
A Resident’s Perspective of Ovarian Cancer

Abstract
:1. Introduction
2. Ovarian Cancer Risk Factors
2.1. Inherent Risk Factors
2.2. Genetic Risk Factors
3. Clinical Presentation
3.1. Symptoms
3.2. Physical Examination Findings
3.3. Ovarian Cancer Paraneoplastic Syndromes
4. Diagnosis of Ovarian Cancer
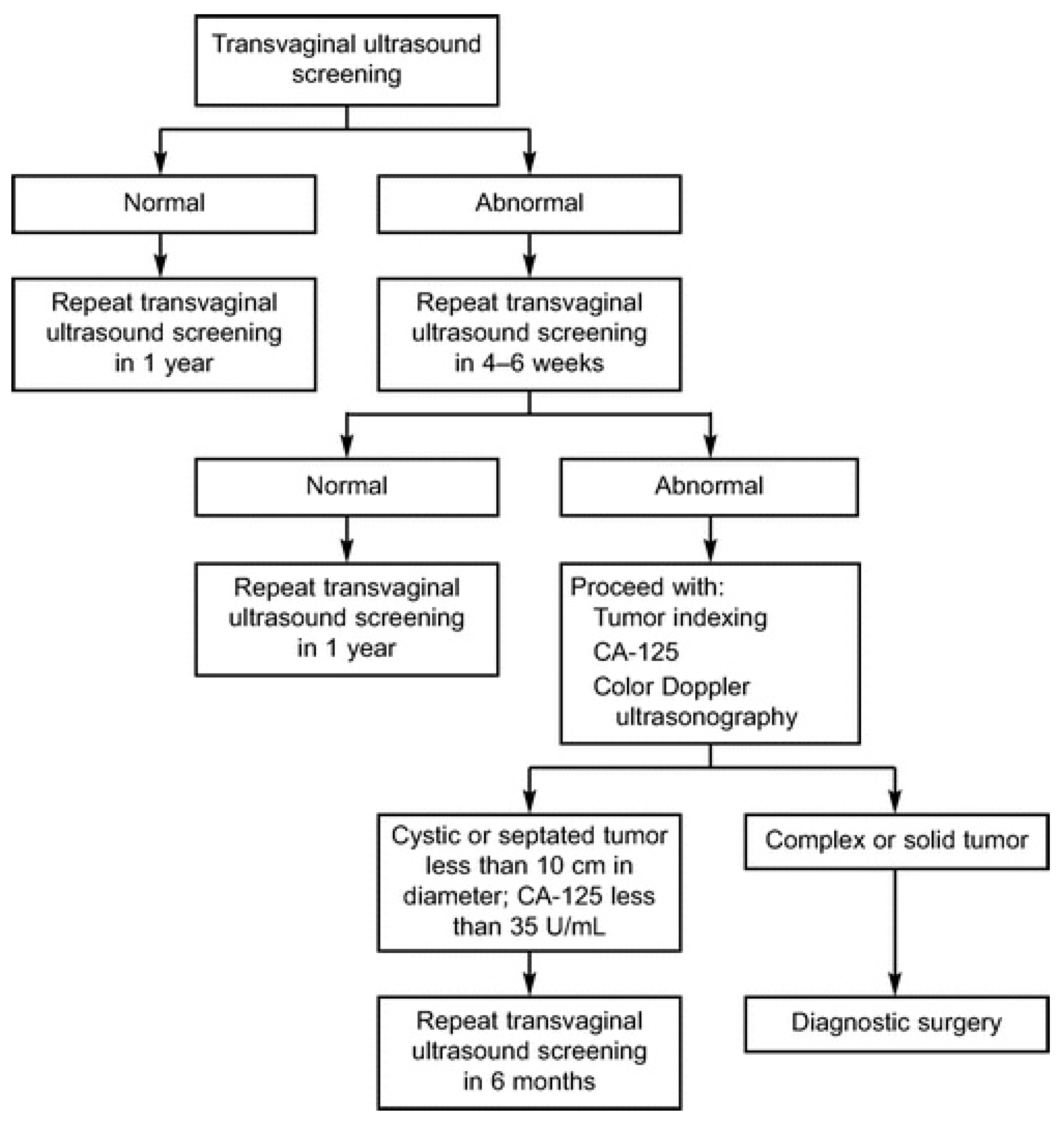
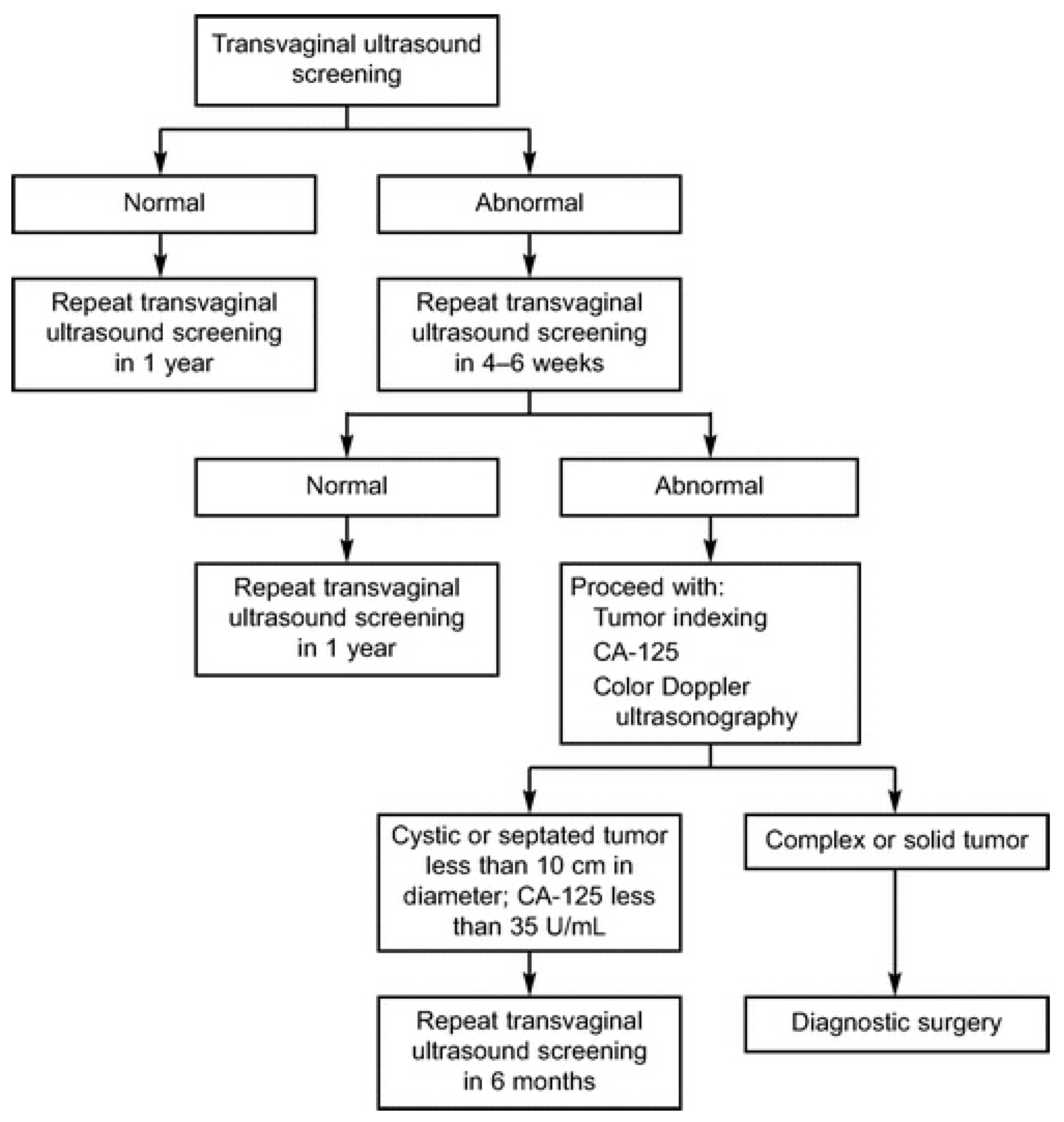
4.1. Diagnostic Schema
4.2. Tumor Markers
5. Ovarian Cancer Staging
6. Treatment of Ovarian Cancer and Side Effects
6.1. Side Effects of Surgery
6.2. Chemotherapy and Associated Side Effects
7. Psychosocial Effects of Ovarian Cancer
8. Ovarian Cancer Screening
8.1. Overview of Early Detection of Ovarian Cancer
8.2. Disease Screening Principles
- High sensitivity: the ability to identify everyone with disease who tests positive (true positive) from everyone with disease (true positives + false negatives). Ideally, a highly sensitive test will have a low rate of false negative results so the test rarely misses subjects with the disease;
- High specificity: the ability to correctly identify subjects without the disease (true negatives) from everyone without disease (true negatives + false positives). A highly specific screening test will have a low false positive rate;
- High positive predictive value: the portion of subjects with disease that tested positive (true positives) relative to all who tested positive (true positives + false positives), a value dependent on the prevalence of the disease;
- High negative predictive value: the portion without disease that tested negative (true negatives) relative to everyone testing negative (true negatives + false negatives), which is inversely dependent on disease prevalence;
- Low cost: to allow maximum test affordability.
8.3. Ovarian Cancer Screening Trials
8.3.1. University of Kentucky Ovarian Cancer Screening Program
8.3.2. Prostate, Lung, Colon, and Ovarian Cancer Screening Trial
8.3.3. United Kingdom Collaborative Trial of Ovarian Cancer Screening Trial
8.3.4. Multi-Center Japan University Trial
9. Life Is More Than Death: An Interview with the Husband of a Recently Deceased Woman Suffering from Advanced Stage Ovarian Cancer
9.1. Pre-Diagnosis Life
9.2. Life after Diagnosis for Both Individuals
9.3. Life during Treatment for Both Individuals
9.4. Life during the Final Months for Both Individuals
9.5. Feelings of the Family (Husband) after the Woman’s Death
10. Conclusions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Van Nagell, J.R.; Miller, R.W.; DeSimone, C.P.; Ueland, F.R.; Podzielinski, I.; Goodrich, S.T.; Elder, J.W.; Huang, B.; Kryscio, R.J.; Pavlik, E.J. Long-term survival of women with epithelial ovarian cancer detected by ultrasonographic screening. Obstet. Gynecol. 2011, 118, 1212–1221. [Google Scholar] [CrossRef] [PubMed]
- Van Nagell, J.R.; Pavlik, E.J. Ovarian cancer screening. Clin. Obstet. Gynecol. 2012, 55, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Bridgewater, J.A.; Rustin, G.J.S. Management of Non-Epithelial Ovarian Tumours. Oncology 1999, 57, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Sundar, S.; Neal, R.D.; Kehoe, S. Diagnosis of ovarian cancer. BMJ 2015, 351, h4443. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Zarkavelis, G.; Seraj, E.; Zerdes, I.; Tatsi, K.; Pentheroudakis, G. Non-epithelial Ovarian Cancer: Elucidating Uncommon Gynaecological Malignancies. Anticancer Res. 2016, 36, 5031–5042. [Google Scholar] [CrossRef] [PubMed]
- Karnezis, A.N.; Cho, K.R.; Gilks, B.; Pearce, C.L.; Huntsman, D.G. The disparate origins of ovarian cancers: Pathogenesis and prevention strategies. Nat. Rev. Cancer 2017, 17, 65–74. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer (Version 1.2016). OV-D. Available online: https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf (accessed on 4 November 2017).
- Alvarado-Cabrero, I.; Navani, S.S.; Young, R.H.; Scully, R.E. Tumors of the Fimbriated End of the Fallopian Tube: A Clinicopathologic Analysis of 20 Cases, Including Nine Carcinomas. Int. J. Gynecol. Pathol. 1997, 16, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Colgan, T.J.; Murphy, J.; Cole, D.E.; Narod, S.; Rosen, B. Occult Carcinoma in Prophylactic Oophorectomy Specimens: Prevalence and Association with BRCA Germline Mutation Status. Am. J. Surg. Pathol. 2001, 25, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Cass, I.; Holschneider, C.; Datta, N.; Barbuto, D.; Walts, A.E.; Karlan, B.Y. BRCA-Mutation-Associated Fallopian Tube Carcinoma: A Distinct Clinical Phenotype? Obstet. Gynecol. 2005, 106, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, F.; Muto, M.G.; Lee, Y.; Elvin, J.A.; Callahan, M.J.; Feltmate, C.; Garber, J.E.; Cramer, D.W.; Crum, C.P. The Tubal Fimbria Is a Preferred Site for Early Adenocarcinoma in Women With Familial Ovarian Cancer Syndrome. Am. J. Surg. Pathol. 2006, 30, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Kindelberger, D.W.; Lee, Y.; Miron, A.; Hirsch, M.S.; Feltmate, C.; Medeiros, F.; Callahan, M.J.; Garner, E.O.; Gordon, R.W.; Birch, C.; et al. Intraepithelial Carcinoma of the Fimbriae and Pelvic Serous Carcinoma: Evidence for a Causal Relationship. Am. J. Surg. Pathol. 2007, 31, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Crum, C.R.; Drapkin, R.; Miron, A.; Ince, T.A.; Muto, M.; Kindelberger, D.W.; Lee, Y. The distal fallopian tube: A new model for pelvic serous carcinogenesis. Curr. Opin. Obstet. Gynecol. 2007, 19, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Landen, C.N.; Birrer, M.J.; Sood, A.K. Early Events in the Pathogenesis of Epithelial Ovarian Cancer. J. Clin. Oncol. 2008, 26, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Lengyel, E. Ovarian Cancer Development and Metastasis. Am. J. Pathol. 2010, 177, 1053–1064. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Shih, L.M. The Origin and Pathogenesis of Epithelial Ovarian Cancer: A Proposed Unifying Theory. Am. J. Surg. Pathol. 2010, 34, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Crum, C.P.; Mckeon, F.D.; Xian, X. The Oviduct and Ovarian Cancer: Causality, Clinical Implications, and “Targeted Prevention”. Clin. Obstet. Gynecol. 2012, 55, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Nezhat, F.R.; Aposto, R.l.; Nezha, C.T.; Pejovic, T. New insights in the pathophysiology of ovarian cancer and implications for screening and prevention. Am. J. Obstet. Gynecol. 2015, 213, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Heikaus, S.; Harter, P.; Heitz, F.; Grimm, C.; Ataseven, B.; Prader, S.; Kurzeder, C.; Ebel, T.; Traut, A.; et al. Serous Tubal Intraepithelial Carcinoma Associated With Extraovarian Metastases. Int. J. Gynecol. Cancer 2017, 27, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Surveillance, Epidemiology, and End Results (SEER) Program. Cancer of the Ovary—SEER Stat Facts Sheet. National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch. Available online: https://seer.cancer.gov/statfacts/html/ovary.html (accessed on 9 November 2016).
- Cancer of the Ovary: SEER Stat Fact Sheets. Available online: http://seer.cancer.gov/statfacts/html/ovary.html (accessed on 27 December 2016).
- Webb, P.M.; Jordan, S.J. Epidemiology of epithelial ovarian cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, R.A. The Biology of Cancer; Garland Science: New York, NJ, USA, 2014; Volume 231. [Google Scholar]
- Duncan, J.A.; Reeves, J.R.; Cooke, T.G. BRCA1 and BRCA2 proteins: Roles in health and disease. Mol. Pathol. 1998, 51, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Miki, Y. Role of BRCA1 and BRCA2 as regulators of DNA repair, transcription, and cell cycle in response to DNA damage. Cancer Sci. 2004, 95, 866–871. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Hereditary Breast and Ovarian Cancer Syndrome; ACOG Practice Bulletin No. 103; American College of Obstetricians and Gynecologists: Washington, DC, USA, 2009; Volume 113, pp. 957–966.
- Antoniou, A.; Pharoah, P.D.P.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average Risks of Breast and Ovarian Cancer Associated with BRCA1 or BRCA2 Mutations Detected in Case Series Unselected for Family History: A Combined Analysis of 22 Studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Brose, M.S.; Rebbeck, T.R.; Calzone, K.A.; Stopfer, J.E.; Nathanson, K.L.; Weber, B.L. Cancer Risk Estimates for BRCA1 Mutation Carriers Identified in a Risk Evaluation Program. J. Natl. Cancer Inst. 2002, 94, 1365–1372. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Lynch Syndrome; Practice Bulletin No. 147; American College of Obstetricians and Gynecologists: Washington, DC, USA, 2014; Volume 124, pp. 1042–1054.
- National Academies of Sciences, Engineering, and Medicine. Ovarian Cancers: Evolving Paradigms in Research and Care; The National Academies Press: Washington, DC, USA, 2016. [Google Scholar]
- Goff, B.A.; Mandel, L.S.; Drescher, C.W.; Urban, N.; Gough, S.; Schurman, K.M.; Patras, J.; Mahony, B.S.; Andersen, M.R. Development of an ovarian cancer symptom index: Possibilities for earlier detection. Cancer 2007, 109, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Goff, B. Symptoms associated with ovarian cancer. Clin. Obstet. Gynecol. 2012, 55, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Pavlik, E.J.; Saunders, B.A.; Doran, S.; McHugh, K.W.; Ueland, F.R.; Desemone, C.P.; Depriest, P.D.; Ware, R.A.; Kryscio, R.J.; van Nagell, J.R., Jr. The search for meaning—Symptoms and transvaginal sonography screening for ovarian cancer. Cancer 2009, 115, 3689–3698. [Google Scholar] [CrossRef] [PubMed]
- Rossing, M.A.; Wicklund, K.G.; Cushing-Haugen, K.L.; Weiss, N.S. Predictive value of symptoms for early detection of ovarian cancer. J. Natl. Cancer Inst. 2010, 102, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Cannistra, S.A. Cancer of the Ovary. N. Engl. J. Med. 2004, 351, 2519–2529. [Google Scholar] [CrossRef] [PubMed]
- Bast, R.C.; Feeney, M.; Lazarus, H.; Nadler, L.M.; Colvin, R.B.; Knapp, R.C. Reactivity of a monoclonal antibody with human ovarian carcinoma. J. Clin. Investig. 1981, 68, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lis, C.G. Role of CA125 in predicting ovarian cancer survival—A review of the epidemiological literature. J. Ovarian Res. 2009, 2, 13. [Google Scholar] [CrossRef] [PubMed]
- Fritsche, H.A.; Bast, R.C. CA 125 in ovarian cancer: Advances and controversy. Clin. Chem. 1998, 44, 1379–1380. [Google Scholar] [PubMed]
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian Cancer. Lancet 2014, 384, 1376–1388. [Google Scholar] [CrossRef]
- Moore, R.G.; Jabre-Raughley, M.; Brown, A.K.; Robison, K.M.; Miller, M.C.; Allard, W.J.; Kurman, R.J.; Bast, R.C.; Skates, S.J. Comparison of a novel multiple marker assay vs. the Risk of Malignancy Index for the prediction of epithelial ovarian cancer in patients with a pelvic mass. Am. J. Obstet. Gynecol. 2010, 203, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Novak, M.; Lukasz, J.; Stachowiak, G.; Stetkiewicz, T.; Wilczynski, J.R. Current clinical application of serum biomarkers to detect ovarian cancer. Prz. Menopauzalny 2015, 14, 254–259. [Google Scholar]
- Thrall, M.M.; Goff, B.A.; Symons, R.G.; Flum, D.R.; Gray, H.J. Thirty-day mortality after primary cytoreductive surgery for advanced ovarian cancer in the elderly. Obstet. Gynecol. 2011, 118, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Gerestein, C.G.; Nieuwenhuyzen-de Boer, G.M.; Eijekmans, M.J.; Kooi, G.S.; Burger, C.W. Prediction of 30-day morbidity after primary cytoreductive surgery for advanced stage ovarian cancer. Eur. J. Cancer 2010, 46, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.C.; Bodurka, D.C.; Weaver, C.B.; Rasu, R.; Wolf, J.K.; Bevers, M.W.; Smith, J.A.; Wharton, J.T.; Rubenstein, E.B. Rankings and symptom assessments of side effects from chemotherapy: Insights from experienced patients with ovarian cancer. Support. Care Cancer 2005, 13, 219–227. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Chemotherapy for Ovarian Cancer. Available online: https://www.cancer.org/cancer/ovarian-cancer/treating/chemotherapy.html (accessed on 9 November 2016).
- Guidozzi, F. Living with Ovarian Cancer. Gynecol. Oncol. 1992, 50, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Matulonis, U.A.; Kornblith, A.; Lee, H.; Bryan, J.; Gibson, C.; Wells, C.; Lee, J.; Sullivan, L.; Penson, R. Long-term adjustment of early-stage ovarian cancer survivors. Int. J. Gynecol. Cancer 2008, 18, 1183–1193. [Google Scholar] [CrossRef] [PubMed]
- Bodurka-Bevers, D.; Basen-Engquist, K.; Carmack, C.L.; Fitzgerald, M.A.; Wolf, J.K.; de Moor, C.; Gershenson, D.M. Depression, anxiety, and quality of life in patients with epithelial ovarian cancer. Gynecol. Oncol. 2000, 78, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Butow, P.N.; Price, M.A.; Bell, M.L.; Webb, P.M.; DeFazio, A.; Australian Ovarian Cancer Study Group; Australian Ovarian Cancer Study Quality of Life Study Investigators; Friedlander, M. Caring for women with ovarian cancer in the last year of life: A longitudinal study of caregiver quality of life, distress and unmet needs. Gynecol. Oncol. 2014, 132, 690–697. [Google Scholar] [PubMed]
- Van Nagell, J.R.; Depriest, P.D.; Gallion, H.H.; Pavlik, E.J. Ovarian cancer screening. Cancer 1993, 71, 1523–1528. [Google Scholar] [CrossRef] [PubMed]
- Maxim, L.D.; Niebo, R.; Utell, M.J. Screening tests: A review with examples. Inhal. Toxicol. 2014, 26, 811–828. [Google Scholar] [CrossRef] [PubMed]
- Van Nagell, J.R., Jr.; DePriest, P.D.; Ueland, F.R.; DeSimone, C.P.; Cooper, A.L.; McDonald, J.M.; Pavlik, E.J.; Kryscio, R.J. Ovarian cancer screening with annual transvaginal sonography: Findings of 25,000 women screened. Cancer 2007, 109, 1887–1896. [Google Scholar] [CrossRef] [PubMed]
- Van Nagell, J.R.; Gallion, H.H.; Pavlik, E.J.; DePriest, P.D. Ovarian cancer screening. Cancer 1995, 76, 2086–2091. [Google Scholar] [CrossRef]
- Pavlik, E.J.; Ueland, F.R.; Miller, R.W.; Ubellacker, J.M.; DeSimone, C.P.; Elder, J.; Hoff, J.; Baldwin, L.; Kryscio, R.J.; van Nagell, J.R., Jr. Frequency and disposition of ovarian abnormalities followed with serial transvaginal ultrasonography. Obstet. Gynecol. 2013, 122, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Van Nagell, J.R.; Hoff, J.T. Transvaginal ultrasonography in ovarian cancer screening: Current perspectives. Int. J. Women Health 2014, 6, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Elder, J.W.; Pavlik, E.J.; Long, A.; Miller, R.W.; DeSimone, C.P.; Hoff, J.T.; Ueland, W.R.; Kryscio, R.J.; van Nagell, J.R., Jr. Serial ultrasonographic evaluation of ovarian abnormalities with morphology index. Gynecol. Oncol. 2014, 135, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Buys, S.S.; Partridge, E.; Black, A.; Johnson, C.C.; Lamerato, L.; Isaacs, C.; Reding, D.J.; Greenlee, R.T.; Yokochi, L.A.; Kessel, B.; et al. Effect of screening on ovarian cancer mortality: The prostate, lung, colorectal and ovarian (PLCO) cancer screening randomized controlled trial. JAMA 2011, 305, 2295–2303. [Google Scholar] [CrossRef] [PubMed]
- Pinsky, P.F.; Yu, K.; Kramer, B.S.; Black, A.; Buys, S.S.; Partridge, E.; Gohagan, J.; Berg, C.D. Extended mortality results for ovarian cancer screening in the PLCO trial with median 15 years follow-up. Gynecol. Oncol. 2016, 135, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Skates, S.S. OCS: Development of the Risk of Ovarian Cancer Algorithm (ROCA) and ROCA screening trials. Int. J. Gynecol. Cancer 2012, 22, S24–S26. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.J.; Menon, U.; Ryan, A.; Gentry-Maharaj, A.; Burnell, A.; Kalsi, J.K.; Amso, N.N.; Apostolidou, S.; Benjamin, E.; Cruickshank, D.; et al. Ovarian cancer screening and mortality in the UK collaborative trial of ovarian cancer screening (UKCTOCS): A randomized controlled trial. Lancet 2016, 387, 945–956. [Google Scholar] [CrossRef]
- Wentzensen, N. Large ovarian cancer screening trial shows modest mortality reduction, but does not justify population-based ovarian cancer screening. Evid. Based Med. 2016, 21, 159. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Yamada, Y.; Sado, T.; Sakata, M.; Yoshida, S.; Kawaguchi, R.; Kanayama, S.; Shigetomi, J.; Haruta, S.; Tsuji, Y.; et al. A randomized study of screening for ovarian cancer: A multicenter study in Japan. Int. J. Gynecol. Cancer 2008, 18, 414–420. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Term | Screening Result | Findings |
|---|---|---|
| True Positive (TP) | Positive | Histologically-proven ovarian cancer |
| False Positive (FP) | Positive | Benign ovarian histology |
| True Negative (TN) | Negative | No evidence of ovarian cancer 12 months after a negative screen |
| False Negative (FN) | Negative | Ovarian cancer diagnosed within 12 months of a negative screen |
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, C.G. A Resident’s Perspective of Ovarian Cancer. Diagnostics 2017, 7, 24. https://doi.org/10.3390/diagnostics7020024
Smith CG. A Resident’s Perspective of Ovarian Cancer. Diagnostics. 2017; 7(2):24. https://doi.org/10.3390/diagnostics7020024
Chicago/Turabian StyleSmith, Christopher G. 2017. "A Resident’s Perspective of Ovarian Cancer" Diagnostics 7, no. 2: 24. https://doi.org/10.3390/diagnostics7020024
APA StyleSmith, C. G. (2017). A Resident’s Perspective of Ovarian Cancer. Diagnostics, 7(2), 24. https://doi.org/10.3390/diagnostics7020024