Myalgic Encephalomyelitis (ME) or What? An Operational Definition


Abstract
1. Introduction
2. Method
3. Results
3.1. Characteristics
3.1.1. An Epidemic and an Endemic Form
3.1.2. An Often Sudden, Sometimes Gradual, Onset
3.1.3. An Acute and a Chronic Phase
3.1.4. Not Just Like Other Post-Viral Fatigue States
3.1.5. A Prolonged Relapsing Course
3.1.6. Diurnal Variability of Symptoms
3.2. Symptoms
3.2.1. Muscle Fatigability/Prolonged Muscle Weakness after Exertion is a Mandatory Feature of ME
3.2.2. Neurological Disturbance Is an Essential Feature of ME
3.2.3. ME Often Coincides with a Number of Symptoms Related to Other Body Systems
3.2.4. ME Is Often Accompanied by Emotional Problems, but Is Not Caused by Those Symptoms
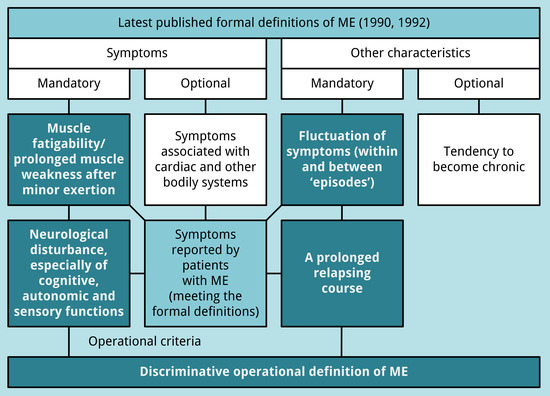
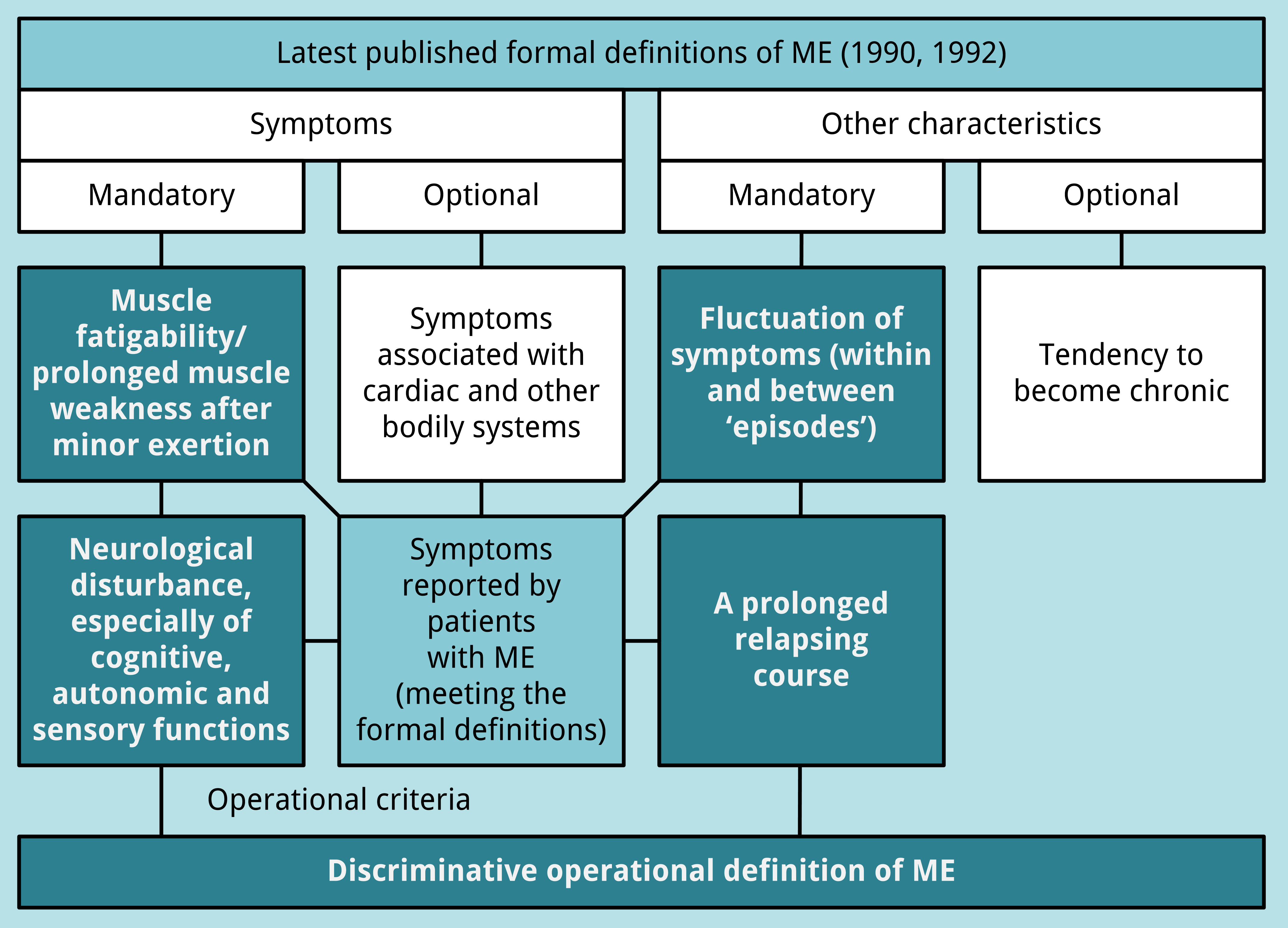
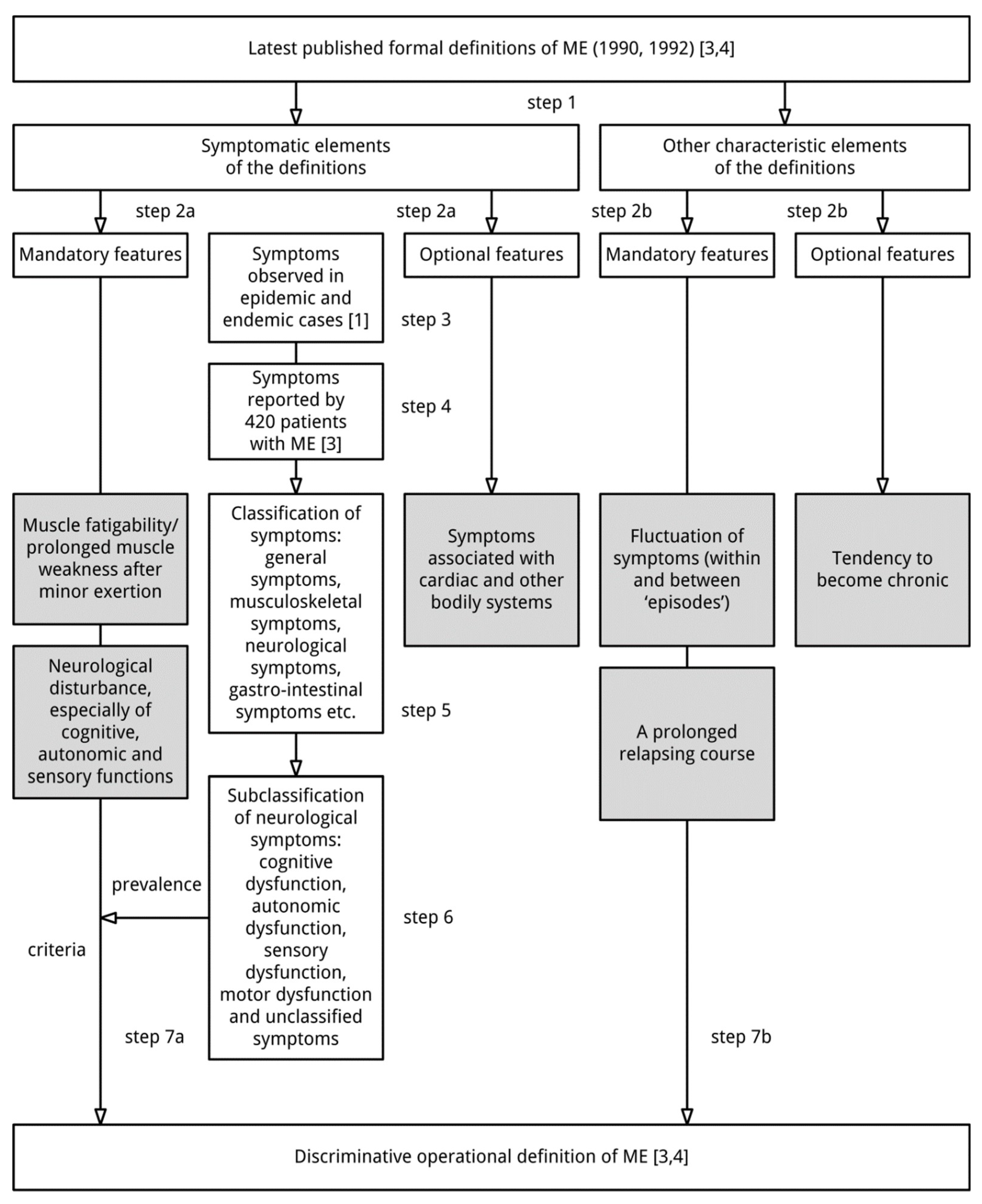
3.3. An Operational Definition of ME
- muscle fatigability/prolonged muscle weakness after trivial exertion;
- neurological disturbance (see Table 3):
- at least one symptom related to cognitive dysfunction or one unclassified neurological symptom;
- at least one symptom related to autonomic dysfunction; and
- at least two symptoms related to sensory dysfunction;
- fluctuation of symptoms (within and between “episodes”); and
- a prolonged relapsing course.
4. Discussion
5. Conclusions
- muscle fatigability/prolonged muscle weakness after trivial exertion;
- neurological disturbance, especially of cognitive, autonomic and sensory functions;
- fluctuation of symptoms (within and between ‘episodes’); and
- a prolonged relapsing course.
Acknowledgments
Conflicts of Interest
References
- Ramsay, A.M. Postviral Fatigue Syndrome—The Saga of Royal Free Disease, 1st ed.; Gower Medical Publishing (for the Myalgic Encephalomyelitis Association): London, UK, 1986. [Google Scholar]
- Dowsett, E.G. Myalgic encephalomyelitis, or what? Lancet 1988, 332, 100–101. [Google Scholar] [CrossRef]
- Dowsett, E.G.; Ramsay, A.M.; McCartney, R.A.; Bell, E.J. Myalgic Encephalomyelitis—A persistent enteroviral infection? Postgrad. Med. J. 1990, 66, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, A.M.; Dowsett, E.G. Myalgic Encephalomyelitis: Then and now, an epidemiological introduction. In The Clinical and Scientific Basis of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Hyde, B.M., Goldstein, J., Levine, P., Eds.; The Nightingale Research Foundation: Ottawa, ON, Canada, 1992; pp. 81–84. [Google Scholar]
- Acheson, E.D. The clinical syndrome variously called benign myalgic encephalomyelitis, Iceland disease and epidemic neuromyasthenia. Am. J. Med. 1959, 26, 569–595. [Google Scholar] [CrossRef]
- Gilliam, A.G. Epidemiological Study on an Epidemic, Diagnosed as Poliomyelitis, Occurring among the Personnel of Los Angeles County General Hospital during the Summer of 1934. Available online: https://babel.hathitrust.org/cgi/pt?id=mdp.39015022082260;view=1up;seq=617 (accessed on 3 August 2018).
- Acheson, D.E. A new clinical entity? Lancet 1956, 267, 789–790. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Diseases, Eighth Revision (ICD-8): I (Code 323): 158; WHO: Geneva, Switzerland, 1967. [Google Scholar]
- World Health Organization. International Classification of Diseases, Tenth Revision (ICD-10): G93.3; WHO: Geneva, Switzerland, 1992; Available online: http://apps.who.int/classifications/icd10/browse/2016/en#/G90-G99 (accessed on 7 September 2018).
- Holmes, G.P.; Kaplan, J.E.; Gantz, N.M.; Komaroff, A.L.; Schonberger, L.B.; Straus, S.E.; Jones, J.F.; Dubois, R.E.; Cunningham-Rundles, C.; Pahwa, S.; et al. Chronic fatigue syndrome: A working case definition. Ann. Intern. Med. 1988, 108, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.; Dobbins, J.G.; Komaroff, A.L. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.; Hickie, I.; Hadzi-Pavlovic, D.; Wakefield, D.; Parker, G.; Straus, S.E.; Dale, J.; McCluskey, D.; Hinds, G.; Brickman, A.; et al. What is chronic fatigue syndrome? Heterogeneity within an international multicentre study. Aust. N. Z. J. Psychiatry 2001, 35, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Twisk, F.N.M. Myalgic Encephalomyelitis, chronic fatigue syndrome, and Systemic Exertion Intolerance Disease: Three distinct clinical entities. Challenges 2018, 9, 19. [Google Scholar] [CrossRef]
- The Medical Staff of the Royal Free Hospital. An outbreak of Encephalomyelitis in the Royal Free Hospital Group, London, in 1955. Br. Med. J. 1957, 2, 895–904. [Google Scholar] [CrossRef]
- Ramsay, A.M. Encephalomyelitis in north west London; an endemic infection simulating poliomyelitis and hysteria. Lancet 1957, 270, 1196–1200. [Google Scholar] [CrossRef]
- Parish, J.G. Early outbreaks of ‘epidemic neuromyasthenia’. Postgrad. Med. J. 1978, 54, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, B.; Sigurjonsson, J.; Sigurdsson, J.H.; Thorkelsson, J.; Gudmundsson, K.R. A disease epidemic in Iceland simulating poliomyelitis. Am. J. Hyg. 1950, 52, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Damrongvachiraphan, D.; Hunnell, J.; Bartgis, L.; Evans, M.; Brown, A. Myalgic Encephalomyelitis: Case definitions. Auton. Control Physiol. State Funct. 2012, 1, 1–14. [Google Scholar] [CrossRef]
- Jason, L.A.; Brown, A.; Clyne, E.; Bartgis, L.; Evans, M.; Brown, M. Contrasting case definitions for chronic fatigue syndrome, Myalgic Encephalomyelitis/chronic fatigue syndrome and Myalgic Encephalomyelitis. Eval. Health Prof. 2012, 35, 280–304. [Google Scholar] [CrossRef] [PubMed]
- Sunnquist, M.; Jason, L.A.; Nehrke, P.; Goudsmit, E.M. A comparison of case definitions for Myalgic Encephalomyelitis and chronic fatigue syndrome. J. Chronic Dis. Manag. 2017, 2, 1013. [Google Scholar] [PubMed]
- Underhill, R.A. Myalgic encephalomyelitis, chronic fatigue syndrome: An infectious disease. Med. Hypotheses 2015, 85, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef] [PubMed]
- Siemionow, V.; Fang, Y.; Calabrese, L.; Sahgal, V.; Yue, G.H. Altered central nervous system signal during motor performance in chronic fatigue syndrome. Clin. Neurophysiol. 2004, 115, 2372–2381. [Google Scholar] [CrossRef] [PubMed]
- Lawrie, S.M.; MacHale, S.M.; Cavanagh, J.T.; O′Carroll, R.E.; Goodwin, G.M. The difference in patterns of motor and cognitive function in chronic fatigue syndrome and severe depressive illness. Psychol. Med. 2000, 30, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.; Wood, L.; Behan, W.M.; Maclaren, W.M. Demonstration of delayed recovery from fatiguing exercise in chronic fatigue syndrome. Eur. J. Neurol. 1999, 6, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Fulcher, K.Y.; White, P.D. Strength and physiological response to exercise in patients with chronic fatigue syndrome. J. Neurol. Neurosurg. Psychiatry 2000, 69, 302–307. [Google Scholar] [CrossRef] [PubMed]
- McKay, M.J.; Baldwin, J.N.; Ferreira, P.; Simic, M.; Vanicek, N.; Burns, J. For the 1000 Norms Project Consortium. Normative reference values for strength and flexibility of 1000 children and adults. Neurology 2017, 88, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Douma, R.K.; Soer, R.; Krijnen, W.P.; Reneman, M.; van der Schans, C.P. Reference values for isometric muscle force among workers for the Netherlands: A comparison of reference values. BMC Sports Sci. Med. Rehabil. 2014, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; van de Sande, M.I.; de Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International consensus criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, J.W.M.; Lloyd, A.R. A controversial consensus—Comment on article by Broderick et al. J. Intern. Med. 2012, 271, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Dowsett, E.G.; Goudsmit, E.; Macintyre, A.; Shepherd, C.B. London criteria for ME. In Report from The National Task Force on Chronic Fatigue Syndrome (CFS), Post Viral Fatigue Syndrome (PVFS), Myalgic Encephalomyelitis (ME); Westcare: Bristol, UK, 1994; pp. 96–98. [Google Scholar]
- Hyde, B. A New and Simple Definition of Myalgic Encephalomyelitis and a New Simple Definition of Chronic Fatigue Syndrome & A Brief History of Myalgic Encephalomyelitis and an Irreverent History of Chronic Fatigue Syndrome. In Proceedings of the Invest in ME Conference 2006, London, UK, 12 May 2006; Available online: http://www.imet.ie/imet_documents/BYRON_HYDE_little_red_book.pdf (accessed on 12 May 2016).


{kind=link}
{kind=link}
| Definition of ME (1990) |
|---|
| “A syndrome commonly initiated by respiratory and/or gastro-intestinal infection but an insidious or more dramatic onset following neurological, cardiac or endocrine disability occurs. |
The pathognomonic features (of ME) are:
|
| Other characteristics include [..] a prolonged relapsing course and variation in intensity of symptoms within and between episodes, tending to chronicity.” |
| Definition of ME (1992) |
|---|
| “A syndrome initiated by a viral infection commonly described as a respiratory/gastro intestinal illness but a gradual or more dramatic onset following neurological, cardiac or endocrine disability is recognised. The cardinal features, in a patient who has previously been physically and mentally fit, with a good work record are:
|
| Cognitive Dysfunction |
|
| Autonomic Dysfunction |
|
| Sensory Dysfunction |
|
| Motor Dysfunction |
|
| Unclassified Neurological Symptoms |
|
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Twisk, F. Myalgic Encephalomyelitis (ME) or What? An Operational Definition. Diagnostics 2018, 8, 64. https://doi.org/10.3390/diagnostics8030064
Twisk F. Myalgic Encephalomyelitis (ME) or What? An Operational Definition. Diagnostics. 2018; 8(3):64. https://doi.org/10.3390/diagnostics8030064
Chicago/Turabian StyleTwisk, Frank. 2018. "Myalgic Encephalomyelitis (ME) or What? An Operational Definition" Diagnostics 8, no. 3: 64. https://doi.org/10.3390/diagnostics8030064
APA StyleTwisk, F. (2018). Myalgic Encephalomyelitis (ME) or What? An Operational Definition. Diagnostics, 8(3), 64. https://doi.org/10.3390/diagnostics8030064