A Brief Questionnaire to Assess Post-Exertional Malaise

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. First-Step DSQ Items
2.2.2. Supplemental DSQ PEM Items
2.3. Statistics
3. Results
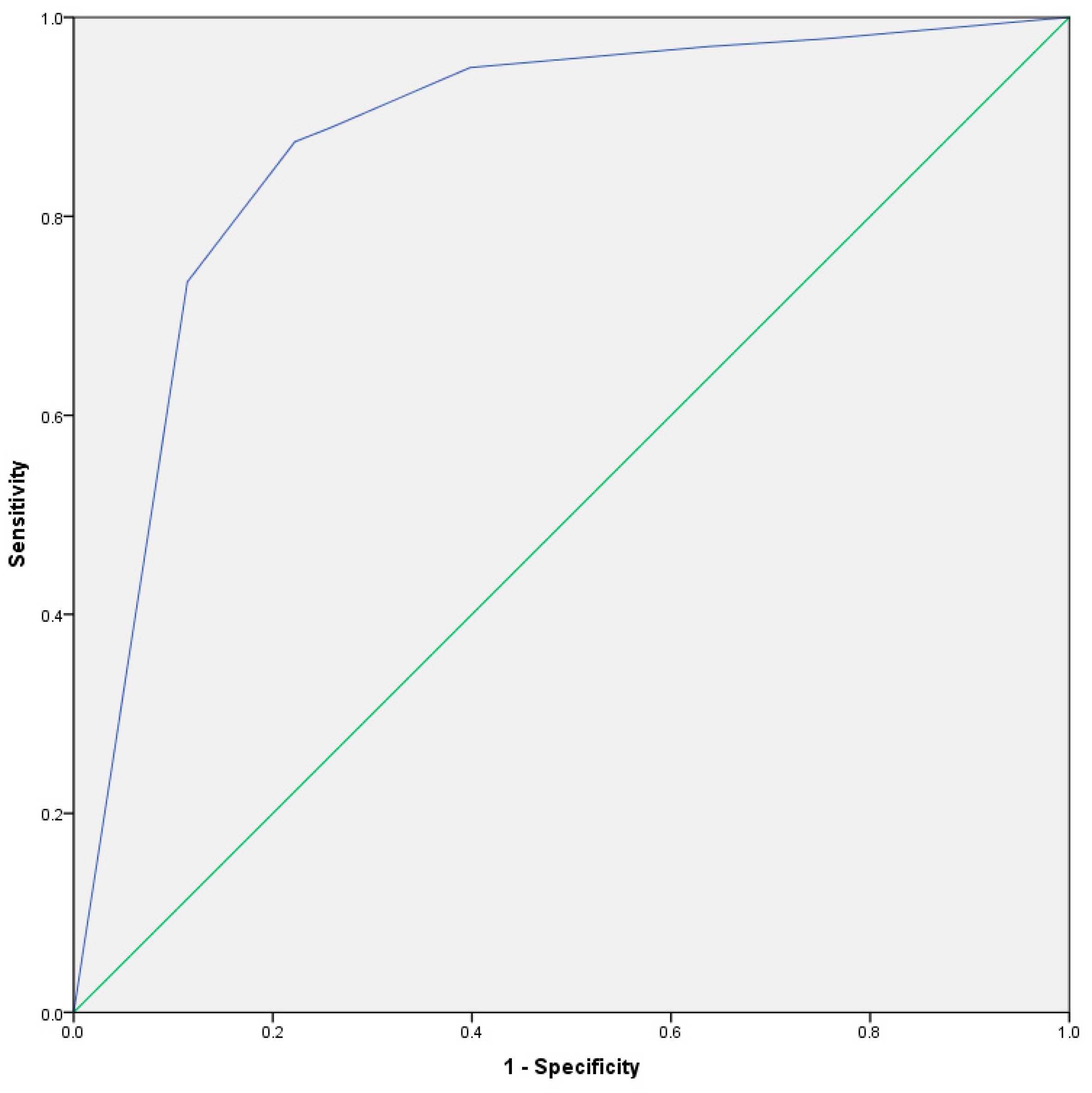
Receiver Operating Characteristic
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Symptoms | Frequency: Throughout the past 6 months, how often have you had this symptom? For each symptom listed below, circle a number from: 0 = none of the time 1 = a little of the time 2 = about half the time 3 = most of the time 4 = all of the time | Severity: Throughout the past 6 months, how much has this symptom bothered you? For each symptom listed below, circle a number from: 0 = symptom not present 1 = mild 2 = moderate 3 = severe 4= very severe |
| 1. Dead, heavy feeling after starting to exercise | 0 1 2 3 4 | 0 1 2 3 4 |
| 2. Next day soreness or fatigue after non-strenuous, everyday activities | 0 1 2 3 4 | 0 1 2 3 4 |
| 3. Mentally tired after the slightest effort | 0 1 2 3 4 | 0 1 2 3 4 |
| 4. Minimum exercise makes you physically tired | 0 1 2 3 4 | 0 1 2 3 4 |
| 5. Physically drained or sick after mild activity | 0 1 2 3 4 | 0 1 2 3 4 |
| 6. If you were to become exhausted after actively participating in extracurricular activities, sports, or outings with friends, would you recover within an hour or two after the activity ended? | Yes | No | ||||
| 7. Do you experience a worsening of your fatigue/energy related illness after engaging in minimal physical effort? | Yes | No | ||||
| 8. Do you experience a worsening of your fatigue/energy related illness after engaging in mental effort? | Yes | No | ||||
| 9. If you feel worse after activities, how long does this last? | <1 h | 2–3 h | 4–10 h | 11–13 h | 14–23 h | ≥ 24 h |
| 10. If you do not exercise, is it because exercise makes your symptoms worse? | Yes | No | ||||
Appendix B
- DSQ-PEM Scoring
- Scoring Step 1
- Items 1–5: A frequency and severity score of 2, 2 on any items 1–5 is indicative of PEM.
- Scoring Step 2
- Items 7, 8: Either item 7 or 8 must have an answer of yes to indicate an ME and/or CFS dx.
- Item 9: A response of >14 h is needed to indicate an ME and/or CFS dx.
- Items 6, 10: Neither item indicates an ME and/or CFS diagnosis, but provides a description of patient PEM for clinical evaluations.
References
- NIH/CDC PEM Working Group Full Definition of PEM. Patient Poll Material. Available online: https://onedrive.live.com/view.aspx?resid=DE9EBA00C8B2F963!6662&ithint=file%2cdocx&app=Word&authkey=!ABf7nbQU6qvJ43EActualworkinggroupdraftavailableat: https://web.archive.org/web/20180203213132/https://www.commondataelements.ninds.nih.gov/Doc/MECFS/04_PostExertional_Malaise_Subgroup_CDE_Draft_Recommendations.pdf (accessed on 1 August 2018).
- Carruthers, B.M.; Jain, A.K.; DeMeirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/chronic fatigue syndrome: Clinical working case definition, diagnostic and treatments protocols. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Jason, L.; Jessen, T.; Porter, N.; Boulton, A.; Gloria-Njoku, M.; Friedberg, F. Examining Types of Fatigue among Individuals with ME/CFS. Disabil. Stud. Q. 2009. [Google Scholar] [CrossRef]
- Jason, L.; Porter, N.; Shelleby, E.; Till, L.; Bell, D.S.; Lapp, C.W.; Meirleir, K.D. Severe versus Moderate Criteria for the New Pediatric Case Definition for ME/CFS. Child Psychiatry Hum. Dev. 2009, 40, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Furst, J.; Cid, M.; Farietta, J.; Strand, E.B. Factor Analysis of the DePaul Symptom Questionnaire: Identifying Core Domains. J. Neurol. Neurobiol. 2015. [Google Scholar] [CrossRef]
- Jason, L.A.; Evans, M.; Porter, N.; Brown, M.; Brown, A.; Hunnell, J.; Friedberg, F. The Development of a Revised Canadian Myalgic Encephalomyelitis Chronic Fatigue Syndrome Case Definition. Am. J. Biochem. Biotechnol. 2010, 6, 120–135. [Google Scholar] [CrossRef]
- Brown, A.A.; Jason, L.A. Validating a measure of myalgic encephalomyelitis/chronic fatigue syndrome symptomatology. Fatigue Biomed. Health Behav. 2014, 2, 132–152. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Mcmanimen, S.L.; Sunnquist, M.; Holtzman, C.S. Patient perceptions of post exertional malaise. Fatigue Biomed. Health Behav. 2018, 6, 92–105. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Evans, M.; So, S.; Scott, J.; Brown, A. Problems in Defining Post-Exertional Malaise. J. Prev. Interv. Community 2015, 43, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Deconstructing post-exertional malaise in myalgic encephalomyelitis/chronic fatigue syndrome: A patient-centered, cross-sectional survey. PLoS ONE 2018. [Google Scholar] [CrossRef] [PubMed]
- Harris, PA.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, Y.C.; Adamson, B.C.; Kinnett-Hopkins, D.; Bohri, M.; Motl, R.W. Results of a feasibility randomised controlled study of the guidelines for exercise in multiple sclerosis project. Contemp. Clin. Trials 2017, 54, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Oncu, J.; Durmaz, B.; Karapolat, H. Short-term effects of aerobic exercise on functional capacity, fatigue, and quality of life in patients with post-polio syndrome. Clin. Rehabil. 2009, 23, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Irving, G.; Neves, A.L.; Dambha-Miller, H.; Oishi, A.; Tagashira, H.; Verho, A.; Holden, J. International variations in primary care physician consultation time: A systematic review of 67 countries. BMJ Open 2017. [Google Scholar] [CrossRef] [PubMed]
- Twisk, F.N. Myalgic Encephalomyelitis, chronic fatigue syndrome, and Systemic Exertion Intolerance Disease: Three distinct clinical entities. Challenges 2018, 9, 19. [Google Scholar] [CrossRef]
- Sunnquist, M.; Jason, L.A.; Nehrke, P.; Goudsmit, E.M. A Comparison of Case Definitions for Myalgic Encephalomyelitis and Chronic Fatigue Syndrome. J. Chronic Dis. Manag. 2017, 2, 1013. [Google Scholar] [PubMed]
- Sotzny, F.; Blanco, J.; Capelli, E.; Castro-Marrero, J.; Steiner, S.; Murovska, M.; Scheibenbogen, C. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome—Evidence for an autoimmune disease. Autoimmun. Rev. 2018, 17, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Mcmanimen, S.; Sunnquist, M.; Newton, J.L.; Strand, E.B. Clinical criteria versus a possible research case definition in chronic fatigue syndrome/myalgic encephalomyelitis. Fatigue Biomed. Health Behav. 2017, 5, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Keller, B.A.; Pryor, J.; Giloteaux, L. Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO2peak indicates functional impairment. J. Transl. Med. 2014, 12. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, G.; Kolling, K. Reproducibility of cardiopulmonary exercise parameters in patients with valvular heart disease. Chest 1996, 110, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Name of Blue Advantage Policy: Cardiopulmonary Exercise Stress Test (CPET/CPX) (1 January 2010). BlueCross BlueShield of Alabama. Available online: https://providers.bcbsal.org/portal/documents/10226/1791629/Cardiopulmonary+Exercise+Stress+Test+%28CPET-CPX%29/0b3b358b-3b61-408e-9da3-d694f0a8399e?version=1.1 (accessed on 15 August 2018).
- Leclerc, K. Cardiopulmonary exercise testing: A contemporary and versatile clinical tool. Cleve. Clin. J. Med. 2017, 84, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Sunnquist, M. The development of the DePaul Symptom Questionnaire: Original, expanded, brief and pediatric versions. 2018, in press. [Google Scholar]

| Symptom | Tier 1 | Tier 2 | Tier 3 | Tier 4 |
|---|---|---|---|---|
| PEM duration | 100 | 2 | 10 | 0 |
| Mental Exacerbation | 0 | 38 | 17 | 0 |
| Exercise Exacerbation | 0 | 19 | 0 | 0 |
| Quick Recovery | 0 | 0 | 0 | 2 |
| Physical Exacerbation | 0 | 0 | 0 | 0 |
| Symptom | MS % (n) | ME and CFS % (n) | PPS % (n) |
|---|---|---|---|
| Quick Recovery | 42.3 (66) | 1.3 (5) | 38.3 (64) |
| Exercise Exacerbation | 10.8 (17) | 47.6 (179) | 34.1 (57) |
| Physical Exacerbation | 65.6 (103) | 94.7 (356) | 68.3 (114) |
| Mental Exacerbation | 55.4 (87) | 91.4 (342) | 34.9 (58) |
| Symptom | MS % (n) | ME and CFS % (n) | PPS % (n) |
|---|---|---|---|
| No Exacerbation | 21.0 (33) | 2.1 (8) | 12.3 (86) |
| ≤1 h | 10.8 (17) | 0.8 (3) | 13.2 (22) |
| 2–3 h | 28.7 (45) | 2.1 (8) | 19.8 (33) |
| 4–10 h | 17.2 (27) | 6.1 (23) | 11.4 (19) |
| 11–13 h | 3.2 (5) | 1.3 (5) | 3.6 (6) |
| 14–23 h | 10.2 (16) | 14.1 (53) | 11.4 (19) |
| ≥24 h | 8.9 (14) | 73.4 (276) | 13.8 (23) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cotler, J.; Holtzman, C.; Dudun, C.; Jason, L.A. A Brief Questionnaire to Assess Post-Exertional Malaise. Diagnostics 2018, 8, 66. https://doi.org/10.3390/diagnostics8030066
Cotler J, Holtzman C, Dudun C, Jason LA. A Brief Questionnaire to Assess Post-Exertional Malaise. Diagnostics. 2018; 8(3):66. https://doi.org/10.3390/diagnostics8030066
Chicago/Turabian StyleCotler, Joseph, Carly Holtzman, Catherine Dudun, and Leonard A. Jason. 2018. "A Brief Questionnaire to Assess Post-Exertional Malaise" Diagnostics 8, no. 3: 66. https://doi.org/10.3390/diagnostics8030066
APA StyleCotler, J., Holtzman, C., Dudun, C., & Jason, L. A. (2018). A Brief Questionnaire to Assess Post-Exertional Malaise. Diagnostics, 8(3), 66. https://doi.org/10.3390/diagnostics8030066