
Engaging Patients with Late-Stage Non-Small Cell Lung Cancer in Shared Decision Making about Treatment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of a DSI Prototype for Use with Patients Diagnosed with Late-Stage NSCLC
2.2. Design Panel
2.3. Physician Panel
2.4. Patient Panel
2.5. The Pilot Study
3. Results
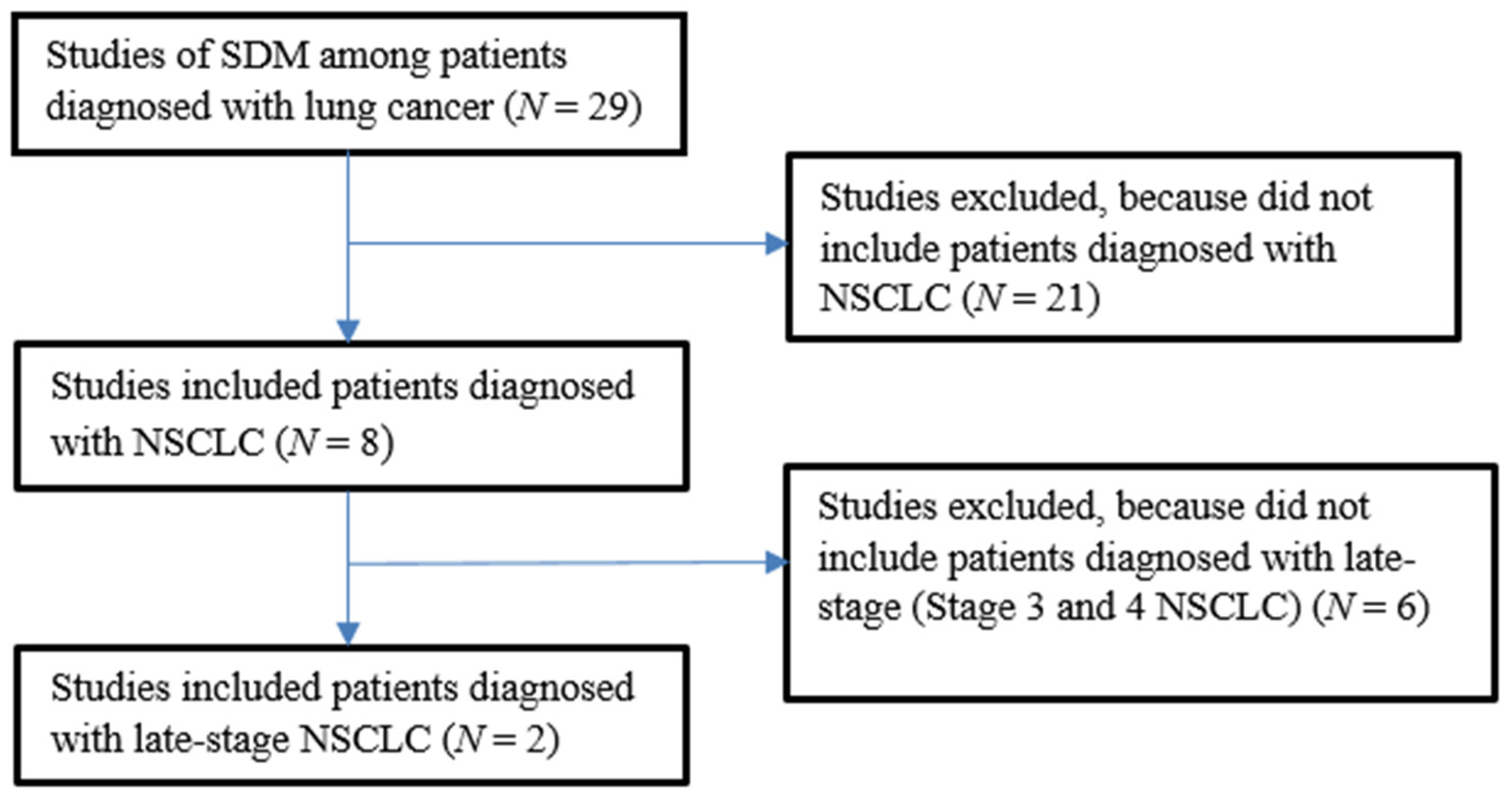
3.1. Scoping Review
3.2. Design Panel
3.3. Physician Panel
3.4. Patient Panel
3.5. The Pilot Study
3.5.1. Demographic Characteristics
3.5.2. Change in Perceptions about Treatment
3.5.3. Change in Decisional Conflict about Treatment
3.5.4. Recommended Treatment Options, Treatment Preference, and Treatment Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Abreu, D.; Powell, S.F.; Hochmair, M.J.; Gadgeel, S.; Esteban, E.; Felip, E.; Speranza, G.; De Angelis, F.; Dómine, M.; Cheng, S.Y.; et al. Pemetrexed plus platinum with or without pembrolizumab in patients with previously untreated metastatic nonsquamous NSCLC: Protocol-specified final analysis from KEYNOTE-189. Ann. Oncol. 2021, 32, 881–895. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy for Metastatic Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score ≥ 50. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. FLAURA Investigators Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Zukin, M.; Barrios, C.H.; Pereira, J.R.; Ribeiro, R.D.A.; de Mendonça Beato, C.A.; do Nascimento, Y.N.; Murad, A.; Franke, F.A.; Precivale, M.; de Lima Araujo, L.H.; et al. Randomized phase III trial of single-agent pemetrexed versus carboplatin and pemetrexed in patients with advanced non-small-cell lung cancer and Eastern Cooperative Oncology Group performance status of 2. J. Clin. Oncol. 2013, 31, 2849–2853. [Google Scholar] [CrossRef] [PubMed]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.F.; et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, D.E.; Kazerooni, E.A.; Baum, S.L.; Eapen, G.A.; Ettinger, D.S.; Hou, L.; Jackman, D.M.; Klippenstein, D.; Kumar, R.; Lackner, R.P.; et al. Lung cancer screening, version 3.2018, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 412–441. [Google Scholar] [CrossRef]
- Cojean, I.; Le Chevalier, T. Chemotherapy of stage IIIB and IV non-small-cell lung cancer. Ann. Oncol. 1995, 6 (Suppl. S3), S41–S44. [Google Scholar] [CrossRef]
- Levinson, W.; Kao, A.; Kuby, A.; Thisted, R.A. Not all patients want to participate in decision making. A national study of public preferences. J. Gen. Intern. Med. 2005, 20, 531–535. [Google Scholar] [CrossRef] [Green Version]
- Leighl, N.B.; Shepherd, F.A.; Zawisza, D.; Burkes, R.L.; Feld, R.; Waldron, J.; Sun, A.; Payne, D.; Bezjak, A.; Tattersall, M.H.N. Enhancing treatment decision-making: Pilot study of a treatment decision aid in stage IV non-small cell lung cancer. Br. J. Cancer 2008, 98, 1769–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, S.H.; Greenfield, S.; Gandek, B.; Rogers, W.H.; Ware, J.E. Characteristics of physicians with participatory decision-making styles. Ann. Intern. Med. 1996, 124, 497–504. [Google Scholar] [CrossRef]
- Elwyn, G.; Edwards, A.; Hood, K.; Robling, M.; Atwell, C.; Russell, I.; Wensing, M.; Grol, R. Study Steering Group Achieving involvement: Process outcomes from a cluster randomized trial of shared decision making skill development and use of risk communication aids in general practice. Fam. Pract. 2004, 21, 337–346. [Google Scholar] [CrossRef]
- Hopmans, W.; Damman, O.C.; Senan, S.; Hartemink, K.J.; Smit, E.F.; Timmermans, D.R.M. A patient perspective on shared decision making in stage I non-small cell lung cancer: A mixed methods study. BMC Cancer 2015, 15, 959. [Google Scholar] [CrossRef] [PubMed]
- Grossman Liu, L.; Ancker, J.S.; Masterson Creber, R.M. Improving patient engagement through patient decision support. Am. J. Prev. Med. 2021, 60, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Titler, M.G.; Reiter, R.C.; Corry, L. Decision-support interventions for patients. Medsurg. Nurs. 1996, 5, 57–61. [Google Scholar]
- Spiegle, G.; Al-Sukhni, E.; Schmocker, S.; Gagliardi, A.R.; Victor, J.C.; Baxter, N.N.; Kennedy, E.D. Patient decision aids for cancer treatment: Are there any alternatives? Cancer 2013, 119, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Flocke, S.A.; Antognoli, E.; Daly, B.J.; Jackson, B.; Fulton, S.E.; Liu, T.M.; Surdam, J.; Manne, S.; Meropol, N.J. The role of oncology nurses in discussing clinical trials. Oncol. Nurs. Forum 2017, 44, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Coulter, A.; Stilwell, D.; Kryworuchko, J.; Mullen, P.D.; Ng, C.J.; van der Weijden, T. A systematic development process for patient decision aids. BMC Med. Inf. Decis. Mak. 2013, 13 (Suppl. S2), S2. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, A.M. Validation of a decisional conflict scale. Med. Decis. Mak. 1995, 15, 25–30. [Google Scholar] [CrossRef]
- Fiset, V.; O’Connor, A.M.; Evans, W.; Graham, I.; Degrasse, C.; Logan, J. Development and evaluation of a decision aid for patients with stage IV non-small cell lung cancer. Health Expect. 2000, 3, 125–136. [Google Scholar] [CrossRef]
- Spronk, I.; Meijers, M.C.; Heins, M.J.; Francke, A.L.; Elwyn, G.; van Lindert, A.; van Dulmen, S.; van Vliet, L.M. Availability and effectiveness of decision aids for supporting shared decision making in patients with advanced colorectal and lung cancer: Results from a systematic review. Eur. J. Cancer Care 2019, 28, e13079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DuBenske, L.L.; Gustafson, D.H.; Shaw, B.R.; Cleary, J.F. Web-based cancer communication and decision making systems: Connecting patients, caregivers, and clinicians for improved health outcomes. Med. Decis. Mak. 2010, 30, 732–744. [Google Scholar] [CrossRef] [PubMed]
- Meropol, N.J.; Egleston, B.L.; Buzaglo, J.S.; Balshem, A.; Benson, A.B.; Cegala, D.J.; Cohen, R.B.; Collins, M.; Diefenbach, M.A.; Miller, S.M.; et al. A Web-based communication aid for patients with cancer: The CONNECT Study. Cancer 2013, 119, 1437–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Leeuw, J.; Larsson, M. Nurse-led follow-up care for cancer patients: What is known and what is needed. Support. Care Cancer 2013, 21, 2643–2649. [Google Scholar] [CrossRef]
- Kufe, D.W.; Holland, J.F.; Frei, E. American Cancer Society. In Cancer Medicine6:Review: A Companion to Holland-Frei Cancer Medicine-6, 6th ed.; B C Decker Inc.: Hamilton, ON, Canada, 2003; p. 178. [Google Scholar]
- Légaré, F.; Stacey, D.; Pouliot, S.; Gauvin, F.-P.; Desroches, S.; Kryworuchko, J.; Dunn, S.; Elwyn, G.; Frosch, D.; Gagnon, M.-P.; et al. Interprofessionalism and shared decision-making in primary care: A stepwise approach towards a new model. J. Interprof. Care 2011, 25, 18–25. [Google Scholar] [CrossRef]
- Alsulamy, N.; Lee, A.; Thokala, P.; Alessa, T. What influences the implementation of shared decision making: An umbrella review. Patient Educ. Couns. 2020, 103, 2400–2407. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Physician Panel Themes | Patient Panel Themes |
|---|---|
| Tailoring Treatment to the patient | Patient and caregiver involvement |
| Physician-patient communication | Physician-patient communication |
| Engaging members of the clinical team | Engaging members of the clinical team |
| Integrating DSIs in clinical care | Integrating DSIs in clinical care |
| Characteristic | Category | N | % |
|---|---|---|---|
| Sex | Female | 3 | 60.0 |
| Male | 2 | 40.0 | |
| Race | Black or African American | 1 | 20.0 |
| White | 4 | 80.0 | |
| Ethnicity | Not Hispanic or Latino | 5 | 100.0 |
| Marital Status | Married | 2 | 40.0 |
| Single | 2 | 40.0 | |
| Widowed | 1 | 20.0 | |
| Education | Less than a High School Diploma | 0 | 0.0 |
| High School Diploma | 2 | 40.0 | |
| Some College or Associate Degree | 2 | 40.0 | |
| Bachelor’s Degree | 1 | 20.0 | |
| Master’s Degree or higher | 0 | 0.0 |
| Variable | Baseline Survey | Exit Survey | |
|---|---|---|---|
| Belief in Cure From Treatment | Yes | 2 | 2 |
| No | 1 | 2 | |
| Unsure | 2 | 1 | |
| Awareness of Treatment Options | Yes | 2 | 5 |
| No | 1 | 0 | |
| Unsure | 2 | 0 | |
| Concern about Treatment Costs | Yes | 3 | 1 |
| No | 2 | 3 | |
| Unsure | 0 | 1 |
| Variable | Mean Baseline Survey Score | Mean Exit Survey Score | Change |
|---|---|---|---|
| Decisional Conflict Scale | 2.2 | 3.2 | +1.0 |
| Participant | Treatment Option 1 | Treatment Option 2 | Treatment Preference | Treatment Status |
|---|---|---|---|---|
| 1 | Chemotherapy and Immunotherapy | Immunotherapy | Chemotherapy and Immunotherapy | Undecided |
| 2 | Chemotherapy and Immunotherapy | Chemotherapy | Chemotherapy and Immunotherapy | Chemotherapy and Immunotherapy |
| 3 | Immunotherapy | Clinical Trial | Immunotherapy | Clinical Trial |
| 4 | Chemotherapy | Clinical Trial | Chemotherapy | Chemotherapy |
| 5 | Immunotherapy | Supportive Care | Immunotherapy | Chemotherapy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myers, R.E.; Advani, S.M.; Myers, P.; Selvan, P.; Garber, G.; Worster, B.; Flomenberg, N.; Chapman, A.; Zinner, R. Engaging Patients with Late-Stage Non-Small Cell Lung Cancer in Shared Decision Making about Treatment. J. Pers. Med. 2021, 11, 998. https://doi.org/10.3390/jpm11100998
Myers RE, Advani SM, Myers P, Selvan P, Garber G, Worster B, Flomenberg N, Chapman A, Zinner R. Engaging Patients with Late-Stage Non-Small Cell Lung Cancer in Shared Decision Making about Treatment. Journal of Personalized Medicine. 2021; 11(10):998. https://doi.org/10.3390/jpm11100998
Chicago/Turabian StyleMyers, Ronald E., Shailesh M. Advani, Pamela Myers, Preethi Selvan, Gregory Garber, Brooke Worster, Neal Flomenberg, Andrew Chapman, and Ralph Zinner. 2021. "Engaging Patients with Late-Stage Non-Small Cell Lung Cancer in Shared Decision Making about Treatment" Journal of Personalized Medicine 11, no. 10: 998. https://doi.org/10.3390/jpm11100998
APA StyleMyers, R. E., Advani, S. M., Myers, P., Selvan, P., Garber, G., Worster, B., Flomenberg, N., Chapman, A., & Zinner, R. (2021). Engaging Patients with Late-Stage Non-Small Cell Lung Cancer in Shared Decision Making about Treatment. Journal of Personalized Medicine, 11(10), 998. https://doi.org/10.3390/jpm11100998