
Dynamic Contrast-Enhanced CT in Patients with Pancreatic Cancer

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
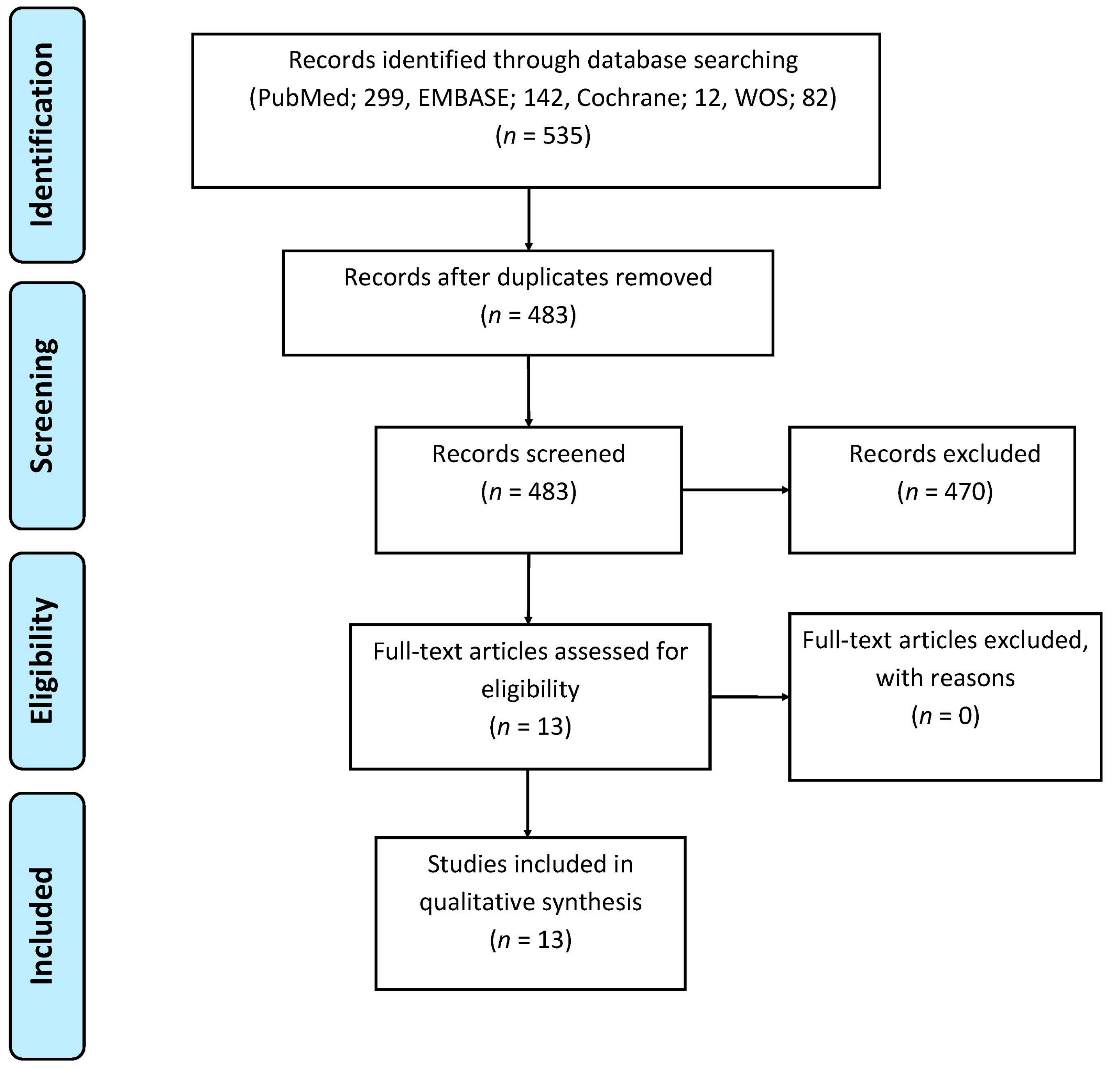
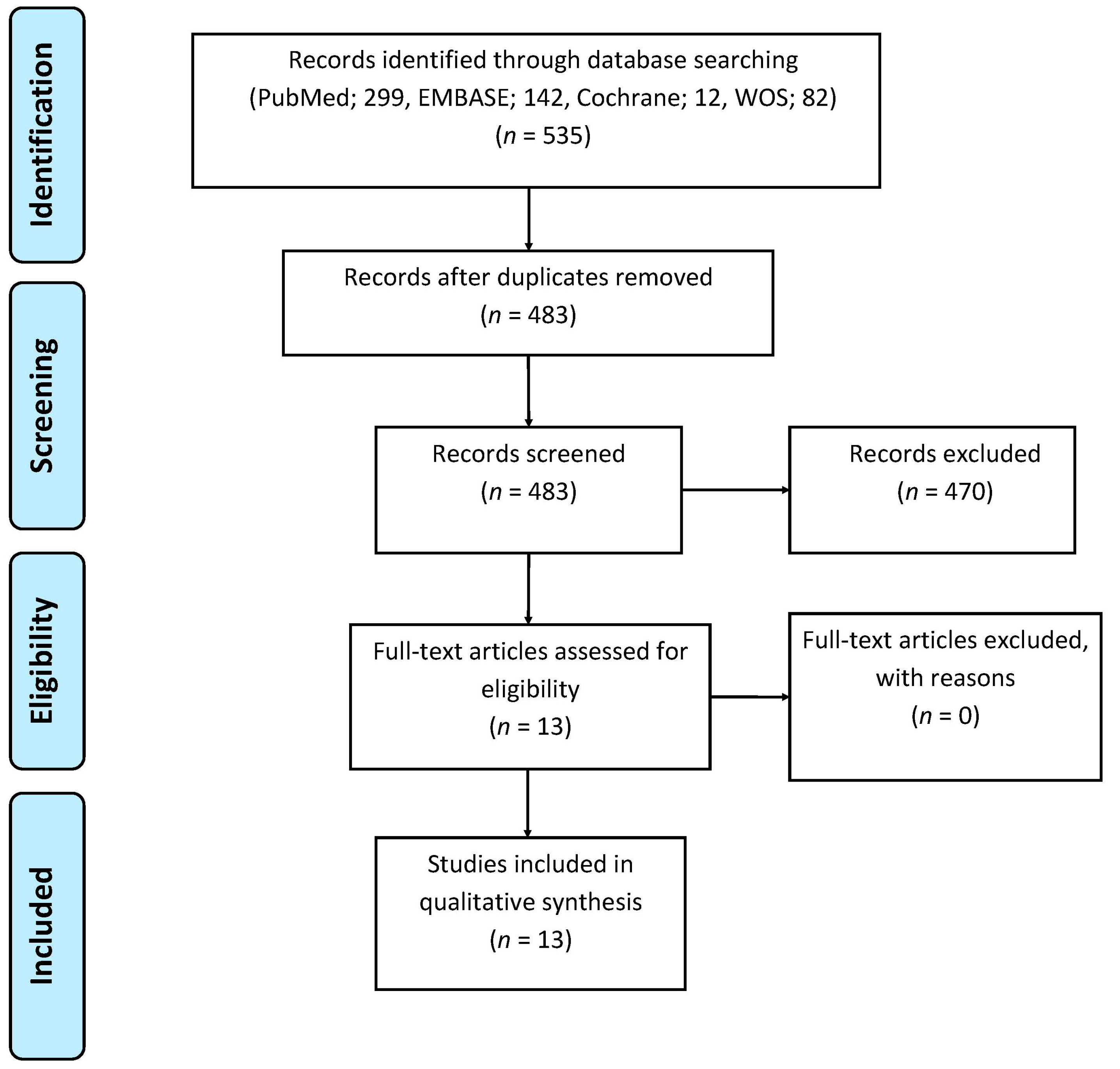
3.1. Study Selection and Division
3.2. Studies Concerning Primary Diagnosis and Staging
3.3. Study Concerning Tumor Response to Treatment
3.4. Studies Concerning Scan Techniques
3.5. Healthy Volunteers Included in the Studies Above
3.6. Risk of Bias and Applicability Concerns
4. Discussion
5. Conclusions
Conflicts of Interest
Abbreviations
| DCE-CT | Dynamic Contrast-Enhanced Computed Tomography |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| QUADAS | Quality Assessment of Diagnostic Accuracy Studies |
| MeSH | Medical Subject Headings |
Appendix A

{kind=link}
| Primary Diagnosis and Staging (All Studies were Prospective) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Authors, Publication Year | No. of Patients | Diagnosis | Scan Parameters | Kinetic Model | Aim | Gold Standard | Results | Conclusion | ||
| Slice | Contrast | kV and mAs | ||||||||
| D’Assignies et al. 2008 [18] | 28 | Pancreatic endocrine tumors | 64 | 40 mL | 100 kV, 100 mAs | Deconvolution/distributed parameter model | To correlate perfusion measurement with MVD and to determine whether perfusion parameters differ between tumor grades. | Histology, MVD, and WHO 2000 criteria † | Pancreatic endocrine tumors: BF tended to be higher in tumors than in pancreatic tissue outside of tumor (p < 0.06). Correlation with MVD: Tumor BF correlated with MVD (p < 0.001). Correlation with WHO: Significantly higher BF in WHO 1 tumors, than in WHO 2 and WHO 3 tumors (p = 0.02). | DCE-CT is feasible in patients with pancreatic endocrine tumors and allows evaluation of tumor angiogenesis. |
| Delrue et al. 2011 [19] | 40 | Pancreatic adenocarcinoma (n = 20) Normal pancreas in healthy volunteers (n = 20) | 128 Dual-source CT | 50 mL | 100 kV, 145 mAs | Maximum slope (single-compartment) | To assess perfusion characteristics in patients with pancreatic adenocarcinoma and to compare with values in normal healthy pancreatic tissue. | Histology | Pancreatic adenocarcinoma: Significantly lower BF, BV, and PS in the tumor center than in tumor rim and in pancreatic tissue outside of tumor (p < 0.05). Healthy volunteers: No significant differences in BF, BV, or PS in the different regions of the pancreas. Comparison-Patients with pancreatic adenocarcinoma and healthy volunteers: Significantly lower BF, BV, and PS in the tumor center compared with normal pancreatic tissue in healthy volunteers (p = 0.01). | DCE-CT provides added value when investigating tumor vascularization in pancreatic adenocarcinoma, compared with image assessment based on tissue density measurements (HU), and can lead to more accurate diagnosis. |
| Delrue et al. 2011 [20] | 54 | Pancreatic adenocarcinoma (n = 19), acute and chronic pancreatitis (n = 3 + 6), neuroendocrine tumors (n = 2), (pseudo)cystic lesions (n = 3), normal pancreas in healthy volunteers (n = 21) | 128 Dual-source CT | 50 mL | 100 kV, 145 mAs | Maximum slope (single-compartment) | To evaluate whether perfusion parameters can distinguish general pathologies of the pancreas and possibly aid in early diagnosis. | Histology | Pancreatic adenocarcinoma: Significantly lower BF and BV in the center of the tumor than in normal pancreatic tissue in healthy volunteers (BF and BV: p < 0.01). Neuroendocrine tumors: Significantly higher values for BF and BV in tumor tissue compared with normal pancreatic tissue in healthy volunteers (p < 0.01). Acute and chronic pancreatitis: Significantly lower BF and BV than in normal pancreatic tissue in healthy volunteers (p < 0.01) Healthy volunteers: No significant differences were found in BF, BV, and PS between head, body, and tail of the pancreas. | Significant decreases in perfusion values in both adenocarcinomas and acute and chronic pancreatitis, and the opposite applies to values in neuroendocrine tumors, which were significantly increased, compared to the control group of healthy volunteers. Different perfusion values can be used as an additional parameter to differentiate pancreatic pathologies. |
| D’Onofrio et al. 2012 [21] | 32 | Pancreatic adenocarcinoma. Pathological analysis; low grade (n = 12) and high grade (n = 20). | 64 | 50 mL | 120 kV, 150 mAs | Maximum slope (single-compartment) | To describe DCE-CT features and to assess whether these features correlate with the tumor grading. | Histology | Significantly lower median values of BV and PEI in high grade neoplasms compared with low grade neoplasms (BV: p ≤ 0.004 and PEI: p ≤ 0.012). | DCE-CT can predict tumor grade of pancreatic adenocarcinoma. |
| Kandel et al. 2009 [22] | 30 | Pancreatic adenocarcinoma | 320 | 60 mL | 100 kV, 22.5 mAs | Maximum slope (single-compartment) | To evaluate a whole-organ DCE-CT protocol and to analyze perfusion differences between tumor tissue and normal pancreatic tissue. | Histology | Significantly lower BF in tumor tissue compared with pancreatic tissue outside of tumor (p ≤ 0.01). | DCE-CT carries the potential to improve detection of pancreatic cancers due to the perfusion differences. |
| Klauss et al. 2012 [23] | 25 | Pancreatic adenocarcinoma | 64 Dual-source | 80 mL | 80 kV and 270 mAs 140 kV and 50 mAs | Patlak model (two-compartment) | To evaluate the feasibility of DCE-CT for assessing differences in perfusion values of tumor tissue and normal pancreatic tissue. | Histology | Significantly lower BF, BV, and PS in tumor tissue than in pancreatic tissue outside of tumor (p < 0.0001). Significantly higher BF in the head of the pancreas than in the tail, measured in pancreatic tissue outside of tumor (p = 0.007). | DCE-CT using the Patlak analysis is feasible. Even isodense tumors could be delineated in the color-coded parameter maps. |
| Lu et al. 2011 [24] | 112 | Pancreatic adenocarcinoma (n = 64), mass-forming chronic pancreatitis (n = 15). Normal pancreas in healthy volunteers (n = 33) | 64 | 50 mL | 80 kV, 50 mAs | Maximum slope (single-compartment) | To investigate characteristics of pancreatic cancer, mass-forming chronic pancreatitis, and normal pancreas with DCE-CT. | Histology and AJCC 2002 classification system * | Corrected p values < 0.016 were considered significant in this study. Pancreatic adenocarcinoma: Significantly lower BF and BV in tumor tissue compared with normal pancreatic tissue in healthy volunteers (p < 0.016). Significantly higher PS in pancreatic tissue outside of tumor than in normal pancreas in healthy volunteers (p < 0.016). Mass-forming chronic pancreatitis: Significantly lower BF and BV in mass-forming chronic pancreatitis than in normal pancreatic tissue in healthy volunteers (p < 0.016). Comparison –Pancreatic adenocarcinoma and mass-forming chronic pancreatitis: Significantly lower BF, BV, and PS values in pancreatic adenocarcinoma than in mass-forming chronic pancreatitis (p < .016). Healthy volunteers: No significant difference between the head, body, and tail of the pancreas. | DCE-CT is feasible in providing quantitative hemodynamic information of pancreatic adenocarcinoma and mass-forming chronic pancreatitis. |
| Nishikawa et al. 2014 [25] | 17 | Pancreatic adenocarcinoma | 64 | 40 mL | 80 kV, 20 mAs | Maximum slope (single-compartment) | To investigate the relationship between patient prognosis and perfusion in tumor tissue and peritumoral tissue. | Histology, TNM * and Japanese classification (prognosis) | Peritumoral tissue: Significant correlation between AUC peritumoral tissue (AUC of the Time Density Curve) or BF peritumoral tissue and survival days from the date on which perfusion CT was performed (AUC: p = 0.04, BF: 0.0005). Higher AUC peritumoral tissue and BF peritumoral tissue values were associated with shorter survival days. Tumor tissue: No significant correlation between BF and AUC in tumor tissue and survival days. | Patient prognosis may be related to perfusion in peritumoral tissue observed with DCE-CT. |
| Xu et al. 2009 [26] | 76 | Pancreatic adenocarcinoma (n = 40). Normal pancreatic tissue in patients with non-pancreatic disease (n = 36) | 64 | 50 mL | 120 kV, 150 mA (rotation time: N/A) | Deconvolution method | To explore the perfusion characteristics of pancreatic adenocarcinoma and normal pancreatic tissue in patients with non-pancreatic disease. | Histology | Pancreatic adenocarcinoma: Significant difference in BF, BV, and PS between tumor tissue, tumor rim, and peripheral pancreatic tissue in pancreatic adenocarcinoma, with gradually increased values from tumor tissue to tumor rim and peripheral pancreatic tissue (p < 0.02). Normal pancreas with non-pancreatic disease: No significant difference in BF, BV, or PS, between the head, neck, body, and tail. Comparison between patients with pancreatic adenocarcinoma and patients with non-pancreatic disease: Significantly lower values of BF, BV, tumor tissue, and tumor rim compared with normal pancreatic tissue in patients with non-pancreatic disease (p < 0.05). Significantly lower PS in tumor tissue compared with normal pancreatic tissue in patients with non-pancreatic disease (p < 0.05). Significantly higher PS in tumor rim and in peripheral pancreatic tissue of pancreatic adenocarcinoma compared with normal pancreatic tissue in patients with non-pancreatic disease (p < 0.05). | DCE-CT can differentiate pathological changes from normal tissue. Therefore, DCE-CT should be considered a potential modality to increase the accuracy of CT diagnosis for pancreatic adenocarcinoma. |
| Tumor Response to Treatment (Prospective Study) | ||||||||||||
| Authors, Publication Year | No. of Patients | Diagnosis | Scan Parameters | Kinetic Model | Aim | Treatment | DCE-CT Scans | Gold Standard | Results | Conclusion | ||
| Slice | Contrast | kV and mAs | ||||||||||
| Park et al. 2009 [27] | 30 | Pancreatic adenocarcinoma | 64 | 50 mL | 100 kV, 100 mAs | Patlak model (two-compartment) | To determine whether DCE-CT parameters, permeability and BV can be used to predict response to concurrent chemotherapy and radiation therapy (CCRT). | CCRT | Baseline. First follow-up: 4–6 weeks. Second follow-up: 10–12 weeks after first follow-up | WHO *, responders (complete or partial response: ≥50% decrease from baseline) and non-responders (progressive disease ≥25% increase in the size of lesion or the appearance of new lesions + those with no change) | First follow-up (n = 30): The baseline permeability value was significantly higher in responders than in non-responders (p = 0.001). No significant difference between baseline BV in responders and non-responders. Second follow-up (n = 18): The results were similar to the first follow-up. The baseline permeability value was significantly higher in responders than in non-responders (p = 0.002) | Tumors with high pretreatment permeability values indicating higher intratumoral flow tended to respond better to the CCRT. DCE-CT may be used to predict the tumor response of CCRT in patients with pancreatic cancer. |
| Scan Techniques (All Studies were Prospective) | ||||||||||||
| Authors, Publication Year | No. of Patients | Diagnosis | Scan Parameters | Kinetic Model | Aim | Gold Standard | Results | Conclusion | ||||
| Slice | Contrast | kV and mAs | ||||||||||
| Klauss et al. 2012 [28] | 24 | Pancreatic adenocarcinoma | 64 Dual-energy CT | 80 mL | 80 kV and 270 mAs 140 kV and 50 mAs | Patlak model (two-compartment) | To evaluate the feasibility of dual-energy DCE-CT for assessing the differences in BF, PS, and BV between pancreatic adenocarcinoma and normal pancreatic tissue. | Histology | BF, BV, and PS was significantly lower in tumor tissue than in pancreatic tissue outside of tumor, for both 80 kV, 140 kV, and weighted average 120 kV (BF, BV, and PS: p < 0.0001). | The use of dual-energy DCE-CT improves the accuracy of DCE-CT of the pancreas by fully exploiting the advantages of enhanced iodine contrast at 80 kV in combination with the noise reduction at 140 kV. Using dual-energy perfusion data could improve the delineation of pancreatic carcinomas. | ||
| Li et al. 2013 [29] | 33 | Pancreatic adenocarcinoma (n = 33) | N/A Dual-source CT | 50 mL | 70 kV and 120 mAs (<70 kg) 80 kV and 100 mAs (≥70 kg) | Patlak model (two-compartment) | To investigate the feasibility of low-dose whole pancreas DCE-CT. | Histology | Pancreatic adenocarcinoma: Significantly lower BF and BV in pancreatic adenocarcinoma compared to the normal pancreatic tissue (p < 0.001). Comparison between weight-dependent scan protocols: No significant difference in BF, BV, and PS in the normal pancreatic tissue between patients <70 kg and patients ≥70 kg. | The low-dose whole-organ DCE-CT of the pancreas can effectively reduce the radiation dose. | ||
| Tan et al. 2015 [30] | 67 | Pancreatic carcinoma (n = 27). Normal pancreas in healthy volunteers (n = 40) | 640 | 40 mL | 100 kV, 50 mA (rotation time: N/A) | Maximum slope (single-compartment) | To evaluate the feasibility of low-dose scanning: Compare changes of tissue peak and BF in normal tissue, lesions, and surrounding areas. Compare the use of the whole sequence (group 1), odd number (group 2), and even number (group 3). | Histology | Pancreatic carcinoma: Significantly lower tissue peak and BF in lesion areas of pancreatic cancer than in lesion-surrounding areas in group 1, 2, and 3 (p ≤ 0.001). Healthy volunteers: No significant difference between the three pancreatic regions no matter which sequence were applied. No significant difference between the three regions comparing the groups. | By using the method of low-dose whole pancreas perfusion, scan sequences, and radiation dose are halved, and the diagnosis capacity is not impaired. | ||
References
- American Cancer Society. Cancer Facts & Figures 2016; American Cancer Society: Atlanta, GA, USA, 2016. [Google Scholar]
- Balachandran, A.; Bhosale, P.R.; Charnsangavej, C.; Tamm, E.P. Imaging of pancreatic neoplasms. Surg. Oncol. Clin. N. Am. 2014, 23, 751–788. [Google Scholar] [CrossRef] [PubMed]
- Miura, F.; Takada, T.; Amano, H.; Yoshida, M.; Furui, S.; Takeshita, K. Diagnosis of pancreatic cancer. HPB (Oxford) 2006, 8, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goere, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the pancreas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. S5), v56–v68. [Google Scholar] [CrossRef] [PubMed]
- Galvin, A.; Sutherland, T.; Little, A.F. Part 1: CT characterisation of pancreatic neoplasms: A pictorial essay. Insight Imaging 2011, 2, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.S.; Lee, J.M. Imaging diagnosis of pancreatic cancer: A state-of-the-art review. World J. Gastroenterol. 2014, 20, 7864–7877. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Akishima-Fukasawa, Y.; Kobayashi, N.; Sano, T.; Kosuge, T.; Nimura, Y.; Kanai, Y.; Hiraoka, N. Prognostic value of tumor architecture, tumor-associated vascular characteristics, and expression of angiogenic molecules in pancreatic endocrine tumors. Clin. Cancer. Res. 2007, 13, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Raman, S.P.; Horton, K.M.; Fishman, E.K. Multimodality imaging of pancreatic cancer-computed tomography, magnetic resonance imaging, and positron emission tomography. Cancer J. 2012, 18, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Lei, G.W.; Wang, S.W.; Zheng, S.W.; Ge, Y.; Wei, F.C. Diagnostic value of CT perfusion imaging for parotid neoplasms. Dentomaxillofacial Radiol. 2014, 43, 20130237. [Google Scholar] [CrossRef] [PubMed]
- Cuenod, C.A.; Fournier, L.; Balvay, D.; Guinebretiere, J.M. Tumor angiogenesis: Pathophysiology and implications for contrast-enhanced mri and CT assessment. Abdom. Imaging 2006, 31, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Petralia, G.; Bonello, L.; Viotti, S.; Preda, L.; d’Andrea, G.; Bellomi, M. CT perfusion in oncology: How to do it. Cancer Imaging 2010, 10, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Figueiras, R.; Goh, V.J.; Padhani, A.R.; Baleato-Gonzalez, S.; Garrido, M.; Leon, L.; Gomez-Caamano, A. CT perfusion in oncologic imaging: A useful tool? Am. J. Roentgenol. 2013, 200, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A.; Lee, T.Y.; Goh, V.; Klotz, E.; Cuenod, C.; Bisdas, S.; Groves, A.M.; Hayball, M.P.; Alonzi, R.; Brunner, T. Current status and guidelines for the assessment of tumour vascular support with dynamic contrast-enhanced computed tomography. Eur. Radiol. 2012, 22, 1430–1441. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A. Molecular imaging with dynamic contrast-enhanced computed tomography. Clin. Radiol. 2010, 65, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Harders, S.W.; Balyasnikowa, S.; Fischer, B.M. Functional imaging in lung cancer. Clin. Physiol. Funct. Imaging 2014, 34, 340–355. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. Quadas-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- D’Assignies, G.; Couvelard, A.; Bahrami, S.; Vullierme, M.P.; Hammel, P.; Hentic, O.; Sauvanet, A.; Bedossa, P.; Ruszniewski, P.; Vilgrain, V. Pancreatic endocrine tumors: Tumor blood flow assessed with perfusion CT reflects angiogenesis and correlates with prognostic factors. Radiology 2009, 250, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Delrue, L.; Blanckaert, P.; Mertens, D.; Cesmeli, E.; Ceelen, W.P.; Duyck, P. Assessment of tumor vascularization in pancreatic adenocarcinoma using 128-slice perfusion computed tomography imaging. J. Comput. Assist. Tomogr. 2011, 35, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Delrue, L.; Blanckaert, P.; Mertens, D.; Van Meerbeeck, S.; Ceelen, W.; Duyck, P. Tissue perfusion in pathologies of the pancreas: Assessment using 128-slice computed tomography. Abdom. Imaging 2012, 37, 595–601. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, M.; Gallotti, A.; Mantovani, W.; Crosara, S.; Manfrin, E.; Falconi, M.; Ventriglia, A.; Zamboni, G.A.; Manfredi, R.; Pozzi Mucelli, R. Perfusion CT can predict tumoral grading of pancreatic adenocarcinoma. Eur. J. Radiol. 2013, 82, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Kandel, S.; Kloeters, C.; Meyer, H.; Hein, P.; Hilbig, A.; Rogalla, P. Whole-organ perfusion of the pancreas using dynamic volume CT in patients with primary pancreas carcinoma: Acquisition technique, post-processing and initial results. Eur. Radiol. 2009, 19, 2641–2646. [Google Scholar] [CrossRef] [PubMed]
- Klauss, M.; Stiller, W.; Fritz, F.; Kieser, M.; Werner, J.; Kauczor, H.U.; Grenacher, L. Computed tomography perfusion analysis of pancreatic carcinoma. J. Comput. Assist. Tomogr. 2012, 36, 237–242. [Google Scholar] [PubMed]
- Lu, N.; Feng, X.Y.; Hao, S.J.; Liang, Z.H.; Jin, C.; Qiang, J.W.; Guo, Q.Y. 64-slice CT perfusion imaging of pancreatic adenocarcinoma and mass-forming chronic pancreatitis. Acad. Radiol. 2011, 18, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, Y.; Tsuji, Y.; Isoda, H.; Kodama, Y.; Chiba, T. Perfusion in the tissue surrounding pancreatic cancer and the patient’s prognosis. BioMed. Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Liang, Z.; Hao, S.; Zhu, L.; Ashish, M.; Jin, C.; Fu, D.; Ni, Q. Pancreatic adenocarcinoma: Dynamic 64-slice helical CT with perfusion imaging. Abdom. Imaging 2009, 34, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Park, M.S.; Klotz, E.; Kim, M.J.; Song, S.Y.; Park, S.W.; Cha, S.W.; Lim, J.S.; Seong, J.; Chung, J.B.; Kim, K.W. Perfusion CT: Noninvasive surrogate marker for stratification of pancreatic cancer response to concurrent chemo- and radiation therapy. Radiology 2009, 250, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Klauss, M.; Stiller, W.; Pahn, G.; Fritz, F.; Kieser, M.; Werner, J.; Kauczor, H.U.; Grenacher, L. Dual-energy perfusion-CT of pancreatic adenocarcinoma. Eur. J. Radiol. 2013, 82, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Li, H.O.; Sun, C.; Xu, Z.D.; Miao, F.; Zhang, D.J.; Chen, J.H.; Li, X.; Wang, X.M.; Liu, C.; Zhao, B. Low-dose whole organ CT perfusion of the pancreas: Preliminary study. Abdom. Imaging 2014, 39, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Tan, Z.; Miao, Q.; Li, X.; Ren, K.; Zhao, Y.; Zhao, L.; Li, X.; Liu, Y.; Chai, R.; Xu, K. The primary study of low-dose pancreas perfusion by 640-slice helical CT: A whole-organ perfusion. Springerplus 2015, 4, 192. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, J.; Dai, J.; Feng, X.; Lu, H.; Zhou, C. Angiogenesis of renal cell carcinoma: Perfusion CT findings. Abdom. Imaging 2010, 35, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Kinney, T. Evidence-based imaging of pancreatic malignancies. Surg. Clin. N. Am. 2010, 90, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Horton, K.M.; Fishman, E.K. Adenocarcinoma of the pancreas: CT imaging. Radiol. Clin. N. Am. 2002, 40, 1263–1272. [Google Scholar] [CrossRef]
- Lundsgaard Hansen, M.; Norling, R.; Lauridsen, C.; Fallentin, E.; Bæksgaard, L.; Kofoed, K.F.; Svendsen, L.B.; Nielsen, M.B. Computed tomography (CT) perfusion in abdominal cancer: Technical aspects. Diagnostics 2013, 3, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Carmeliet, P.; Jain, R.K. Angiogenesis in cancer and other diseases. Nature 2000, 407, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Kambadakone, A.R.; Sahani, D.V. Body perfusion CT: Technique, clinical applications, and advances. Radiol. Clin. North Am. 2009, 47, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A. Perfusion CT for the assessment of tumour vascularity: Which protocol? Br. J. Radiol. 2003, 76, S36–S42. [Google Scholar] [CrossRef] [PubMed]
- Kenneth, A.; Miles, C.-A.C. Multidetector Computed Tomography in Oncology—CT Perfusion Imaging; Informa healthcare: Boca Raton, FL, USA, 2011. [Google Scholar]
- Kaufmann, S.; Schulze, M.; Horger, T.; Oelker, A.; Nikolaou, K.; Horger, M. Reproducibility of VPCT parameters in the normal pancreas: Comparison of two different kinetic calculation models. Acad. Radiol. 2015, 22, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A.; Griffiths, M.R. Perfusion CT: A worthwhile enhancement? Br. J. Radiol. 2003, 76, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Goh, V.; Dattani, M.; Farwell, J.; Shekhdar, J.; Tam, E.; Patel, S.; Juttla, J.; Simcock, I.; Stirling, J.; Mandeville, H.; et al. Radiation dose from volumetric helical perfusion CT of the thorax, abdomen or pelvis. Eur. Radiol. 2011, 21, 974–981. [Google Scholar] [CrossRef] [PubMed]
| Study | Risk of Bias | Applicability Concerns | |||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
| D’Assignies et al. 2008 [18] | |||||||
| Delrue et al. 2011 [19] | |||||||
| Delrue et al. 2011 [20] | |||||||
| D’Onofrio et al. 2012 [21] | |||||||
| Kandel et al. 2009 [22] | |||||||
| Klauss et al. 2012 [23] | |||||||
| Lu et al. 2011 [24] | |||||||
| Nishikawa et al. 2014 [25] | |||||||
| Xu et al. 2009 [26] | |||||||
| Park et al. 2009 [27] | |||||||
| Klauss et al. 2012 [28] | |||||||
| Li et al. 2013 [29] | |||||||
| Tan et al. 2015 [30] | |||||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eriksen, R.Ø.; Strauch, L.S.; Sandgaard, M.; Kristensen, T.S.; Nielsen, M.B.; Lauridsen, C.A. Dynamic Contrast-Enhanced CT in Patients with Pancreatic Cancer. Diagnostics 2016, 6, 34. https://doi.org/10.3390/diagnostics6030034
Eriksen RØ, Strauch LS, Sandgaard M, Kristensen TS, Nielsen MB, Lauridsen CA. Dynamic Contrast-Enhanced CT in Patients with Pancreatic Cancer. Diagnostics. 2016; 6(3):34. https://doi.org/10.3390/diagnostics6030034
Chicago/Turabian StyleEriksen, Rie Ø., Louise S. Strauch, Michael Sandgaard, Thomas S. Kristensen, Michael B. Nielsen, and Carsten A. Lauridsen. 2016. "Dynamic Contrast-Enhanced CT in Patients with Pancreatic Cancer" Diagnostics 6, no. 3: 34. https://doi.org/10.3390/diagnostics6030034
APA StyleEriksen, R. Ø., Strauch, L. S., Sandgaard, M., Kristensen, T. S., Nielsen, M. B., & Lauridsen, C. A. (2016). Dynamic Contrast-Enhanced CT in Patients with Pancreatic Cancer. Diagnostics, 6(3), 34. https://doi.org/10.3390/diagnostics6030034