
Arrhythmic Risk Stratification in Patients with Arrhythmogenic Cardiomyopathy

 , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Medical History
Sex Differences
3. Electrical Parameters
4. Diagnostics
4.1. Echocardiography
4.2. Cardiac Magnetic Resonance
4.3. Cardiac Computer Tomography
5. Ablative Treatment
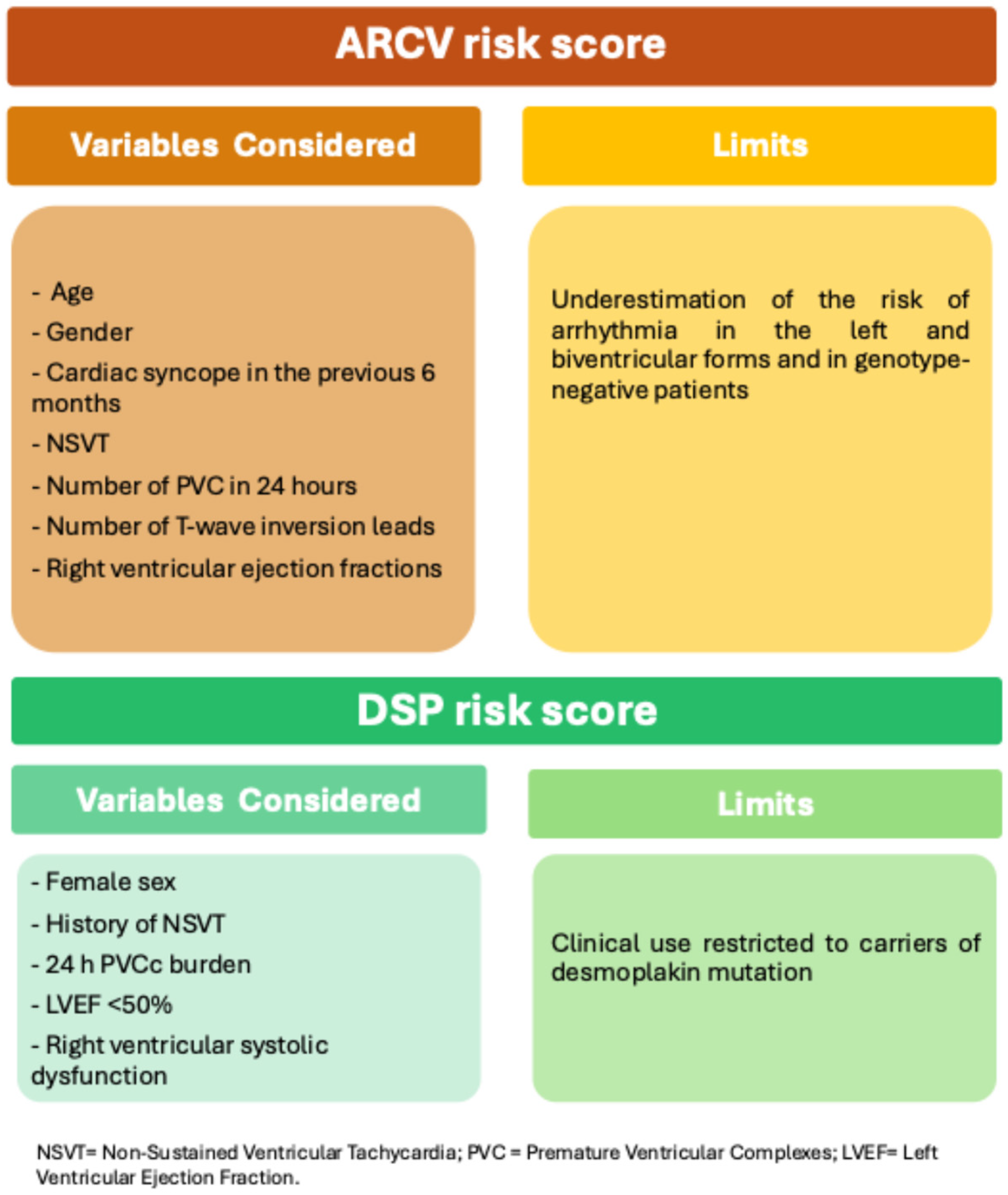
6. Risk Score
7. Genetics
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Basso, C.; Thiene, G.; Corrado, D.; Angelini, A.; Nava, A.; Valente, M. Arrhythmogenic right ventricular cardiomyopathy. Dysplasia, dystrophy, or myocarditis? Circulation 1996, 94, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Thiene, G.; Nava, A.; Corrado, D.; Rossi, L.; Pennelli, N. Right ventricular cardiomyopathy and sudden death in young people. N. Engl. J. Med. 1988, 318, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Marcus, F.I.; Fontaine, G.H.; Guiraudon, G.; Frank, R.; Laurenceau, J.L.; Malergue, C.; Grosgogeat, Y. Right ventricular dysplasia: A report of 24 adult cases. Circulation 1982, 65, 384–398. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Perazzolo Marra, M.; Zorzi, A.; Beffagna, G.; Cipriani, A.; Lazzari, M.; Migliore, F.; Pilichou, K.; Rampazzo, A.; Rigato, I.; et al. Diagnosis of arrhythmogenic cardiomyopathy: The Padua criteria. Int. J. Cardiol. 2020, 319, 106–114. [Google Scholar] [CrossRef]
- Corrado, D.; Basso, C.; Judge, D.P. Arrhythmogenic Cardiomyopathy. Circ. Res. 2017, 121, 784–802. [Google Scholar] [CrossRef]
- Bomma, C.; Rutberg, J.; Tandri, H.; Nasir, K.; Roguin, A.; Tichnell, C.; Rodriguez, R.; James, C.; Kasper, E.; Spevak, P.; et al. Misdiagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. J. Cardiovasc. Electrophysiol. 2004, 15, 300–306. [Google Scholar] [CrossRef]
- Peters, S.; Trümmel, M.; Meyners, W. Prevalence of right ventricular dysplasia-cardiomyopathy in a non-referral hospital. Int. J. Cardiol. 2004, 97, 499–501. [Google Scholar] [CrossRef]
- Mazzanti, A.; Ng, K.; Faragli, A.; Maragna, R.; Chiodaroli, E.; Orphanou, N.; Monteforte, N.; Memmi, M.; Gambelli, P.; Novelli, V.; et al. Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Course and Predictors of Arrhythmic Risk. J. Am. Coll. Cardiol. 2016, 68, 2540–2550. [Google Scholar] [CrossRef]
- Lie, Ø.H.; Rootwelt-Norberg, C.; Dejgaard, L.A.; Leren, I.S.; Stokke, M.K.; Edvardsen, T.; Haugaa, K.H. Prediction of Life-Threatening Ventricular Arrhythmia in Patients with Arrhythmogenic Cardiomyopathy: A Primary Prevention Cohort Study. JACC Cardiovasc. Imaging 2018, 11, 1377–1386. [Google Scholar] [CrossRef]
- Gandjbakhch, E.; Redheuil, A.; Pousset, F.; Charron, P.; Frank, R. Clinical Diagnosis, Imaging, and Genetics of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 784–804. [Google Scholar] [CrossRef]
- Varrenti, M.; Preda, A.; Frontera, A.; Baroni, M.; Gigli, L.; Vargiu, S.; Colombo, G.; Carbonaro, M.; Paolucci, M.; Giordano, F.; et al. Arrhythmogenic Cardiomyopathy: Definition, Classification and Arrhythmic Risk Stratification. J. Clin. Med. 2024, 13, 456. [Google Scholar] [CrossRef] [PubMed]
- Carrick, R.T.; De Marco, C.; Gasperetti, A.; Bosman, L.P.; Gourraud, J.B.; Trancuccio, A.; Mazzanti, A.; Murray, B.; Pendleton, C.; Tichnell, C.; et al. Implantable cardioverter defibrillator use in arrhythmogenic right ventricular cardiomyopathy in North America and Europe. Eur. Heart J. 2024, 45, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Castelletti, S.; Orini, M.; Vischer, A.S.; McKenna, W.J.; Lambiase, P.D.; Pantazis, A.; Crotti, L. Circadian and Seasonal Pattern of Arrhythmic Events in Arrhythmogenic Cardiomyopathy Patients. Int. J. Environ. Res. Public. Health 2023, 20, 2872. [Google Scholar] [CrossRef] [PubMed]
- Vicent, L.; Martínez-Sellés, M. Circadian rhythms, cardiac arrhythmias and sudden death. Front. Biosci. (Landmark Ed.) 2021, 26, 1305–1311. [Google Scholar] [CrossRef]
- McKenna, W.J.; Caforio, A.L.P. Myocardial Inflammation and Sudden Death in the Inherited Cardiomyopathies. Can. J. Cardiol. 2022, 38, 427–438. [Google Scholar] [CrossRef]
- Bariani, R.; Cipriani, A.; Rizzo, S.; Celeghin, R.; Bueno Marinas, M.; Giorgi, B.; De Gaspari, M.; Rigato, I.; Leoni, L.; Zorzi, A.; et al. ‘Hot phase’ clinical presentation in arrhythmogenic cardiomyopathy. Europace 2021, 23, 907–917. [Google Scholar] [CrossRef]
- Platonov, P.G.; Haugaa, K.H.; Bundgaard, H.; Svensson, A.; Gilljam, T.; Hansen, J.; Madsen, T.; Holst, A.G.; Carlson, J.; Lie, Ø.H.; et al. Primary Prevention of Sudden Cardiac Death with Implantable Cardioverter-Defibrillator Therapy in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy. Am. J. Cardiol. 2019, 123, 1156–1162. [Google Scholar] [CrossRef]
- Olivetti, N.Q.S.; Sacilotto, L.; Wulkan, F.; D’Arezzo Pessente, G.; Lombardi Peres de Carvalho, M.; Moleta, D.; Tessariol Hachul, D.; Veronese, P.; Hardy, C.; Pisani, C.; et al. Clinical Features, Genetic Findings, and Risk Stratification in Arrhythmogenic Right Ventricular Cardiomyopathy: Data From a Brazilian Cohort. Circ. Arrhythm. Electrophysiol. 2023, 16, e011391. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Maresi, E.; Coppola, G.; Rotolo, A.; Clemenza, F.; Giordano, U.; Lombardo, E.; Schicchi, R.; Torcivia, R.; Arrotti, S.; et al. Anatomical features and clinical correlations in Caucasian patients with definite arrhythmogenic right ventricular dysplasia/cardiomyopathy. Minerva Cardioangiol. 2014, 62, 369–378. [Google Scholar]
- Link, M.S.; Laidlaw, D.; Polonsky, B.; Zareba, W.; McNitt, S.; Gear, K.; Marcus, F.; Estes, N.A., 3rd. Ventricular arrhythmias in the North American multidisciplinary study of ARVC: Predictors, characteristics, and treatment. J. Am. Coll. Cardiol. 2014, 64, 119–125. [Google Scholar] [CrossRef]
- Roudijk, R.W.; Verheul, L.; Bosman, L.P.; Bourfiss, M.; Breur, J.; Slieker, M.G.; Blank, A.C.; Dooijes, D.; van der Heijden, J.F.; van den Heuvel, F.; et al. Clinical Characteristics and Follow-Up of Pediatric-Onset Arrhythmogenic Right Ventricular Cardiomyopathy. JACC Clin. Electrophysiol. 2022, 8, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Rootwelt-Norberg, C.; Lie, Ø.H.; Dejgaard, L.A.; Chivulescu, M.; Leren, I.S.; Edvardsen, T.; Haugaa, K.H. Life-threatening arrhythmic presentation in patients with arrhythmogenic cardiomyopathy before and after entering the genomic era; a two-decade experience from a large volume center. Int. J. Cardiol. 2019, 279, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Vega, A.M.; Kommata, V.; Svennblad, B.; Wisten, A.; Hagström, E.; Stattin, E.L. Family History and Warning Symptoms Precede Sudden Cardiac Death in Arrhythmogenic Right Ventricular Cardiomyopathy (from a Nationwide Study in Sweden). Am. J. Cardiol. 2022, 178, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Tichnell, C.; Murray, B.; Rizzo, S.; Te Riele, A.; Tandri, H.; Judge, D.P.; Thiene, G.; Basso, C.; Calkins, H.; et al. Comparison of Features of Fatal Versus Nonfatal Cardiac Arrest in Patients with Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy. Am. J. Cardiol. 2017, 120, 111–117. [Google Scholar] [CrossRef]
- Cappelletto, C.; Gregorio, C.; Barbati, G.; Romani, S.; De Luca, A.; Merlo, M.; Mestroni, L.; Stolfo, D.; Sinagra, G. Antiarrhythmic therapy and risk of cumulative ventricular arrhythmias in arrhythmogenic right ventricle cardiomyopathy. Int. J. Cardiol. 2021, 334, 58–64. [Google Scholar] [CrossRef]
- Kimura, Y.; Noda, T.; Otsuka, Y.; Wada, M.; Nakajima, I.; Ishibashi, K.; Miyamoto, K.; Okamura, H.; Aiba, T.; Kamakura, S.; et al. Potentially Lethal Ventricular Arrhythmias and Heart Failure in Arrhythmogenic Right Ventricular Cardiomyopathy: What Are the Differences Between Men and Women? JACC Clin. Electrophysiol. 2016, 2, 546–555. [Google Scholar] [CrossRef]
- Ren, J.; Chen, L.; Zhang, N.; Chen, X.; Zhao, Q.; Chen, K.; Li, X.; Ruschitzka, F.; Duru, F.; Song, J. Plasma testosterone and arrhythmic events in male patients with arrhythmogenic right ventricular cardiomyopathy. ESC Heart Fail. 2020, 7, 1547–1559. [Google Scholar] [CrossRef]
- Akdis, D.; Saguner, A.M.; Shah, K.; Wei, C.; Medeiros-Domingo, A.; von Eckardstein, A.; Lüscher, T.F.; Brunckhorst, C.; Chen, H.S.V.; Duru, F. Sex hormones affect outcome in arrhythmogenic right ventricular cardiomyopathy/dysplasia: From a stem cell derived cardiomyocyte-based model to clinical biomarkers of disease outcome. Eur. Heart J. 2017, 38, 1498–1508. [Google Scholar] [CrossRef]
- Lin, C.Y.; Chung, F.P.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Chao, T.F.; Liao, J.N.; Chang, Y.T.; et al. Gender differences in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy: Clinical manifestations, electrophysiological properties, substrate characteristics, and prognosis of radiofrequency catheter ablation. Int. J. Cardiol. 2017, 227, 930–937. [Google Scholar] [CrossRef]
- Rootwelt-Norberg, C.; Lie, Ø.H.; Chivulescu, M.; Castrini, A.I.; Sarvari, S.I.; Lyseggen, E.; Almaas, V.M.; Bogsrud, M.P.; Edvardsen, T.; Haugaa, K.H. Sex differences in disease progression and arrhythmic risk in patients with arrhythmogenic cardiomyopathy. Europace 2021, 23, 1084–1091. [Google Scholar] [CrossRef]
- Corrado, D.; Wichter, T.; Link, M.S.; Hauer, R.N.; Marchlinski, F.E.; Anastasakis, A.; Bauce, B.; Basso, C.; Brunckhorst, C.; Tsatsopoulou, A.; et al. Treatment of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: An International Task Force Consensus Statement. Circulation 2015, 132, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Bhonsale, A.; James, C.A.; Tichnell, C.; Murray, B.; Gagarin, D.; Philips, B.; Dalal, D.; Tedford, R.; Russell, S.D.; Abraham, T.; et al. Incidence and predictors of implantable cardioverter-defibrillator therapy in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy undergoing implantable cardioverter-defibrillator implantation for primary prevention. J. Am. Coll. Cardiol. 2011, 58, 1485–1496. [Google Scholar] [CrossRef] [PubMed]
- Bosman, L.P.; Sammani, A.; James, C.A.; Cadrin-Tourigny, J.; Calkins, H.; van Tintelen, J.P.; Hauer, R.N.W.; Asselbergs, F.W.; Te Riele, A. Predicting arrhythmic risk in arrhythmogenic right ventricular cardiomyopathy: A systematic review and meta-analysis. Heart Rhythm. 2018, 15, 1097–1107. [Google Scholar] [CrossRef]
- Zorzi, A.; Migliore, F.; Elmaghawry, M.; Silvano, M.; Marra, M.P.; Niero, A.; Nguyen, K.; Rigato, I.; Bauce, B.; Basso, C.; et al. Electrocardiographic predictors of electroanatomic scar size in arrhythmogenic right ventricular cardiomyopathy: Implications for arrhythmic risk stratification. J. Cardiovasc. Electrophysiol. 2013, 24, 1321–1327. [Google Scholar] [CrossRef]
- Svensson, A.; Jensen, H.K.; Boonstra, M.J.; Tétreault-Langlois, M.; Dahlberg, P.; Bundgaard, H.; Christensen, A.H.; Rylance, R.T.; Svendsen, J.H.; Cadrin-Tourigny, J.; et al. Natural Course of Electrocardiographic Features in Arrhythmogenic Right Ventricular Cardiomyopathy and Their Relation to Ventricular Arrhythmic Events. J. Am. Heart Assoc. 2024, 13, e031893. [Google Scholar] [CrossRef]
- Saguner, A.M.; Ganahl, S.; Baldinger, S.H.; Kraus, A.; Medeiros-Domingo, A.; Nordbeck, S.; Saguner, A.R.; Mueller-Burri, A.S.; Haegeli, L.M.; Wolber, T.; et al. Usefulness of electrocardiographic parameters for risk prediction in arrhythmogenic right ventricular dysplasia. Am. J. Cardiol. 2014, 113, 1728–1734. [Google Scholar] [CrossRef]
- Vischer, A.S.; Castelletti, S.; Syrris, P.; McKenna, W.J.; Pantazis, A. Heart failure in patients with arrhythmogenic right ventricular cardiomyopathy: Genetic characteristics. Int. J. Cardiol. 2019, 286, 99–103. [Google Scholar] [CrossRef]
- Klingenheben, T.; Zabel, M.; D’Agostino, R.B.; Cohen, R.J.; Hohnloser, S.H. Predictive value of T-wave alternans for arrhythmic events in patients with congestive heart failure. Lancet 2000, 356, 651–652. [Google Scholar] [CrossRef]
- Chung, F.P.; Lin, Y.J.; Chong, E.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Chao, T.F.; Liao, J.N.; Chen, S.A. The Application of Ambulatory Electrocardiographically-Based T-Wave Alternans in Patients with Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy. Can. J. Cardiol. 2016, 32, 1355.e15–1355.e22. [Google Scholar] [CrossRef]
- Peters, S.; Truemmel, M.; Koehler, B. Prognostic value of QRS fragmentation in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. J. Cardiovasc. Med. 2012, 13, 295–298. [Google Scholar] [CrossRef]
- Canpolat, U.; Kabakçi, G.; Aytemir, K.; Dural, M.; Sahiner, L.; Yorgun, H.; Sunman, H.; Bariş Kaya, E.; Tokgözoğlu, L.; Oto, A. Fragmented QRS complex predicts the arrhythmic events in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. J. Cardiovasc. Electrophysiol. 2013, 24, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Santangeli, P.; Dello Russo, A.; Pieroni, M.; Casella, M.; Di Biase, L.; Burkhardt, J.D.; Sanchez, J.; Lakkireddy, D.; Carbucicchio, C.; Zucchetti, M.; et al. Fragmented and delayed electrograms within fibrofatty scar predict arrhythmic events in arrhythmogenic right ventricular cardiomyopathy: Results from a prospective risk stratification study. Heart Rhythm. 2012, 9, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Turrini, P.; Corrado, D.; Basso, C.; Nava, A.; Bauce, B.; Thiene, G. Dispersion of ventricular depolarization-repolarization: A noninvasive marker for risk stratification in arrhythmogenic right ventricular cardiomyopathy. Circulation 2001, 103, 3075–3080. [Google Scholar] [CrossRef] [PubMed]
- Folino, A.F.; Buja, G.; Bauce, B.; Thiene, G.; dalla Volta, S.; Nava, A. Heart rate variability in arrhythmogenic right ventricular cardiomyopathy correlation with clinical and prognostic features. Pacing Clin. Electrophysiol. 2002, 25, 1285–1292. [Google Scholar] [CrossRef]
- Battipaglia, I.; Scalone, G.; Macchione, A.; Pinnacchio, G.; Laurito, M.; Milo, M.; Pelargonio, G.; Bencardino, G.; Bellocci, F.; Pieroni, M.; et al. Association of heart rate variability with arrhythmic events in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. Circ. J. 2012, 76, 618–623. [Google Scholar] [CrossRef]
- Wang, W.; Cadrin-Tourigny, J.; Bhonsale, A.; Tichnell, C.; Murray, B.; Monfredi, O.; Chrispin, J.; Crosson, J.; Tandri, H.; James, C.A.; et al. Arrhythmic outcome of arrhythmogenic right ventricular cardiomyopathy patients without implantable defibrillators. J. Cardiovasc. Electrophysiol. 2018, 29, 1396–1402. [Google Scholar] [CrossRef]
- Migliore, F.; Zorzi, A.; Silvano, M.; Bevilacqua, M.; Leoni, L.; Marra, M.P.; Elmaghawry, M.; Brugnaro, L.; Dal Lin, C.; Bauce, B.; et al. Prognostic value of endocardial voltage mapping in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. Circ. Arrhythm. Electrophysiol. 2013, 6, 167–176. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) Endorsed by the Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Haugaa, K.H.; Basso, C.; Badano, L.P.; Bucciarelli-Ducci, C.; Cardim, N.; Gaemperli, O.; Galderisi, M.; Habib, G.; Knuuti, J.; Lancellotti, P.; et al. Comprehensive multi-modality imaging approach in arrhythmogenic cardiomyopathy-an expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 237–253. [Google Scholar] [CrossRef]
- Leren, I.S.; Saberniak, J.; Haland, T.F.; Edvardsen, T.; Haugaa, K.H. Combination of ECG and Echocardiography for Identification of Arrhythmic Events in Early ARVC. JACC Cardiovasc. Imaging 2017, 10, 503–513. [Google Scholar] [CrossRef]
- te Riele, A.S.; Bhonsale, A.; James, C.A.; Rastegar, N.; Murray, B.; Burt, J.R.; Tichnell, C.; Madhavan, S.; Judge, D.P.; Bluemke, D.A.; et al. Incremental value of cardiac magnetic resonance imaging in arrhythmic risk stratification of arrhythmogenic right ventricular dysplasia/cardiomyopathy-associated desmosomal mutation carriers. J. Am. Coll. Cardiol. 2013, 62, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; De Luca, A.; Cappelletto, C.; Raimondi, F.; Bianco, F.; Botto, N.; Lesizza, P.; Grigoratos, C.; Minati, M.; Dell’Omodarme, M.; et al. Prognostic Value of Magnetic Resonance Phenotype in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy. J. Am. Coll. Cardiol. 2020, 75, 2753–2765. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.; Erhart, L.; Anwer, S.; Heiniger, P.S.; Winkler, N.E.; Cimen, T.; Kuzo, N.; Hess, R.; Akdis, D.; Costa, S.; et al. Tissue Doppler echocardiography and outcome in arrhythmogenic right ventricular cardiomyopathy. Int. J. Cardiol. 2022, 368, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Kirkels, F.P.; Rootwelt-Norberg, C.; Bosman, L.P.; Aabel, E.W.; Muller, S.A.; Castrini, A.I.; Taha, K.; van Osta, N.; Lie, Ø.H.; Asselbergs, F.W.; et al. The added value of abnormal regional myocardial function for risk prediction in arrhythmogenic right ventricular cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1710–1718. [Google Scholar] [CrossRef]
- Cadrin-Tourigny, J.; Bosman, L.P.; Nozza, A.; Wang, W.; Tadros, R.; Bhonsale, A.; Bourfiss, M.; Fortier, A.; Lie, Ø.H.; Saguner, A.M.; et al. A new prediction model for ventricular arrhythmias in arrhythmogenic right ventricular cardiomyopathy. Eur. Heart J. 2019, 40, 1850–1858. [Google Scholar] [CrossRef]
- Mast, T.P.; Taha, K.; Cramer, M.J.; Lumens, J.; van der Heijden, J.F.; Bouma, B.J.; van den Berg, M.P.; Asselbergs, F.W.; Doevendans, P.A.; Teske, A.J. The Prognostic Value of Right Ventricular Deformation Imaging in Early Arrhythmogenic Right Ventricular Cardiomyopathy. JACC Cardiovasc. Imaging 2019, 12, 446–455. [Google Scholar] [CrossRef]
- Segura-Rodríguez, D.; Bermúdez-Jiménez, F.J.; González-Camacho, L.; Moreno Escobar, E.; García-Orta, R.; Alcalá-López, J.E.; Bautista Pavés, A.; Oyonarte-Ramírez, J.M.; López-Fernández, S.; Álvarez, M.; et al. Layer-Specific Global Longitudinal Strain Predicts Arrhythmic Risk in Arrhythmogenic Cardiomyopathy. Front. Cardiovasc. Med. 2021, 8, 748003. [Google Scholar] [CrossRef]
- Grimault, D.; Serfaty, J.M.; Guyomarch, B.; Marteau, L.; Goudal, A.; Schmitt, S.; Warin-Fresse, K.; Clero, S.; Fellah, I.; Thollet, A.; et al. Description of the Two-Dimensional Layer-Specific Strain Echocardiography Phenotype of Arrhythmogenic Left Ventricular Cardiomyopathy. J. Am. Soc. Echocardiogr. 2024, 37, 960–970. [Google Scholar] [CrossRef]
- Deac, M.; Alpendurada, F.; Fanaie, F.; Vimal, R.; Carpenter, J.P.; Dawson, A.; Miller, C.; Roussin, I.; di Pietro, E.; Ismail, T.F.; et al. Prognostic value of cardiovascular magnetic resonance in patients with suspected arrhythmogenic right ventricular cardiomyopathy. Int. J. Cardiol. 2013, 168, 3514–3521. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Pingitore, A.; Di Bella, G.; Piaggi, P.; Gaeta, R.; Grigoratos, C.; Altinier, A.; Pantano, A.; Strata, E.; De Caterina, R.; et al. Prognostic Role of Cardiac Magnetic Resonance in Arrhythmogenic Right Ventricular Cardiomyopathy. Am. J. Cardiol. 2018, 122, 1745–1753. [Google Scholar] [CrossRef]
- Feliu, E.; Moscicki, R.; Carrillo, L.; García-Fernández, A.; Martínez Martínez, J.G.; Ruiz-Nodar, J.M. Importance of cardiac magnetic resonance findings in the diagnosis of left dominant arrythmogenic cardiomyopathy. Rev. Española De Cardiol. (Engl. Ed.) 2020, 73, 885–892. [Google Scholar] [CrossRef]
- Marra, M.P.; Leoni, L.; Bauce, B.; Corbetti, F.; Zorzi, A.; Migliore, F.; Silvano, M.; Rigato, I.; Tona, F.; Tarantini, G.; et al. Imaging study of ventricular scar in arrhythmogenic right ventricular cardiomyopathy: Comparison of 3D standard electroanatomical voltage mapping and contrast-enhanced cardiac magnetic resonance. Circ. Arrhythm. Electrophysiol. 2012, 5, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Castrichini, M.; De Luca, A.; De Angelis, G.; Neves, R.; Paldino, A.; Dal Ferro, M.; Barbati, G.; Medo, K.; Barison, A.; Grigoratos, C.; et al. Magnetic Resonance Imaging Characterization and Clinical Outcomes of Dilated and Arrhythmogenic Left Ventricular Cardiomyopathies. J. Am. Coll. Cardiol. 2024, 83, 1841–1851. [Google Scholar] [CrossRef] [PubMed]
- Parisi, V.; Graziosi, M.; Lopes, L.R.; De Luca, A.; Pasquale, F.; Tini, G.; Targetti, M.; Cueto, M.R.; Moura, A.R.; Ditaranto, R.; et al. Arrhythmic risk stratification in patients with left ventricular ring-like scar. Eur. J. Prev. Cardiol. 2024; in press. [Google Scholar] [CrossRef]
- Yang, Y.; Wei, X.; Lu, G.; Xie, J.; Tan, Z.; Du, Z.; Ye, W.; Xu, H.; Li, X.; Liu, E.; et al. Ringlike late gadolinium enhancement provides incremental prognostic value in non-classical arrhythmogenic cardiomyopathy. J. Cardiovasc. Magn. Reson. 2023, 25, 72. [Google Scholar] [CrossRef]
- Lu, G.; Cao, L.; Ye, W.; Wei, X.; Xie, J.; Du, Z.; Zhang, X.; Luo, X.; Ou, J.; Zhang, Q.; et al. Incremental Prognostic Value of Cardiac MRI Feature Tracking and T1 Mapping in Arrhythmogenic Right Ventricular Cardiomyopathy. Radiol. Cardiothorac. Imaging 2024, 6, e230430. [Google Scholar] [CrossRef]
- Augustine, D.; Lewandowski, A.J.; Lazdam, M.; Rai, A.; Francis, J.; Myerson, S.; Noble, A.; Becher, H.; Neubauer, S.; Petersen, S.E.; et al. Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: Comparison with tagging and relevance of gender. J. Cardiovasc. Magn. Reson. 2013, 15, 8. [Google Scholar] [CrossRef]
- Song, Y.; Li, L.; Chen, X.; Ji, K.; Lu, M.; Hauer, R.; Chen, L.; Zhao, S. Left Ventricular Longitudinal Dyssynchrony by CMR Feature Tracking Is Related to Adverse Prognosis in Advanced Arrhythmogenic Cardiomyopathy. Front. Cardiovasc. Med. 2021, 8, 712832. [Google Scholar] [CrossRef]
- Yu, L.Y.; Xiang, J.Y.; Chen, B.H.; An, D.A.; Wu, R.; Shi, R.Y.; Zheng, J.Y.; Zhao, L.; Wu, L.M. Prognostic value of magnetic resonance imaging (MRI)-based cardiac adipose tissue in arrhythmogenic right ventricular cardiomyopathy. Clin. Radiol. 2025, 81, 106708. [Google Scholar] [CrossRef]
- Ma, N.; Cheng, H.; Lu, M.; Jiang, S.; Yin, G.; Zhao, S. Cardiac magnetic resonance imaging in arrhythmogenic right ventricular cardiomyopathy: Correlation to the QRS dispersion. Magn. Reson. Imaging 2012, 30, 1454–1460. [Google Scholar] [CrossRef]
- Aliyari Ghasabeh, M.; Te Riele, A.; James, C.A.; Chen, H.S.V.; Tichnell, C.; Murray, B.; Eng, J.; Kral, B.G.; Tandri, H.; Calkins, H.; et al. Epicardial Fat Distribution Assessed with Cardiac CT in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy. Radiology 2018, 289, 641–648. [Google Scholar] [CrossRef]
- Aziz, W.; Claridge, S.; Ntalas, I.; Gould, J.; de Vecchi, A.; Razeghi, O.; Toth, D.; Mountney, P.; Preston, R.; Rinaldi, C.A.; et al. Emerging role of cardiac computed tomography in heart failure. ESC Heart Fail. 2019, 6, 909–920. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, Y.; Jadidi, A.; Sacher, F.; Denis, A.; Daly, M.; Derval, N.; Shah, A.; Lehrmann, H.; Park, C.I.; Weber, R.; et al. Relationship between MDCT-imaged myocardial fat and ventricular tachycardia substrate in arrhythmogenic right ventricular cardiomyopathy. J. Am. Heart Assoc. 2014, 3, e000935. [Google Scholar] [CrossRef] [PubMed]
- Ustunkaya, T.; Desjardins, B.; Wedan, R.; Chahal, C.A.A.; Zimmerman, S.L.; Saju, N.; Zahid, S.; Sharma, A.; Han, Y.; Trayanova, N.; et al. Epicardial Conduction Speed, Electrogram Abnormality, and Computed Tomography Attenuation Associations in Arrhythmogenic Right Ventricular Cardiomyopathy. JACC Clin. Electrophysiol. 2019, 5, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; de Boer, R.A.; et al. 2023 ESC Guidelines for the management of cardiomyopathies: Developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur. Heart J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef]
- Christiansen, M.K.; Haugaa, K.H.; Svensson, A.; Gilljam, T.; Madsen, T.; Hansen, J.; Holst, A.G.; Bundgaard, H.; Edvardsen, T.; Svendsen, J.H.; et al. Incidence, Predictors, and Success of Ventricular Tachycardia Catheter Ablation in Arrhythmogenic Right Ventricular Cardiomyopathy (from the Nordic ARVC Registry). Am. J. Cardiol. 2020, 125, 803–811. [Google Scholar] [CrossRef]
- Berruezo, A.; Acosta, J.; Fernández-Armenta, J.; Pedrote, A.; Barrera, A.; Arana-Rueda, E.; Bodegas, A.I.; Anguera, I.; Tercedor, L.; Penela, D.; et al. Safety, long-term outcomes and predictors of recurrence after first-line combined endoepicardial ventricular tachycardia substrate ablation in arrhythmogenic cardiomyopathy. Impact of arrhythmic substrate distribution pattern. A prospective multicentre study. Europace 2017, 19, 607–616. [Google Scholar] [CrossRef]
- Lin, C.Y.; Chung, F.P.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Chao, T.F.; Liao, J.N.; Chang, T.Y.; et al. Clinical significance of structural remodeling concerning substrate characteristics and outcomes in arrhythmogenic right ventricular cardiomyopathy. Heart Rhythm O2 2022, 3, 422–429. [Google Scholar] [CrossRef]
- Shen, L.; Liu, S.; Zhang, Z.; Xiong, Y.; Lai, Z.; Hu, F.; Zheng, L.; Yao, Y. Catheter ablation of ventricular tachycardia in patients with arrhythmogenic right ventricular cardiomyopathy and biventricular involvement. Europace 2024, 26, euae059. [Google Scholar] [CrossRef]
- Peters, S.; Peters, H.; Thierfelder, L. Risk stratification of sudden cardiac death and malignant ventricular arrhythmias in right ventricular dysplasia-cardiomyopathy. Int. J. Cardiol. 1999, 71, 243–250. [Google Scholar] [CrossRef]
- Jordà, P.; Bosman, L.P.; Gasperetti, A.; Mazzanti, A.; Gourraud, J.B.; Davies, B.; Frederiksen, T.C.; Weidmann, Z.M.; Di Marco, A.; Roberts, J.D.; et al. Arrhythmic risk prediction in arrhythmogenic right ventricular cardiomyopathy: External validation of the arrhythmogenic right ventricular cardiomyopathy risk calculator. Eur. Heart J. 2022, 43, 3041–3052. [Google Scholar] [CrossRef]
- Carrick, R.T.; Te Riele, A.; Gasperetti, A.; Bosman, L.; Muller, S.A.; Pendleton, C.; Tichnell, C.; Murray, B.; Yap, S.C.; van den Berg, M.P.; et al. Longitudinal Prediction of Ventricular Arrhythmic Risk in Patients with Arrhythmogenic Right Ventricular Cardiomyopathy. Circ. Arrhythm. Electrophysiol. 2022, 15, e011207. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Gasperetti, A.; Gaetano, F.; Busana, M.; Sommariva, E.; Catto, V.; Sicuso, R.; Rizzo, S.; Conte, E.; Mushtaq, S.; et al. Long-term follow-up analysis of a highly characterized arrhythmogenic cardiomyopathy cohort with classical and non-classical phenotypes-a real-world assessment of a novel prediction model: Does the subtype really matter. Europace 2020, 22, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Protonotarios, A.; Bariani, R.; Cappelletto, C.; Pavlou, M.; García-García, A.; Cipriani, A.; Protonotarios, I.; Rivas, A.; Wittenberg, R.; Graziosi, M.; et al. Importance of genotype for risk stratification in arrhythmogenic right ventricular cardiomyopathy using the 2019 ARVC risk calculator. Eur. Heart J. 2022, 43, 3053–3067. [Google Scholar] [CrossRef]
- Martini, M.; Rigato, I.; Masini, M.; De Lazzari, M.; Mattesi, G.; Pilichou, K.; Pittorru, R.; Migliore, F.; Bauce, B. Risk stratification in arrhythmogenic cardiomyopathy: Scoring or personalized medicine? Eur. Heart J. Suppl. 2025, 27, i36–i39. [Google Scholar] [CrossRef]
- Carrick, R.T.; Gasperetti, A.; Protonotarios, A.; Murray, B.; Laredo, M.; van der Schaaf, I.; Dooijes, D.; Syrris, P.; Cannie, D.; Tichnell, C.; et al. A novel tool for arrhythmic risk stratification in desmoplakin gene variant carriers. Eur. Heart J. 2024, 45, 2968–2979. [Google Scholar] [CrossRef]
- de Brouwer, R.; Bosman, L.P.; Gripenstedt, S.; Wilde, A.A.M.; van den Berg, M.P.; Peter van Tintelen, J.; de Boer, R.A.; Te Riele, A. Value of genetic testing in the diagnosis and risk stratification of arrhythmogenic right ventricular cardiomyopathy. Heart Rhythm. 2022, 19, 1659–1665. [Google Scholar] [CrossRef]
- Corrado, D.; Anastasakis, A.; Basso, C.; Bauce, B.; Blomström-Lundqvist, C.; Bucciarelli-Ducci, C.; Cipriani, A.; De Asmundis, C.; Gandjbakhch, E.; Jiménez-Jáimez, J.; et al. Proposed diagnostic criteria for arrhythmogenic cardiomyopathy: European Task Force consensus report. Int. J. Cardiol. 2024, 395, 131447. [Google Scholar] [CrossRef]
- Mazzanti, A.; Kukavica, D.; Trancuccio, A.; Scilabra, G.G.; Coppini, L.; Pergola, V.; Tempo, E.; Pili, G.; Napolitano, C.; Priori, S.G. Genetics in arrhythmogenic cardiomyopathies: Where are we now and where are we heading to? Eur. Heart J. Suppl. 2025, 27, i98–i102. [Google Scholar] [CrossRef]
- Gasperetti, A.; Carrick, R.; Protonotarios, A.; Laredo, M.; van der Schaaf, I.; Syrris, P.; Murray, B.; Tichnell, C.; Cappelletto, C.; Gigli, M.; et al. Long-Term Arrhythmic Follow-Up and Risk Stratification of Patients with Desmoplakin-Associated Arrhythmogenic Right Ventricular Cardiomyopathy. JACC Adv. 2024, 3, 100832. [Google Scholar] [CrossRef]
- Castelletti, S.; Vischer, A.S.; Syrris, P.; Crotti, L.; Spazzolini, C.; Ghidoni, A.; Parati, G.; Jenkins, S.; Kotta, M.C.; McKenna, W.J.; et al. Desmoplakin missense and non-missense mutations in arrhythmogenic right ventricular cardiomyopathy: Genotype-phenotype correlation. Int. J. Cardiol. 2017, 249, 268–273. [Google Scholar] [CrossRef]
- Di Lorenzo, F.; Marchionni, E.; Ferradini, V.; Latini, A.; Pezzoli, L.; Martino, A.; Romeo, F.; Iorio, A.; Bianchi, S.; Iascone, M.; et al. DSP-Related Cardiomyopathy as a Distinct Clinical Entity? Emerging Evidence from an Italian Cohort. Int. J. Mol. Sci. 2023, 24, 2490. [Google Scholar] [CrossRef] [PubMed]
- Bhonsale, A.; Groeneweg, J.A.; James, C.A.; Dooijes, D.; Tichnell, C.; Jongbloed, J.D.; Murray, B.; te Riele, A.S.; van den Berg, M.P.; Bikker, H.; et al. Impact of genotype on clinical course in arrhythmogenic right ventricular dysplasia/cardiomyopathy-associated mutation carriers. Eur. Heart J. 2015, 36, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.H.; Platonov, P.G.; Jensen, H.K.; Chivulescu, M.; Svensson, A.; Dahlberg, P.; Madsen, T.; Frederiksen, T.C.; Heliö, T.; Lie, Ø.H.; et al. Genotype-phenotype correlation in arrhythmogenic right ventricular cardiomyopathy-risk of arrhythmias and heart failure. J. Med. Genet. 2022, 59, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Hermida, A.; Fressart, V.; Hidden-Lucet, F.; Donal, E.; Probst, V.; Deharo, J.C.; Chevalier, P.; Klug, D.; Mansencal, N.; Delacretaz, E.; et al. High risk of heart failure associated with desmoglein-2 mutations compared to plakophilin-2 mutations in arrhythmogenic right ventricular cardiomyopathy/dysplasia. Eur. J. Heart Fail. 2019, 21, 792–800. [Google Scholar] [CrossRef]
- Rigato, I.; Bauce, B.; Rampazzo, A.; Zorzi, A.; Pilichou, K.; Mazzotti, E.; Migliore, F.; Marra, M.P.; Lorenzon, A.; De Bortoli, M.; et al. Compound and digenic heterozygosity predicts lifetime arrhythmic outcome and sudden cardiac death in desmosomal gene-related arrhythmogenic right ventricular cardiomyopathy. Circ. Cardiovasc. Genet. 2013, 6, 533–542. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Right Ventricle | Left Ventricle | |
|---|---|---|
| Morpho-functional ventricular abnormalities | Major: - Regional RV akinesia, dyskinesia, or bulging plus one of the following: - Global RV dilatation (an increase in RV EDV according to the imaging test-specific nomograms); - Global RV systolic dysfunction (reduction in RV EF according to the imaging test-specific nomograms). Minor: - Regional RV akinesia, dyskinesia, or aneurysm of RV free wall. | Minor: - Global LV systolic dysfunction (depression of LV EF or reduction in echo-cardiographic global longitudinal strain), with or without LV dilatation (an increase in LV EDV according to the imaging test-specific nomograms for age, sex, and BSA). - Regional LV hypokinesia or akinesia of LV free wall, septum, or both. |
| Structural myocardial abnormalities | By CE-CMR: Major: - Transmural LGE (stria pattern) of ≥1 RV region(s) (inlet, outlet, and apex in 2 orthogonal views). By EMB (limited indications): Major: - Fibrous replacement of the myocardium in ≥1 sample, with or without fatty tissue. | Major: - LV LGE (stria pattern) of ≥1 Bull’s Eye segment(s) (in 2 orthogonal views) of the free wall (subepicardial or midmyocardial), septum, or both (excluding septal junctional LGE). |
| Repolarization abnormalities | Major: - Inverted T-waves in right precordial leads (V1, V2, and V3) or beyond in individuals with complete pubertal development (in the absence of complete RBBB). Minor: - Inverted T-waves in leads V1 and V2 in individuals with completed pubertal development (in the absence of complete RBBB). - Inverted T-waves in V1, V2, V3, and V4 in individuals with completed pubertal development in the presence of complete RBBB. | Minor: - Inverted T-waves in left precordial leads (V4-V6) (in the absence of complete LBBB). |
| Depolarization abnormalities | Minor: - Epsilon wave (reproducible low-amplitude signals between the end of the QRS complex to the onset of the T-wave) in the right precordial leads (V1 to V3). - Terminal activation duration of QRS ≥55 ms measured from the nadir of the S wave to the end of the QRS, including R’, in V1, V2, or V3 (in the absence of complete RBBB). | Minor: - Low QRS voltages (<0.5 mV peak to peak) in limb leads (in the absence of obesity, emphysema, or pericardial effusion). |
| Ventricular arrhythmias | Major: - Frequent ventricular extrasystoles (>500 per 24 h), non-sustained or sustained ventricular tachycardia of LBBB morphology. Minor: - Frequent ventricular extrasystoles (>500 per 24 h), non-sustained or sustained ventricular tachycardia of LBBB morphology with inferior axis (“RVOT pattern”). | Minor: - Frequent ventricular extrasystoles (>500 per 24 h), non-sustained or sustained ventricular tachycardia with an RBBB morphology (excluding the “fascicular pattern”). |
| Family history/genetics | Major: - ACM confirmed in a first-degree relative who meets diagnostic criteria. - ACM confirmed pathologically at autopsy or surgery in a first-degree relative. - Identification of a pathogenic or likely pathogenetic ACM mutation in the patient under evaluation. Minor: - History of ACM in a first-degree relative in whom it is not possible or practical to determine whether the family member meets diagnostic criteria. - Premature sudden death (>35 years of age) due to suspected ACM in a first-degree relative. - ACM confirmed pathologically or by diagnostic criteria in a second-degree relative. | |
| Desmosomal Genes | Non-Desmosomal Genes |
|---|---|
| - Plakophilin C (PKP2) - Desmoplakin (DSP) - Desmocollin-2 (DSC2) - Desmoglein-2 (DSG2) - Plakoglobin (JUP | - Transmembrane protein 43—luma (TMEM 43) - Phospholamban (PLN) - Filamin C (FLNC) - Desmin (DES) - LMNA (Lamin A/C) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varrenti, M.; Bonvicini, E.; Milillo, L.F.; Garofani, I.; Carbonaro, M.; Baroni, M.; Gigli, L.; Colombo, G.; Giordano, F.; Falco, R.; et al. Arrhythmic Risk Stratification in Patients with Arrhythmogenic Cardiomyopathy. Diagnostics 2025, 15, 1149. https://doi.org/10.3390/diagnostics15091149
Varrenti M, Bonvicini E, Milillo LF, Garofani I, Carbonaro M, Baroni M, Gigli L, Colombo G, Giordano F, Falco R, et al. Arrhythmic Risk Stratification in Patients with Arrhythmogenic Cardiomyopathy. Diagnostics. 2025; 15(9):1149. https://doi.org/10.3390/diagnostics15091149
Chicago/Turabian StyleVarrenti, Marisa, Eleonora Bonvicini, Leandro Fabrizio Milillo, Ilaria Garofani, Marco Carbonaro, Matteo Baroni, Lorenzo Gigli, Giulia Colombo, Federica Giordano, Raffaele Falco, and et al. 2025. "Arrhythmic Risk Stratification in Patients with Arrhythmogenic Cardiomyopathy" Diagnostics 15, no. 9: 1149. https://doi.org/10.3390/diagnostics15091149
APA StyleVarrenti, M., Bonvicini, E., Milillo, L. F., Garofani, I., Carbonaro, M., Baroni, M., Gigli, L., Colombo, G., Giordano, F., Falco, R., Frontera, A., Menè, R., Preda, A., Vargiu, S., Mazzone, P., & Guarracini, F. (2025). Arrhythmic Risk Stratification in Patients with Arrhythmogenic Cardiomyopathy. Diagnostics, 15(9), 1149. https://doi.org/10.3390/diagnostics15091149