
Assessment of Sexual Function in Relation to Microbiological Findings in Patients with Chronic Bacterial Prostatitis



Abstract
1. Introduction
2. Materials and Methods
Statistics
3. Results
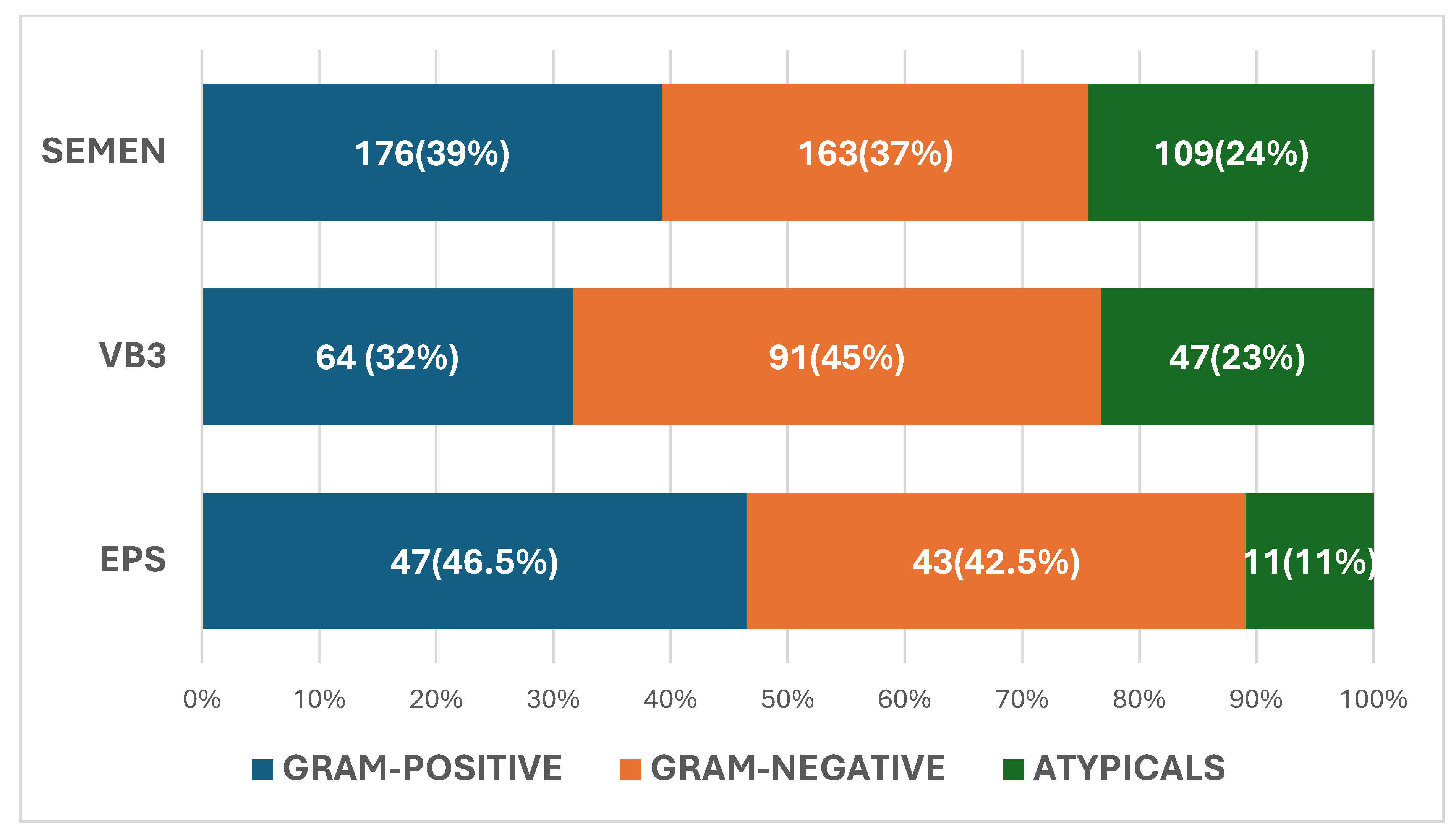
3.1. Microbiological Findings
3.1.1. VB3 Urine
3.1.2. Semen
3.1.3. Expressed Prostate Secretion (EPS)
3.1.4. Identical Pathogens in Different Biological Samples
3.2. Demographics and Clinical Characteristics
3.3. Biological Samples and Type of Infection
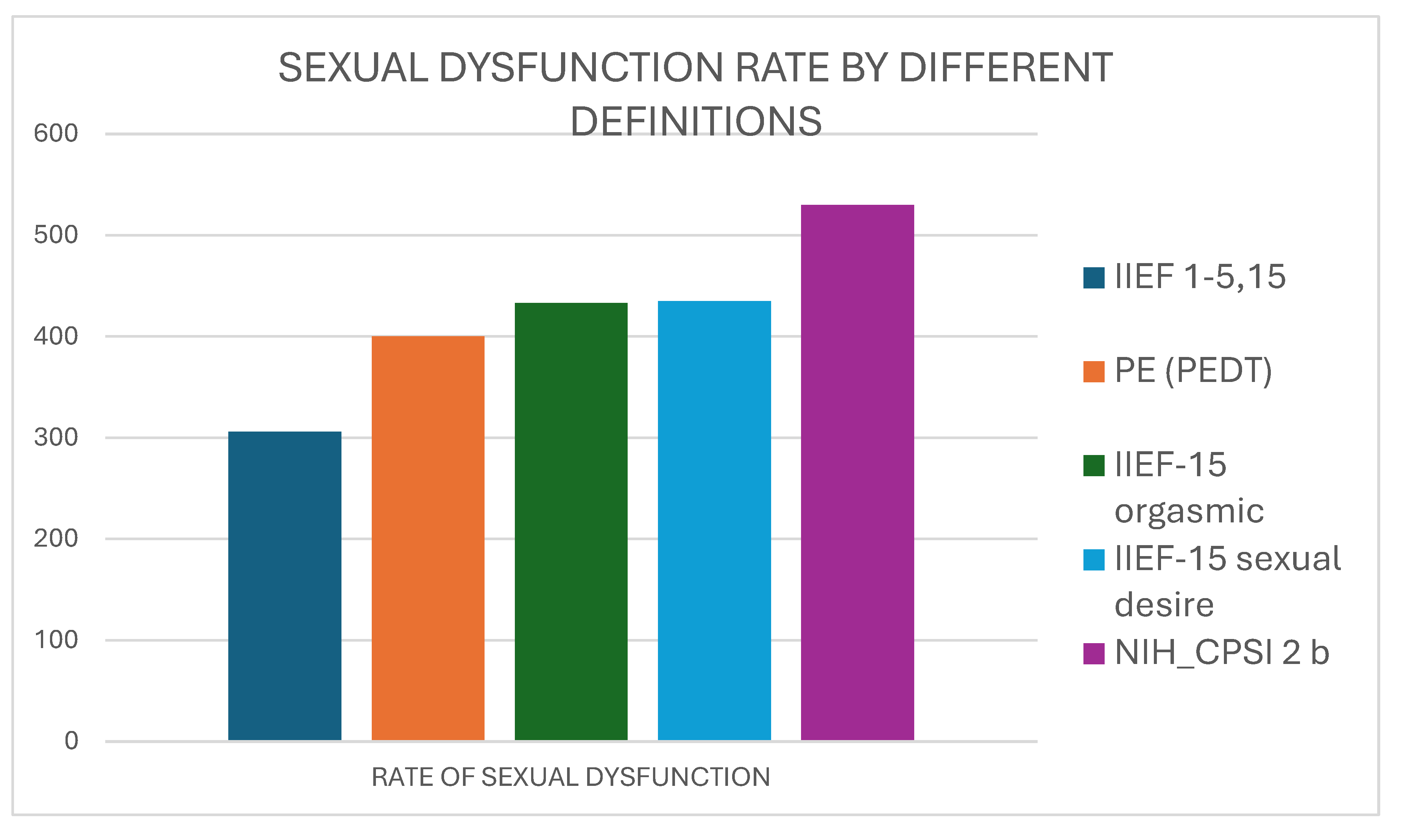
3.4. Prevalence of Sexual Dysfunction Symptoms
3.5. UPOINT Classification
3.6. UPOINTS
3.7. A New Tool for Investigating Sexual Function in CBP
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CBP | chronic bacterial prostatitis |
| ED | erectile dysfunction |
| PE | premature ejaculation |
| EPS | expressed prostatic secretion |
| VB3 | voiding bladder 3 |
| PVR | post-voiding residual |
| NIH-CPSI | National Institute of Health-Chronic Prostatitis Symptom Index |
| IPSS | International Prostatic Symptom Score |
| IIEF-15 | International Index of Erectile Function-15 |
| UPOINT | Urinary Psychosocial Organ-specific Infection Neurologic Tenderness |
References
- Trinchieri, A.; Magri, V.; Cariani, L.; Bonamore, R.; Restelli, A.; Garlaschi, M.C.; Perletti, G. Prevalence of sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome. Arch. Ital. Urol. Androl. 2007, 79, 67–70. [Google Scholar] [PubMed]
- Meares, E.M., Jr.; Stamey, T.A. The diagnosis and management of bacterial prostatitis. Br. J. Urol. 1972, 44, 175–179. [Google Scholar]
- Litwin, M.S.; McNaughton-Collins, M.; Fowler, F.J., Jr.; Nickel, J.C.; Calhoun, E.A.; Pontari, M.A.; Alexander, R.B.; Farrar, J.T.; O’Leary, M.P. The National Institutes of Health chronic prostatitis symptom index: Development and validation of a new outcome measure. Chronic Prostatitis Collaborative Research Network. J. Urol. 1999, 162, 369–375. [Google Scholar] [PubMed]
- Chen, X.; Zhou, Z.; Qiu, X.; Wang, B.; Dai, J. The Effect of Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS) on Erectile Function: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0141447. [Google Scholar]
- Evans-Durán, B.; Tripp, D.A.; Campbell, J.; Doiron, R.C.; Nickel, J.C. Chronic prostatitis/chronic pelvic pain syndrome-related pain symptoms and their impact on sexual functioning. Can. Urol. Assoc. J. 2022, 16, 222–227. [Google Scholar]
- Li, H.J.; Kang, D.Y. Prevalence of sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: A meta-analysis. World J. Urol. 2015, 34, 1009–1017. [Google Scholar]
- Krieger, J.N.; Egan, K.J.; Ross, S.O.; Jacobs, R.; Berger, R.E. Chronic pelvic pains represent the most prominent urogenital symptoms of chronic prostatitis. Urology 1996, 48, 715–722. [Google Scholar]
- Aubin, S.; Berger, R.E.; Heiman, J.R.; Ciol, M.A. The association between sexual function, pain, and psychological adaptation of men diagnosed with chronic pelvic pain syndrome Type III. J. Sex. Med. 2008, 5, 657–667. [Google Scholar]
- Pereira, R.; Margarida Oliveira, C.; Nobre, P. Sexual functioning and cognitions during sexual activity in men with genital pain: A comparative study. J. Sex. Marital. Ther. 2015, 42, 602–615. [Google Scholar]
- Shoskes, D.A.; Nickel, J.C.; Dolinga, R.; Prots, D. Clinical phenotyping of patients with chronic prostatitis/chronic pelvic pain syndrome and correlation with symptom severity. Urology 2009, 73, 538–542. [Google Scholar]
- Peyronnet, B.; Seisen, T.; Phé, V.; Misrai, V.; de la Taille, A.; Rouprêt, M. Symptômes du bas appareil urinaire secondaire à une hyperplasie bénigne de prostate et dysfonction érectile: Une revue systématique de la littérature [Lower urinary tract symptoms related to benign prostatic hyperplasia and erectile dysfunction: A systematic review]. Presse Med. 2017, 46, 145–153. [Google Scholar] [PubMed]
- Welliver, C.; MacLachlan, L.S.; Riggs, S.; Kukreja, J.B.; Miles-Thomas, J. A Multifaceted Assessment of Benign Prostatic Hyperplasia Practice and AUA Guideline Adherence. Urol. Pract. 2024, 11, 950–955. [Google Scholar] [CrossRef]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar]
- Symonds, T.; Perelman, M.A.; Althof, S.; Giuliano, F.; Martin, M.; May, K.; Abraham, L.; Crossland, A.; Morris, M. Development and validation of a premature ejaculation diagnostic tool. Eur. Urol. 2007, 52, 565–573. [Google Scholar] [PubMed]
- Li, X.C.; Zhang, X.B.; Liao, Z.C.; Tang, Z.Y.; Li, D.J. Is mild erectile dysfunction associated with severe psychological symptoms in Chinese patients with moderate-to-severe chronic prostatitis/chronic pelvic pain syndrome? Asian J. Androl. 2021, 23, 319–324. [Google Scholar] [PubMed]
- Ma, C.; Cai, Z.; Xiong, J.; Li, H. History of Prostatitis Is an Independent Risk Factor for Erectile Dysfunction: A Cross-Sectional Study. Biomed. Res. Int. 2020, 2020, 8964673. [Google Scholar]
- Lee, J.H.; Yoo, T.K.; Kang, J.Y.; Cho, J.M.; Park, Y.W.; Lee, S.W.; Choi, J.D. Relationship between erectile dysfunction and moderate to severe prostatitis-like symptoms in middle-aged men: A propensity score-matched analysis. Int. Urol. Nephrol. 2021, 53, 2261–2266. [Google Scholar]
- Loh-Doyle, J.C.; Stephens-Shields, A.J.; Rolston, R.; Newcomb, C.; Taple, B.; Sutcliffe, S.; Yang, C.C.; Lai, H.; Rodriguez, L.V. Predictors of Male Sexual Dysfunction in Urologic Chronic Pelvic Pain Syndrome (UCPPS), Other Chronic Pain Syndromes, and Healthy Controls in the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network. J. Sex. Med. 2022, 19, 1804–1812. [Google Scholar]
- Stamatiou, K.; Magri, V.; Trinchieri, M.; Trinchieri, A.; Perletti, G. Psychological and sexological assessment of patients with chronic prostatitis. Arch. Ital. Urol. Androl. 2024, 96, 12452. [Google Scholar] [CrossRef]
- Gao, J.; Gao, R.; Liu, X.; Li, C.; Gao, P.; Du, J.; Zhang, X. Correlations between Personality Traits, Patient-Reported Outcome, and Chronic Prostatitis Symptoms in Men with Different Premature Ejaculation Syndromes. Biomed. Res. Int. 2022, 2022, 8049976. [Google Scholar]
- Fan, D.; Mao, W.; Wang, G.; Shi, H.; Wu, Z.; Xie, J.; Yin, L.; Xu, T.; Wang, K.; Peng, B. Study on the relationship between sex hormone changes and erectile dysfunction in patients with chronic prostatitis/chronic pelvic pain syndrome. Ann. Palliat. Med. 2021, 10, 1739–1747. [Google Scholar] [PubMed]
- Gacci, M.; Eardley, I.; Giuliano, F.; Hatzichristou, D.; Kaplan, S.A.; Maggi, M.; McVary, K.T.; Mirone, V.; Porst, H.; Roehrborn, C.G. Critical analysis of the relationship between sexual dysfunctions and lower urinary tract symptoms due to benign prostatic hyperplasia. Eur. Urol. 2011, 60, 809–825. [Google Scholar] [CrossRef]
- Camacho, M.E.; Reyes-Ortiz, C.A. Sexual dysfunction in the elderly: Age or disease? Int. J. Impot. Res. 2005, 17 (Suppl. 1), S52–S56. [Google Scholar] [PubMed]
- Zhang, Y.; Zang, N.; Xiang, Y.; Lin, F.; Liu, X.; Zhang, J. A comprehensive analysis of erectile dysfunction prevalence and the impact of prostate conditions on ED among US adults: Evidence from NHANES 2001–2004. Front. Endocrinol. 2025, 15, 1412369. [Google Scholar]
- Park, S.H.; Ryu, J.K.; Choo, G.Y.; Chung, Y.G.; Seong, D.H.; Kim, C.H.; Choe, W.S.; Ryu, D.S.; Hyun, I.Y.; Suh, J.K. Chronic bacterial seminal vesiculitis as a potential disease entity in men with chronic prostatitis. Int. J. Urol. 2015, 22, 508–512. [Google Scholar]
- La Vignera, S. Male accessory gland infections: Anatomical extension of inflammation and severity of symptoms evaluated by an original questionnaire. Andrologia 2012, 44 (Suppl. 1), 739–746. [Google Scholar] [CrossRef] [PubMed]
- La Vignera, S.; Condorelli, R.; Vicari, E.; D’Agata, R.; Calogero, A.E. High frequency of sexual dysfunction in patients with male accessory gland infections. Andrologia 2012, 44 (Suppl. 1), 438–446. [Google Scholar]
- Baldelli, V.; Scaldaferri, F.; Putignani, L.; Del Chierico, F. The Role of Enterobacteriaceae in Gut Microbiota Dysbiosis in Inflammatory Bowel Diseases. Microorganisms 2021, 9, 697. [Google Scholar] [CrossRef]
- Scales, B.S.; Dickson, R.P.; Huffnagle, G.B. A Tale of Two Sites: How Inflammation Can Reshape the Microbiomes of the Gut and Lungs. J. Leukoc. Biol. 2016, 100, 943–950. [Google Scholar]
- Hemmi, H.; Takeuchi, O.; Kawai, T.; Kaisho, T.; Sato, S.; Sanjo, H.; Matsumoto, M.; Hoshino, K.; Wagner, H.; Takeda, K. A Toll-like Receptor Recognizes Bacterial DNA. Nature 2000, 408, 740–745. [Google Scholar] [CrossRef]
- Mirsepasi-Lauridsen, H.C.; Vallance, B.A.; Krogfelt, K.A.; Petersen, A.M. Escherichia coli Pathobionts Associated with Inflammatory Bowel Disease. Clin. Microbiol. Rev. 2019, 32, e00060-18. [Google Scholar] [CrossRef] [PubMed]
- Horner, P.; Donders, G.; Cusini, M.; Gomberg, M.; Jensen, J.S.; Unemo, M. Should we be testing for urogenital Mycoplasma hominis, Ureaplasma parvum and Ureaplasma urealyticum in men and women? A position statement from the European STI Guidelines Editorial Board. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1845–1851. [Google Scholar] [CrossRef]
- Blans, M.C.; Visseren, F.L.; Banga, J.D.; Hoekstra, J.B.; van der Graaf, Y.; Diepersloot, R.J.; Bouter, K.P. Infection induced inflammation is associated with erectile dysfunction in men with diabetes. Eur. J. Clin. Investig. 2006, 36, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Pisano, F.; Magri, V.; Verze, P.; Mondaini, N.; D’Elia, C.; Malossini, G.; Mazzoli, S.; Perletti, G.; Gontero, P.; et al. Chlamydia trachomatis infection is related to premature ejaculation in chronic prostatitis patients: Results from a cross sectional study. J. Sex. Med. 2014, 11, 3085–3092. [Google Scholar] [CrossRef] [PubMed]
- Mazzoli, S. Biofilms in chronic bacterial prostatitis (NIH-II) and in prostatic calcifications. FEMS Immunol. Med. Microbiol. 2010, 59, 337–344. [Google Scholar] [CrossRef]
- Ch’ng, J.H.; Chong, K.K.L.; Lam, L.N.; Wong, J.J.; Kline, K.A. Biofilm-associated infection by enterococci. Nat. Rev. Microbiol. 2019, 17, 82–94. [Google Scholar] [CrossRef]
- Bartoletti, R.; Cai, T.; Nesi, G.; Albanese, S.; Meacci, F.; Mazzoli, S.; Naber, K. The impact of biofilm-producing bacteria on chronic bacterial prostatitis treatment: Results from a longitudinal cohort study. World J. Urol. 2014, 32, 737–742. [Google Scholar] [CrossRef]
- Tran, C.N.; Li, J.; Shoskes, D.A. An online UPOINT tool for phenotyping patients with chronic prostatitis. Can. J. Urol. 2014, 21, 7195–7200. [Google Scholar]
- Arda, E.; Cakiroglu, B.; Tas, T.; Ekici, S.; Uyanik, B.S. Use of the UPOINT Classification in Turkish Chronic Prostatitis or Chronic Pelvic Pain Syndrome Patients. Urology 2016, 97, 227–231. [Google Scholar] [CrossRef]
- Ichihara, K.; Takahashi, S.; Hiyama, Y.; Masumori, N.; Nagae, H.; Ito, S.; Wada, K.; Betsunoh, H.; Hamasuna, R.; Togo, Y.; et al. Distribution of the positive UPOINT domain in patients with chronic prostatitis or chronic pelvic pain syndrome: A multicenter observational study. J. Infect. Chemother. 2022, 28, 631–634. [Google Scholar] [CrossRef]
- Samplaski, M.K.; Li, J.; Shoskes, D.A. Inclusion of erectile domain to UPOINT phenotype does not improve correlation with symptom severity in men with chronic prostatitis/chronic pelvic pain syndrome. Urology 2011, 78, 653–658. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Demographic and Clinical Parameters | Questionnaire Scores | ||
|---|---|---|---|
| Age (years) | 45.6 ± 13.9 | NIH-CPSI pain | 10.4 ± 5.7 |
| PSA (ng/mL) | 2.3 ± 2.8 | NIH-CPSI micturition | 4.5 ± 2.7 |
| Qmax (mL/s) | 16.1 ± 9.3 | NIH-CPSI QoL | 7.8 ± 2.7 |
| PVR (mL) | 43.1 ± 55.9 | NIH-CPSI total | 22.7 ± 7.2 |
| WBC VB3 (n° hpf) | 9.1 ± 10.8 | IPSS | 11.9 ± 7.4 |
| WBC semen (n° hpf) | 9.1 ± 8.1 | IIEF1–5,15 erectile function | 21.9 ± 7.8 |
| Prostatic calcification | 255/614 (41.5%) | IIEF6–8 intercourse | 9.8 ± 4.0 |
| Hematospermia | 183/614 (29.8%) | IIEF 9–10 orgasmic function | 7.2 ± 2.6 |
| Premature ejaculation | 250/614 (40.7%) | IIEF 11–12 desire | 6.8 ± 2.5 |
| Risk factors for erectile dysfunction | 37/614 (6%) | IIEF 13–14 overall | 6.5 ± 2.5 |
| PEDT Total * | 7.027 ± 5.290 | ||
| EPS/VB3 | Semen | EPS/VB3 + Semen | Sig | ||
|---|---|---|---|---|---|
| Patients | N° | 155 | 307 | 141 | |
| Erectile function IIEF 1–5,15 | ≤16 N° (%) | 36 23.2% | 53 17.2% | 33 23.4% | 0.206 |
| Orgasmic function IIEF 9–10 | ≤2 N° | 41 | 89 | 39 | 0.609 |
| Impaired desire IIEF 11–12 | ≤2 N° | 45 | 84 | 36 | 0.646 |
| Premature ejaculation | Yes N° | 50 | 144 | 50 | 0.172 |
| Hemospermia | Yes N° (%) | 39/150 26% | 93/329 28.3% | 48/118 40.7% | 0.241 |
| Prostatic calcifications | Yes N° (%) | 65/150 43.3% | 127/329 38.6% | 60/118 50.8% | 0.971 |
| EPS/VB3 | Gram-neg | Gram-pos | Atypical | Sig | |
| Patients | N° | 91 | 64 | 47 | |
| Erectile function IIEF 1–5,15 | ≤16 | 40 43.9% | 20 31.2% | 9 19.1% | 0.045 |
| Orgasmic function IIEF 9–10 | ≤2 | 43 47.2% | 28 43.7% | 9 19.1% | 0.004 |
| Impaired desire IIEF 11–12 | ≤2 | 44/116 | 23/99 | 14/53 | 0.077 |
| Premature ejaculation | yes | 42/116 | 37/99 | 21/53 | 0.913 |
| Hematospermia | yes | 46/116 | 29/99 | 12/53 | 0.190 |
| Prostatic calcifications | yes | 45/116 | 53/99 | 27/53 | 0.108 |
| Semen | 163 | 176 | 109 | ||
| Erectile function IIEF 1–5,15 | ≤16 | 32/142 | 29/196 | 25/107 | 0.117 |
| Orgasmic function IIEF 9–10 | ≤2 | 40/143 | 56/196 | 32/108 | 0.955 |
| Impaired desire IIEF 11–12 | ≤2 | 40/143 | 44/196 | 36/108 | 0.275 |
| Premature ejaculation | yes | 59/143 | 87/196 | 48/108 | 0.137 |
| Hematospermia | yes | 51 31.2% | 67 38.0% | 23 21.1% | 0.011 |
| Prostatic calcifications | yes | 53 32.5% | 89 50.5% | 45 41.2% | 0.003 |
| NIH-CPSI Total | NIH-CPSI Pain | NIH-CPSI Mict | NIH-CPSI QoL | |||
|---|---|---|---|---|---|---|
| UPOINT | r | 0.262 | 0.164 | 0.272 | 0.245 | |
| p | 0.000 | 0.000 | 0.000 | 0.000 | ||
| UPOINTS-1 | r | 0.250 | 0.154 | 0.273 | 0.232 | |
| p | 0.000 | 0.018 | 0.000 | 0.000 | ||
| UPOINTS-2 | r | 0.268 | 0.176 | 0.266 | 0.247 | |
| p | 0.000 | 0.009 | 0.000 | 0.000 | ||
| UPOINTS-5 | r | 0.288 | 0.194 | 0.284 | 0.252 | |
| p | 0.000 | 0.004 | 0.000 | 0.000 | ||
| IIEF-15 erectile | intercourse | orgasmic | desire | satisfaction | ||
| UPOINT | r | −0.006 | −0.027 | −0.025 | −0.044 | −0.050 |
| p | 0.876 | 0.488 | 0.536 | 0.280 | 0.245 | |
| UPOINTS-1 | r | −0.211 | −0.171 | −0.161 | −0.183 | −0.197 |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| UPOINTS-2 | r | −0.138 | −0.118 | −0.116 | −0.127 | −0.143 |
| p | 0.001 | 0.004 | 0.004 | 0.002 | 0.001 | |
| UPOINTS-5 | r | −0.077 | −0.081 | −0.086 | −0.095 | −0.106 |
| p | 0.057 | 0.046 | 0.034 | 0.019 | 0.014 |
| NIH-CPSI Total | NIH-CPSI Pain | NIH-CPSI Mict | NIH-CPSI QoL | |||
|---|---|---|---|---|---|---|
| 3-questions | r | 0.177 | 0.168 | 0.063 | 0.186 | |
| p | 0.000 | 0.000 | 0.119 | 0.000 | ||
| 4-questions | r | 0.307 | 0.321 | 0.123 | 0.275 | |
| p | 0.000 | 0.000 | 0.002 | 0.000 | ||
| IIEF-15 erectile | intercourse | orgasmic | desire | satisfaction | ||
| 3-questions | r | −0.408 | −0.368 | −0.490 | −0.377 | −0.400 |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| 4-questions | r | −0.355 | −0.301 | −0.445 | −0.311 | −0.351 |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magri, V.; Perletti, G.; Stamatiou, K.; Trinchieri, A. Assessment of Sexual Function in Relation to Microbiological Findings in Patients with Chronic Bacterial Prostatitis. Diagnostics 2025, 15, 887. https://doi.org/10.3390/diagnostics15070887
Magri V, Perletti G, Stamatiou K, Trinchieri A. Assessment of Sexual Function in Relation to Microbiological Findings in Patients with Chronic Bacterial Prostatitis. Diagnostics. 2025; 15(7):887. https://doi.org/10.3390/diagnostics15070887
Chicago/Turabian StyleMagri, Vittorio, Gianpaolo Perletti, Konstantinos Stamatiou, and Alberto Trinchieri. 2025. "Assessment of Sexual Function in Relation to Microbiological Findings in Patients with Chronic Bacterial Prostatitis" Diagnostics 15, no. 7: 887. https://doi.org/10.3390/diagnostics15070887
APA StyleMagri, V., Perletti, G., Stamatiou, K., & Trinchieri, A. (2025). Assessment of Sexual Function in Relation to Microbiological Findings in Patients with Chronic Bacterial Prostatitis. Diagnostics, 15(7), 887. https://doi.org/10.3390/diagnostics15070887