
Personalized Reconstruction of Genital Defects in Complicated Wounds with Vertical Rectus Abdominis Myocutaneous Flaps including Urethral Neo-Orifice





Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Patients and Methods
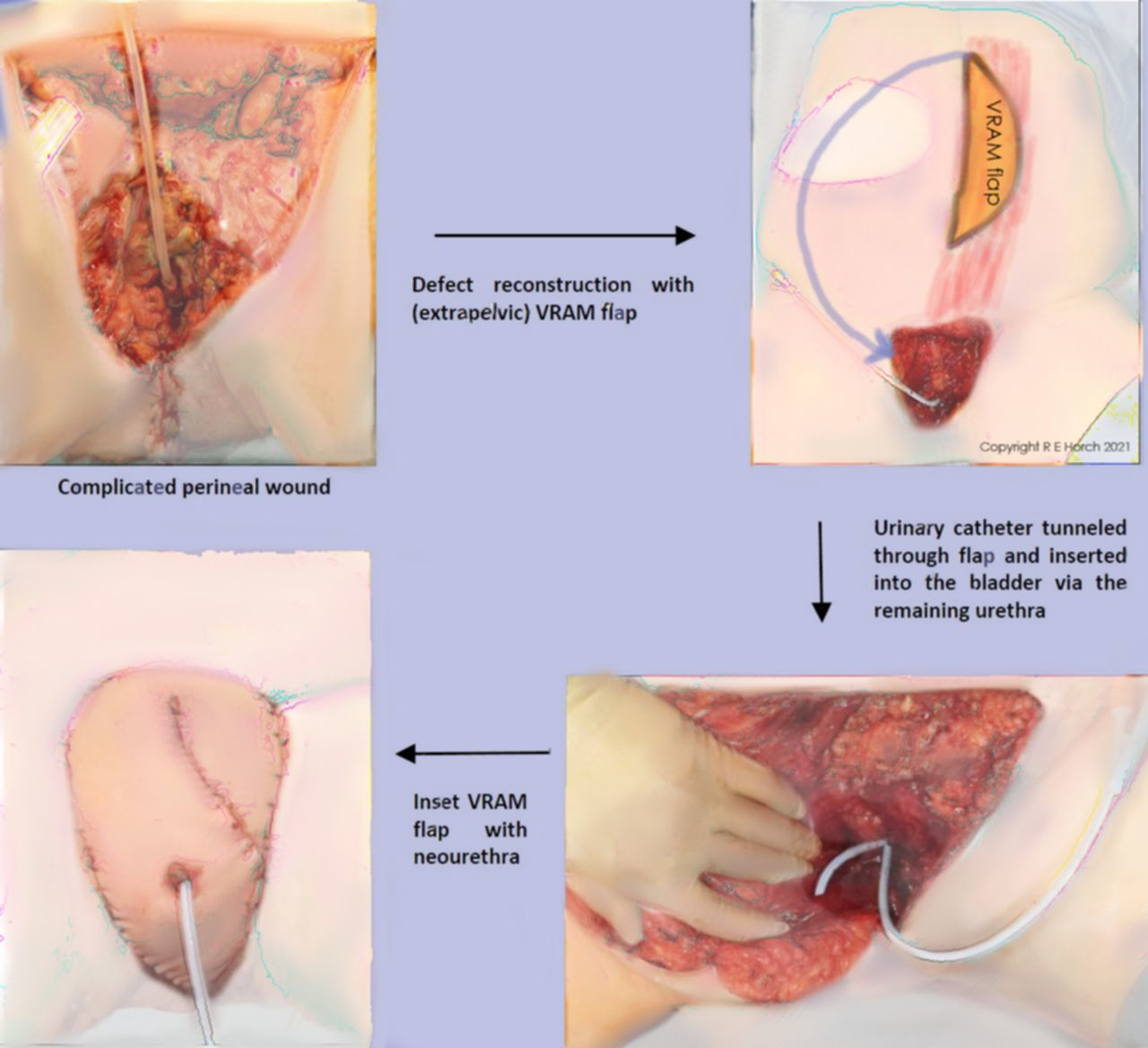
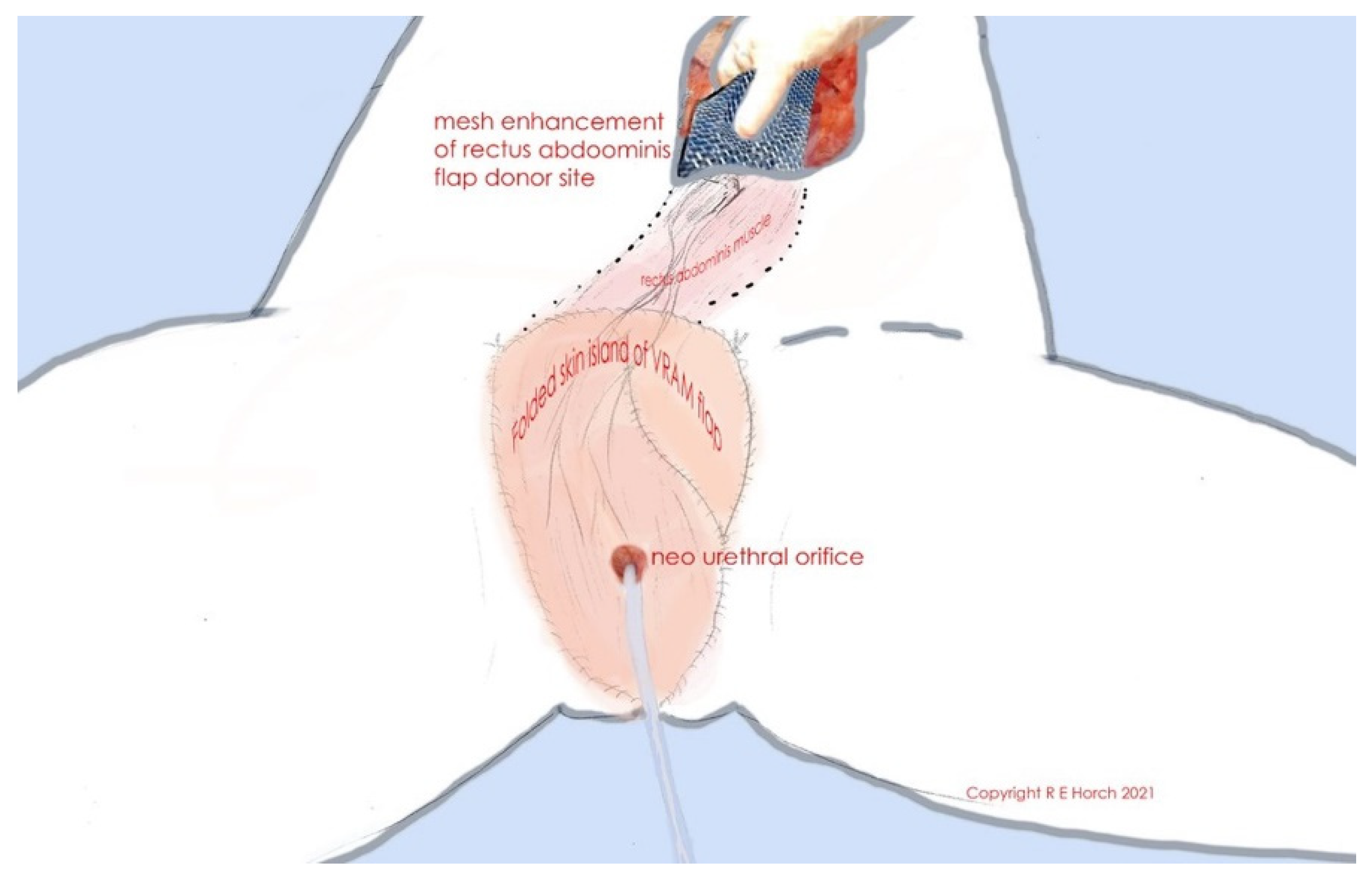
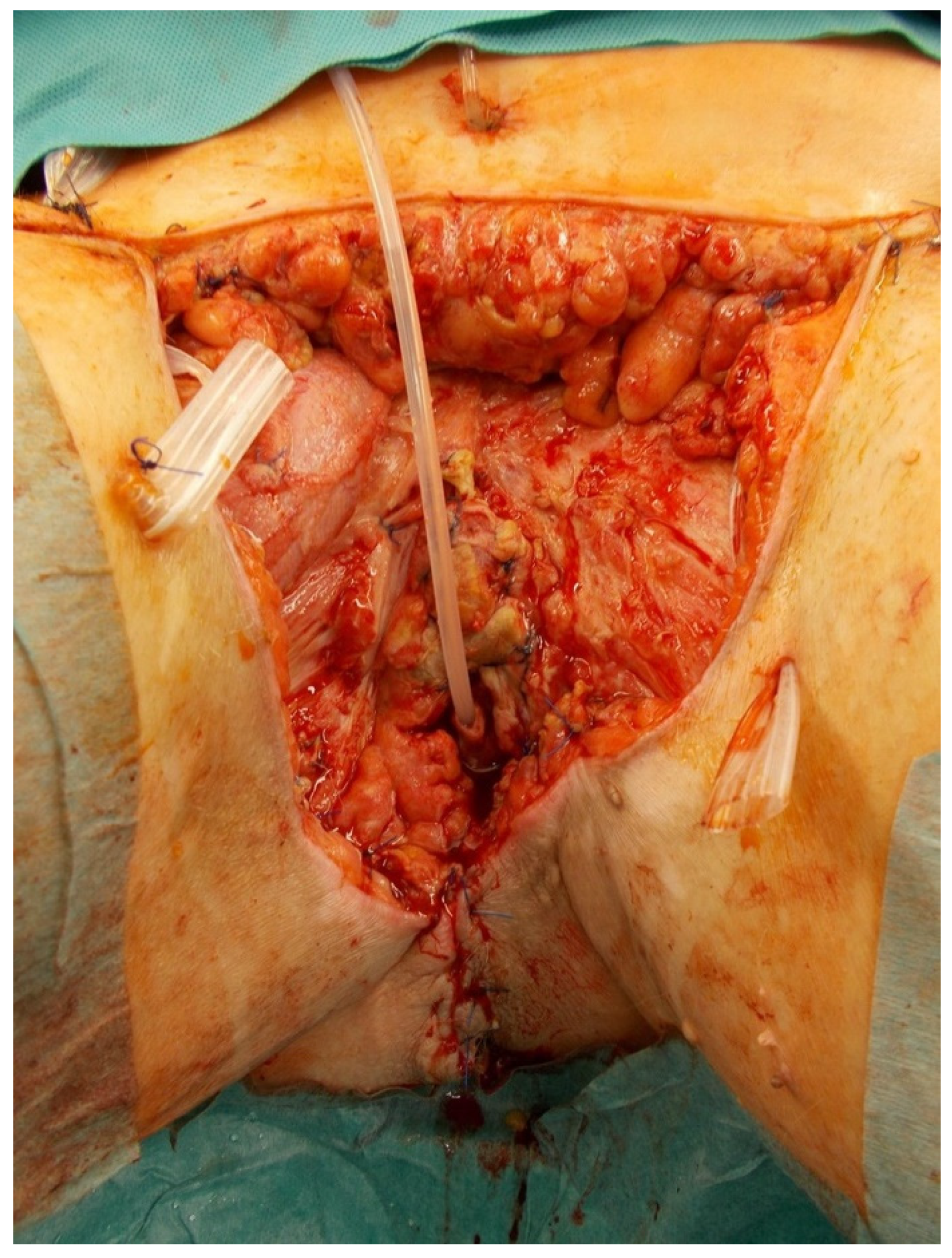
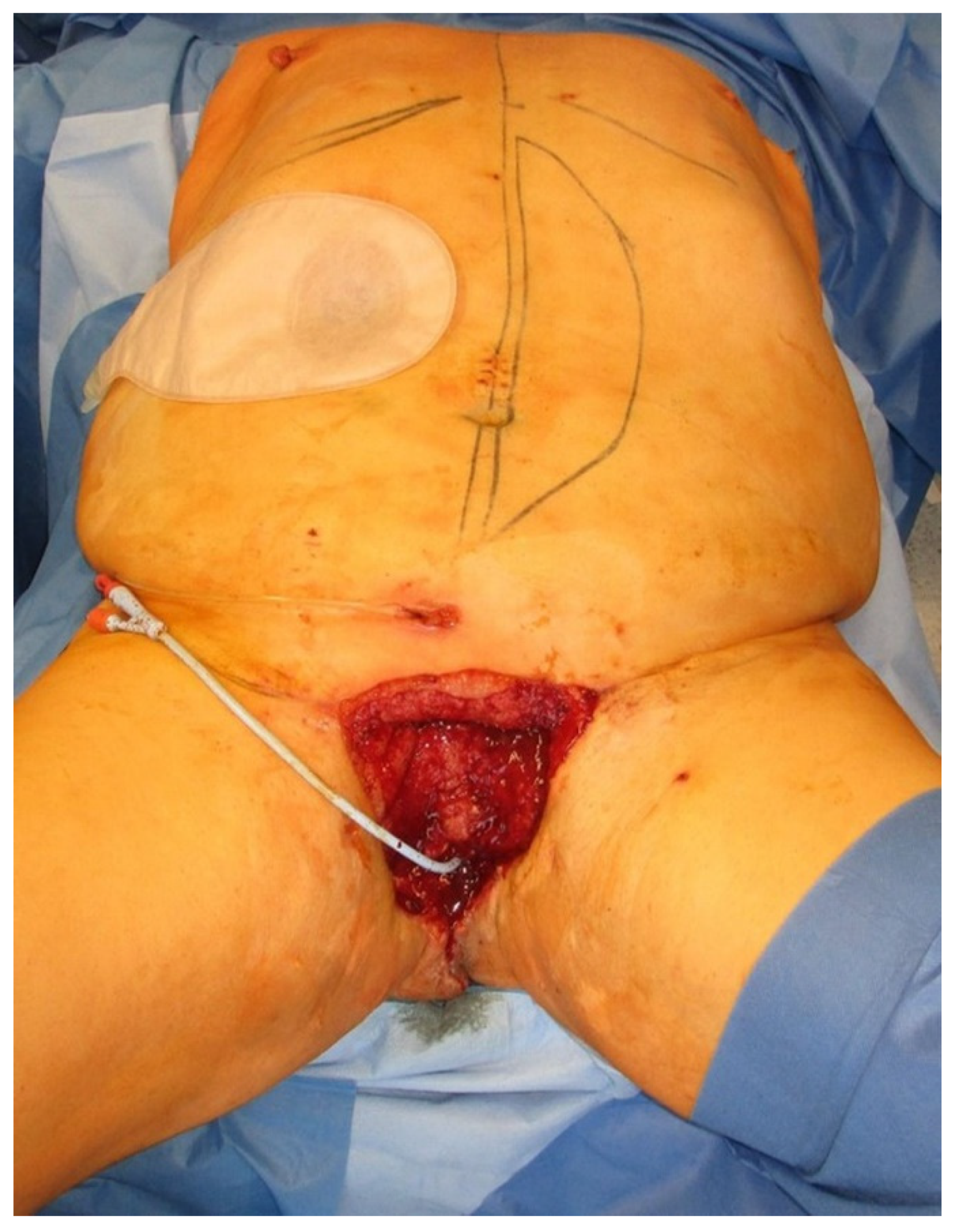
2.1. Technique of Surgery
2.2. Case 1
2.3. Case 2
2.4. Case 3
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karian, L.S.; Chung, S.Y.; Lee, E.S. Reconstruction of Defects After Fournier Gangrene: A Systematic Review. Eplasty 2015, 15, e18. [Google Scholar]
- Wong, A.A.; Delclos, M.E.; Wolff, R.A.; Evans, D.B.; Abbruzzese, J.L.; Tamm, E.P.; Xiong, H.Q.; Ho, L.; Crane, C.H. Radiation dose considerations in the palliative treatment of locally advanced adenocarcinoma of the pancreas. Am. J. Clin. Oncol. 2005, 28, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.S.; Cummings, B.J.; Brierley, J.D.; Catton, C.N.; McLean, M.; Catton, P.; Hao, Y. Treatment of locally recurrent rectal carcinoma—Results and prognostic factors. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 427–435. [Google Scholar] [CrossRef]
- Sugiyama, T.; Yakushiji, M.; Noda, K.; Ikeda, M.; Kudoh, R.; Yajima, A.; Tomoda, Y.; Terashima, Y.; Takeuchi, S.; Hiura, M.; et al. Phase II study of irinotecan and cisplatin as first-line chemotherapy in advanced or recurrent cervical cancer. Oncology 2000, 58, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Gerard, J.P.; Romestaing, P.; Chapet, O. Radiotherapy alone in the curative treatment of rectal carcinoma. Lancet Oncol. 2003, 4, 158–166. [Google Scholar] [CrossRef]
- Brodbeck, R.; Horch, R.E.; Arkudas, A.; Beier, J.P. Plastic and Reconstructive Surgery in the Treatment of Oncological Perineal and Genital Defects. Front. Oncol. 2015, 5, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beier, J.P.; Croner, R.S.; Lang, W.; Arkudas, A.; Schmitz, M.; Gohl, J.; Hohenberger, W.; Horch, R.E. Avoidance of complications in oncological surgery of the pelvic region: Combined oncosurgical and plastic reconstruction measures. Chirurg 2015, 86, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Bregendahl, S.; Emmertsen, K.J.; Lindegaard, J.C.; Laurberg, S. Urinary and sexual dysfunction in women after resection with and without preoperative radiotherapy for rectal cancer: A population-based cross-sectional study. Colorectal. Dis. 2015, 17, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Jakowatz, J.G.; Porudominsky, D.; Riihimaki, D.U.; Kemeny, M.; Kokal, W.A.; Braly, P.S.; Terz, J.J.; Beatty, J.D. Complications of pelvic exenteration. Arch. Surg. 1985, 120, 1261–1265. [Google Scholar] [CrossRef] [PubMed]
- Horch, R.E.; Hohenberger, W.; Eweida, A.; Kneser, U.; Weber, K.; Arkudas, A.; Merkel, S.; Gohl, J.; Beier, J.P. A hundred patients with vertical rectus abdominis myocutaneous (VRAM) flap for pelvic reconstruction after total pelvic exenteration. Int. J. Colorectal. Dis. 2014, 29, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Krautz, C.; Weber, K.; Croner, R.; Denz, A.; Maak, M.; Horch, R.E.; Grutzmann, R. Cylindric Abdominoperineal Rectum Exstirpation with Partial Vulvar and Vaginal Resection as well as Perineal and Vaginal Defect Reconstruction by a Vertical Rectus Abdominis Myocutaneous (VRAM) Flap. Zentralbl. Chir. 2017, 142, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Horch, R.E.; Ludolph, I.; Cai, A.; Weber, K.; Grutzmann, R.; Arkudas, A. Interdisciplinary Surgical Approaches in Vaginal and Perineal Reconstruction of Advanced Rectal and Anal Female Cancer Patients. Front. Oncol. 2020, 10, 719. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.L.; Westin, S.N.; Fellman, B.; Rallapali, V.; Frumovitz, M.; Ramirez, P.T.; Sood, A.K.; Soliman, P.T. Modified vertical rectus abdominis myocutaneous flap vaginal reconstruction: An analysis of surgical outcomes. Gynecol. Oncol. 2012, 125, 252–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connell, C.; Mirhashemi, R.; Kassira, N.; Lambrou, N.; McDonald, W.S. Formation of functional neovagina with vertical rectus abdominis musculocutaneous (VRAM) flap after total pelvic exenteration. Ann. Plast. Surg. 2005, 55, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Nigriny, J.F.; Wu, P.; Butler, C.E. Perineal reconstruction with an extrapelvic vertical rectus abdominis myocutaneous flap. Int. J. Gynecol. Cancer 2010, 20, 1609–1612. [Google Scholar] [CrossRef]
- Insua-Pereira, I.; Ferreira, P.C.; Teixeira, S.; Barreiro, D.; Silva, A. Fournier’s gangrene: A review of reconstructive options. Cent. Eur. J. Urol 2020, 73, 74–79. [Google Scholar] [CrossRef]
- Tan, B.K.; Tan, K.C.; Khoo, A.K. Total scrotal reconstruction after Fournier’s gangrene—A case report using rectus abdominis myocutaneous flap. Ann. Acad. Med. Singap. 1996, 25, 890–892. [Google Scholar] [PubMed]
- Mirhashemi, R.; Averette, H.E.; Lambrou, N.; Penalver, M.A.; Mendez, L.; Ghurani, G.; Salom, E. Vaginal reconstruction at the time of pelvic exenteration: A surgical and psychosexual analysis of techniques. Gynecol. Oncol. 2002, 87, 39–45. [Google Scholar] [CrossRef]
- Penalver, M.A.; Angioli, R.; Mirhashemi, R.; Malik, R. Management of early and late complications of ileocolonic continent urinary reservoir (Miami pouch). Gynecol. Oncol. 1998, 69, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Pazar, B.; Yava, A.; Basal, S. Health-related quality of life in persons living with a urostomy. J. Wound Ostomy Cont. Nurs. 2015, 42, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Horch, R.E.; Ludolph, I.; Arkudas, A. Reconstruction of oncological defects of the perianal region. Chirurg 2021. [Google Scholar] [CrossRef]
- Schellerer, V.S.; Bartholomé, L.; Langheinrich, M.C.; Grützmann, R.; Horch, R.E.; Merkel, S.; Weber, K. Donor Site Morbidity of Patients Receiving Vertical Rectus Abdominis Myocutaneous Flap for Perineal, Vaginal or Inguinal Reconstruction. World J. Surg. 2021, 45, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Ludolph, I.; Arkudas, A.; Schmitz, M.; Boos, A.M.; Taeger, C.D.; Rother, U.; Horch, R.E.; Beier, J.P. Cracking the perfusion code? Laser-assisted Indocyanine Green angiography and combined laser Doppler spectrophotometry for intraoperative evaluation of tissue perfusion in autologous breast reconstruction with DIEP or ms-TRAM flaps. J. Plast Reconstr. Aesthet. Surg. 2016, 69, 1382–1388. [Google Scholar] [CrossRef] [PubMed]
- Ludolph, I.; Horch, R.E.; Arkudas, A.; Schmitz, M. Enhancing Safety in Reconstructive Microsurgery Using Intraoperative Indocyanine Green Angiography. Front. Surg. 2019, 6, 39. [Google Scholar] [CrossRef] [Green Version]
- Gentileschi, S.; Servillo, M.; Garganese, G.; Simona, F.; Scambia, G.; Salgarello, M. Versatility of pedicled anterolateral thigh flap in gynecologic reconstruction after vulvar cancer extirpative surgery. Microsurgery 2017, 37, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Fuzzard, S.K.; Mah, E.; Choong, P.F.M.; Grinsell, D. Lymphoedema rates in pedicled anterolateral thigh flaps for coverage of irradiated groin defects. ANZ J. Surg. 2020, 90, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Lefevre, J.H.; Parc, Y.; Kerneis, S.; Shields, C.; Touboul, E.; Chaouat, M.; Tiret, E. Abdomino-perineal resection for anal cancer: Impact of a vertical rectus abdominis myocutaneus flap on survival, recurrence, morbidity, and wound healing. Ann. Surg. 2009, 250, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Hui, K.; Zhang, F.; Pickus, E.; Rodriguez, L.F.; Teng, N.; Lineaweaver, W.C. Modification of the vertical rectus abdominis musculocutaneous (VRAM) flap for functional reconstruction of complex vulvoperineal defects. Ann. Plast. Surg. 2003, 51, 556–560. [Google Scholar] [CrossRef]
- Franchi, M.; Uccella, S.; Zorzato, P.C.; Dalle Carbonare, A.; Garzon, S.; Lagana, A.S.; Casarin, J.; Ghezzi, F. Vaginal flap for urethral neomeatus reconstruction after radical surgery for vulvar cancer: A retrospective cohort analysis. Int. J. Gynecol. Cancer 2019, 29, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Dabernig, J.; Shelley, O.P.; Cuccia, G.; Schaff, J. Urethral reconstruction using the radial forearm free flap: Experience in oncologic cases and gender reassignment. Eur. Urol 2007, 52, 547–553. [Google Scholar] [CrossRef]
- Hoang, D.; Goel, P.; Chen, V.W.; Carey, J. Phalloplasty Following Penectomy for Fournier’s Gangrene at a Tertiary Care Center. Cureus 2018, 10, e3698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horch, R.E. Fournier-Gangrän. Chirurg 2008, 79, 1080–1081. [Google Scholar] [CrossRef]
- Horch, R.E.; Gitsch, G.; Schultze-Seemann, W. Bilateral pedicled myocutaneous vertical rectus abdominus muscle flaps to close vesicovaginal and pouch-vaginal fistulas with simultaneous vaginal and perineal reconstruction in irradiated pelvic wounds. Urology 2002, 60, 502–507. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horch, R.E.; Ludolph, I.; Arkudas, A.; Cai, A. Personalized Reconstruction of Genital Defects in Complicated Wounds with Vertical Rectus Abdominis Myocutaneous Flaps including Urethral Neo-Orifice. J. Pers. Med. 2021, 11, 1076. https://doi.org/10.3390/jpm11111076
Horch RE, Ludolph I, Arkudas A, Cai A. Personalized Reconstruction of Genital Defects in Complicated Wounds with Vertical Rectus Abdominis Myocutaneous Flaps including Urethral Neo-Orifice. Journal of Personalized Medicine. 2021; 11(11):1076. https://doi.org/10.3390/jpm11111076
Chicago/Turabian StyleHorch, Raymund E., Ingo Ludolph, Andreas Arkudas, and Aijia Cai. 2021. "Personalized Reconstruction of Genital Defects in Complicated Wounds with Vertical Rectus Abdominis Myocutaneous Flaps including Urethral Neo-Orifice" Journal of Personalized Medicine 11, no. 11: 1076. https://doi.org/10.3390/jpm11111076
APA StyleHorch, R. E., Ludolph, I., Arkudas, A., & Cai, A. (2021). Personalized Reconstruction of Genital Defects in Complicated Wounds with Vertical Rectus Abdominis Myocutaneous Flaps including Urethral Neo-Orifice. Journal of Personalized Medicine, 11(11), 1076. https://doi.org/10.3390/jpm11111076