
Structured Reporting in Sleep Medicine

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size Calculation
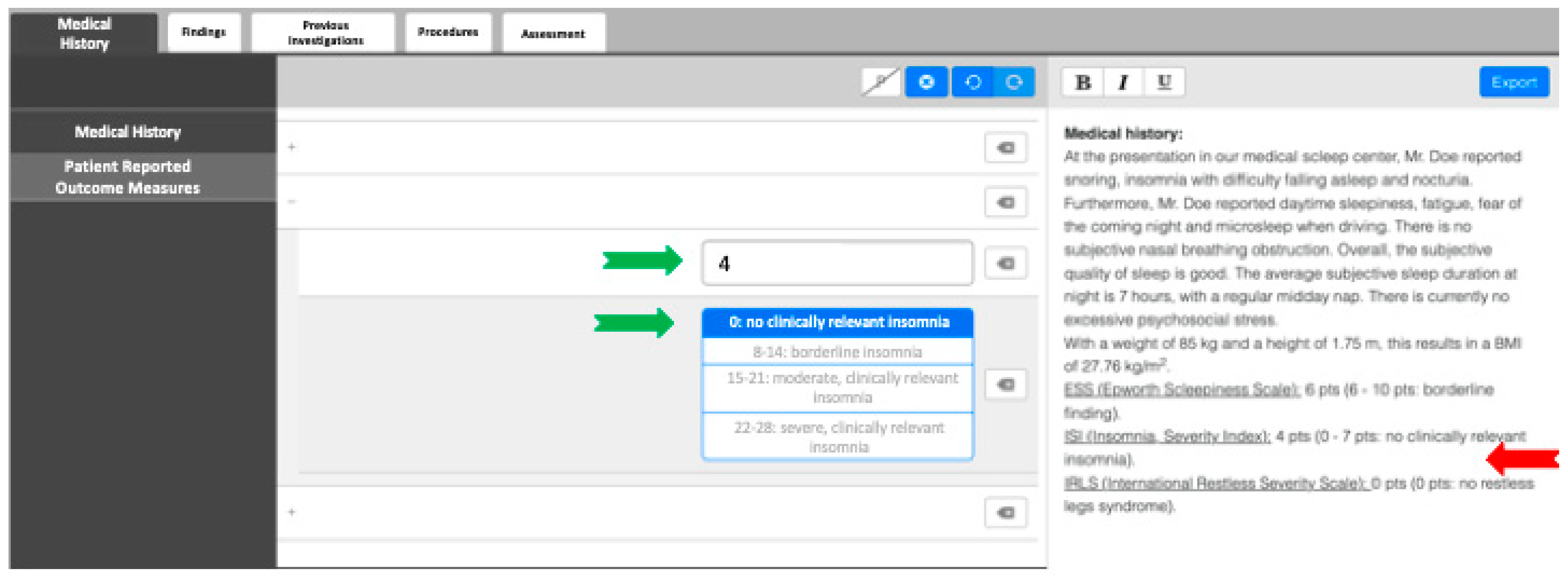
2.3. FTRs and SRs
2.4. Report Evaluation
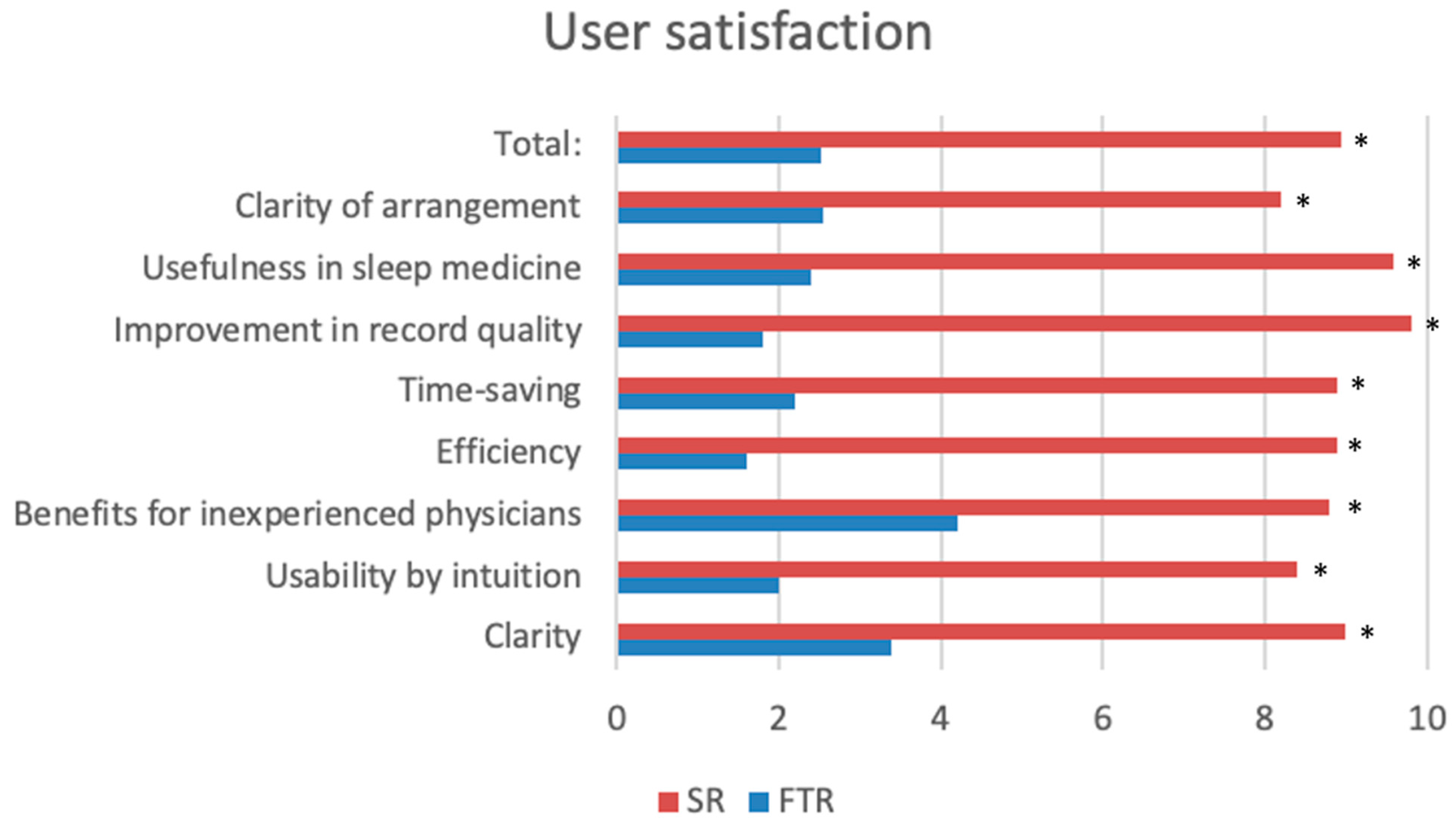
2.5. User Satisfaction
2.6. Statistical Analysis
3. Results
3.1. Report Analysis
3.2. User Satisfaction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DGSM | German Sleep Society |
| ENT | Ear–Nose–Throat |
| FTR | Free-text report |
| OSA | Obstructive sleep apnea |
| SR | Structured reporting |
| VAS | Visual analogue scale |
References
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Mehra, R. Sleep apnea and the heart. Clevel. Clin. J. Med. 2019, 86, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Bahr, K.; Bopp, M.; Kewader, W.; Dootz, H.; Döge, J.; Huppertz, T.; Simon, P.; Prokosch-Willing, V.; Matthias, C.; Gouveris, H. Obstructive sleep apnea as a risk factor for primary open angle glaucoma and ocular hypertension in a monocentric pilot study. Respir. Res. 2020, 21, 258. [Google Scholar] [CrossRef]
- Stevenson, J.E. Diagnosis of sleep apnea. Wis. Med. J. 2003, 102, 25–27. [Google Scholar]
- Society, G.S. Checkliste zur Qualitätssicherung der DGSM. Available online: https://www.dgsm.de/fileadmin/Fachinformationen/Qualitaetsmanagement/Qualitaetsicherung/QS_Checkliste_2022-09.pdf (accessed on 24 April 2025).
- Ernst, B.P.; Hodeib, M.; Strieth, S.; Künzel, J.; Bischof, F.; Hackenberg, B.; Huppertz, T.; Weber, V.; Bahr, K.; Eckrich, J.; et al. Structured reporting of head and neck ultrasound examinations. BMC Med. Imaging 2019, 19, 25. [Google Scholar] [CrossRef]
- dos Santos, D.P.; Hempel, J.-M.; Mildenberger, P.; Klöckner, R.; Persigehl, T. Structured Reporting in Clinical Routine. Rofo 2019, 191, 33–39. [Google Scholar] [CrossRef]
- Weimer, J.M.; Künzel, J.; Ernst, B.P.; Dörsching, C.; Bozzato, A.; Gabrielpillai, J.; Becker, S.; Froelich, M.F.; Kramer, B.; Sproll, C.; et al. Structured Reporting of Head and Neck Sonography Achieves Substantial Interrater Reliability. Ultrasound Int. Open 2023, 9, E26–E32. [Google Scholar] [CrossRef] [PubMed]
- Gassenmaier, S.; Armbruster, M.; Haasters, F.; Helfen, T.; Henzler, T.; Alibek, S.; Pförringer, D.; Sommer, W.H.; Sommer, N.N. Structured reporting of MRI of the shoulder—Improvement of report quality? Eur. Radiol. 2017, 27, 4110–4119. [Google Scholar] [CrossRef]
- Schoeppe, F.; Sommer, W.H.; Haack, M.; Havel, M.; Rheinwald, M.; Wechtenbruch, J.; Fischer, M.R.; Meinel, F.G.; Sabel, B.O.; Sommer, N.N. Structured reports of videofluoroscopic swallowing studies have the potential to improve overall report quality compared to free text reports. Eur. Radiol. 2018, 28, 308–315. [Google Scholar] [CrossRef]
- Bin Park, S.; Kim, M.-J.; Ko, Y.; Sim, J.Y.; Kim, H.J.; Lee, K.H.; LOCAT Group. Structured Reporting versus Free-Text Reporting for Appendiceal Computed Tomography in Adolescents and Young Adults: Preference Survey of 594 Referring Physicians, Surgeons, and Radiologists from 20 Hospitals. Korean J. Radiol. 2019, 20, 246–255. [Google Scholar] [CrossRef]
- Lacerda, T.C.; von Wangenheim, C.G.; von Wangenheim, A.; Giuliano, I. Does the use of structured reporting improve usability? A comparative evaluation of the usability of two approaches for findings reporting in a large-scale telecardiology context. J. Biomed. Inform. 2014, 52, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Reiner, B.I. The challenges, opportunities, and imperative of structured reporting in medical imaging. J. Digit. Imaging 2009, 22, 562–568. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, D.P.; Baeßler, B. Big data, artificial intelligence, and structured reporting. Eur. Radiol. Exp. 2018, 2, 42. [Google Scholar] [CrossRef]
- Bosmans, J.M.L.; Peremans, L.; Menni, M.; De Schepper, A.M.; Duyck, P.O.; Parizel, P.M. Structured reporting: If, why, when, how-and at what expense? Results of a focus group meeting of radiology professionals from eight countries. Insights Into Imaging 2012, 3, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Gunderman, R.B.; McNeive, L.R. Is structured reporting the answer? Radiology 2014, 273, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Mayer, G.; Arzt, M.; Braumann, B.; Ficker, J.H.; Fietze, I.; Frohnhofen, H.; Galetke, W.; Maurer, J.T.; Orth, M.; Penzel, T.; et al. German S3 Guideline Nonrestorative Sleep/Sleep Disorders, chapter “Sleep-Related Breathing Disorders in Adults,” short version. Somnologie 2017, 21, 290–301. [Google Scholar] [CrossRef]
- Stuck, B.A.; Arzt, M.; Fietze, I.; Galetke, W.; Hein, H.; Heiser, C.; Herkenrath, S.D.; Hofauer, B.; Maurer, J.T.; Mayer, G.; et al. Partial update of the German S3 Guideline Sleep-Related Breathing Disorders in Adults. Somnologie 2022, 28, 277–309. [Google Scholar] [CrossRef]
- Lin, E.; Powell, D.K.; Kagetsu, N.J. Efficacy of a Checklist-Style Structured Radiology Reporting Template in Reducing Resident Misses on Cervical Spine Computed Tomography Examinations. J. Digit. Imaging 2014, 27, 588–593. [Google Scholar] [CrossRef]
- Ernst, B.P.; Katzer, F.; Künzel, J.; Hodeib, M.; Strieth, S.; Eckrich, J.; Tattermusch, A.; Froelich, M.F.; Matthias, C.; Sommer, W.H.; et al. Impact of structured reporting on developing head and neck ultrasound skills. BMC Med. Educ. 2019, 19, 102. [Google Scholar] [CrossRef]
- Johnson, A.J.; Chen, M.Y.M.; Swan, J.S.; Applegate, K.E.; Littenberg, B. Cohort Study of Structured Reporting Compared with Conventional Dictation. Radiology 2009, 253, 74–80. [Google Scholar] [CrossRef]
- Larson, D.B. Strategies for Implementing a Standardized Structured Radiology Reporting Program. Radiographics 2018, 38, 1705–1716. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| FTR | SR | p | |
|---|---|---|---|
| Number of reports | 25 | 25 | |
| Overall completeness | 54.2% | 88% | <0.001 |
| Medical history | 48% | 99.3% | <0.001 |
| Clinical examination | 56% | 86.1% | <0.005 |
| Instrument-based diagnostics | 34.2% | 88% | <0.001 |
| Time required to complete | 16.8 min | 10.2 min | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahr-Hamm, K.; Gouveris, H.; Leggewie, B.; Becker, S.; Bärhold, F.; Ernst, B.P. Structured Reporting in Sleep Medicine. Diagnostics 2025, 15, 1117. https://doi.org/10.3390/diagnostics15091117
Bahr-Hamm K, Gouveris H, Leggewie B, Becker S, Bärhold F, Ernst BP. Structured Reporting in Sleep Medicine. Diagnostics. 2025; 15(9):1117. https://doi.org/10.3390/diagnostics15091117
Chicago/Turabian StyleBahr-Hamm, Katharina, Haralampos Gouveris, Barbara Leggewie, Sven Becker, Friederike Bärhold, and Benjamin Philipp Ernst. 2025. "Structured Reporting in Sleep Medicine" Diagnostics 15, no. 9: 1117. https://doi.org/10.3390/diagnostics15091117
APA StyleBahr-Hamm, K., Gouveris, H., Leggewie, B., Becker, S., Bärhold, F., & Ernst, B. P. (2025). Structured Reporting in Sleep Medicine. Diagnostics, 15(9), 1117. https://doi.org/10.3390/diagnostics15091117