic Morphine | Lumbar Morphine | p Value | |
|---|---|---|---|---|---|
| (n = 45) | (n = 49) | (n = 49) | (n = 46) | ||
| Surgical profile | |||||
| Operation time (min) | 50.0 ± 14.4 | 50.7 ± 12.2 | 49.4 ± 14.2 | 50.0 ± 12.2 | p = 0.977 |
| Blood loss (mL) | 422 ± 173 | 437 ± 170 | 431 ± 119 | 414 ± 89 | p= 0.878 |
| Epidural profile | |||||
| Skin-epidural depth (cm) | 4.8 ± 0.6 | 4.8 ± 0.7 | 4.8 ± 0.8 | 4.9 ± 0.8 | p = 0.755 |
| Procedure time (sec) | 313 ± 309 | 299 ± 255 | 272 ± 203 | 309 ± 341 | p = 0.891 |
| Redirection (n) | 1.4 ± 1.3 | 2.0 ± 3.7 | 1.6 ± 1.6 | 1.9 ± 1.8 | p = 0.488 |
| Anesthesia profile | |||||
| SA level (n; %) | p = 0.054 | ||||
| T6 or above | 45 (100%) | 46 (93.9%) | 49 (100%) | 42 (91.3%) | |
| Below T6 | 0 (0%) | 3 (6.1%) | 0 (0%) | 4 (8.7%) | p = 0.676 |
| Intravenous fluid (mL) | 1009 ± 345 | 1029 ± 281 | 966 ± 295 | 963 ± 338 | |
| Norepinephrine (mcg) | 25 ± 21 | 25 ± 21 | 24 ± 25 | 28 ± 33 | p = 0.895 |
| Low Thoracic PCEA | Lumbar PCEA | Low Thoracic Morphine | Lumbar Morphine | p Value | |
|---|---|---|---|---|---|
| (n = 45) | (n = 49) | (n = 49) | (n = 46) | ||
| Worst Bromage score (n; %) | p = 0.005 | ||||
| 0 | 41 (91.1%) # | 34 (69.4%) * | 43 (87.7%) # | 42 (91.3%) # | |
| 1 | 4 (8.9%) | 9 (18.4%) | 4 (8.2%) | 3 (6.5%) | |
| 2 | 0 (0%) | 5 (10.2%) | 2 (4.1%) | 1 (2.2%) | |
| 3 | 0 (0%) | 1 (2.0%) | 0 (0%) | 0 (0%) | |
| Pruritus (n; %) | p = 0.099 | ||||
| Mild or none | 32 (71.1%) | 40 (81.6%) | 36 (73.5%) | 33 (71.7%) | |
| Moderate | 12 (26.7%) | 9 (18.4%) | 13 (26.5%) | 9 (19.6%) | |
| Severe | 1 (2.2%) | 0 (0%) | 0 (0%) | 4 (8.7%) | |
| PONV (n; %) | p = 0.221 | ||||
| None | 40 (88.9%) | 40 (81.6%) | 37 (75.5%) | 38 (82.6%) | |
| Nausea | 2 (4.4%) | 8 (16.3%) | 4 (8.2%) | 4 (8.7%) | |
| Retch | 0 (0%) | 0 (0%) | 1 (2.0%) | 0 (0%) | |
| Vomiting | 3 (6.7%) | 1 (2.1%) | 7 (14.3%) | 4 (8.7%) | |
| Ramsay Sedation Scale ≠ 2 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | p = 0966 |
| First passage of flatulence (hr) | 17.3 ± 7.5 | 20.8 ± 8.4 | 26.2 ± 7.9 *# | 25.1 ± 7.6 *# | p < 0.001 |
| Recovery numeric rating scale (0–100) | 76.2 ± 10.1 # | 70.8 ± 7.4 * | 76.9 ± 8.7 # | 78.3 ± 8.6 # | p < 0.001 |
| Low Thoracic PCEA | Lumbar PCEA | Low Thoracic Morphine | Lumbar Morphine | p Value | |
|---|---|---|---|---|---|
| (n = 45) | (n = 49) | (n = 49) | (n = 46) | ||
| PCEA profile | 206 (193–228) | 275 (228–308) | NA | NA | p< 0.001 |
| Total dose (mL) | |||||
| Demand number | 9 (4–25) | 21 (9–37) | p = 0.007 | ||
| Delivery number | 7 (2–18) | 11 (7–25) | p = 0.002 | ||
| Demand/delivery ratio | 1.8 ± 1.2 | 1.6 ± 0.9 | p = 0.371 | ||
| Total epidural morphine dose (mg) | NA | NA | 10 (10–11.3) | 11 (10–11) | p = 0.686 |
| Number of rescue intervention (n) | 1.0 ± 1.1 # | 2.5 ± 1.5 * | 1.6 ± 1.8 # | 1.7 ± 1.7 * | p < 0.001 |
| Supplement epidural morphine dose (mg) | 0.1 ± 0.4 | 0.7 ± 0.9 * | 0.9 ± 1.1 * | 0.8 ± 1.0 * | p < 0.001 |
| IV analgesic dose | |||||
| Nabuphine (mg) | 1.1 ± 3.2 | 2.5 ± 5.2 | 3.0 ± 6.7 | 2.6 ± 7.1 | p = 0.442 |
| Tenoxicam (mg) | 18.7 ± 20.2 | 23.7 ± 21.5 | 16.3 ± 19.9 | 21.7 ± 20.1 | p = 0.301 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-H.; Chou, W.-H.; Yie, J.-C.; Teng, H.-C.; Wu, Y.-L.; Wu, C.-Y. Influence of Catheter–Incision Congruency in Epidural Analgesia on Postcesarean Pain Management: A Single-Blinded Randomized Controlled Trial. J. Pers. Med. 2021, 11, 1099. https://doi.org/10.3390/jpm11111099
Chen Y-H, Chou W-H, Yie J-C, Teng H-C, Wu Y-L, Wu C-Y. Influence of Catheter–Incision Congruency in Epidural Analgesia on Postcesarean Pain Management: A Single-Blinded Randomized Controlled Trial. Journal of Personalized Medicine. 2021; 11(11):1099. https://doi.org/10.3390/jpm11111099
Chicago/Turabian StyleChen, Ying-Hsi, Wei-Han Chou, Jr-Chi Yie, Hsiao-Chun Teng, Yi-Luen Wu, and Chun-Yu Wu. 2021. "Influence of Catheter–Incision Congruency in Epidural Analgesia on Postcesarean Pain Management: A Single-Blinded Randomized Controlled Trial" Journal of Personalized Medicine 11, no. 11: 1099. https://doi.org/10.3390/jpm11111099
APA StyleChen, Y.-H., Chou, W.-H., Yie, J.-C., Teng, H.-C., Wu, Y.-L., & Wu, C.-Y. (2021). Influence of Catheter–Incision Congruency in Epidural Analgesia on Postcesarean Pain Management: A Single-Blinded Randomized Controlled Trial. Journal of Personalized Medicine, 11(11), 1099. https://doi.org/10.3390/jpm11111099