The Role of Ultrasound in Screening Dense Breasts—A Review of the Literature and Practical Solutions for Implementation

Abstract
:1. Introduction
2. Review of the Literature—Handheld Screening Breast Ultrasound
3. Review of the Literature—Automated Screening Breast Ultrasound and Integrating SBU into Clinical Practice
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Cancer Society. About Breast Cancer. Available online: https://www.cancer.org/content/dam/CRC/PDF/Public/8577.00.pdf (accessed on 30 December 2017).
- Etzioni, R.; Urban, N.; Ramsey, S.; McIntosh, M.; Schwartz, S.; Reid, B.; Radich, J.; Anderson, G.; Hartwell, L. The case for early detection. Nat. Rev. Cancer 2003, 3, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Arleo, E.K.; Hendrick, R.E.; Helvie, M.A.; Sickles, E.A. Comparison of recommendations for screening mammography using CISNET models. Cancer 2017, 123, 3673–3680. [Google Scholar] [CrossRef] [PubMed]
- D’Orsi, C.J.; Sickles, E.A.; Mendelson, E.B. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Irshad, A.; Leddy, R.; Ackerman, S.; Cluver, A.; Pavic, D.; Abid, A.; Lewis, M.C. Effects of changes in BI-RADS density assessment guidelines (fourth versus fifth edition) on breast density assessment: Intra and interreader agreements and density distribution. AJR 2016, 207, 1366–1371. [Google Scholar] [CrossRef] [PubMed]
- Kolb, T.M.; Lichy, J.; Newhouse, J.H. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: An analysis of 27,825 patient evaluations. Radiology 2002, 225, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.F.; Guo, H.; Martin, L.J.; Sun, L.; Stone, J.; Fishell, E.; Jong, R.A.; Hislop, G.; Chiarelli, A.; Minkin, S.; et al. Mammographic density and the risk and detection of breast cancer. N. Engl. J. Med. 2007, 356, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Yaghjyan, L.; Colditz, G.A.; Rosner, B.; Tamimi, R.M. Mammographic breast density and subsequent risk of breast cancer in postmenopausal women according to the time since the mammogram. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Pisano, E.D.; Hendrick, R.E.; Yaffe, M.J.; Baum, J.K.; Acharyya, S.; Cormack, J.B.; Hanna, L.A.; Conant, E.F.; Fajardo, L.L.; Bassett, L.W.; et al. Diagnostic accuracy of digital versus film mammography: Exploratory analysis of selected population subgroups in DMIST. Radiology 2008, 246, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Dense Breast-Info, Legislation and Regulations—What is Required? Available online: http://densebreast-info.org/legislation.aspx (accessed on 2 February 2018).
- Leach, M.O.; Boggis, C.R.; Dixon, A.K.; Easton, D.F.; Eeles, R.A.; Evans, D.G.; Gilbert, F.J.; Griebsch, I.; Hoff, R.J.; Kessar, P.; et al. Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: A prospective multicentre cohort study (MARIBS). Lancet 2005, 365, 1769–1778. [Google Scholar] [PubMed]
- Kriege, M.; Brekelmans, C.T.; Boetes, C.; Besnard, P.E.; Zonderland, H.M.; Obdeijn, I.M.; Manoliu, R.A.; Kok, T.; Peterse, H.; Tilanus-Linthorst, M.M.; et al. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N. Engl. J. Med. 2004, 351, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Lehman, C.D.; Isaacs, C.; Schnall, M.D.; Pisano, E.D.; Ascher, S.M.; Weatherall, P.T.; Bluemke, D.A.; Bowen, D.J.; Marcom, P.K.; Armstrong, D.K.; et al. Cancer yield of mammography, MR, and US in high-risk women: Prospective multi-institution breast cancer screening study. Radiology 2007, 244, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Monticciolo, D.; Newell, M.S.; Moy, L.; Niell, B.; Monsees, B.; Sickles, E.A. Breast Cancer Screening in Women at Higher-Than-Average Risk: Recommendations from the ACR. J. Am. Coll. Radiol. 2018, in press. [Google Scholar]
- Kaplan, S.S. Clinical utility of bilateral whole-breast US in the evaluation of women with dense breast tissue. Radiology 2001, 221, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Leconte, I.; Feger, C.; Galant, C.; Berlière, M.; Berg, B.V.; D’Hoore, W.; Maldague, B. Mammography and subsequent whole-breast sonography of nonpalpable breast cancers: The importance of radiologic breast density. AJR Am. J. Roentgenol. 2003, 180, 1675–1679. [Google Scholar] [CrossRef] [PubMed]
- Berg, W.A.; Blume, J.D.; Cormack, J.B.; Mendelson, E.B.; Lehrer, D.; Böhm-Vélez, M.; Pisano, E.D.; Jong, R.A.; Evans, W.P.; Morton, M.J.; et al. Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA 2008, 299, 2151–2163. [Google Scholar] [CrossRef] [PubMed]
- Berg, W.A.; Zhang, Z.; Lehrer, D.; Jong, R.A.; Pisano, E.D.; Barr, R.G.; Böhm-Vélez, M.; Mahoney, M.C.; Evans, W.P.; Larsen, L.H.; et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 2012, 307, 1394–1404. [Google Scholar] [PubMed]
- Hooley, R.J.; Greenberg, K.L.; Stackhouse, R.M.; Geisel, J.L.; Butler, R.S.; Philpotts, L.E. Screening US in patients with mammographically dense breasts: Initial experience with Connecticut Public Act 09-41. Radiology 2012, 265, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Weigert, J.; Steenbergen, S. The Connecticut experiment: The role of ultrasound in the screening of women with dense breasts. Breast J. 2012, 18, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Weigert, J.; Steenbergen, S. The Connecticut experiments second year: Ultrasound in the screening of women with dense breasts. Breast J. 2015, 21, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Brem, R.F.; Tabar, L.; Duffy, S.W.; Inciardi, M.F.; Guingrich, J.A.; Hashimoto, B.E.; Lander, M.R.; Lapidus, R.L.; Peterson, M.K.; Rapelyea, J.A.; et al. Assessing improvement in detection of breast cancer with three-dimensional automated breast US in women with dense breast tissue: The SomoInsight Study. Radiology 2015, 274, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Tagliafico, A.S.; Calabrese, M.; Mariscotti, G.; Durando, M.; Tosto, S.; Monetti, F.; Airaldi, S.; Bignotti, B.; Nori, J.; Bagni, A.; et al. Adjunct screening with tomosynthesis or ultrasound in women with mammography-negative dense breasts: Interim report of a prospective comparative trial. J. Clin. Oncol. 2016, 34, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Ohuchi, N.; Suzuki, A.; Sobue, T.; Kawai, M.; Yamamoto, S.; Zheng, Y.F.; Shiono, Y.N.; Saito, H.; Kuriyama, S.; Tohno, E.; et al. Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): A randomised controlled trial. Lancet 2016, 387, 341–348. [Google Scholar] [CrossRef]
- Giger, M.L.; Inciardi, M.F.; Edwards, A.; Papaioannou, J.; Drukker, K.; Jiang, Y.; Brem, R.; Brown, J.B. Automated Breast Ultrasound in Breast Cancer Screening of Women With Dense Breasts: Reader Study of Mammography-Negative and Mammography-Positive Cancers. AJR Am. J. Roentgenol. 2016, 206, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Wilczek, B.; Wilczek, H.E.; Rasouliyan, L.; Leifland, K. Adding 3D automated breast ultrasound to mammography screening in women with heterogeneously and extremely dense breasts: Report from a hospital-based, high-volume, single-center breast cancer screening program. Eur. J. Radiol. 2016, 85, 1554–1563. [Google Scholar] [CrossRef] [PubMed]
- Weigert, J.M. The Connecticut Experiment; The Third Installment: 4 Years of Screening Women with Dense Breasts with Bilateral Ultrasound. Breast J. 2017, 23, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Destounis, S.; Arieno, A.; Morgan, R. New York state breast density mandate: Follow-up data with screening sonography. Ultrasound Med. 2017, 36, 2511–2517. [Google Scholar] [CrossRef] [PubMed]
- Corsetti, V.; Houssami, N.; Ghirardi, M.; Ferrari, A.; Speziani, M.; Bellarosa, S.; Remida, G.; Gasparotti, C.; Galligioni, E.; Ciatto, S. Evidence of the effect of adjunct ultrasound screening in women with mammography-negative dense breasts: Interval breast cancers at 1 year follow-up. EUR J. Cancer 2011, 47, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Uematsu, T. The need for supplemental breast cancer screening modalities: A perspective of population-based breast cancer screening programs in Japan. Breast Cancer 2017, 24, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Vourtsis, A.; Kachulis, A. The performance of 3D ABUS versus HHUS in the visualization and BI-RADS characterization of breast lesions in a large cohort of 1,886 women. Eur. Radiol. 2017, 28, 592–601. [Google Scholar] [CrossRef] [PubMed]
- Berg, W. Current status of supplemental screening in dense breasts. J. Clin. Oncol. 2016, 34, 1840–1843. [Google Scholar] [CrossRef] [PubMed]
- Brem, R.F.; Lenihan, M.J.; Lieberman, J.; Torrente, J. Screening breast ultrasound: Past, present, and future. AJR Am. J. Roentgenol. 2015, 204, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Van Zelst, J.C.M.; Tan, T.; Clauser, P.; Domingo, A.; Dorrius, M.D.; Drieling, D.; Golatta, M.; Gras, F.; de Jong, M.; Pijnappel, R.; et al. Dedicated computer-aided detection software for automated 3D breast ultrasound; an efficient tool for the radiologist in supplemental screening of women with dense breasts. Eur. Radiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.L.; Maroglies, L.R.; Schwager, S.J.; Zuckerman, S.; Patel, N.; Szabo, J.; Sonnenblick, E. Early discussion of breast density and supplemental breast cancer screening: Is it possible? Breast J. 2014, 20, 229–234. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
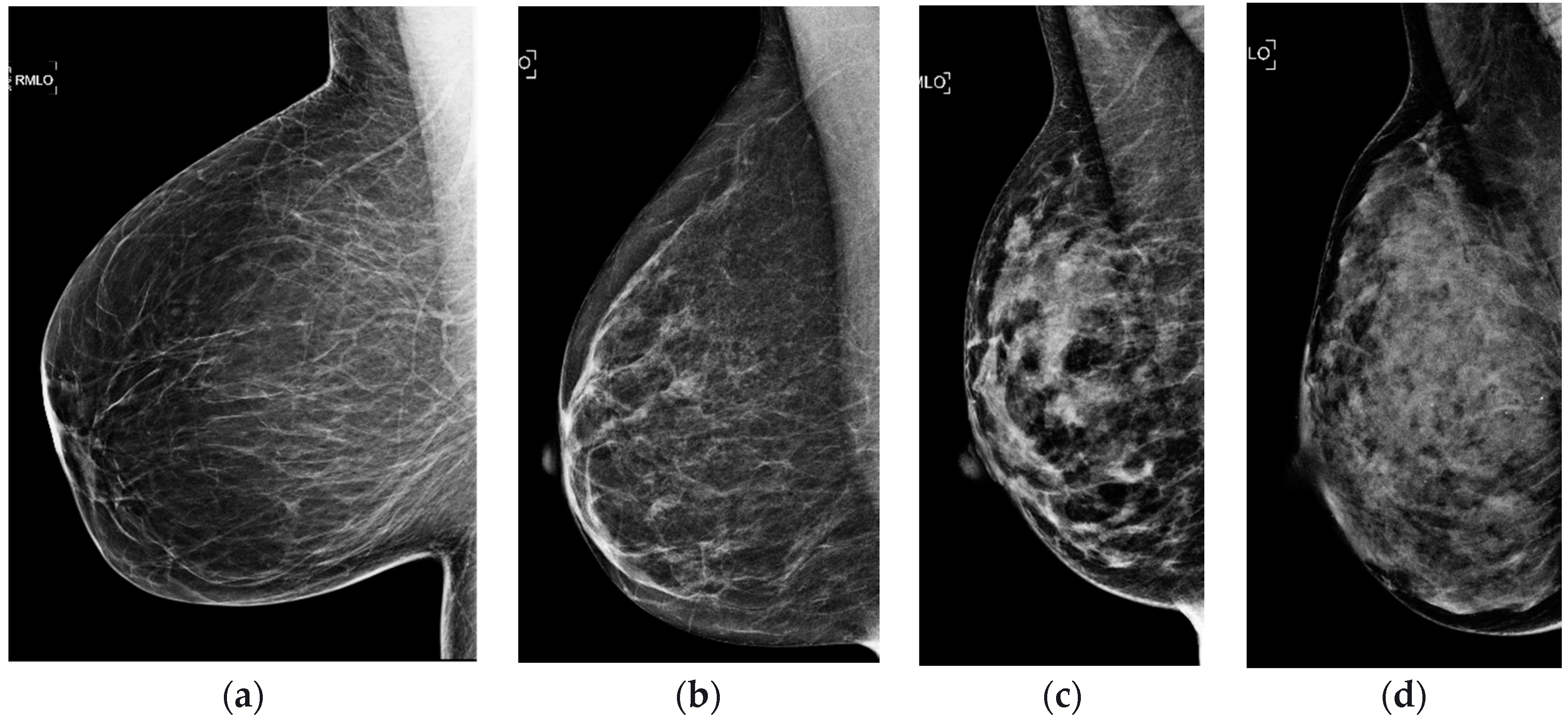
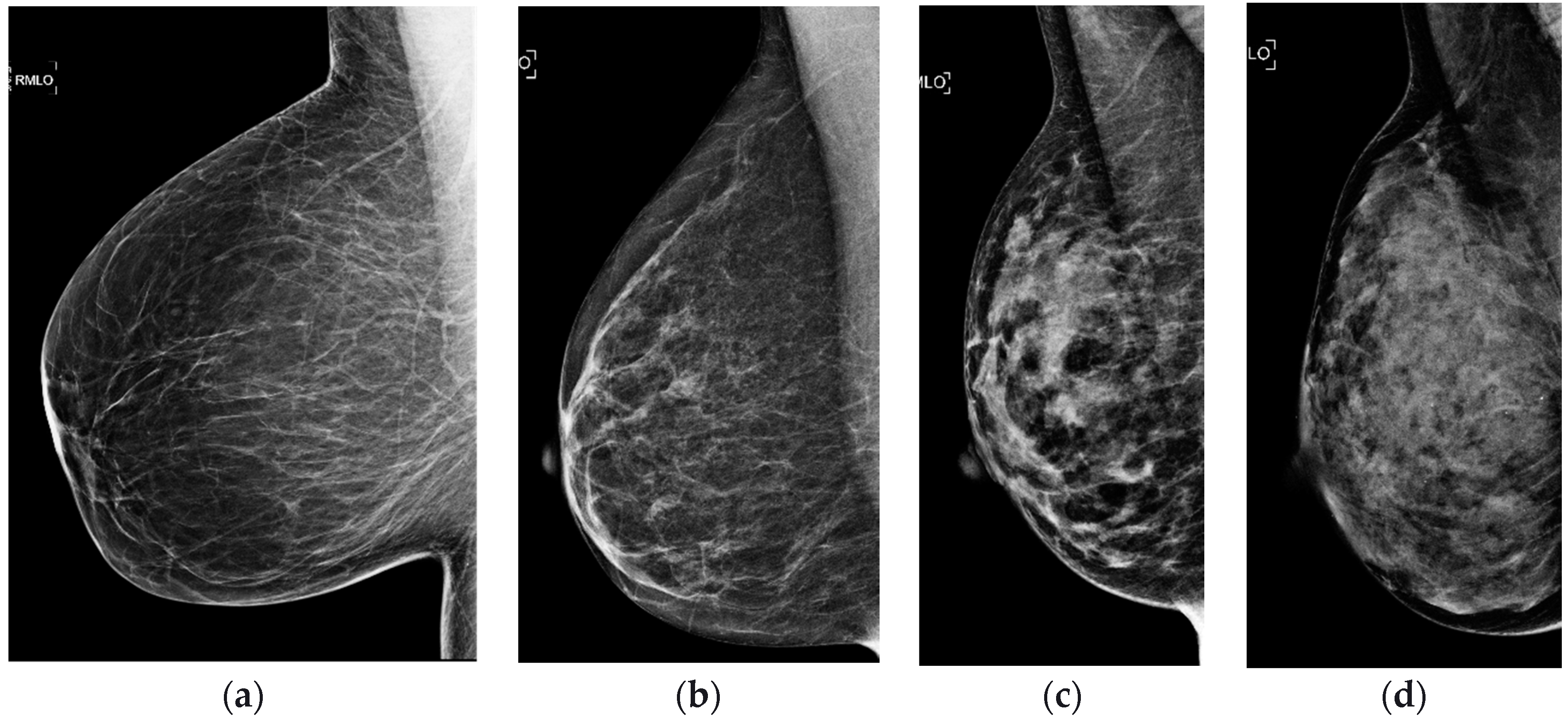
| Tissue Composition | 4th Edition | 5th Edition |
|---|---|---|
| Almost entirely fatty | 1 | a |
| Scattered fibroglandular tissues | 2 | b |
| Heterogeneously dense | 3 | c |
| Extremely dense | 4 | d |
| Study | Study Description | Method | No. of Screening US Exam | No. of US-Only Cancers | Mammography Plus Ultrasound | Additional Cancer Yield from US per 1000 Women Screened | ||
|---|---|---|---|---|---|---|---|---|
| Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | ||||||
| Kaplan [15] | BI-RADS c-d density; patients with negative clinical examination and mammographic findings; in patients with focal abnormal mammographic findings or palpable abnormalities, all areas of the breast outside of the quadrant with abnormalities were evaluated with ultrasound | Tech HHUS | 1862 | 6 | - | - | - | 3.2 |
| Kolb et al. [6] | BI-RADS b-d density; patients with no clinical symptoms | MD HHUS | 13,547 | 37 | 97.3 | - | - | 2.73 |
| Leconte et al. [16] | BI-RADS a-d density; palpable abnormalities were excluded from analysis | MD HHUS | 4236 | 16 | B1-2 density: MA = 80 US = 88 | - | - | 3.8 |
| B3-4 density: MA = 56 US = 88 | ||||||||
| Berg et al. [17] | BI-RADS c-d density in at least one quadrant and at high risk; radiologist blinded to mammography and physical examination findings | MD HHUS | 2809 | 12 | 77.5 | - | 11.2 | 4.2 |
| Berg et al. [18] | BI-RADS c-d density in at least one quadrant and at high risk; radiologist blinded to mammography and physical examination findings | MD HHUS | 2809 | 32 | 76 | 84 | 16 | 3.7 |
| Hooley et al. [19] | BI-RADS c-d density; patients with no clinical symptoms; mammographic findings were excluded | Tech HHUS | 935 | 3 | - | - | 6.5 | 3.2 |
| Weigert and Steenberge [20] | BI-RADS c-d density; patients with normal mammograms; no clinical symptoms | Tech HHUS | 8647 | 28 | 96.6 | 94.9 | 6.7 | 3.25 |
| Weigert and Steenbergen [21] | BI-RADS c-d density; patients with normal mammograms; no clinical symptoms | Tech HHUS | 10,282 | 24 | - | 96 | 9 | 2.3 |
| Brem et al. [22] | BI-RADS c-d density; patients with normal mammograms and no clinical symptoms | Tech ABUS | 15,318 | 30 | 100 | 72 | 2.6 | 1.9 |
| Tagliafico et al. [23] | BI-RADS c-d density; patients with no clinical symptoms; mammography-negative; radiologist who performed ultrasound aware of negative 2D mammography and blinded to tomosynthesis | MD HHUS | 3231 | 11 (not seen on 2D or 3D) | - | - | - | 3.4 (not seen on 2D or 3D) |
| 23 (seen also on 3D) | 7.1 (seen also on 3D) | |||||||
| Ohuchi et al. [24] | BI-RADS a-d density; intervention group included mammography and ultrasound on all patients; control group included mammography only; radiologists blinded to mammography and ultrasound findings | Tech HHUS | 36,752 | 67 | - | - | - | 1.8 |
| Giger et al. [25] | BI-RADS c-d density; patients with no clinical symptoms; retrospective study design | Tech ABUS | 185 | 31 | 74.1 | 76.1 | - | |
| Wilczek et al. [26] | BI-RADS c-d density; patients with no clinical symptoms; first reader interpreted mammogram and ultrasound; second reader interpreted ultrasound only | Tech ABUS | 1668 | 4 | - | - | 33.3 | 2.4 |
| Weigert [27] | BI-RADS c-d density; patients with normal mammograms; no clinical symptoms; 4 year retrospective study design | Tech HHUS | Year 1: 2706 | 11 | - | - | 7.3 | 4 |
| Year 2: 3351 | 9 | - | - | 5 | 2.7 | |||
| Year 3: 4128 | 11 | - | - | 7.4 | 2.7 | |||
| Year 4: 3331 | 10 | - | - | 18.9 | 3 | |||
| Destounis et al. [28] | BI-RADS c-d density; patients with no clinical symptoms | HHUS | 5434 | 18 | - | - | 18 | 3.3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thigpen, D.; Kappler, A.; Brem, R. The Role of Ultrasound in Screening Dense Breasts—A Review of the Literature and Practical Solutions for Implementation. Diagnostics 2018, 8, 20. https://doi.org/10.3390/diagnostics8010020
Thigpen D, Kappler A, Brem R. The Role of Ultrasound in Screening Dense Breasts—A Review of the Literature and Practical Solutions for Implementation. Diagnostics. 2018; 8(1):20. https://doi.org/10.3390/diagnostics8010020
Chicago/Turabian StyleThigpen, Denise, Amanda Kappler, and Rachel Brem. 2018. "The Role of Ultrasound in Screening Dense Breasts—A Review of the Literature and Practical Solutions for Implementation" Diagnostics 8, no. 1: 20. https://doi.org/10.3390/diagnostics8010020
APA StyleThigpen, D., Kappler, A., & Brem, R. (2018). The Role of Ultrasound in Screening Dense Breasts—A Review of the Literature and Practical Solutions for Implementation. Diagnostics, 8(1), 20. https://doi.org/10.3390/diagnostics8010020