
Incidence, Pathogenesis, Risk Factors, and Treatment of Cystoid Macula Oedema Following Cataract Surgery: A Systematic Review


 , , and
, , and
Abstract
1. Introduction
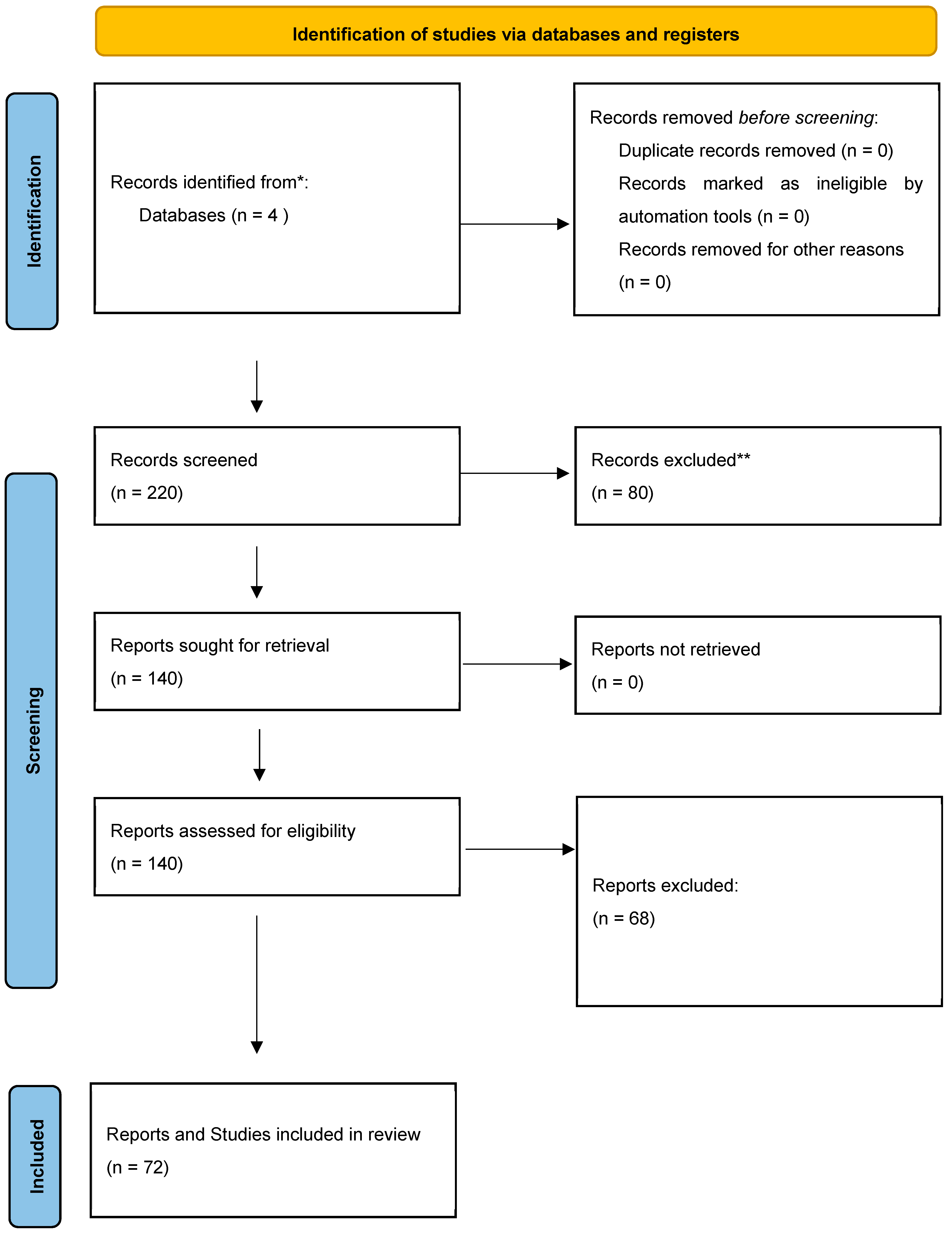
2. Materials and Methods
3. Results
3.1. Definition and Incidence
- Angiographic CMO (based on angiographic findings from fundus fluorescein angiography),
- Optical coherence tomography (OCT)-based CMO (from OCT findings of central subfield macular thickening),
- Clinical CMO (from clinical findings of reduced visual acuity and findings on fundoscopy).
3.2. Clinical Presentation
3.3. Pathogenesis
3.4. Risk Factors
3.5. Prophylaxis
3.5.1. Topical NSAIDs Prior to Surgery
3.5.2. Topical NSAIDs After Surgery
3.5.3. Intra-Operative Treatment in Diabetic Eyes
3.5.4. Topical NSAIDs After Surgery in Diabetic Eyes
3.5.5. Topical NSAIDs Before and After Surgery in Diabetic Eyes
3.6. Treatments and Outcomes
3.6.1. Topical Treatment
3.6.2. Periocular Steroids
3.6.3. Intravitreal Steroid Injection
3.6.4. Intravitreal Dexamethasone Implant (Ozurdex)
3.6.5. Intravitreal Bevacizumab
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NODaudit 2023. Available online: https://nodaudit.org.uk/sites/default/files/2023-08/NOD%20Cataract%20Audit%20Full%20Annual%20Report%202023.pdf (accessed on 1 November 2024).
- Rossi, T.; Romano, M.R.; Iannetta, D.; Romano, V.; Gualdi, L.; D’Agostino, I.; Ripandelli, G. Cataract surgery practice patterns worldwide: A survey. BMJ Open Ophthalmol. 2021, 6, e000464. [Google Scholar] [CrossRef]
- Jaycock, P.; Johnston, R.L.; Taylor, H.; Adams, M.; Tole, D.M.; Galloway, P.; Canning, C.; Sparrow, J.M. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: Updating benchmark standards of care in the United Kingdom and internationally. Eye 2009, 23, 38–49. [Google Scholar] [CrossRef]
- Drolsum, L.; Haaskjold, E. Causes of decreased visual acuity after cataract extraction. J. Cataract. Refract. Surg. 1995, 21, 59–63. [Google Scholar] [CrossRef]
- Irvine, S.R. A newly defined vitreous syndrome following cataract surgery. Am. J. Ophthalmol. 1953, 36, 599–619. [Google Scholar] [CrossRef]
- Bradford, D.J.; Wilkinson, C.P.; Bradford, R.H., Jr. Cystoid macular edema following extracapsular cataract extraction and posterior chamber intraocular lens implantation. Retina 1988, 8, 161–164. [Google Scholar] [CrossRef]
- Mentes, J.; Erakgun, T.; Afrashi, F.; Kerci, G. Incidence of cystoid macular edema after uncomplicated phacoemulsification. Ophthalmologica 2003, 217, 408–412. [Google Scholar] [CrossRef]
- Wetzig, P.C.; Thatcher, D.B.; Christiansen, J.M. The intracapsular versus the extracapsular cataract technique in relationship to retinal problems. Trans. Am. Ophthalmol. Soc. 1979, 77, 339–347. [Google Scholar]
- Chu, C.J.; Johnston, R.L.; Buscombe, C.; Sallam, A.B.; Mohamed, Q.; Yang, Y.C. Risk Factors and Incidence of Macular Edema after Cataract Surgery: A Database Study of 81984 Eyes. Ophthalmology 2016, 123, 316–323. [Google Scholar] [CrossRef]
- Levitz, L.; Reich, J.; Roberts, T.V.; Lawless, M. Incidence of cystoid macular edema: Femtosecond laser-assisted cataract surgery versus manual cataract surgery. J. Cataract. Refract. Surg. 2015, 41, 683–686. [Google Scholar] [CrossRef]
- Ching, H.Y.; Wong, A.C.; Wong, C.C.; Woo, D.C.; Chan, C.W. Cystoid macular oedema and changes in retinal thickness after phacoemulsification with optical coherence tomography. Eye 2006, 20, 297–303. [Google Scholar] [CrossRef]
- Lobo, C.L.; Faria, P.M.; Soares, M.A.; Bernardes, R.C.; Cunha-Vaz, J.G. Macular alterations after small-incision cataract surgery. J. Cataract. Refract. Surg. 2004, 30, 752–760. [Google Scholar] [CrossRef]
- Yoshioka, H.; Kawashima, K.; Sugita, T. Cystoid macular edema following cataract extraction. 2. Nippon Ganka Gakkai Zasshi 1972, 76, 1118–1124. [Google Scholar]
- Solomon, L.D.; Boyaner, D.; Breslin, C.W.; Demco, T.A.; LeBlanc, R.; Lemire, J.; Mintsioulis, G.; Ober, M.; Ramsey, M.; Sutton, H.F.; et al. Efficacy of topical flurbiprofen and indomethacin in preventing pseudophakic cystoid macular edema. J. Cataract. Refract. Surg. 1995, 21, 73–81. [Google Scholar] [CrossRef]
- Warren, K.A.; Fox, J.E. Topical nepafenac as an alternate treatment for cystoid macular edema in steroid responsive patients. Retina 2008, 28, 1427–1434. [Google Scholar] [CrossRef]
- Flach, A.J. The incidence, pathogenesis and treatment of cystoid macular edema following cataract surgery. Trans. Am. Ophthalmol. Soc. 1998, 96, 557–634. [Google Scholar]
- Wright, P.L.; Wilkinson, C.P.; Balyeat, H.D.; Popham, J.; Reinke, M. Angiographic cystoid macular edema after posterior chamber lens implantation. Arch. Ophthalmol. 1988, 106, 740–744. [Google Scholar] [CrossRef]
- Miyake, K.; Masuda, K.; Shirato, S.; Oshika, T.; Eguchi, K.; Hoshi, H.; Majima, Y.; Kimura, W.; Hayashi, F. Comparison of diclofenac and fluorometholone in preventing cystoid macular edema after small incision cataract surgery: A multicentered prospective trial. Jpn. J. Ophthalmol. 2000, 44, 58–67. [Google Scholar] [CrossRef]
- Han, J.V.; Patel, D.V.; Squirrell, D.; McGhee, C.N. Cystoid macular oedema following cataract surgery: A review. Clin. Exp. Ophthalmol. 2019, 47, 346–356. [Google Scholar] [CrossRef]
- Nussenblatt, R.B.; Kaufman, S.C.; Palestine, A.G.; Davis, M.D.; Ferris, F.L., III. Macular thickening and visual acuity: Measurement in patients with cystoid macular edema. Ophthalmology 1987, 94, 1134–1139. [Google Scholar] [CrossRef]
- Ouyang, Y.; Keane, P.A.; Sadda, S.R.; Walsh, A.C. Detection of cystoid macular edema with three-dimensional optical coherence tomography versus fluorescein angiography. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5213–5218. [Google Scholar] [CrossRef]
- Kim, S.J.; Bressler, N.M. Optical coherence tomography and cataract surgery. Curr. Opin. Ophthalmol. 2009, 20, 46–51. [Google Scholar] [CrossRef]
- Kim, B.Y.; Smith, S.D.; Kaiser, P.K. Optical coherence tomographic patterns of diabetic macular edema. Am. J. Ophthalmol. 2006, 142, 405–412. [Google Scholar] [CrossRef]
- Staurenghi, G.; Invernizzi, A.; de Polo, L.; Pellegrini, M. Diagnosis and detection. Dev. Ophthalmol. 2010, 47, 27–48. [Google Scholar] [CrossRef]
- Wittpenn, J.R.; Silverstein, S.; Heier, J.; Kenyon, K.R.; Hunkeler, J.D.; Earl, M. A randomized, masked comparison of topical ketorolac 0.4% plus steroid vs. steroid alone in low-risk cataract surgery patients. Am. J. Ophthalmol. 2008, 146, 554–560. [Google Scholar] [CrossRef]
- Eriksson, U.; Alm, A.; Bjärnhall, G.; Granstam, E.; Matsson, A.W. Macular edema and visual outcome following cataract surgery in patients with diabetic retinopathy and controls. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 349–359. [Google Scholar] [CrossRef]
- Sacconi, R.; Corbelli, E.; Carnevali, A.; Mercuri, S.; Rabiolo, A.; Querques, L.; Marchini, G.; Bandello, F.; Querques, G. Optical coherence tomography angiography in pseudophakic cystoid macular oedema compared to diabetic macular oedema: Qualitative and quantitative evaluation of retinal vasculature. Br. J. Ophthalmol. 2018, 102, 1684–1690. [Google Scholar] [CrossRef]
- Lupidi, M.; Coscas, F.; Cagini, C.; Coscas, G. Optical Coherence Tomography Angiography in Macular Edema. Dev. Ophthalmol. 2017, 58, 63–73. [Google Scholar] [CrossRef]
- Gass, J.D.; Norton, E.W. Cystoid macular edema and papilledema following cataract extraction: A fluorescein fundoscopic and angiographic study. Arch. Ophthalmol. 1966, 76, 646–661. [Google Scholar] [CrossRef]
- Gass, J.D.; Norton, E.W. Fluorescein studies of patients with macular edema and papilledema following cataract extraction. Trans. Am. Ophthalmol. Soc. 1966, 64, 232–249. [Google Scholar]
- Ursell, P.G.; Spalton, D.J.; Whitcup, S.M.; Nussenblatt, R.B. Cystoid macular edema after phacoemulsification: Relationship to blood-aqueous barrier damage and visual acuity. J. Cataract. Refract. Surg. 1999, 25, 1492–1497. [Google Scholar] [CrossRef]
- Akçay, B.I.S.; Bozkurt, T.K.; Guney, E.; Erdogan, G.; Ünlü, C.; Akcali, G.; Bayramlar, H. Quantitative analysis of macular thickness following uneventful and complicated cataract surgery. Clin. Ophthalmol. 2012, 6, 1507–1511. [Google Scholar] [CrossRef] [PubMed]
- Benitah, N.R.; Arroyo, J.G. Pseudophakic cystoid macular edema. Int. Ophthalmol. Clin. 2010, 50, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Hudes, G.R.; Li, W.Y.; Rockey, J.H.; White, P. Prostacyclin is the major prostaglandin synthesized by bovine retinal capillary pericytes in culture. Investig. Ophthalmol. Vis. Sci. 1988, 29, 1511–1516. [Google Scholar]
- Panteleontidis, V.; Detorakis, E.T.; Pallikaris, I.G.; Tsilimbaris, M.K. Latanoprost-Dependent Cystoid Macular Edema Following Uncomplicated Cataract Surgery in Pseudoexfoliative Eyes. Ophthalmic Surg. Lasers Imaging Retin. 2010, 41, 1–5. [Google Scholar] [CrossRef]
- Schmier, J.K.; Halpern, M.T.; Covert, D.W.; Matthews, G.P. Evaluation of costs for cystoid macular edema among patients after cataract surgery. Retina 2007, 27, 621–628. [Google Scholar] [CrossRef]
- Oyewole, K.; Tsogkas, F.; Westcott, M.; Patra, S. Benchmarking cataract surgery outcomes in an ethnically diverse and diabetic population: Final post-operative visual acuity and rates of post-operative cystoid macular oedema. Eye 2017, 31, 1672–1677. [Google Scholar] [CrossRef]
- Bélair, M.-L.; Kim, S.J.; Thorne, J.E.; Dunn, J.P.; Kedhar, S.R.; Brown, D.M.; Jabs, D.A. Incidence of cystoid macular edema after cataract surgery in patients with and without uveitis using optical coherence tomography. Am. J. Ophthalmol. 2009, 148, 128–135.e2. [Google Scholar] [CrossRef]
- Henderson, B.A.; Kim, J.Y.; Ament, C.S.; Ferrufino-Ponce, Z.K.; Grabowska, A.; Cremers, S.L. Clinical pseudophakic cystoid macular edema: Risk factors for development and duration after treatment. J. Cataract. Refract. Surg. 2007, 33, 1550–1558. [Google Scholar] [CrossRef]
- Schaub, F.; Adler, W.; Enders, P.; Koenig, M.C.; Koch, K.R.; Cursiefen, C.; Kirchhof, B.; Heindl, L.M. Preexisting epiretinal membrane is associated with pseudophakic cystoid macular edema. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 909–917. [Google Scholar] [CrossRef]
- Law, S.K.; Kim, E.; Yu, F.; Caprioli, J. Clinical cystoid macular edema after cataract surgery in glaucoma patients. J. Glaucoma 2010, 19, 100–104. [Google Scholar] [CrossRef]
- Taipale, C.; Holmström, E.J.; Ilveskoski, L.; Tuuminen, R. Incidence of pseudophakic cystoid macular edema in eyes with and without pupil expansion device. Acta Ophthalmol. 2019, 97, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Sivaprasad, S.; Gupta, B.; Gulliford, M.C.; Dodhia, H.; Mann, S.; Nagi, D.; Evans, J. Ethnic variation in the prevalence of visual impairment in people attending diabetic retinopathy screening in the United Kingdom (DRIVE UK). PLoS ONE 2012, 7, e39608. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Hwang, H.J.; Kim, H.S.; Lee, D.W.; Kim, C.G.; Kim, B.Y.; Kim, J.W. Macular Edema After Cataract Surgery in Eyes with Preoperative Retinal Vein Occlusion. Retina 2018, 38, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Martin, D.F.; Hubbard, G.B.; Srivastava, S.K.; Yan, J.; Bergstrom, C.S.; Aaberg, T.M. Incidence of postvitrectomy macular edema using optical coherence tomography. Ophthalmology 2009, 116, 1531–1537. [Google Scholar] [CrossRef]
- Banker, T.P.; Reilly, G.S.; Jalaj, S.; Weichel, E.D. Epiretinal membrane and cystoid macular edema after retinal detachment repair with small-gauge pars plana vitrectomy. Eur. J. Ophthalmol. 2015, 25, 565–570. [Google Scholar] [CrossRef]
- Wendel, C.; Zakrzewski, H.; Carleton, B.; Etminan, M.; Mikelberg, F.S. Association of Postoperative Topical Prostaglandin Analog or Beta-Blocker Use and Incidence of Pseudophakic Cystoid Macular Edema. J. Glaucoma 2018, 27, 402–406. [Google Scholar] [CrossRef]
- Lee, K.M.; Lee, E.J.; Kim, T.W.; Kim, H. Pseudophakic Macular Edema in Primary Open-Angle Glaucoma: A Prospective Study Using Spectral-Domain Optical Coherence Tomography. Am. J. Ophthalmol. 2017, 179, 97–109. [Google Scholar] [CrossRef]
- Donnenfeld, E.D.; Perry, H.D.; Wittpenn, J.R.; Solomon, R.; Nattis, A.; Chou, T. Preoperative ketorolac tromethamine 0.4% in phacoemulsification outcomes: Pharmacokinetic-response curve. J. Cataract. Refract. Surg. 2006, 32, 1474–1482. [Google Scholar] [CrossRef]
- Yavas, G.F.; Oztürk, F.; Küsbeci, T. Preoperative topical indomethacin to prevent pseudophakic cystoid macular edema. J. Cataract. Refract. Surg. 2007, 33, 804–807. [Google Scholar] [CrossRef]
- Kim, S.J.; Schoenberger, S.D.; Thorne, J.E.; Ehlers, J.P.; Yeh, S.; Bakri, S.J. Topical Nonsteroidal Anti-Inflammatory Drugs and Cataract Surgery: A Report by the American Academy of Ophthalmology. Ophthalmology 2015, 122, 2159–2168. [Google Scholar] [CrossRef]
- Kessel, L.; Tendal, B.; Jørgensen, K.J.; Erngaard, D.; Flesner, P.; Andresen, J.L.; Hjortdal, J. Post-cataract prevention of inflammation and macular edema by steroid and nonsteroidal anti-inflammatory eye drops: A systematic review. Ophthalmology 2014, 121, 1915–1924. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.X.; Lim, C.H.; Lim, D.K.; Evans, J.R.; Bunce, C.; Wormald, R. Prophylactic non-steroidal anti-inflammatory drugs for the prevention of macular oedema after cataract surgery. Cochrane Database Syst. Rev. 2016, 11, CD006683. [Google Scholar] [CrossRef] [PubMed]
- Juthani, V.V.; Clearfield, E.; Chuck, R.S. Non-steroidal anti-inflammatory drugs versus corticosteroids for controlling inflammation after uncomplicated cataract surgery. Cochrane Database Syst. Rev. 2017, 7, CD010516. [Google Scholar] [CrossRef] [PubMed]
- Wielders, L.H.; Schouten, J.S.; Winkens, B.; Biggelaar, F.J.v.D.; Veldhuizen, C.A.; Findl, O.; Murta, J.C.; Goslings, W.R.; Tassignon, M.-J.; Joosse, M.V.; et al. European multicenter trial of the prevention of cystoid macular edema after cataract surgery in nondiabetics: ESCRS PREMED study report 1. J. Cataract. Refract. Surg. 2018, 44, 429–439. [Google Scholar] [CrossRef]
- Shorstein, N.H.; Liu, L.; Waxman, M.D.; Herrinton, L.J. Comparative Effectiveness of Three Prophylactic Strategies to Prevent Clinical Macular Edema After Phacoemulsification Surgery. Ophthalmology 2015, 122, 2450–2456. [Google Scholar] [CrossRef]
- Almeida, D.R.; Khan, Z.; Xing, L.; Bakar, S.N.; Rahim, K.; Urton, T.; El-Defrawy, S.R. Prophylactic nepafenac and ketorolac versus placebo in preventing postoperative macular edema after uneventful phacoemulsification. J. Cataract. Refract. Surg. 2012, 38, 1537–1543. [Google Scholar] [CrossRef]
- Lee, T.H.; Choi, W.; Ji, Y.S.; Yoon, K.C. Comparison of ketorolac 0.45% versus diclofenac 0.1% for macular thickness and volume after uncomplicated cataract surgery. Acta Ophthalmol. 2016, 94, e177–e182. [Google Scholar] [CrossRef]
- Wang, Q.-W.; Yao, K.; Xu, W.; Chen, P.-Q.; Shentu, X.-C.; Xie, X.; Weng, Y.; Zhang, L.; Jin, C.-F.; Wu, W.; et al. Bromfenac sodium 0.1%, fluorometholone 0.1% and dexamethasone 0.1% for control of ocular inflammation and prevention of cystoid macular edema after phacoemulsification. Ophthalmologica 2013, 229, 187–194. [Google Scholar] [CrossRef]
- Wielders, L.H.; Schouten, J.S.; Winkens, B.; Biggelaar, F.J.v.D.; Veldhuizen, C.A.; Murta, J.C.; Goslings, W.R.; Kohnen, T.; Tassignon, M.-J.; Joosse, M.V.; et al. Randomized controlled European multicenter trial on the prevention of cystoid macular edema after cataract surgery in diabetics: ESCRS PREMED Study Report 2. J. Cataract. Refract. Surg. 2018, 44, 836–847. [Google Scholar] [CrossRef]
- McCafferty, S.; Harris, A.; Kew, C.; Kassm, T.; Lane, L.; Levine, J.; Raven, M. Pseudophakic cystoid macular edema prevention and risk factors; prospective study with adjunctive once daily topical nepafenac 0.3% versus placebo. BMC Ophthalmol. 2017, 17, 16. [Google Scholar] [CrossRef]
- Singh, R.; Alpern, L.; Jaffe, G.J.; Lehmann, R.P.; Lim, J.; Reiser, H.J.; Sall, K.; Walters, T.; Sager, D. Evaluation of nepafenac in prevention of macular edema following cataract surgery in patients with diabetic retinopathy. Clin. Ophthalmol. 2012, 6, 1259–1269. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.R.; Dellaporta, A. Natural history of cystoid macular edema after cataract extraction. Am. J. Ophthalmol. 1974, 77, 445–447. [Google Scholar] [CrossRef]
- Sivaprasad, S.; Bunce, C.; Crosby-Nwaobi, R. Non-steroidal anti-inflammatory agents for treating cystoid macular oedema following cataract surgery. Cochrane Database Syst. Rev. 2012, 2, CD004239. [Google Scholar] [CrossRef] [PubMed]
- Thach, A.B.; Dugel, P.U.; Flindall, R.J.; Sipperley, J.O.; Sneed, S.R. A comparison of retrobulbar versus sub-Tenon’s corticosteroid therapy for cystoid macular edema refractory to topical medications. Ophthalmology 1997, 104, 2003–2008. [Google Scholar] [CrossRef] [PubMed]
- Suleman, H.; Mathew, M.; Lakshmanan, A.; Abedin, A.; Orr, G. Orbital floor triamcinolone acetonide in the treatment of pseudophakic cystoid macular oedema. Acta Ophthalmol. 2008, 86, 1. [Google Scholar] [CrossRef]
- Yüksel, B.; Uzunel, U.D.; Kerci, S.G.; Sağban, L.; Küsbeci, T.; Örsel, T. Comparison of Subtenon Triamcinolone Acetonide Injection with Topical Nepafenac for the Treatment of Pseudophakic Cystoid Macular Edema. Ocul. Immunol. Inflamm. 2017, 25, 513–519. [Google Scholar] [CrossRef]
- Koutsandrea, C.; Moschos, M.M.; Brouzas, D.; Loukianou, E.; Apostolopoulos, M.; Moschos, M. Intraocular triamcinolone acetonide for pseudophakic cystoid macular edema: Optical coherence tomography and multifocal electroretinography study. Retina 2007, 27, 159–164. [Google Scholar] [CrossRef]
- Benhamou, N.; Massin, P.; Haouchine, B.; Audren, F.; Tadayoni, R.; Gaudric, A. Intravitreal triamcinolone for refractory pseudophakic macular edema. Am. J. Ophthalmol. 2003, 135, 246–249. [Google Scholar] [CrossRef]
- Bellocq, D.; Pierre-Kahn, V.; Matonti, F.; Burillon, C.; Voirin, N.; Dot, C.; Akesbi, J.; Milazzo, S.; Baillif, S.; Soler, V.; et al. Effectiveness and safety of dexamethasone implants for postsurgical macular oedema including Irvine-Gass syndrome: The EPISODIC-2 study. Br. J. Ophthalmol. 2017, 101, 333–341. [Google Scholar] [CrossRef]
- Mayer, W.J.; Kurz, S.; Wolf, A.; Kook, D.; Kreutzer, T.; Kampik, A.; Priglinger, S.; Haritoglou, C. Dexamethasone implant as an effective treatment option for macular edema due to Irvine-Gass syndrome. J. Cataract. Refract. Surg. 2015, 41, 1954–1961. [Google Scholar] [CrossRef]
- Falavarjani, K.G.; Parvaresh, M.-M.; Modarres, M.; Hashemi, M.; Samiy, N. Intravitreal bevacizumab for pseudophakic cystoid macular edema; a systematic review. J. Ophthalmic Vis. Res. 2012, 7, 235–239. [Google Scholar]


{kind=link}
{kind=link}
| Cataract Extraction Technique | Incidence of Clinical CMO (%) | Incidence of OCT-Based CMO (%) | Incidence of Angiographic CMO (%) |
|---|---|---|---|
| Intracapsular cataract extraction | 8 [6] | Not available | 36–60 [13] |
| Extracapsular cataract extraction | 0.8–20 [7] | Not available | 16–32.2 [14,15,16] |
| Phacoemulsification | 0.1–2.35 [8,9] | 3–41 [11,12] | 20–54.7 [17,18] |
| Femtosecond-assisted cataract surgery | 1.18 [10] | 1.18 [10] | Not available |
| Authors | Risk Factor | Level of Evidence | Study Type (No. of Eyes) | Follow-Up (Months) | Incidence of CMO (%) | Relative Risk (95% Confidence Interval) |
|---|---|---|---|---|---|---|
| Systemic Risk Factors | ||||||
| Diabetes Mellitus (DM) | ||||||
| Chu et al., 2016 [9] | DM without DR | III-2 | Retrospective (81,984) | 3 | 2.15 | 1.80 (1.38–2.36) |
| Ocular Risk Factors | ||||||
| Diabetes Mellitus (DM) | ||||||
| Chu et al., 2016 [9] | DM with any DR | III-2 | Retrospective (81,984) | 3 | 7.27 | 6.23 (5.12–7.58) |
| DM with stable PDR and previous PRP | 10.63 | 9.11 (6.07–13.68) | ||||
| DM with PDR | 12.07 | 10.34 (5.13–20.85) | ||||
| DM with severe NPDR | 7.69 | 6.59 (2.21–19.63) | ||||
| DM with moderate NPDR | 9.95 | 8.53 (5.62–12.93) | ||||
| DM with mild NPDR | 9.43 | 8.08 (6.03–10.85) | ||||
| Schimer et al., 2007 [36] | DM | III-2 | Retrospective (139,759) | 12 | 3.05 | 1.77 (1.62–1.92) |
| Patra et al., 2017 [37] | DM | III-2 | Retrospective (262 eyes) | 12 | 10.7 | 3.06 |
| Uveitis | ||||||
| Chu et al., 2016 [9] | Uveitis | III-2 | Retrospective (81,984) | 3 | 3.36 | 2.88 (1.50–5.51) |
| Belair et al., 2009 [38] | Previous non-infectious uveitis | III-2 | Prospective (93) | 3 | 12 | 3.11 (0.64–15.20) |
| Previous uveitis, but no active uveitis within 3 months of surgery | 6 | 1.55 | ||||
| Previous uveitis and active uveitis within 3 months of surgery | 38 | 9.87 | ||||
| Retinal Vein Occlusion (RVO) | ||||||
| Chu et al., 2016 [9] | Previous RVO | III-2 | Retrospective (81,984) | 3 | 5.22 | 4.47 (2.56–7.82) |
| Henderson et al., 2007 [39] | Previous RVO | III-2 | Retrospective (1659) | 12 | 10.3 | 4.64 |
| Epiretinal membrane (ERM) | ||||||
| Chu et al., 2016 [9] | Pre-existing ERM | III-2 | Retrospective (81,984) | 3 | 6.53 | 5.60 (3.45–9.07) |
| Henderson et al., 2007 [39] | History of ERM | III-2 | Retrospective (1659) | 12 | 7.14 | 3.21 (1.03–10.00) |
| Schaub et al., 2018 [40] | Pre-existing ERM | III-2 | Retrospective (357) | 11 | 15.69 | 2.67 (1.31–5.42) |
| Retinal Detachment (RD) | ||||||
| Chu et al., 2016 [9] | Previous RD repair | III-2 | Retrospective (81,984) | 3 | 4.58 | 3.93 (2.60–5.92) |
| Schaub et al., 2018 [40] | Vitrectomy for RD | III-2 | Retrospective (357) | 11 | 28.13 | 2.86 (1.50–5.44) |
| Glaucoma medications | ||||||
| Chu et al., 2016 [9] | Pre-op prostaglandin use | III-2 | Retrospective (81,984) | 3 | 1.30 | 1.11 (0.82–1.51) |
| Henderson et al., 2007 [39] | Historyof ERM | III-2 | Retrospective (1659) | 12 | 3.4 | 1.53 |
| Intra-Operative Risk Factors | ||||||
| Posterior Capsular Rupture (PCR) | ||||||
| Chu et al., 2016 [9] | PCR +/− vitreous loss | III-2 | Retrospective (81,984) | 3 | 3.05 | 2.61 (1.57–4.34) |
| Law et al., 2010 [41] | PCR + vitrectomy | III-2 | Retrospective (1253) | 3 | 15 | 2.94 (1.35–6.38) |
| Henderson et al., 2000 [39] | PCR +/− vitreous loss | III-2 | Retrospective (1659) | 12 | 12.8 | 5.77 |
| Use of pupil expansion device | ||||||
| Taipale et al., 2019 [42] | Malyugin Ring used | III-2 | Prospective (536) | 3 | 15.0 | 5.41 (1.35–21.71) |
| Authors | Level of Evidence | Study Type (No. of Eyes) | Intervention | Conclusions |
|---|---|---|---|---|
| Pre-Operative NSAID in Non-Diabetics | ||||
| Donnenfeld et al., 2006 [49] | II | RCT (100) | Ketorolac 0.4% prior to surgery for
|
|
| Yavas et al., 2007 [50] | II | RCT (179 eyes) | Indomethacin 0.1% 1 drop 4 times daily for 3 days |
|
| Post-Operative NSAID in Non-Diabetics | ||||
| Kim et al., 2017 [51] | I | Systematic review | NSAID vs. steroid |
|
| Kessel et al., 2014 [52] | I | Systematic review | NSAID vs. steroid |
|
| Lim et al., 2016 [53] | I | Systematic review | NSAID vs. steroid alone vs. NSAID + steroid |
|
| Juthani et al., 2018 [54] | I | Systematic review | NSAID vs. steroid alone vs. NSAID + steroid |
|
| Wielders et al., 2018 [55] | II | RCT (914 eyes) | NSAID vs. steroid alone vs. NSAID + steroid |
|
| Shorstein et al., 2015 [56] | III | Retrospective cohort (16,070 eyes) | NSAID vs. NSAID + steroid |
|
| Comparing Post-Operative NSAID in Non-Diabetics | ||||
| Almeida et al., 2012 [57] | II | RCT (162 eyes) | Ketorolac 0.5% vs. nepafenac 0.1% |
|
| Lee et al., 2015 [58] | III | Retrospective cohort (76 eyes) | Ketorolac 0.45% vs. diclofenac 0.1% |
|
| Wang et al., 2013 [59] | II | RCT (167 eyes) | Bromfenac 0.1% vs. fluoromethalone 0.1% |
|
| Intra-Operative Treatment in Diabetics | ||||
| Wielders et al., 2018 [60] | III | RCT (213 eyes) | Subconjunctival 40 mg triamcinolone vs. intravitreal 1.25 mg bevacizumab vs. no treatment |
|
| Post-Operative NSAID in diabetics | ||||
| Henderson et al., 2007 [39] | III | Retrospective cohort (1659) | Ketorolac 0.5% or diclofenac 0.1% |
|
| McCafferty et al., 2017 [61] | II | RCT (1000 eyes) | Nepafenac 0.3% vs. placebo |
|
| Pre and Post-Operative NSAID in Diabetics | ||||
| Singh et al., 2012 [62] | II | RCT (263 eyes) | Nepafenac vs. placebo from day 1 prior to surgery to day 90 post surgery |
|
| Authors | Level of Evidence | Study Type (No. of Eyes) | Intervention | Conclusions |
|---|---|---|---|---|
| Topical Therapy | ||||
| Sivaprasad et al., 2012 [64] | I | Systematic review | Topical NSAID, oral NSAID | Acute CMO
|
| Periocular Steroids | ||||
| Thach et al., 1997 [65] | III | Retrospective cohort (49 eyes) | Retrobulbar TCA vs. Subtenons TCA |
|
| Suleman et al., 2008 [66] | IV | Case series (6 eyes) | Orbital floor TCA |
|
| Periocular Steroid vs. Topical NSAID | ||||
| Yuksel et al., 2017 [67] | III | Prospective randomized (48 eyes) | Nepafenac drops vs. single sub-Tenons triamcinolone |
|
| Intravitreal Steroid Injection | ||||
| Koutsandrea et al., 2007 [68] | IV | Retrospective case series (14 eyes) | Intravitreal TCA |
|
| Benhamou et al., 2003 [69] | IV | Prospective case series (3 eyes) | Intravitreal 8 mg TCA |
|
| Intravitreal Dexamethasone Implant | ||||
| Bellocq et al., 2017 [70] | IV | Retrospective (58 eyes) | Ozurdex implant |
|
| Mayer et al. [71] | III | Prospective case series (23 eyes) | Ozurdex implant |
|
| Intravitreal Bevacizumab | ||||
| Falavarjani et al., 2012 [72] | I | Systematic review | Intravitreal bevacizumab |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferro Desideri, L.; Arun, K.; Bernardi, E.; Sagurski, N.; Anguita, R. Incidence, Pathogenesis, Risk Factors, and Treatment of Cystoid Macula Oedema Following Cataract Surgery: A Systematic Review. Diagnostics 2025, 15, 667. https://doi.org/10.3390/diagnostics15060667
Ferro Desideri L, Arun K, Bernardi E, Sagurski N, Anguita R. Incidence, Pathogenesis, Risk Factors, and Treatment of Cystoid Macula Oedema Following Cataract Surgery: A Systematic Review. Diagnostics. 2025; 15(6):667. https://doi.org/10.3390/diagnostics15060667
Chicago/Turabian StyleFerro Desideri, Lorenzo, Kirupakaran Arun, Enrico Bernardi, Nicola Sagurski, and Rodrigo Anguita. 2025. "Incidence, Pathogenesis, Risk Factors, and Treatment of Cystoid Macula Oedema Following Cataract Surgery: A Systematic Review" Diagnostics 15, no. 6: 667. https://doi.org/10.3390/diagnostics15060667
APA StyleFerro Desideri, L., Arun, K., Bernardi, E., Sagurski, N., & Anguita, R. (2025). Incidence, Pathogenesis, Risk Factors, and Treatment of Cystoid Macula Oedema Following Cataract Surgery: A Systematic Review. Diagnostics, 15(6), 667. https://doi.org/10.3390/diagnostics15060667