Development of a Nomogram Model for Treatment of Elderly Patients with Locoregionally Advanced Nasopharyngeal Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Extraction and Patient Selection
2.2. Examinations and Treatment Protocols
2.3. Follow-Up and Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics and Follow-Up
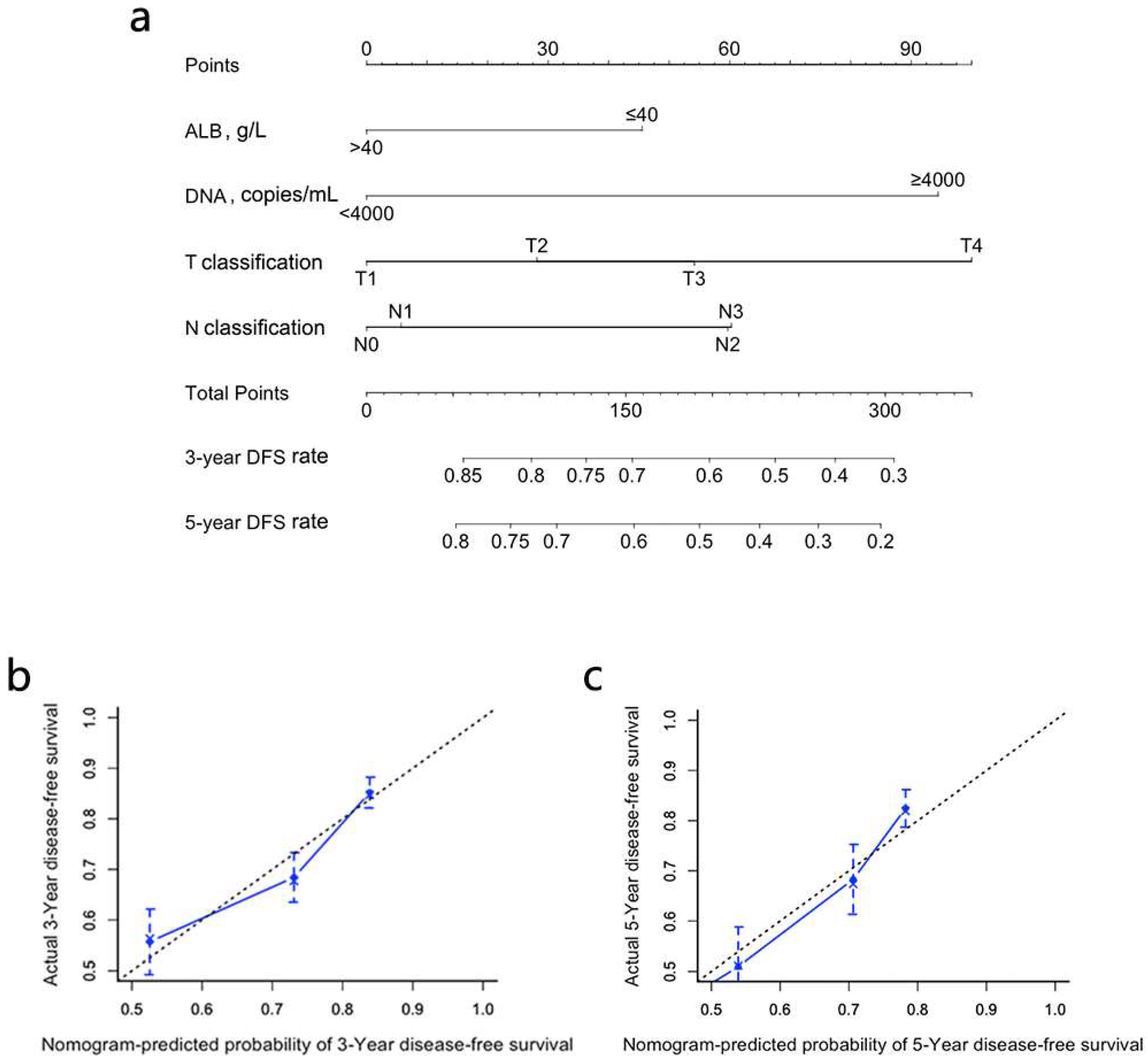
3.2. Development and Validation of Nomograms for DFS
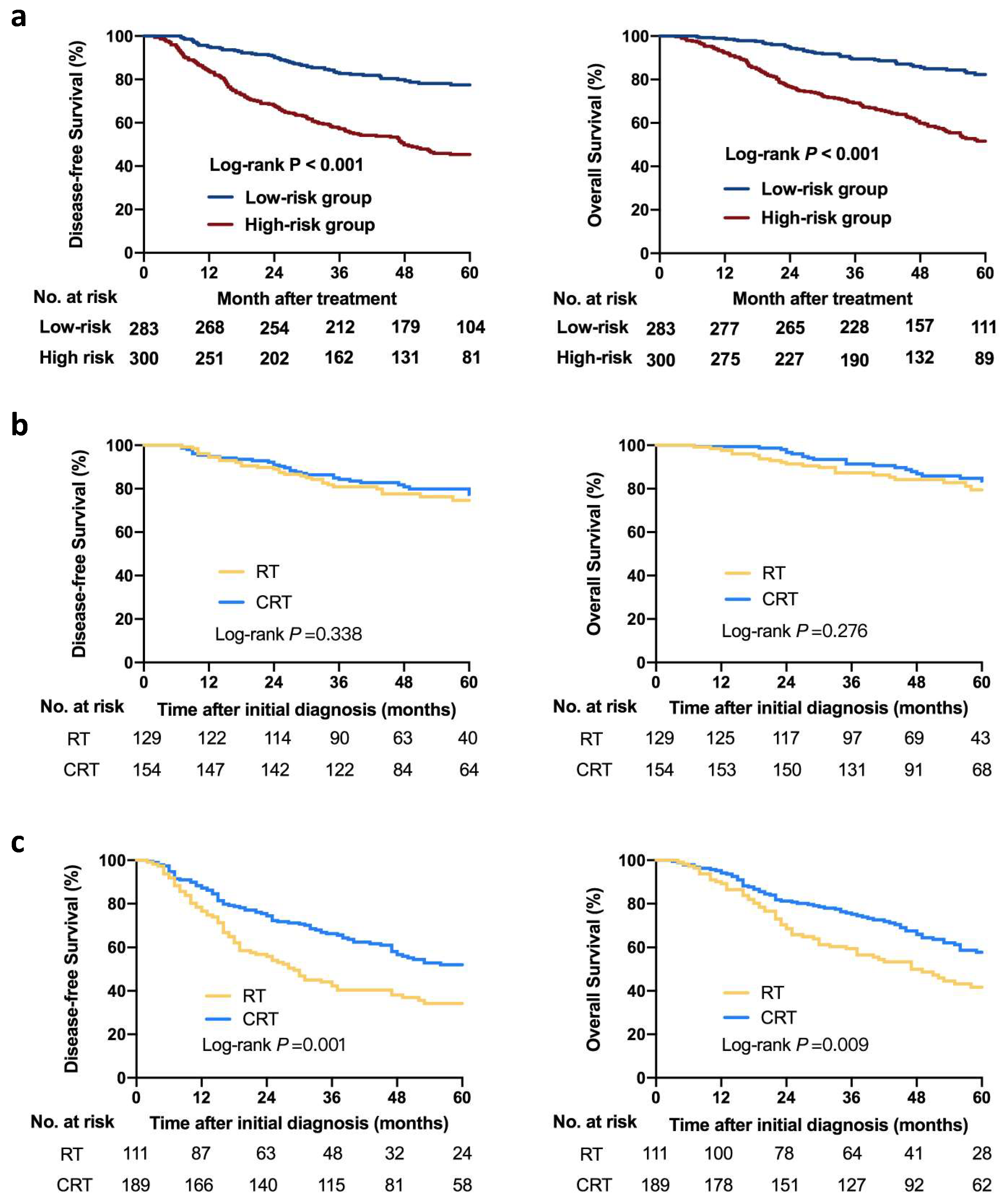
3.3. Risk Stratification Based on the Nomogram
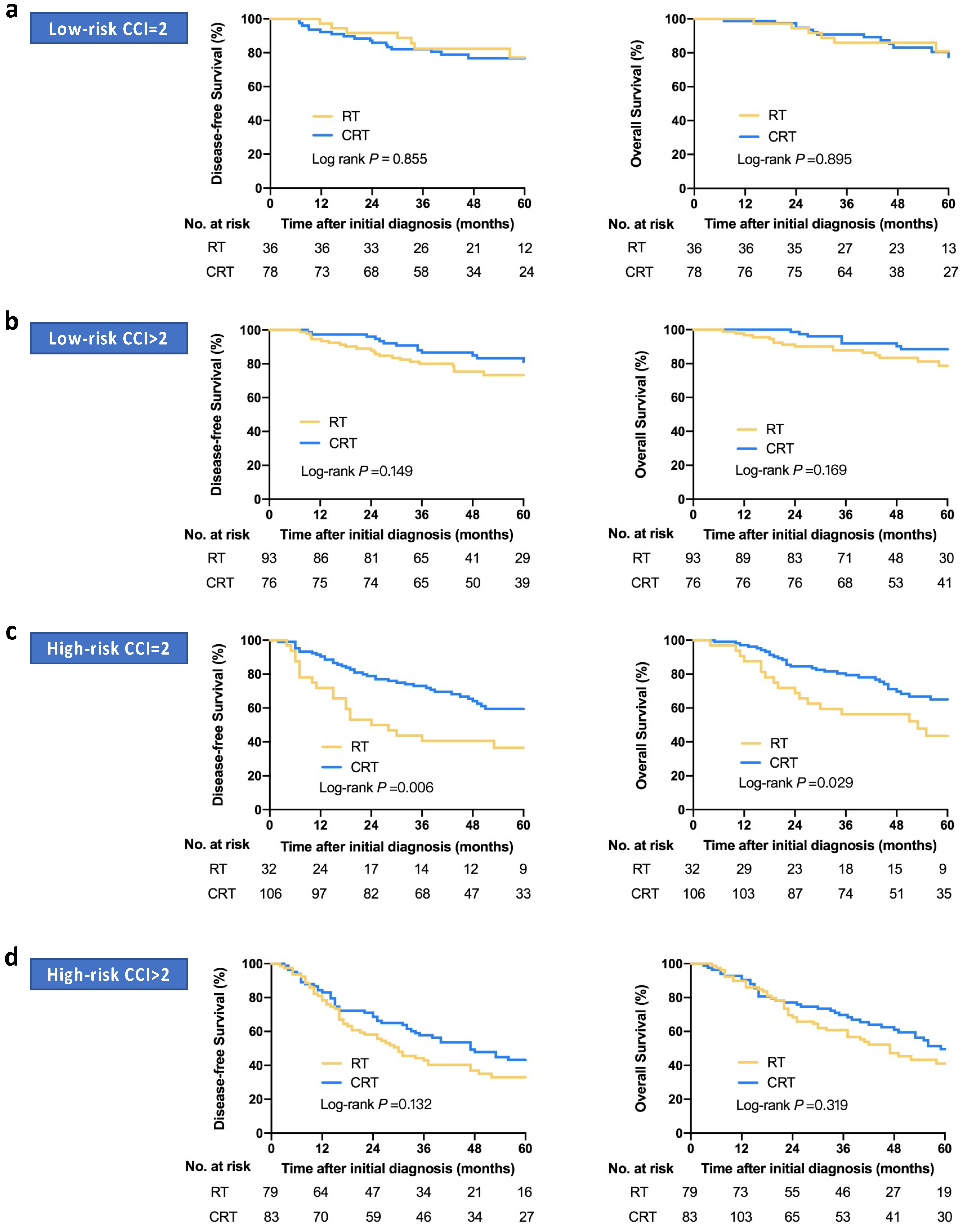
3.4. Risk-Adapted Treatment Strategies Based on the Nomogram and CCI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Wei, K.-R.; Zheng, R.-S.; Zhang, S.-W.; Liang, Z.-H.; Li, Z.-M.; Chen, W.-Q. Nasopharyngeal carcinoma incidence and mortality in China, 2013. Chin. J. Cancer 2017, 36, 90. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Haugen, M.; Moger, T.A.; Tretli, S.; Aalen, O.O.; Grotmol, T. Age-incidence curves of nasopharyngeal carcinoma worldwide: Bimodality in low-risk populations and aetiologic implications. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2356–2365. [Google Scholar]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.-G.; Liao, X.-L.; He, Z.-Y.; Tang, L.-Y.; Chen, X.-T.; Wang, Y.; Lin, Q. Demographic and clinicopathological characteristics of nasopharyngeal carcinoma and survival outcomes according to age at diagnosis: A population-based analysis. Oral Oncol. 2017, 73, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Hu, C.-S.; Chen, X.-Z.; Hu, G.-Q.; Cheng, Z.-B.; Sun, Y.; Li, W.-X.; Chen, Y.-Y.; Xie, F.-Y.; Liang, S.-B.; et al. Concurrent chemoradiotherapy plus adjuvant chemotherapy versus concurrent chemoradiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma: A phase 3 multicentre randomised controlled trial. Lancet Oncol. 2012, 13, 163–171. [Google Scholar] [CrossRef]
- Lin, J.-C.; Jan, J.-S.; Hsu, C.-Y.; Liang, W.-M.; Jiang, R.-S.; Wang, W.-Y. Phase III Study of Concurrent Chemoradiotherapy Versus Radiotherapy Alone for Advanced Nasopharyngeal Carcinoma: Positive Effect on Overall and Progression-Free Survival. J. Clin. Oncol. 2003, 21, 631–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Li, W.-F.; Chen, N.-Y.; Zhang, N.; Hu, G.-Q.; Xie, F.-Y.; Sun, Y.; Chen, X.-Z.; Li, J.-G.; Zhu, X.-D.; et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: A phase 3, multicentre, randomised controlled trial. Lancet Oncol. 2016, 17, 1509–1520. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, L.; Hu, G.-Q.; Zhang, N.; Zhu, X.-D.; Yang, K.-Y.; Jin, F.; Shi, M.; Chen, Y.P.; Hu, W.-H.; et al. Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma. N. Engl. J. Med. 2019, 381, 1124–1135. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New York, NY, USA, 2017. [Google Scholar]
- Lin, J.-C.; Wang, W.-Y.; Chen, K.Y.; Wei, Y.-H.; Liang, W.-M.; Jan, J.-S.; Jiang, R.-S. Quantification of Plasma Epstein–Barr Virus DNA in Patients with Advanced Nasopharyngeal Carcinoma. N. Engl. J. Med. 2004, 350, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.M.; Chan, A.T.C.; Chan, L.Y.; Leung, S.F.; Lam, C.W.; Huang, D.P.; Johnson, P.J. Molecular prognostication of nasopharyngeal carcinoma by quantitative analysis of circulating Epstein-Barr virus DNA. Cancer Res. 2000, 60, 6878–6881. [Google Scholar]
- Guo, R.; Tang, L.-L.; Mao, Y.-P.; Du, X.; Chen, L.; Zhang, Z.-C.; Liu, L.-Z.; Tian, L.; Luo, X.-T.; Xie, Y.; et al. Proposed modifications and incorporation of plasma Epstein-Barr virus DNA improve the TNM staging system for Epstein-Barr virus-related nasopharyngeal carcinoma. Cancer 2019, 125, 79–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.-L.; Sun, Z.-Q.; Guo, R.; Liu, X.; Mao, Y.-P.; Peng, H.; Tian, L.; Lin, A.-H.; Li, L.; Shao, J.-Y.; et al. Plasma Epstein-Barr Virus DNA Load After Induction Chemotherapy Predicts Outcome in Locoregionally Advanced Nasopharyngeal Carcinoma. Int. J. Radiat. Oncol. 2019, 104, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Leung, S.F.; Chan, K.C.; Ma, B.B.; Hui, E.P.; Mo, F.; Chow, K.C.; Leung, L.; Chu, K.W.; Zee, B.; Lo, Y.M.; et al. Plasma Epstein–Barr viral DNA load at midpoint of radiotherapy course predicts outcome in advanced-stage nasopharyngeal carcinoma. Ann. Oncol. 2014, 25, 1204–1208. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.Q.; Li, C.F.; Li, J.; Chen, W.H.; Chen, Q.Y.; Yuan, L.X.; Lai, X.P.; He, Y.; Xu, Y.X.; Hu, D.P.; et al. Establishment and Validation of Prognostic Nomograms for Endemic Nasopharyngeal Carcinoma. J. Natl. Cancer Inst. 2016, 108, djv291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, J.; He, Y.; Sun, X.S.; Li, J.M.; Xin, M.Z.; Li, W.Q.; Li, Z.X.; Nie, S.; Wang, C.; Li, Y.Z.; et al. Construction of a comprehensive nutritional index and its correlation with quality of life and survival in patients with nasopharyngeal carcinoma undergoing IMRT: A prospective study. Oral Oncol. 2019, 98, 62–68. [Google Scholar] [CrossRef]
- Gao, J.; Hu, J.Y.; Xia, Y.F.; Yi, W.; Tao, Y.L.; Li, G. Continuous fall in hemoglobin level is a poor prognostic factor in patients with nasopharyngeal carcinoma treated with radiotherapy. Chin. J. Cancer 2010, 29, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Tao, Y.L.; Li, G.; Yi, W.; Xia, Y.-F. Involvement of Difference in Decrease of Hemoglobin Level in Poor Prognosis of Stage I and II Nasopharyngeal Carcinoma: Implication in Outcome of Radiotherapy. Int. J. Radiat. Oncol. 2012, 82, 1471–1478. [Google Scholar] [CrossRef]
- Wan, X.B.; Wei, L.; Li, H.; Dong, M.; Lin, Q.; Ma, X.K.; Huang, P.Y.; Wen, J.Y.; Li, X.; Chen, J.; et al. High pretreatment serum lactate dehydrogenase level correlates with disease relapse and predicts an inferior outcome in locally advanced nasopharyngeal carcinoma. Eur. J. Cancer 2013, 49, 2356–2364. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.X.; Zhang, H.B.; Shi, J.L.; Lu, X.; Wang, L.; Ye, Y.F.; Cao, K.J.; Qian, C.N.; Guo, X.; Xiang, Y.Q. A prognostic model predicts the risk of distant metastasis and death for patients with nasopharyngeal carcinoma based on pre-treatment serum C-reactive protein and N-classification. Eur. J. Cancer 2013, 49, 2152–2160. [Google Scholar] [CrossRef] [PubMed]
- Bøje, C.R. Impact of comorbidity on treatment outcome in head and neck squamous cell carcinoma—A systematic review. Radiother. Oncol. 2014, 110, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.D.; Zhou, G.Q.; Lv, J.W.; Zhou, H.Q.; Zhong, C.W.; Wu, C.F.; Zheng, Z.Q.; He, X.J.; Peng, L.; Ma, J.; et al. Competing risk nomograms for nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: A big-data, intelligence platform-based analysis. Radiother. Oncol. 2018, 129, 389–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Chan, A.T.; Lo, Y.M.; Zee, B.; Chan, L.Y.; Ma, B.B.; Leung, S.F.; Mo, F.; Lai, M.; Ho, S.; Huang, D.P.; et al. Plasma Epstein-Barr Virus DNA and Residual Disease After Radiotherapy for Undifferentiated Nasopharyngeal Carcinoma. J. Natl. Cancer Inst. 2002, 94, 1614–1619. [Google Scholar] [CrossRef]
- Leung, S.F.; Zee, B.; Ma, B.B.; Hui, E.P.; Mo, F.; Lai, M.; Chan, K.A.; Chan, L.Y.; Kwan, W.-H.; Lo, Y.D.; et al. Plasma Epstein-Barr Viral Deoxyribonucleic Acid Quantitation Complements Tumor-Node-Metastasis Staging Prognostication in Nasopharyngeal Carcinoma. J. Clin. Oncol. 2006, 24, 5414–5418. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Cao, S.M.; Guo, L.; Hua, Y.J.; Huang, P.Y.; Zhang, X.L.; Lin, M.; You, R.; Zou, X.; Liu, Y.P.; et al. Induction chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: Long-term results of a phase III multicentre randomised controlled trial. Eur. J. Cancer 2019, 119, 87–96. [Google Scholar] [CrossRef]
- Liu, H.; Chen, Q.-Y.; Guo, L.; Tang, L.-Q.; Mo, H.-Y.; Zhong, Z.-L.; Huang, P.-Y.; Luo, D.-H.; Sun, R.; Guo, X.; et al. Feasibility and efficacy of chemoradiotherapy for elderly patients with locoregionally advanced nasopharyngeal carcinoma: Results from a matched cohort analysis. Radiat. Oncol. 2013, 8, 70. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Q.; Xiang, Y.Q.; Wu, P.H.; Lv, X.; Qian, C.-N.; Guo, X. A Matched Cohort Study of Standard Chemo-Radiotherapy versus Radiotherapy Alone in Elderly Nasopharyngeal Carcinoma Patients. PLoS ONE 2015, 10, e0119593. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.N.; Zhang, W.; Cai, X.Y.; Li, M.S.; Lawrence, W.R.; Wang, S.Y.; Mai, D.M.; Du, Y.Y.; Luo, D.H.; Mo, H.Y. The Characteristics and Survival Outcomes in Patients Aged 70 Years and Older with Nasopharyngeal Carcinoma in the Intensity-Modulated Radiotherapy Era. Cancer Res. Treat. 2019, 51, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miao, J.; Wang, L.; Zhu, M.; Xiao, W.; Wu, H.; Di, M.; Huang, Y.; Huang, S.; Han, F.; Deng, X.; et al. Long-term survival and late toxicities of elderly nasopharyngeal carcinoma (NPC) patients treated by high-total- and fractionated-dose simultaneous modulated accelerated radiotherapy with or without chemotherapy. Oral Oncol. 2018, 89, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Sommat, K.; Yit, N.L.F.; Wang, F.; Lim, J.H.C. Impact of comorbidity on tolerability and survival following curative intent intensity modulated radiotherapy in older patients with nasopharyngeal cancer. J. Geriatr. Oncol. 2018, 9, 352–358. [Google Scholar] [CrossRef]
- Lv, J.; Chen, Y.; Zhou, G.; Qi, Z.; Tan, K.R.L.; Wang, H.; Lin, L.; Chen, F.; Zhang, L.; Huang, X.; et al. Liquid biopsy tracking during sequential chemo-radiotherapy identifies distinct prognostic phenotypes in nasopharyngeal carcinoma. Nat. Commun. 2019, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Balducci, L.; Corcoran, M.B. Antineoplastic chemotherapy of the older cancer patient. Hematol. Oncol. Clin. N. Am. 2000, 14, 193–212. [Google Scholar] [CrossRef]
- Hoppe, S.; Rainfray, M.; Fonck, M.; Hoppenreys, L.; Blanc, J.F.; Ceccaldi, J.; Mertens, C.; Blanc-Bisson, C.; Imbert, Y.; Cany, L.; et al. Functional Decline in Older Patients With Cancer Receiving First-Line Chemotherapy. J. Clin. Oncol. 2013, 31, 3877–3882. [Google Scholar] [CrossRef]
- Huang, W.Y.; Lin, C.L.; Lin, C.Y.; Jen, Y.M.; Lo, C.H.; Sung, F.C.; Kao, C.H. Survival outcome of patients with nasopharyngeal carcinoma: A nationwide analysis of 13 407 patients in Taiwan. Clin. Otolaryngol. 2015, 40, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Piccirillo, J.F.; Tierney, R.M.; Costas, I.; Grove, L.; Spitznagel, E.L., Jr. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA 2004, 291, 2441–2447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.H.; Yen, Y.C.; Yang, H.C.; Liu, S.H.; Yuan, S.P.; Wu, L.L.; Lee, F.P.; Lin, K.C.; Lai, M.T.; Wu, C.C.; et al. Curative-Intent Aggressive Treatment Improves Survival in Elderly Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma and High Comorbidity Index. Medicine 2016, 95, e3268. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Entire Cohort No. (%) | p-Value | HR (95% CI) |
|---|---|---|---|
| Age, years | |||
| ≤68 | 336 (57.6%) | Ref. | |
| >68 | 247 (42.4%) | 0.076 | 1.26 (0.97–1.63) |
| Gender | |||
| Male | 463 (79.4) | Ref. | |
| Female | 120 (20.6) | 0.373 | 0.86 (0.61–1.20) |
| Histological type (WHO) 1 | |||
| Type I–II | 18 (3.1) | Ref. | |
| Type III | 565 (96.9) | 0.749 | 1.14 (0.51–2.57) |
| Smoking | |||
| Yes | 232 (39.8) | Ref. | |
| No | 351 (60.2) | 0.992 | 1.00 (0.77–1.30) |
| Drinking | |||
| Yes | 92 (15.8) | Ref. | |
| No | 491 (84.2) | 0.970 | 0.99 (0.70–1.42) |
| Family history of NPC | |||
| Yes | 115 (19.7) | Ref. | |
| No | 468 (80.3) | 0.321 | 0.84 (0.60–1.18) |
| EBV DNA, copies/mL 2 | |||
| <4000 | 320 (54.9) | Ref. | |
| ≥4000 | 263 (45.1) | < 0.001 | 2.65 (2.03–3.47) |
| LDH, IU/L 2 | |||
| ≤250 | 540 (92.6) | Ref. | |
| >250 | 43 (7.4) | 0.243 | 1.32 (0.83–2.12) |
| HGB, g/L 2 | |||
| ≤120 | 51 (8.7) | Ref. | |
| >120 | 532 (91.3) | 0.024 | 0.63 (0.42–0.94) |
| CRP, mg/L 2 | |||
| ≤3 | 349 (59.9) | Ref. | |
| >3 | 234 (40.1) | 0.043 | 1.31 (1.01–1.69) |
| ALB, g/L 2 | |||
| ≤40 | 117 (20.1) | Ref. | |
| >40 | 466 (79.9) | < 0.001 | 0.59 (0.44–0.78) |
| T classification 3 | |||
| T4 | 161 (27.5) | Ref. | |
| T1 | 19 (3.3) | 0.146 | 0.56 (0.26–1.22) |
| T2 | 18 (3.1) | 0.369 | 0.70 (0.32–1.51) |
| T3 | 385 (66.0) | < 0.001 | 0.53 (0.41–0.69) |
| N classification 3 | |||
| N0 | 92 (15.8) | Ref. | |
| N1 | 265 (45.5) | 0.362 | 1.22 (0.80–1.87) |
| N2 | 138 (23.7) | 0.003 | 1.97 (1.26–3.08) |
| N3 | 88 (15.1) | < 0.001 | 2.34 (1.46–3.77) |
| Overall stage 3 | |||
| III | 358 (61.4) | Ref. | |
| IVa | 225 (38.6) | < 0.001 | 1.99 (1.54–2.58) |
| Radiotherapy techniques | |||
| IMRT | 569 (97.6%) | Ref. | |
| 2D-RT/3D-CRT | 14 (2.4%) | 0.752 | 0.88 (0.38–1.97) |
| CCI 4 | |||
| =2 | 252 (43.2) | - | - |
| >2 | 331 (56.8) | - | - |
| Treatment modality | |||
| RT alone | 240 (41.2) | - | - |
| CRT | 343 (58.8) | - | - |
| Risk Factors | C-Index (95% CI) | p-Value | AUC (95% CI) | p-Value |
|---|---|---|---|---|
| Prognostic models | ||||
| Nomogram | 0.668 (0.633–0.703) | Ref. | 0.710 (0.671–0.746) | Ref. |
| 8th TNM staging system 1 | 0.585 (0.552–0.618) | <0.001 | 0.607 (0.567–0.647) | <0.001 |
| Single risk factors | ||||
| EBV DNA | 0.619 (0.587–0.652) | <0.001 | 0.656 (0.617–0.695) | <0.001 |
| T classification 1 | 0.561 (0.528–0.595) | <0.001 | 0.588 (0.547–0.628) | <0.001 |
| N classification 1 | 0.584 (0.548–0.620) | <0.001 | 0.590 (0.549–0.630) | <0.001 |
| ALB | 0.549 (0.520–0.578) | <0.001 | 0.558 (0.517–0.599) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kou, J.; Zhang, L.-L.; Yang, X.-L.; Wen, D.-W.; Zhou, G.-Q.; Wu, C.-F.; Xu, S.-S.; Zheng, W.-H.; Qi, Z.-Y.; Sun, Y.; et al. Development of a Nomogram Model for Treatment of Elderly Patients with Locoregionally Advanced Nasopharyngeal Carcinoma. J. Pers. Med. 2021, 11, 1065. https://doi.org/10.3390/jpm11111065
Kou J, Zhang L-L, Yang X-L, Wen D-W, Zhou G-Q, Wu C-F, Xu S-S, Zheng W-H, Qi Z-Y, Sun Y, et al. Development of a Nomogram Model for Treatment of Elderly Patients with Locoregionally Advanced Nasopharyngeal Carcinoma. Journal of Personalized Medicine. 2021; 11(11):1065. https://doi.org/10.3390/jpm11111065
Chicago/Turabian StyleKou, Jia, Lu-Lu Zhang, Xing-Li Yang, Dan-Wan Wen, Guan-Qun Zhou, Chen-Fei Wu, Si-Si Xu, Wei-Hong Zheng, Zhen-Yu Qi, Ying Sun, and et al. 2021. "Development of a Nomogram Model for Treatment of Elderly Patients with Locoregionally Advanced Nasopharyngeal Carcinoma" Journal of Personalized Medicine 11, no. 11: 1065. https://doi.org/10.3390/jpm11111065