
Predictive Potential of Contrast-Enhanced MRI-Based Delta-Radiomics for Chemoradiation Responsiveness in Muscle-Invasive Bladder Cancer

 , , ,
, , ,  , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
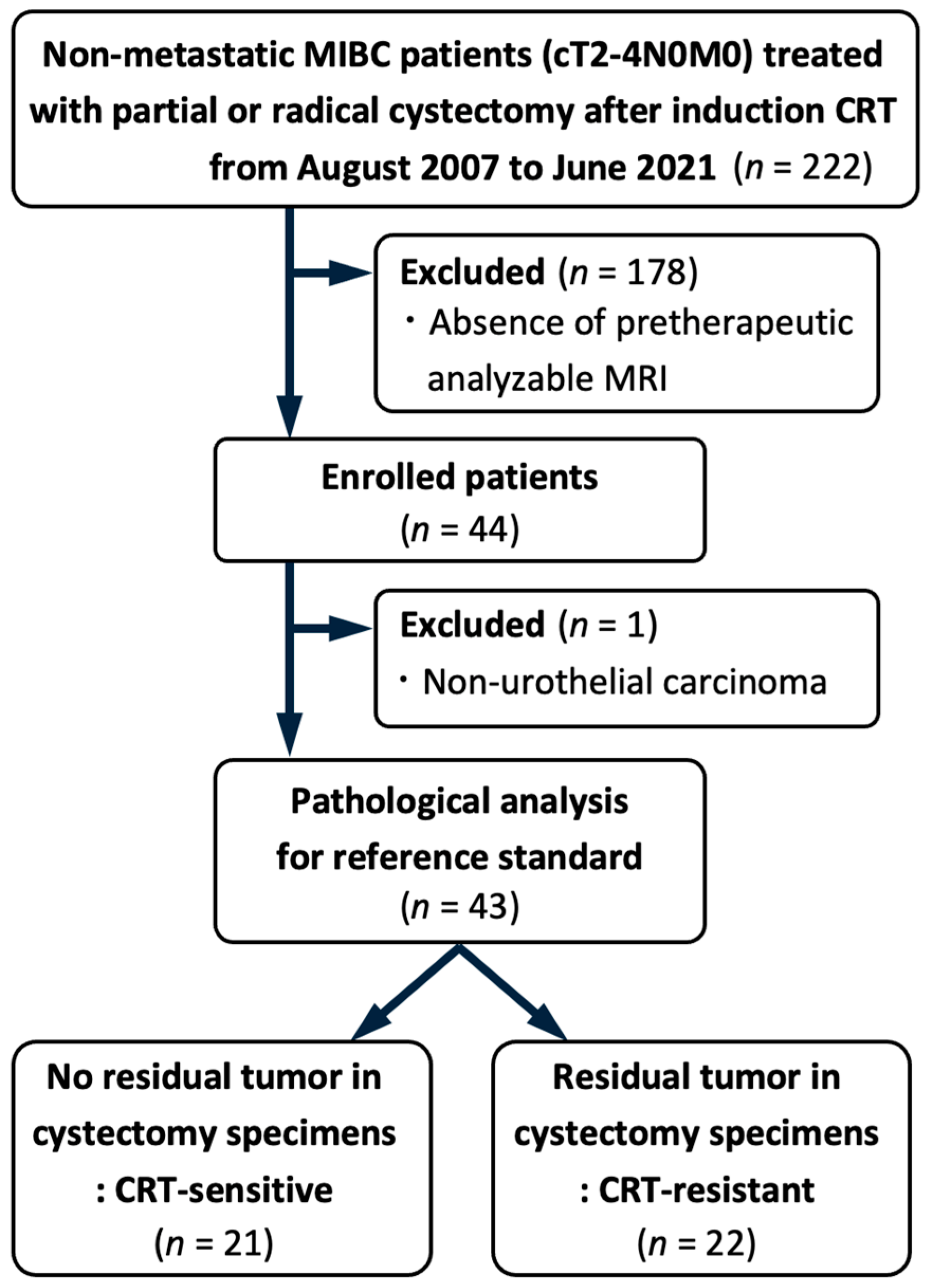
2.1. Patients
2.2. Data Collection
2.3. Pathological Analysis and CRT Response Evaluation
2.4. MRI Protocol
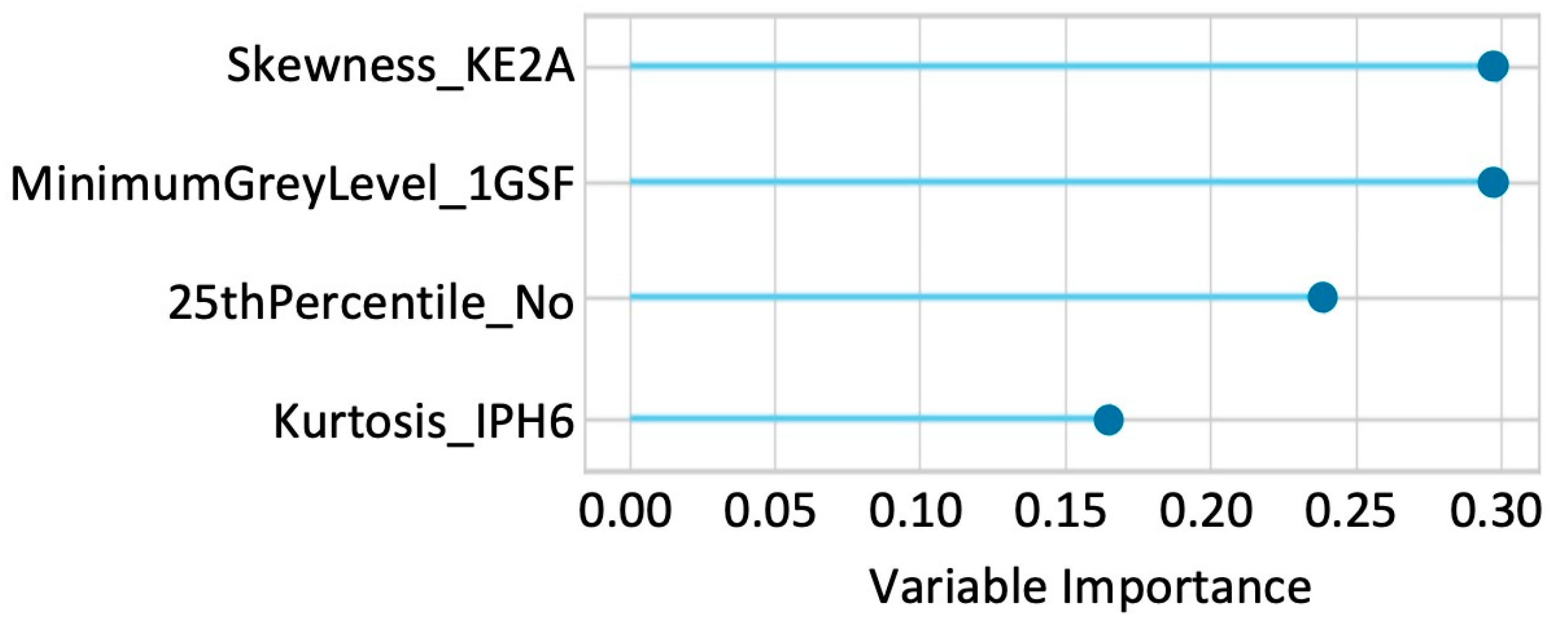
2.5. Delta-Radiomics Analysis
2.6. Model Development and Statistical Analyses
3. Results
3.1. Patient and Tumor Characteristics
3.2. Clinicopathological Variables Associated with CRT Sensitivity
3.3. Diagnostic Performance for CRT Sensitivity of Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alfred Witjes, J.; Max Bruins, H.; Carrion, A.; Cathomas, R.; Comperat, E.; Efstathiou, J.A.; Fietkau, R.; Gakis, G.; Lorch, A.; Martini, A.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2023 Guidelines. Eur. Urol. 2024, 85, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 2017, 198, 552–559. [Google Scholar] [CrossRef]
- Ploussard, G.; Daneshmand, S.; Efstathiou, J.A.; Herr, H.W.; James, N.D.; Rodel, C.M.; Shariat, S.F.; Shipley, W.U.; Sternberg, C.N.; Thalmann, G.N.; et al. Critical analysis of bladder sparing with trimodal therapy in muscle-invasive bladder cancer: A systematic review. Eur. Urol. 2014, 66, 120–137. [Google Scholar] [CrossRef]
- Mitin, T.; George, A.; Zietman, A.L.; Heney, N.M.; Kaufman, D.S.; Uzzo, R.G.; Dreicer, R.; Wallace, H.J., 3rd; Souhami, L.; Dobelbower, M.C.; et al. Long-Term Outcomes Among Patients Who Achieve Complete or Near-Complete Responses After the Induction Phase of Bladder-Preserving Combined-Modality Therapy for Muscle-Invasive Bladder Cancer: A Pooled Analysis of NRG Oncology/RTOG 9906 and 0233. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 67–74. [Google Scholar] [CrossRef]
- Panebianco, V.; Narumi, Y.; Altun, E.; Bochner, B.H.; Efstathiou, J.A.; Hafeez, S.; Huddart, R.; Kennish, S.; Lerner, S.; Montironi, R.; et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System). Eur. Urol. 2018, 74, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Urologic, I.; Allen, B.C.; Oto, A.; Akin, O.; Alexander, L.F.; Chong, J.; Froemming, A.T.; Fulgham, P.F.; Lloyd, S.; Maranchie, J.K.; et al. ACR Appropriateness Criteria(R) Post-Treatment Surveillance of Bladder Cancer. J. Am. Coll. Radiol. 2019, 16, S417–S427. [Google Scholar] [CrossRef]
- Petralia, G.; Summers, P.E.; Agostini, A.; Ambrosini, R.; Cianci, R.; Cristel, G.; Calistri, L.; Colagrande, S. Dynamic contrast-enhanced MRI in oncology: How we do it. Radiol. Med. 2020, 125, 1288–1300. [Google Scholar] [CrossRef]
- Tuncbilek, N.; Kaplan, M.; Altaner, S.; Atakan, I.H.; Sut, N.; Inci, O.; Demir, M.K. Value of dynamic contrast-enhanced MRI and correlation with tumor angiogenesis in bladder cancer. AJR Am. J. Roentgenol. 2009, 192, 949–955. [Google Scholar] [CrossRef]
- Hassanien, O.A.; Abouelkheir, R.T.; Abou El-Ghar, M.I.; Badawy, M.E.; El Gamal, S.A.; El-Hamid, M.A. Dynamic Contrast-Enhanced Magnetic Resonance Imaging as a Diagnostic Tool in the Assessment of Tumour Angiogenesis in Urinary Bladder Cancer. Can. Assoc. Radiol. J. 2019, 70, 254–263. [Google Scholar] [CrossRef]
- Shi, Z.; Yang, Z.; Zhang, G.; Cui, G.; Xiong, X.; Liang, Z.; Lu, H. Characterization of texture features of bladder carcinoma and the bladder wall on MRI: Initial experience. Acad. Radiol. 2013, 20, 930–938. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, S.; Leijenaar, R.T.H.; Troost, E.G.C.; van Elmpt, W.; Muratet, J.P.; Denis, F.; De Ruysscher, D.; Aerts, H.J.W.L.; Lambin, P. 42—Early variation of FDG-PET radiomics features in NSCLC is related to overall survival—The “delta radiomics” concept. Radiother. Oncol. 2016, 118, S20–S21. [Google Scholar] [CrossRef]
- Chang, Y.; Lafata, K.; Sun, W.; Wang, C.; Chang, Z.; Kirkpatrick, J.P.; Yin, F.F. An investigation of machine learning methods in delta-radiomics feature analysis. PLoS ONE 2019, 14, e0226348. [Google Scholar] [CrossRef]
- Nardone, V.; Reginelli, A.; Grassi, R.; Vacca, G.; Giacobbe, G.; Angrisani, A.; Clemente, A.; Danti, G.; Correale, P.; Carbone, S.F.; et al. Ability of Delta Radiomics to Predict a Complete Pathological Response in Patients with Loco-Regional Rectal Cancer Addressed to Neoadjuvant Chemo-Radiation and Surgery. Cancers 2022, 14, 3004. [Google Scholar] [CrossRef] [PubMed]
- Nardone, V.; Reginelli, A.; Guida, C.; Belfiore, M.P.; Biondi, M.; Mormile, M.; Banci Buonamici, F.; Di Giorgio, E.; Spadafora, M.; Tini, P.; et al. Delta-radiomics increases multicentre reproducibility: A phantom study. Med. Oncol. 2020, 37, 38. [Google Scholar] [CrossRef]
- Panebianco, V.; Briganti, A.; Efstathiou, J.; Galgano, S.; Luk, L.; Muglia, V.F.; Redd, B.; de Rooij, M.; Takeuchi, M.; Woo, S.; et al. The Role of Multiparametric Magnetic Resonance Imaging and the Vesical Imaging-Reporting and Data System (VI-RADS) in the Management of Patients with Bladder Cancer: Vision of the American College of Radiology VI-RADS Steering Committee. Eur. Urol. 2024, 86, 485–487. [Google Scholar] [CrossRef]
- Koga, F.; Kihara, K.; Fujii, Y.; Yoshida, S.; Saito, K.; Masuda, H.; Kageyama, Y.; Kawakami, S. Favourable outcomes of patients with clinical stage T3N0M0 bladder cancer treated with induction low-dose chemo-radiotherapy plus partial or radical cystectomy vs immediate radical cystectomy: A single-institutional retrospective comparative study. BJU Int. 2009, 104, 189–194. [Google Scholar] [CrossRef]
- Koga, F.; Yoshida, S.; Kawakami, S.; Kageyama, Y.; Yokoyama, M.; Saito, K.; Fujii, Y.; Kobayashi, T.; Kihara, K. Low-dose chemoradiotherapy followed by partial or radical cystectomy against muscle-invasive bladder cancer: An intent-to-treat survival analysis. Urology 2008, 72, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Mostofi, F.K.; Sobin, L.; Torloni, H. International Histological Classification of Tumours: Histological Typing of Urinary Bladder Tumours; World Health Organization: Geneva, Switzerland, 1973. [Google Scholar]
- Wittekind, C.; Compton, C.C.; Greene, F.L.; Sobin, L.H. TNM residual tumor classification revisited. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2002, 94, 2511–2516. [Google Scholar] [CrossRef]
- Arita, Y.; Woo, S.; Kwee, T.C.; Shigeta, K.; Ueda, R.; Nalavenkata, S.; Edo, H.; Miyai, K.; Das, J.; Andrieu, P.I.C.; et al. Pictorial review of multiparametric MRI in bladder urothelial carcinoma with variant histology: Pearls and pitfalls. Abdom. Radiol. 2024, 49, 2797–2811. [Google Scholar] [CrossRef]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuze, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A Freeware for Radiomic Feature Calculation in Multimodality Imaging to Accelerate Advances in the Characterization of Tumor Heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [PubMed]
- Bochner, B.H.; Cote, R.J.; Weidner, N.; Groshen, S.; Chen, S.C.; Skinner, D.G.; Nichols, P.W. Angiogenesis in bladder cancer: Relationship between microvessel density and tumor prognosis. J. Natl. Cancer Inst. 1995, 87, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Fus, L.P.; Górnicka, B. Role of angiogenesis in urothelial bladder carcinoma. Cent. Eur. J. Urol. 2016, 69, 258–263. [Google Scholar] [CrossRef]
- Shames, D.M.; Kuwatsuru, R.; Vexler, V.; Mühler, A.; Brasch, R.C. Measurement of capillary permeability to macromolecules by dynamic magnetic resonance imaging: A quantitative noninvasive technique. Magn. Reson. Med. 1993, 29, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.J.; Tofts, P.S. Pharmacokinetic Analysis of Neoplasms Using Contrast-enhance^ Dynamic Magnetic Resonance Imaging. Top. Magn. Reson. Imaging 1999, 10, 130–142. [Google Scholar] [CrossRef]
- Dobson, M.J.; Carrington, B.M.; Collins, C.D.; Ryder, W.D.; Read, G.; Hutchinson, C.E.; Hawnaur, J.M. The assessment of irradiated bladder carcinoma using dynamic contrast-enhanced MR imaging. Clin. Radiol. 2001, 56, 94–98. [Google Scholar] [CrossRef]
- Yoshida, S.; Koga, F.; Kawakami, S.; Ishii, C.; Tanaka, H.; Numao, N.; Sakai, Y.; Saito, K.; Masuda, H.; Fujii, Y.; et al. Initial experience of diffusion-weighted magnetic resonance imaging to assess therapeutic response to induction chemoradiotherapy against muscle-invasive bladder cancer. Urology 2010, 75, 387–391. [Google Scholar] [CrossRef]
- Arita, Y.; Kwee, T.C.; Akin, O.; Shigeta, K.; Paudyal, R.; Roest, C.; Ueda, R.; Lema-Dopico, A.; Nalavenkata, S.; Ruby, L.; et al. Multiparametric MRI and artificial intelligence in predicting and monitoring treatment response in bladder cancer. Insights Imaging 2025, 16, 7. [Google Scholar] [CrossRef]
- Ganeshan, B.; Miles, K.A. Quantifying tumour heterogeneity with CT. Cancer Imaging 2013, 13, 140–149. [Google Scholar] [CrossRef]
- Zhao, B.; Tan, Y.; Tsai, W.Y.; Qi, J.; Xie, C.; Lu, L.; Schwartz, L.H. Reproducibility of radiomics for deciphering tumor phenotype with imaging. Sci. Rep. 2016, 6, 23428. [Google Scholar] [CrossRef]
- Wong, O.L.; Yuan, J.; Zhou, Y.; Yu, S.K.; Cheung, K.Y. Longitudinal acquisition repeatability of MRI radiomics features: An ACR MRI phantom study on two MRI scanners using a 3D T1W TSE sequence. Med. Phys. 2021, 48, 1239–1249. [Google Scholar] [CrossRef]
- Yoshida, S.; Takahara, T.; Kwee, T.C.; Waseda, Y.; Kobayashi, S.; Fujii, Y. DWI as an Imaging Biomarker for Bladder Cancer. AJR Am. J. Roentgenol. 2017, 208, 1218–1228. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Yoshida, S.; Tsuchiya, J.; Yamada, I.; Tanaka, H.; Yokoyama, M.; Matsuoka, Y.; Yoshimura, R.; Tateishi, U.; Fujii, Y. Usefulness of texture features of apparent diffusion coefficient maps in predicting chemoradiotherapy response in muscle-invasive bladder cancer. Eur. Radiol. 2022, 32, 671–679. [Google Scholar] [CrossRef]
- Fave, X.; Zhang, L.; Yang, J.; Mackin, D.; Balter, P.; Gomez, D.; Followill, D.; Jones, A.K.; Stingo, F.; Liao, Z.; et al. Delta-radiomics features for the prediction of patient outcomes in non-small cell lung cancer. Sci. Rep. 2017, 7, 588. [Google Scholar] [CrossRef]
- Nasief, H.; Zheng, C.; Schott, D.; Hall, W.; Tsai, S.; Erickson, B.; Allen Li, X. A machine learning based delta-radiomics process for early prediction of treatment response of pancreatic cancer. NPJ Precis. Oncol. 2019, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Waingankar, N.; Jia, R.; Marqueen, K.E.; Audenet, F.; Sfakianos, J.P.; Mehrazin, R.; Ferket, B.S.; Mazumdar, M.; Galsky, M.D. The impact of pathologic response to neoadjuvant chemotherapy on conditional survival among patients with muscle-invasive bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 572.e21–572.e28. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, M.; Del Giudice, F.; Magliocca, F.; Simone, G.; Flammia, S.; Leonardo, C.; Messina, E.; De Berardinis, E.; Cortesi, E.; Panebianco, V. Vesical Imaging-Reporting and Data System (VI-RADS) for assessment of response to systemic therapy for bladder cancer: Preliminary report. Abdom. Radiol. 2022, 47, 763–770. [Google Scholar] [CrossRef]
- Necchi, A.; Basile, G.; Gibb, E.A.; Raggi, D.; Calareso, G.; de Padua, T.C.; Patanè, D.; Crupi, E.; Mercinelli, C.; Cigliola, A.; et al. Vesical Imaging-Reporting and Data System use predicting the outcome of neoadjuvant pembrolizumab in muscle-invasive bladder cancer. BJU Int. 2024, 133, 214–222. [Google Scholar] [CrossRef]
- Hua, J.; Xiong, Z.; Lowey, J.; Suh, E.; Dougherty, E.R. Optimal number of features as a function of sample size for various classification rules. Bioinformatics 2005, 21, 1509–1515. [Google Scholar] [CrossRef]
- Kocak, B.; Akinci D’Antonoli, T.; Mercaldo, N.; Alberich-Bayarri, A.; Baessler, B.; Ambrosini, I.; Andreychenko, A.E.; Bakas, S.; Beets-Tan, R.G.H.; Bressem, K.; et al. METhodological RadiomICs Score (METRICS): A quality scoring tool for radiomics research endorsed by EuSoMII. Insights Imaging 2024, 15, 8. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Achieva 1.5 T, n = 43 | ||||||
|---|---|---|---|---|---|---|
| T2WI | DWI | DCE Imaging | ||||
| Period (year) | 2007–2016 | 2017–2021 | 2007–2016 | 2017–2021 | 2007–2016 | 2017–2021 |
| Type of sequence | 2D-FSE | 3D-FSE | SS-EPI | SS-EPI | 3D-GRE | 3D-GRE |
| Orientation | Axial | Axial | Axial | Axial | Axial | Axial or Sagittal |
| TR/TE (ms) | 4500/100 | 1500/144 | 5000/80 | 5000/80 | 4.0–4.5/2.0–2.2 | 4.8/2.4 |
| Flip angle (degree) | 90 | 90 | 90 | 90 | 13 | 15 |
| FOV (cm) | 30 | 30 | 30 | 30 | 22–30 | 22 |
| Matrix | 512 × 512 | 512 × 512 | 256 × 256 | 256 × 256 | 288 × 288–512 × 512 | 288 × 288 |
| Slice thickness (mm) | 4.4–5.0 | 1.6 | 4.4–5.0 | 4.4 | 2.0–6.5 | 2.0 |
| Slice gap (mm) | 0.4–0.5 | 0 | 0.4–0.5 | 0.4 | 0 | 0 |
| Number of excitations | 2–3 | 1 | 2–6 | 3 | 1–2 | 1 |
| b-value (s/mm2) | — | — | 0, 500, 1000, 2000 | 0, 1000, 2000 | — | — |
| Variables | n (%) | CRT-Sensitive (n = 21) | CRT-Resistant (n = 22) | p Value |
|---|---|---|---|---|
| Age, years * | 68 (63–73) | 69 (63–74) | 67 (63–74) | 0.60 |
| Gender Male Female | 32 (74) 11 (26) | 18 (86) 3 (14) | 14 (64) 8 (36) | 0.10 |
| Clinical T stage T2 T3 T4 | 13 (30) 28 (65) 2 (5) | 2 (24) 3 (71) 4 (5) | 8 (36) 13 (59) 1 (5) | 0.67 |
| Size of index tumor (cm) * | 3.0 (2.0–4.0) | 2.7 (2.0–5.1) | 3.0 (2.0–4.0) | 0.88 |
| Multiplicity Yes No | 15 (35) 28 (65) | 5 (24) 16 (76) | 10 (45) 12 (55) | 0.14 |
| Presence of concomitant CIS Yes No | 1 (2) 42 (98) | 1 (5) 20 (95) | 0 (0) 22 (100) | 0.49 |
| Highest tumor grade Grade 2 Grade 3 | 1 (2) 42 (98) | 1 (5) 21 (95) | 0 (0) 22 (100) | 0.49 |
| Cystectomy after induction CRT Partial Radical | 25 (58) 18 (42) | 15 (71) 6 (29) | 10 (46) 12 (55) | 0.08 |
| Pathologic T stage T0 Ta/is/1 T2 T3 | 21 (49) 9 (21) 3 (7) 10 (23) | 21 (100) 0 (0) 0 (0) 0 (0) | 0 (0) 9 (41) 3 (14) 10 (46) | <0.01 |
| Pathologic N stage N0/x N+ | 42 (98) 1 (2) | 21 (100) 0 (0) | 21 (95) 1 (5) | 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isemoto, K.; Waseda, Y.; Fujiwara, M.; Kimura, K.; Hirahara, D.; Saho, T.; Takaya, E.; Arita, Y.; Kwee, T.C.; Fukuda, S.; et al. Predictive Potential of Contrast-Enhanced MRI-Based Delta-Radiomics for Chemoradiation Responsiveness in Muscle-Invasive Bladder Cancer. Diagnostics 2025, 15, 801. https://doi.org/10.3390/diagnostics15070801
Isemoto K, Waseda Y, Fujiwara M, Kimura K, Hirahara D, Saho T, Takaya E, Arita Y, Kwee TC, Fukuda S, et al. Predictive Potential of Contrast-Enhanced MRI-Based Delta-Radiomics for Chemoradiation Responsiveness in Muscle-Invasive Bladder Cancer. Diagnostics. 2025; 15(7):801. https://doi.org/10.3390/diagnostics15070801
Chicago/Turabian StyleIsemoto, Kohei, Yuma Waseda, Motohiro Fujiwara, Koichiro Kimura, Daisuke Hirahara, Tatsunori Saho, Eichi Takaya, Yuki Arita, Thomas C. Kwee, Shohei Fukuda, and et al. 2025. "Predictive Potential of Contrast-Enhanced MRI-Based Delta-Radiomics for Chemoradiation Responsiveness in Muscle-Invasive Bladder Cancer" Diagnostics 15, no. 7: 801. https://doi.org/10.3390/diagnostics15070801
APA StyleIsemoto, K., Waseda, Y., Fujiwara, M., Kimura, K., Hirahara, D., Saho, T., Takaya, E., Arita, Y., Kwee, T. C., Fukuda, S., Tanaka, H., Yoshida, S., & Fujii, Y. (2025). Predictive Potential of Contrast-Enhanced MRI-Based Delta-Radiomics for Chemoradiation Responsiveness in Muscle-Invasive Bladder Cancer. Diagnostics, 15(7), 801. https://doi.org/10.3390/diagnostics15070801