Relative Biological Effectiveness of Carbon Ions for Head-and-Neck Squamous Cell Carcinomas According to Human Papillomavirus Status

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Line and Cell Culture
2.2. Clonogenic Assays
2.3. Irradiation
2.4. Statistics
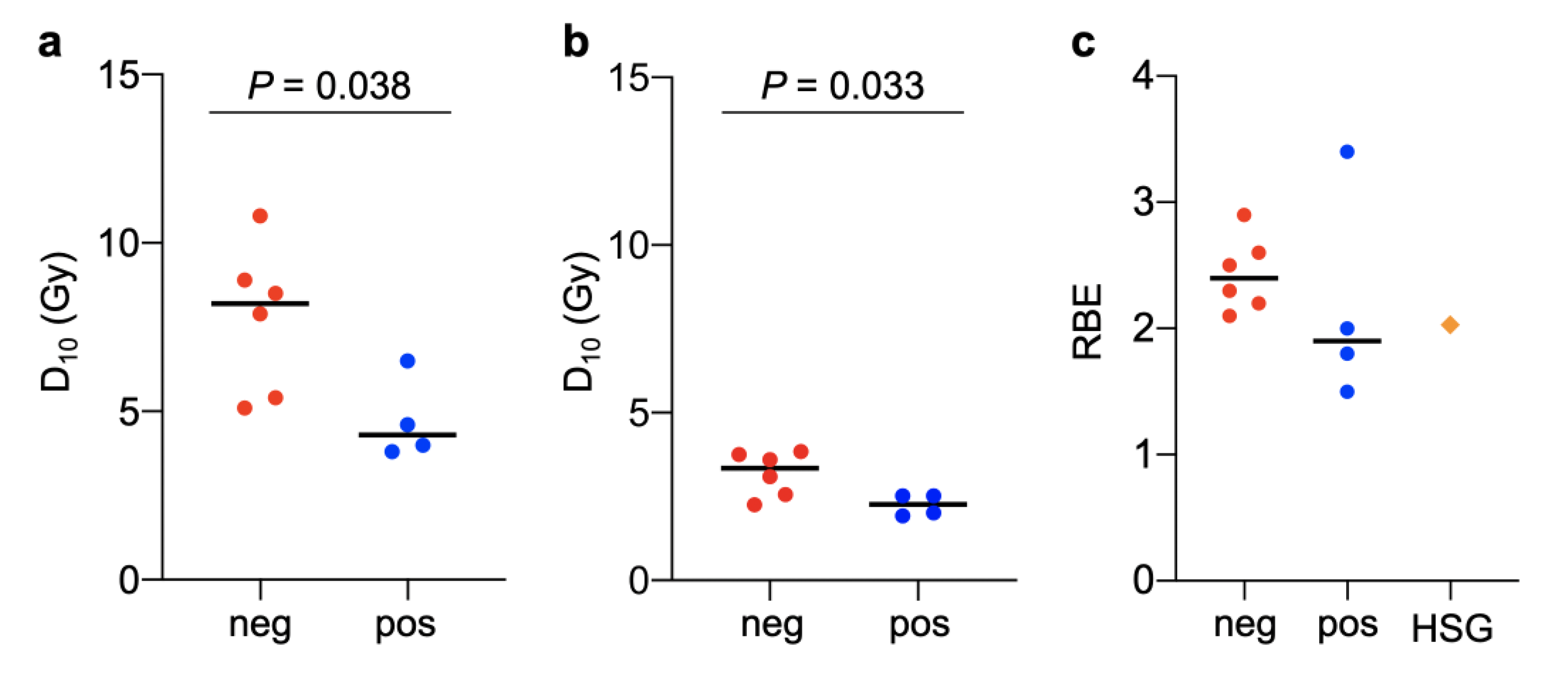
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schlaff, C.D.; Krauze, A.; Belard, A.; O’Connell, J.J.; Camphausen, K.A. Bringing the heavy: Carbon ion therapy in the radiobiological and clinical context. Radiat. Oncol. 2014, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Loeffler, J.S.; Durante, M. Charged particle therapy-optimization, challenges and future directions. Nat. Rev. Clin. Oncol. 2013, 10, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Pauli, C.; Hopkins, B.D.; Prandi, D.; Shaw, R.; Fedrizzi, T.; Sboner, A.; Sailer, V.; Augello, M.; Puca, L.; Rosati, R.; et al. Personalized In Vitro and In Vivo Cancer Models to Guide Precision Medicine. Cancer Discov. 2017, 7, 462–477. [Google Scholar] [CrossRef] [PubMed]
- Amornwichet, N.; Oike, T.; Shibata, A.; Nirodi, C.S.; Ogiwara, H.; Makino, H.; Kimura, Y.; Hirota, Y.; Isono, M.; Yoshida, Y.; et al. The EGFR mutation status affects the relative biological effectiveness of carbon-ion beams in non-small cell lung carcinoma cells. Sci. Rep. 2015, 5, 11305. [Google Scholar] [CrossRef]
- Yagishita, S.; Horinouchi, H.; Katsui Taniyama, T.; Nakamichi, S.; Kitazono, S.; Mizugaki, H.; Kanda, S.; Fujiwara, Y.; Nokihara, H.; Yamamoto, N.; et al. Epidermal growth factor receptor mutation is associated with longer local control after definitive chemoradiotherapy in patients with stage III nonsquamous non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 140–148. [Google Scholar] [CrossRef]
- Torres-Roca, J.F. A molecular assay of tumor radiosensitivity: A roadmap towards biology-based personalized radiation therapy. Pers. Med. 2012, 9, 547–557. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef]
- Mirghani, H.; Amen, F.; Tao, Y.; Deutsch, E.; Levy, A. Increased radiosensitivity of HPV-positive head and neck cancers: Molecular basis and therapeutic perspectives. Cancer Treat. Rev. 2015, 41, 844–852. [Google Scholar] [CrossRef]
- Friedrich, T.; Scholz, U.; Elsässer, T.; Durante, M.; Scholz, M. Systematic analysis of RBE and related quantities using a database of cell survival experiments with ion beam irradiation. J. Radiat. Res. 2013, 54, 494–514. [Google Scholar] [CrossRef]
- Olthof, N.C.; Huebbers, C.U.; Kolligs, J.; Henfling, M.; Ramaekers, F.C.; Cornet, I.; van Lent-Albrechts, J.A.; Stegmann, A.P.; Silling, S.; Wieland, U.; et al. Viral load, gene expression and mapping of viral integration sites in HPV16-associated HNSCC cell lines. Int. J. Cancer 2015, 136, E207–E218. [Google Scholar] [CrossRef]
- Brenner, J.C.; Graham, M.P.; Kumar, B.; Saunders, L.M.; Kupfer, R.; Lyons, R.H.; Bradford, C.R.; Carey, T.E. Genotyping of 73 UM-SCC head and neck squamous cell carcinoma cell lines. Head Neck 2010, 32, 417–426. [Google Scholar] [CrossRef] [PubMed]
- St. John, L.S.; Sauter, E.R.; Herlyn, M.; Litwin, S.; Adler-Storthz, K. Endogenous p53 gene status predicts the response of human squamous cell carcinomas to wild-type p53. Cancer Gene Ther. 2000, 7, 749–756. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nichols, A.C.; Yoo, J.; Palma, D.A.; Fung, K.; Franklin, J.H.; Koropatnick, J.; Mymryk, J.S.; Batada, N.N.; Barrett, J.W. Frequent mutations in TP53 and CDKN2A found by next-generation sequencing of head and neck cancer cell lines. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 732–739. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cooper, T.; Biron, V.L.; Fast, D.; Tam, R.; Carey, T.; Shmulevitz, M.; Seikaly, H. Oncolytic activity of reovirus in HPV positive and negative head and neck squamous cell carcinoma. J. Otolaryngol. Head Neck Surg. 2015, 44, 8. [Google Scholar] [CrossRef]
- Kanai, T.; Endo, M.; Minohara, S.; Miyahara, N.; Koyama-ito, H.; Tomura, H.; Matsufuji, N.; Futami, Y.; Fukumura, A.; Hiraoka, T.; et al. Biophysical characteristics of HIMAC clinical irradiation system for heavy-ion radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 201–210. [Google Scholar] [CrossRef]
- Anakura, M.; Nachankar, A.; Kobayashi, D.; Amornwichet, N.; Hirota, Y.; Shibata, A.; Oike, T.; Nakano, T. Radiosensitivity Differences between EGFR Mutant and Wild-Type Lung Cancer Cells are Larger at Lower Doses. Int. J. Mol. Sci. 2019, 20, 3635. [Google Scholar] [CrossRef]
- Oike, T.; Ogiwara, H.; Torikai, K.; Nakano, T.; Yokota, J.; Kohno, T. Garcinol, a histone acetyltransferase inhibitor, radiosensitizes cancer cells by inhibiting non-homologous end joining. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 815–821. [Google Scholar] [CrossRef]
- Kagawa, K.; Murakami, M.; Hishikawa, Y.; Abe, M.; Akagi, T.; Yanou, T.; Kagiya, G.; Furusawa, Y.; Ando, K.; Nojima, K.; et al. Preclinical biological assessment of proton and carbon ion beams at Hyogo Ion Beam Medical Center. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 928–938. [Google Scholar] [CrossRef]
- Yoshida, Y.; Musha, A.; Kawamura, H.; Kanai, T.; Takahashi, T. Biology research. In Annual Report for Fiscal Year 2009–2011; Gunma University Heavy Ion Medical Center, Ed.; Gunma University Heavy Ion Medical Center: Maebashi, Japan, 2013; pp. 83–84. [Google Scholar]
- Mizoe, J.E.; Hasegawa, A.; Jingu, K.; Takagi, R.; Bessyo, H.; Morikawa, T.; Tonoki, M.; Tsuji, H.; Kamada, T.; Tsujii, H.; et al. Results of carbon ion radiotherapy for head and neck cancer. Radiother. Oncol. 2012, 103, 32–37. [Google Scholar] [CrossRef]
- Wang, H.; Wang, X.; Zhang, P.; Wang, Y. The Ku-dependent non-homologous end-joining but not other repair pathway is inhibited by high linear energy transfer ionizing radiation. DNA Repair (Amst) 2008, 7, 725–733. [Google Scholar] [CrossRef]
- Tang, A.L.; Hauff, S.J.; Owen, J.H.; Graham, M.P.; Czerwinski, M.J.; Park, J.J.; Walline, H.; Papagerakis, S.; Stoerker, J.; McHugh, J.B.; et al. UM-SCC-104: A new human papillomavirus-16-positive cancer stem cell-containing head and neck squamous cell carcinoma cell line. Head Neck 2012, 34, 1480–1491. [Google Scholar] [CrossRef]
- Das, A.K.; Chen, B.P.; Story, M.D.; Sato, M.; Minna, J.D.; Chen, D.J.; Nirodi, C.S. Somatic mutations in the tyrosine kinase domain of epidermal growth factor receptor (EGFR) abrogate EGFR-mediated radioprotection in non-small cell lung carcinoma. Cancer Res. 2007, 67, 5267–5274. [Google Scholar] [CrossRef]
- Martin, D.; Abba, M.C.; Molinolo, A.A.; Vitale-Cross, L.; Wang, Z.; Zaida, M.; Delic, N.C.; Samuels, Y.; Lyons, J.G.; Gutkind, J.S. The head and neck cancer cell oncogenome: A platform for the development of precision molecular therapies. Oncotarget 2014, 5, 8906–8923. [Google Scholar] [CrossRef]
- Telmer, C.A.; An, J.; Malehorn, D.E.; Zeng, X.; Gollin, S.M.; Ishwad, C.S.; Jarvik, J.W. Detection and assignment of TP53 mutations in tumor DNA using peptide mass signature genotyping. Hum. Mutat. 2003, 22, 158–165. [Google Scholar] [CrossRef]
- Tanaka, N.; Zhao, M.; Tang, L.; Patel, A.A.; Xi, Q.; Van, H.T.; Takahashi, H.; Osman, A.A.; Zhang, J.; Wang, J.; et al. Gain-of-function mutant p53 promotes the oncogenic potential of head and neck squamous cell carcinoma cells by targeting the transcription factors FOXO3a and FOXM1. Oncogene 2018, 37, 1279–1292. [Google Scholar] [CrossRef]
- Amornwichet, N.; Oike, T.; Shibata, A.; Ogiwara, H.; Tsuchiya, N.; Yamauchi, M.; Saitoh, Y.; Sekine, R.; Isono, M.; Yoshida, Y.; et al. Carbon-ion beam irradiation kills X-ray-resistant p53-null cancer cells by inducing mitotic catastrophe. PLoS ONE 2014, 9, e115121. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Cell Line | HPV Status | Origin | Reference |
|---|---|---|---|
| UD-SCC-2 | Positive | Pharynx | [10] |
| UM-SCC-47 | Positive | Tongue | [11] |
| UM-SCC-104 | Positive | Oral cavity | [10] |
| UPCI:SCC154 | Positive | Tongue | [10] |
| A-253 | Negative | Salivary gland | [12] |
| Detroit 562 | Negative | Pharynx | [13] |
| FaDu | Negative | Pharynx | [13] |
| SCC-9 | Negative | Tongue | [14] |
| SCC-25 | Negative | Tongue | [13] |
| UM-SCC-1 | Negative | Oral cavity | [11] |
| Cell Line | HPV Status | D10-X (Gy) | D10-C (Gy) | RBE |
|---|---|---|---|---|
| UD-SCC-2 | Positive | 4.58 | 2.52 | 1.81 |
| UM-SCC-47 | Positive | 3.98 | 2.01 | 1.98 |
| UM-SCC-104 | Positive | 6.52 | 1.92 | 3.38 |
| UPCI:SCC154 | Positive | 3.80 | 2.52 | 1.50 |
| A-253 | Negative | 5.40 | 2.56 | 2.10 |
| Detroit 562 | Negative | 8.48 | 3.84 | 2.20 |
| FaDu | Negative | 8.85 | 3.60 | 2.45 |
| SCC-9 | Negative | 10.83 | 3.75 | 2.88 |
| SCC-25 | Negative | 5.06 | 2.25 | 2.25 |
| UM-SCC-1 | Negative | 7.90 | 3.09 | 2.56 |
| Cell Line | TP53 | Reference |
|---|---|---|
| UD-SCC-2 | wild-type | [24] |
| UM-SCC-47 | wild-type | [24] |
| UM-SCC-104 | wild-type | [22] |
| UPCI:SCC154 | wild-type | [25] |
| A-253 | mutant (deletion) | [12] |
| Detroit 562 | mutant (codon 248) | [12] |
| FaDu | mutant (codon 258) | [12] |
| SCC-9 | mutant (deletion) | [12] |
| SCC-25 | mutant (deletion) | [24] |
| UM-SCC-1 | mutant (splice site) | [26] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osu, N.; Kobayashi, D.; Shirai, K.; Musha, A.; Sato, H.; Hirota, Y.; Shibata, A.; Oike, T.; Ohno, T. Relative Biological Effectiveness of Carbon Ions for Head-and-Neck Squamous Cell Carcinomas According to Human Papillomavirus Status. J. Pers. Med. 2020, 10, 71. https://doi.org/10.3390/jpm10030071
Osu N, Kobayashi D, Shirai K, Musha A, Sato H, Hirota Y, Shibata A, Oike T, Ohno T. Relative Biological Effectiveness of Carbon Ions for Head-and-Neck Squamous Cell Carcinomas According to Human Papillomavirus Status. Journal of Personalized Medicine. 2020; 10(3):71. https://doi.org/10.3390/jpm10030071
Chicago/Turabian StyleOsu, Naoto, Daijiro Kobayashi, Katsuyuki Shirai, Atsushi Musha, Hiro Sato, Yuka Hirota, Atsushi Shibata, Takahiro Oike, and Tatsuya Ohno. 2020. "Relative Biological Effectiveness of Carbon Ions for Head-and-Neck Squamous Cell Carcinomas According to Human Papillomavirus Status" Journal of Personalized Medicine 10, no. 3: 71. https://doi.org/10.3390/jpm10030071
APA StyleOsu, N., Kobayashi, D., Shirai, K., Musha, A., Sato, H., Hirota, Y., Shibata, A., Oike, T., & Ohno, T. (2020). Relative Biological Effectiveness of Carbon Ions for Head-and-Neck Squamous Cell Carcinomas According to Human Papillomavirus Status. Journal of Personalized Medicine, 10(3), 71. https://doi.org/10.3390/jpm10030071