Digital Interventions for Psychological Comorbidities in Chronic Diseases—A Systematic Review

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
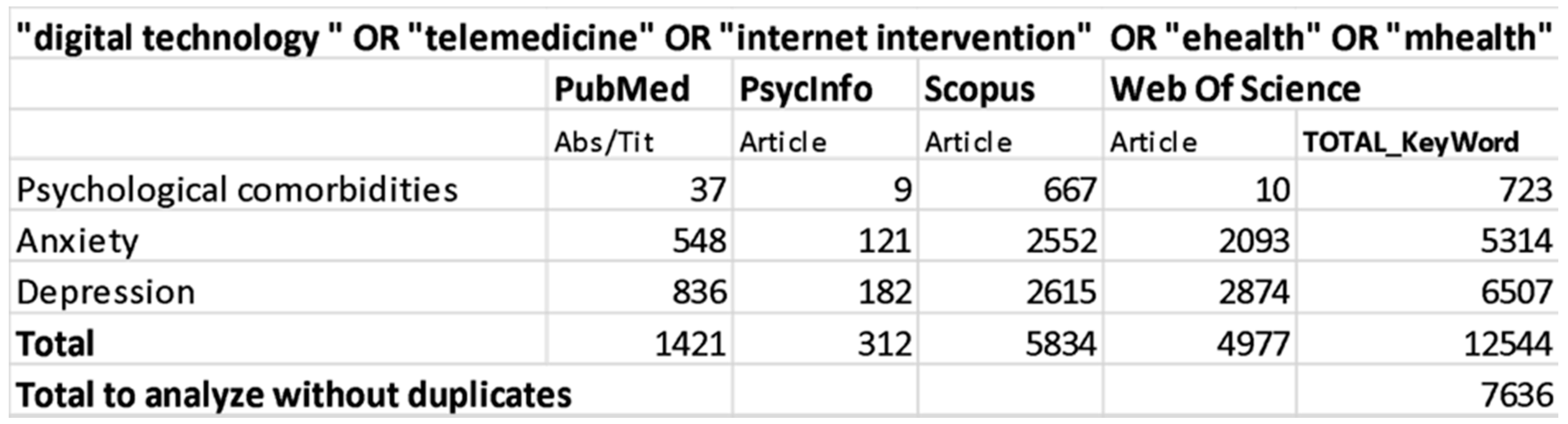
2.1. Search Strategy
2.2. Study Eligibility and Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
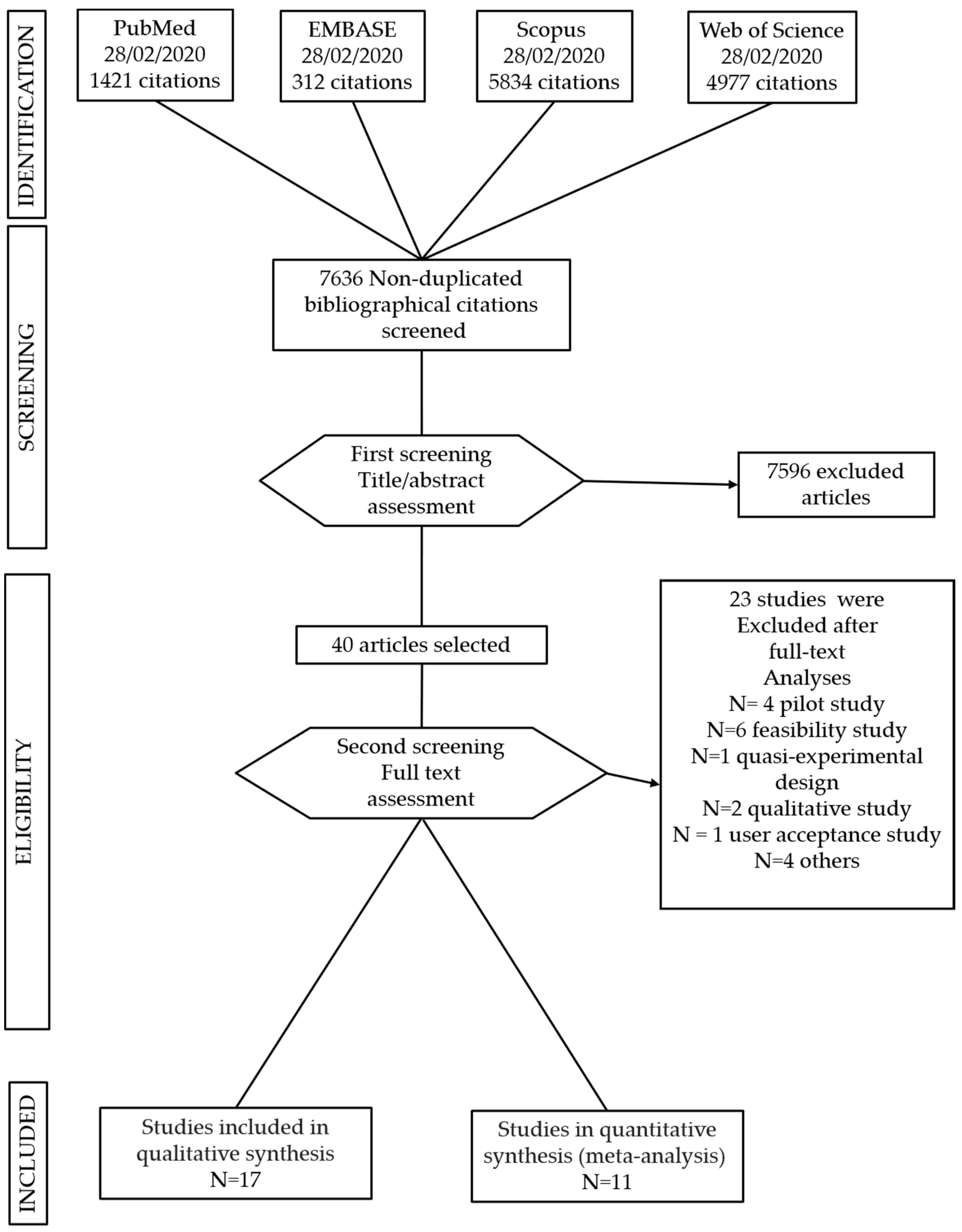
3.1. Studies Included
3.2. Risk of Bias
3.3. Interventions’ Description
3.4. Treatment Efficacy on Psychological Comorbidities
3.5. Results of the Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases. Key Facts [Internet] Geneva. (GVA). Available online: https://www.who.int/health-topics/noncommunicable-diseases#tab=tab_1 (accessed on 7 May 2020).
- Pryor, L.; Da Silva, M.A.; Melchior, M. Mental Health and Global Strategies to Reduce NCDs and Premature Mortality. Lancet Public Health 2017, 2, e350–e351. [Google Scholar] [CrossRef]
- Lee, J.A.; Choi, M.; Lee, S.A.; Jiang, N. Effective Behavioral Intervention Strategies Using Mobile Health Applications for Chronic Disease Management: A Systematic Review. BMC Med. Inform. Decis. Mak. 2018, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.H.; Brath, H. A Global View on the Development of Non Communicable Diseases. Prev. Med. 2012, 54, S38–S41. [Google Scholar] [CrossRef] [PubMed]
- Ngo, V.K.; Rubinstein, A.; Ganju, V.; Kanellis, P.; Loza, N.; Rabadan-Diehl, C.; Daar, A.S. Grand Challenges: Integrating Mental Health Care into the Non-Communicable Disease Agenda. PLoS Med. 2013, 10, e1001443. [Google Scholar] [CrossRef]
- Herrick, C. The Optics of Noncommunicable Diseases: From Lifestyle to Environmental Toxicity. Sociol. Health Illn. 2020, 42, 1041–1059. [Google Scholar] [CrossRef]
- Verma, M.; Grover, S.; Tripathy, J.P.; Singh, T.; Nagaraja, S.B.; Kathirvel, S.; Singh, G.; Nehra, R. Co-Existing Non-Communicable Diseases and Mental Illnesses amongst the Elderly in Punjab, India. Eur. Endocrinol. 2019, 15, 106–112. [Google Scholar] [CrossRef]
- Anderson, R.; Freedland, K.; RE, C.; Lustman, P.J. The Prevalence of Comorbid Depression. Diabetes Care 2001, 24, 1069–1078. [Google Scholar] [CrossRef]
- Moussavi, S.; Chatterji, S.; Verdes, E.; Tandon, A.; Patel, V.; Ustun, B. Depression, Chronic Diseases, and Decrements in Health: Results from the World Health Surveys. Lancet 2007, 370, 851–858. [Google Scholar] [CrossRef]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and Cardiovascular Disease: A Clinical Review. Eur. Heart J. 2014, 35, 1365–1372. [Google Scholar] [CrossRef]
- Shao, M.; Lin, X.; Jiang, D.; Tian, H.; Xu, Y.; Wang, L.; Ji, F.; Zhou, C.; Song, X.; Zhuo, C. Depression and Cardiovascular Disease: Shared Molecular Mechanisms and Clinical Implications. Psychiatry Res. 2020, 285, 112802. [Google Scholar] [CrossRef]
- Bucciarelli, V.; Caterino, A.L.; Bianco, F.; Caputi, C.G.; Salerni, S.; Sciomer, S.; Maffei, S.; Gallina, S. Depression and Cardiovascular Disease: The Deep Blue Sea of Women’s Heart. Trends Cardiovasc. Med. 2020, 30, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Panagioti, M.; Scott, C.; Blakemore, A.; Coventry, P.A. Overview of the Prevalence, Impact, and Management of Depression and Anxiety in Chronic Obstructive Pulmonary Disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 1289–1306. [Google Scholar] [PubMed]
- Easton, K.; Coventry, P.; Lovell, K.; Carter, L.A.; Deaton, C. Prevalence and Measurement of Anxiety in Samples of Patients with Heart Failure. J. Cardiovasc. Nurs. 2016, 31, 367–379. [Google Scholar] [CrossRef]
- Kunik, M.E.; Roundy, K.; Veazey, C.; Souchek, J.; Richardson, P.; Wray, N.P.; Stanley, M.A. Surprisingly High Prevalence of Anxiety and Depression in Chronic Breathing Disorders. Chest 2005, 127, 1205–1211. [Google Scholar] [CrossRef]
- Willgoss, T.G.; Yohannes, A.M. Anxiety Disorders in Patients with COPD: A Systematic Review. Respir. Care 2013, 58, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.W.B.; Ho, R.C.M.; Cheung, M.W.L.; Fu, E.; Mak, A. Prevalence of Depressive Symptoms in Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review, Meta-Analysis and Meta-Regression. Gen. Hosp. Psychiatry 2011, 33, 217–223. [Google Scholar] [CrossRef]
- Alva, M.L. Co-Occurrence of Diabetes and Depression in the U.S. PLoS ONE 2020, 15, 1–10. [Google Scholar] [CrossRef]
- Mosaku, K.; Kolawole, B.; Mume, C.; Ikem, R. Depression, Anxiety and Quality of Life among Diabetic Patients: A Comparative Study. J. Natl. Med. Assoc. 2008, 100, 73–78. [Google Scholar] [CrossRef]
- Glick, G.; Druss, B.; Pina, J.; Lally, C.; Conde, M. Use of Mobile Technology in a Community Mental Health Setting. J. Telemed. Telecare 2016, 22, 430–435. [Google Scholar] [CrossRef]
- Prince, M.; Patel, V.; Saxena, S.; Maj, M.; Maselko, J.; Phillips, M.R.; Rahman, A. Global Mental Health 1—No Health without Mental Health. Lancet 2007, 370, 859–877. [Google Scholar] [CrossRef]
- Mechael, P.; Batavia, H.; Kaonga, N.; Searle, S.; Kwan, A.; Goldberger, A.; Fu, J.; Ossman, J. Barriers and Gaps Affecting Mhealth in Low- and Middle-Income Countries: Policy White Paper; MHealth Alliance: Washington, DC, USA, 2010. [Google Scholar]
- Kruse, C.S.; Soma, M.; Pulluri, D.; Nemali, N.T.; Brooks, M. The Effectiveness of Telemedicine in the Management of Chronic Heart Disease—A Systematic Review. JRSM Open 2017, 8, 205427041668174. [Google Scholar] [CrossRef] [PubMed]
- Meskó, B.; Drobni, Z.; Bényei, É.; Gergely, B.; Győrffy, Z. Digital Health Is a Cultural Transformation of Traditional Healthcare. mHealth 2017, 3, 38. [Google Scholar] [CrossRef] [PubMed]
- Ahmadvand, A.; Gatchel, R.; Brownstein, J.; Nissen, L. The Biopsychosocial-Digital Approach to Health and Disease: Call for a Paradigm Expansion. J. Med. Internet Res. 2018, 20, e189. [Google Scholar] [CrossRef] [PubMed]
- Matamala-Gomez, M.; Maisto, M.; Montana, J.I.; Mavrodiev, P.A.; Baglio, F.; Rossetto, F.; Mantovani, F.; Riva, G.; Realdon, O. The Role of Engagement in Teleneurorehabilitation: A Systematic Review. Front. Neurol. 2020, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Nittari, G.; Khuman, R.; Baldoni, S.; Pallotta, G.; Battineni, G.; Sirignano, A.; Amenta, F.; Ricci, G. Telemedicine Practice: Review of the Current Ethical and Legal Challenges. Telemed. E Health 2020, 26, 1427–1437. [Google Scholar] [CrossRef] [PubMed]
- Hamine, S.; Gerth-Guyette, E.; Faulx, D.; Green, B.B.; Ginsburg, A.S. Impact of MHealth Chronic Disease Management on Treatment Adherence and Patient Outcomes: A Systematic Review. J. Med. Internet Res. 2015, 17, e52. [Google Scholar] [CrossRef]
- Park, Y.T. Emerging New Era of Mobile Health Technologies. Healthc. Inform. Res. 2016, 253–254. [Google Scholar] [CrossRef]
- Fiordelli, M.; Diviani, N.; Schulz, P.J. Mapping Mhealth Research: A Decade of Evolution. J. Med. Internet Res. 2013. [Google Scholar] [CrossRef]
- Cavalera, C.; Pepe, A.; Zurloni, V.; Diana, B.; Realdon, O. A Short Version of the State Shame and Guilt Scale (SSGS-8). TPM Test. Psychom. Methodol. Appl. Psychol. 2017, 24, 99–106. [Google Scholar] [CrossRef]
- Riva, E.; Freire, T.; Bassi, M. The Flow Experience in Clinical Settings: Applications in Psychotherapy and Mental Health Rehabilitation. In Flow Experience; Harmat, L., Ørstead Andersen, F., Ullén, F., Wright, J., Sadlo, G., Eds.; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Timpel, P.; Oswald, S.; Schwarz, P.E.H.; Harst, L. Mapping the Evidence on the Effectiveness of Telemedicine Interventions in Diabetes, Dyslipidemia and Hypertension: An Umbrella Review of Systematic Reviews and Meta-Analyses. J. Med. Internet Res. 2020, 22, e16791. [Google Scholar] [CrossRef]
- Bertoncello, C.; Cocchio, S.; Fonzo, M.; Bennici, S.E.; Russo, F.; Putoto, G. The Potential of Mobile Health Clinics in Chronic Disease Prevention and Health Promotion in Universal Healthcare Systems. An on-Field Experiment. Int. J. Equity Health 2020, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Debon, R.; Coleone, J.D.; Bellei, E.A.; De Marchi, A.C.B. Mobile Health Applications for Chronic Diseases: A Systematic Review of Features for Lifestyle Improvement. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2507–2512. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllidis, A.; Kondylakis, H.; Votis, K.; Tzovaras, D.; Maglaveras, N.; Rahimi, K. Features, Outcomes and Challenges in Mobile Health Interventions for Patients Living with Chronic Diseases: A Review of Systematic Reviews. Int. J. Med. Inform. 2019, 132, 103984. [Google Scholar] [CrossRef] [PubMed]
- Gandapur, Y.; Kianoush, S.; Kelli, H.M.; Misra, S.; Urrea, B.; Blaha, M.J.; Graham, G.; Marvel, F.A.; Martin, S.S. The Role of MHealth for Improving Medication Adherence in Patients with Cardiovascular Disease: A Systematic Review. Eur. Heart J. Qual. Care Clin. Outcomes 2016, 2, 237–244. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, M.; Kim, J.; Jing, Y.; Khadra, M.; Nanan, R. A Systematic Review on Incentive-Driven Mobile Health Technology: As Used in Diabetes Management. J. Telemed. Telecare 2017, 23, 26–35. [Google Scholar] [CrossRef]
- Cui, M.; Wu, X.; Mao, J.; Wang, X.; Nie, M. T2DM Self-Management via Smartphone Applications: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0166718. [Google Scholar] [CrossRef]
- Sieverdes, J.C.; Treiber, F.; Jenkins, C. Improving Diabetes Management with Mobile Health Technology. Am. J. Med. Sci. 2013, 345, 289–295. [Google Scholar] [CrossRef]
- Cichosz, S.L.; Udsen, F.W.; Hejlesen, O. The Impact of Telehealth Care on Health-Related Quality of Life of Patients with Heart Failure: Results from the Danish TeleCare North Heart Failure Trial. J. Telemed. Telecare 2020, 26, 452–461. [Google Scholar] [CrossRef]
- Whitehead, L.; Seaton, P. The Effectiveness of Self-Management Mobile Phone and Tablet Apps in Long-Term Condition Management: A Systematic Review. J. Med. Internet Res. 2016. [Google Scholar] [CrossRef]
- Sirina Keesara, M.D.; Andrea Jonas, M.D.; Kevin Schulman, M. Covid-19 and Health Care’s Digital Revolution. N. Engl. J. Med. 2020, 382, 1–2. [Google Scholar] [CrossRef]
- Kyu, H.H.; Abate, D.; Abate, K.H. Global, Regional and National Disability-Adjusted Life-Years (DALYs) for 359 Diseases and Injuries and Healthy Life Expectancy (HALE) for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R. Meta-Analytic Procedures for Social Science Research Sage Publications: Beverly Hills, 1984, 148p. Educ. Res. 1986, 15, 18–20. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Islam, S.M.S.; Chow, C.K.; Redfern, J.; Kok, C.; Radholm, K.; Stepien, S.; Rodgers, A.; Hackett, M.L. Effect of Text Messaging on Depression in Patients with Coronary Heart Disease: A Substudy Analysis from the TEXT ME Randomised Controlled Trial. BMJ Open 2019, 9, e022637. [Google Scholar] [CrossRef]
- Johansson, P.; Westas, M.; Andersson, G.; Alehagen, U.; Broström, A.; Jaarsma, T.; Mourad, G.; Lundgren, J. An Internet-Based Cognitive Behavioral Therapy Program Adapted to Patients with Cardiovascular Disease and Depression: Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, 1–14. [Google Scholar] [CrossRef]
- Clarke, J.; Sanatkar, S.; Baldwin, P.A.; Fletcher, S.; Gunn, J.; Wilhelm, K.; Campbell, L.; Zwar, N.; Harris, M.; Lapsley, H.; et al. A Web-Based Cognitive Behavior Therapy Intervention to Improve Social and Occupational Functioning in Adults with Type 2 Diabetes (The SpringboarD Trial): Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, e12246. [Google Scholar] [CrossRef]
- Schlicker, S.; Weisel, K.K.; Buntrock, C.; Berking, M.; Nobis, S.; Lehr, D.; Baumeister, H.; Snoek, F.J.; Riper, H.; Ebert, D.D. Do Nonsuicidal Severely Depressed Individuals with Diabetes Profit from Internet-Based Guided Self-Help? Secondary Analyses of a Pragmatic Randomized Trial. J. Diabetes Res. 2019. [Google Scholar] [CrossRef]
- Vloothuis, J.D.M.; Mulder, M.; Nijland, R.H.M.; Goedhart, Q.S.; Konijnenbelt, M.; Mulder, H.; Hertogh, C.M.P.M.; van Tulder, M.; van Wegen, E.E.H.; Kwakkel, G. Caregiver-Mediated Exercises with e-Health Support for Early Supported Discharge after Stroke (CARE4STROKE): A Randomized Controlled Trial. PLoS ONE 2019, 14, e0214241. [Google Scholar] [CrossRef]
- Doyle, C.; Bhar, S.; Fearn, M.; Ames, D.; Osborne, D.; You, E.; Gorelik, A.; Dunt, D. The Impact of Telephone-Delivered Cognitive Behaviour Therapy and Befriending on Mood Disorders in People with Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Br. J. Health Psychol. 2017, 22, 542–556. [Google Scholar] [CrossRef] [PubMed]
- Egede, L.E.; Walker, R.J.; Payne, E.H.; Knapp, R.G.; Acierno, R.; Frueh, B.C. Effect of Psychotherapy for Depression via Home Telehealth on Glycemic Control in Adults with Type 2 Diabetes: Subgroup Analysis of a Randomized Clinical Trial. J. Telemed. Telecare 2017, 24, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Nobis, S.; Lehr, D.; Baumeister, H.; Riper, H.; Auerbach, R.P.; Snoek, F.; Cuijpers, P.; Berking, M. The 6-Month Effectiveness of Internet-Based Guided Self-Help for Depression in Adults with Type 1 and 2 Diabetes Mellitus. Diabet. Med. 2017, 34, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.D.; Hundt, N.E.; Vaughan, E.M.; Petersen, N.J.; Zeno, D.; Kunik, M.E.; Cully, J.A. Effect of Telephone-Delivered Collaborative Goal Setting and Behavioral Activation vs Enhanced Usual Care for Depression among Adults with Uncontrolled Diabetes: A Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e198634. [Google Scholar] [CrossRef] [PubMed]
- Wayne, N.; Perez, D.F.; Kaplan, D.M.; Ritvo, P. Health Coaching Reduces HbA1c in Type 2 Diabetic Patients From a Lower-Socioeconomic Status Community: A Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e224. [Google Scholar] [CrossRef] [PubMed]
- Glozier, N.; Christensen, H.; Naismith, S.; Cockayne, N.; Donkin, L.; Neal, B.; Mackinnon, A.; Hickie, I. Internet-Delivered Cognitive Behavioural Therapy for Adults with Mild to Moderate Depression and High Cardiovascular Disease Risks: A Randomised Attention-Controlled Trial. PLoS ONE 2013, 8, e59139. [Google Scholar] [CrossRef]
- van Bastelaar, K.M.P.; Pouwer, F.; Cuijpers, P.; Riper, H.; Snoek, F.J. Web-Based Depression Treatment for Type 1 and Type 2 Diabetic Patients A Randomized, Controlled Trial. Diabetes Care 2011, 34, 320–325. [Google Scholar] [CrossRef]
- Bond, G.E.; Burr, R.L.; Wolf, F.M.; Feldt, K. The Effects of a Web-Based Intervention on Psychosocial Well-Being among Adults Aged 60 and Older with Diabetes A Randomized Trial. Diabetes Educ. 2010, 36, 446–456. [Google Scholar] [CrossRef]
- Lewis, K.E.; Annandale, J.A.; Warm, D.L.; Hurlin, C.; Lewis, M.J.; Lewis, L. Home Telemonitoring and Quality of Life in Stable, Optimised Chronic Obstructive Pulmonary Disease. J. Telemed. Telecare 2010, 16, 253–259. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, 1–8. [Google Scholar] [CrossRef]
- Baron, J.S.; Hirani, S.; Newman, S.P. A Randomised, Controlled Trial of the Effects of a Mobile Telehealth Intervention on Clinical and Patient-Reported Outcomes in People with Poorly Controlled Diabetes. J. Telemed. Telecare 2016, 23, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Antypas, K.; Wangberg, S.C. An Internet- and Mobile-Based Tailored Intervention to Enhance Maintenance of Physical Activity after Cardiac Rehabilitation: Short-Term Results of a Randomized Controlled Trial. J. Med. Internet Res. 2014, 16, e77. [Google Scholar] [CrossRef] [PubMed]
- Pinnock, H.; Hanley, J.; McCloughan, L.; Todd, A.; Krishan, A.; Lewis, S.; Stoddart, A.; van der Pol, M.; MacNee, W.; Sheikh, A.; et al. Effectiveness of Telemonitoring Integrated into Existing Clinical Services on Hospital Admission for Exacerbation of Chronic Obstructive Pulmonary Disease: Researcher Blind, Multicentre, Randomised Controlled Trial. BMJ Br. Med. J. 2013, 347, 16070. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, D.A.; Gee, P.M.; Fatkin, K.J.; Peeples, M. A Systematic Review of Reviews Evaluating Technology-Enabled Diabetes Self-Management Education and Support. J. Diabetes Sci. Technol. 2017, 11, 1015–1027. [Google Scholar] [CrossRef]
- Di Tella, S.; Pagliari, C.; Blasi, V.; Mendozzi, L.; Rovaris, M.; Baglio, F. Integrated Telerehabilitation Approach in Multiple Sclerosis: A Systematic Review and Meta-Analysis. J. Telemed. Telecare 2019, 26, 385–399. [Google Scholar] [CrossRef]
- Isernia, S.; Pagliari, C.; Jonsdottir, J.; Castiglioni, C.; Gindri, P.; Gramigna, C.; Palumbo, G.; Salza, M.; Molteni, F.; Baglio, F. Efficiency and Patient-Reported Outcome Measures from Clinic to Home: The Human Empowerment Aging and Disability Program for Digital-Health Rehabilitation. Front. Neurol. 2019, 10, 1–13. [Google Scholar] [CrossRef]
- Riva, G.; Baños, R.M.; Botella, C.; Wiederhold, B.K.; Gaggioli, A. Positive Technology: Using Interactive Technologies to Promote Positive Functioning. Cyberpsychol. Behav. Soc. Netw. 2012, 15, 69–77. [Google Scholar] [CrossRef]
- Realdon, O.; Rossetto, F.; Nalin, M.; Baroni, I.; Romano, M.; Catania, F.; Frontini, D.; Mancastroppa, S.; Alberoni, M.; Zurloni, V.; et al. The Technology-Enhanced Ability Continuum-of-Care Home Program for People with Cognitive Disorders: Concept Design and Scenario of Use. In Pervasive Computing Paradigms for Mental Health. MindCare 2018. Lecture Notes of the Institute for Computer Sciences, Social Informatics and Telecommunications Engineering; Cipresso, P., Serino, S., Ostrovsky, Y., Baker, J., Eds.; Springer: Cham, Switzerland, 2018; pp. 64–73. [Google Scholar]
- Nicholas, J.; Ringland, K.E.; Graham, A.K.; Knapp, A.A.; Lattie, E.G.; Kwasny, M.J.; Mohr, D.C. Stepping Up: Predictors of “Stepping” within an ICBT Stepped-Care Intervention for Depression. Int. J. Environ. Res. Public Health 2019, 16, 4689. [Google Scholar] [CrossRef]
- Thase, M.E.; McCrone, P.; Barrett, M.S.; Eells, T.D.; Wisniewski, S.R.; Balasubramani, G.K.; Brown, G.K.; Wright, J.H. Improving Cost-Effectiveness and Access to Cognitive Behavior Therapy for Depression: Providing Remote-Ready, Computer-Assisted Psychotherapy in Times of Crisis and Beyond. Psychother. Psychosom. 2020, 89, 307–313. [Google Scholar] [CrossRef]
- Dobkin, R.D.; Mann, S.L.; Gara, M.A.; Interian, A.; Rodriguez, K.M.; Menza, M. Telephone-Based Cognitive Behavioral Therapy for Depression in Parkinson Disease: A Randomized Controlled Trial. Neurology 2020, 94, E1764–E1773. [Google Scholar] [CrossRef]
- Mohr, D.C.; Ho, J.; Duffecy, J.; Reifler, D.; Sokol, L.; Burns, M.N.; Jin, L.; Siddique, J. Effect of Telephone-Administered vs Face-to-Face Cognitive Behavioral Therapy on Adherence to Therapy and Depression Outcomes among Primary Care Patients: A Randomized Trial. JAMA J. Am. Med. Assoc. 2012, 307, 2278–2285. [Google Scholar] [CrossRef] [PubMed]
- Irvine, A.; Drew, P.; Bower, P.; Brooks, H.; Gellatly, J.; Armitage, C.J.; Barkham, M.; McMillan, D.; Bee, P. Are There Interactional Differences between Telephone and Face-to-Face Psychological Therapy? A Systematic Review of Comparative Studies. J. Affect. Disord. 2020, 265, 120–131. [Google Scholar] [CrossRef]
- Stowell, E.; Lyson, M.C.; Saksono, H.; Wurth, R.C.; Jimison, H.; Pavel, M.; Parker, A.G. Designing and Evaluating MHealth Interventions for Vulnerable Populations: A Systematic Review. Conf. Hum. Factors Comput. Syst. Proc. 2018, 2018, 1–17. [Google Scholar] [CrossRef]
- Jimison, H.; Gorman, P.; Woods, S.; Nygren, P.; Walker, M.; Norris, S.; Hersh, W. Barriers and Drivers of Health Information Technology Use for the Elderly, Chronically Ill and Underserved. Evid. Rep. Technol. Assess. (Full. Rep.) 2008, 175, 1–1422. [Google Scholar]
- Cheng, Z.J.; Shan, J. 2019 Novel Coronavirus: Where We Are and What We Know. Infection 2020, 48, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Azarpazhooh, M.R.; Morovatdar, N.; Avan, A.; Phan, T.G.; Divani, A.A.; Yassi, N.; Stranges, S.; Silver, B.; Biller, J.; Tokazebani Belasi, M.; et al. COVID-19 pandemic and burden of non-communicable diseases: An ecological study on data of 185 countries. J. Stroke Cerebrovasc. Dis. 2020, 29, 105089. [Google Scholar] [CrossRef]
- He, F.; Deng, Y.; Li, W. Coronavirus Disease 2019: What We Know? J. Med. Virol. 2020, 92, 719–725. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Carin, L.; Dzau, V.; Wong, T.Y. Digital Technology and COVID-19. Nat. Med. 2020, 26, 459–461. [Google Scholar] [CrossRef]
- Robb, C.E.; de Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of Social Isolation with Anxiety and Depression During the Early COVID-19 Pandemic: A Survey of Older Adults in London, UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef]
- Ohannessian, R.; Duong, T.A.; Odone, A. Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action. JMIR Public Health Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef]
- WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening; World Health Organization: Geneva, Switzerlands, 2019; Licence: CC BY-NC-SA 3.0 IGO.
- Tuckson, R.V.; Edmunds, M.; Hodgkins, M.L. Telehealth. N. Engl. J. Med. 2017, 377, 1585–1592. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maisto, M.; Diana, B.; Di Tella, S.; Matamala-Gomez, M.; Montana, J.I.; Rossetto, F.; Mavrodiev, P.A.; Cavalera, C.; Blasi, V.; Mantovani, F.; et al. Digital Interventions for Psychological Comorbidities in Chronic Diseases—A Systematic Review. J. Pers. Med. 2021, 11, 30. https://doi.org/10.3390/jpm11010030
Maisto M, Diana B, Di Tella S, Matamala-Gomez M, Montana JI, Rossetto F, Mavrodiev PA, Cavalera C, Blasi V, Mantovani F, et al. Digital Interventions for Psychological Comorbidities in Chronic Diseases—A Systematic Review. Journal of Personalized Medicine. 2021; 11(1):30. https://doi.org/10.3390/jpm11010030
Chicago/Turabian StyleMaisto, Marta, Barbara Diana, Sonia Di Tella, Marta Matamala-Gomez, Jessica Isbely Montana, Federica Rossetto, Petar Aleksandrov Mavrodiev, Cesare Cavalera, Valeria Blasi, Fabrizia Mantovani, and et al. 2021. "Digital Interventions for Psychological Comorbidities in Chronic Diseases—A Systematic Review" Journal of Personalized Medicine 11, no. 1: 30. https://doi.org/10.3390/jpm11010030
APA StyleMaisto, M., Diana, B., Di Tella, S., Matamala-Gomez, M., Montana, J. I., Rossetto, F., Mavrodiev, P. A., Cavalera, C., Blasi, V., Mantovani, F., Baglio, F., & Realdon, O. (2021). Digital Interventions for Psychological Comorbidities in Chronic Diseases—A Systematic Review. Journal of Personalized Medicine, 11(1), 30. https://doi.org/10.3390/jpm11010030