
Factors Influencing the Development of Metachronous Fractures in Patients with Osteoporotic Vertebral Fractures Treated with Conservative Management or Vertebroplasty

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
- Patients diagnosed with acute OVF by X-rays and CT.
- Patients with radiological follow-up of their fracture at least 12 months after diagnosis.
- Management with CM or PV (in the latter case, during the first 6 months after diagnosis).
- Lack of follow-up X-rays and/or CT at least 12 months after initial diagnosis.
- Presence of two or more simultaneous OVFs.
- Patients treated by spinal surgery prior to the diagnosis of OVF or during follow-up.
- Patients with non-diagnostic-quality imaging examinations.
2.2. Study Variables
- Morphological (wedge-shaped, biconcave, crush) and quantitative (grade 0, 1, 2, 3) classifications by Genant (34).
- Classification of the German Society of Orthopedics and Traumatology (DGOU) (OF2-OF5) (35).
- Classification of the AO Spine (A1 to A4) (32,33).
- Sugita classification (swelled-front, bow-shaped, projecting, concave, dented) (36).
2.3. Statistical Analysis
3. Results
3.1. Main Characteristics of Patients and Vertebral Fractures in Our Sample
3.2. Variables Associated with the Development of Metachronous Vertebral Fractures
3.3. Predictors for the Development of Metachronous Vertebral Fractures
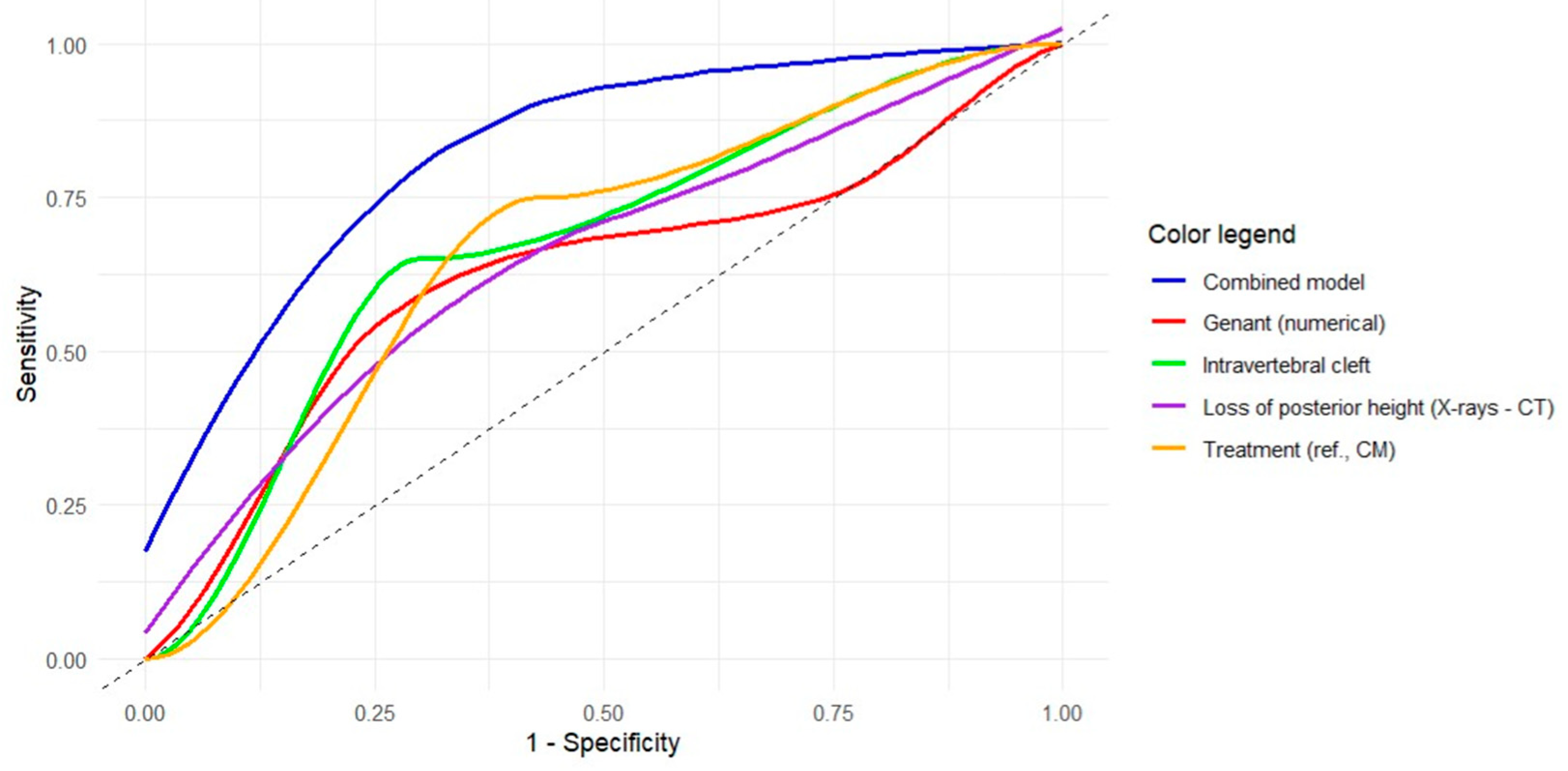
3.4. Discriminative Power of the Models for Predicting Metachronous Fractures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xie, L.; Zhao, Z.G.; Zhang, S.J.; Hu, Y. Bin Percutaneous Vertebroplasty versus Conservative Treatment for Osteoporotic Vertebral Compression Fractures: An Updated Meta-Analysis of Prospective Randomized Controlled Trials. Int. J. Surg. 2017, 47, 25–32. [Google Scholar] [CrossRef]
- Yamauchi, K.; Adachi, A.; Kameyama, M.; Murakami, M.; Sato, Y.; Kato, C.; Kato, T. A Risk Factor Associated with Subsequent New Vertebral Compression Fracture after Conservative Therapy for Patients with Vertebral Compression Fracture: A Retrospective Observational Study. Arch. Osteoporos. 2020, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.A.; McCabe, E.; Bergin, D.; Kearns, S.R.; McCabe, J.P.; Armstrong, C.; Heaney, F.; Carey, J.J. Osteoporotic Vertebral Fractures Are Common in Hip Fracture Patients and Are Under-Recognized. J. Clin. Densitom. 2021, 24, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Sun, R.; Zhang, S.D.; Wu, X.T. Comparison of Acute Single versus Multiple Osteoporotic Vertebral Compression Fractures in Radiographic Characteristic and Bone Fragility. J. Orthop. Surg. Res. 2023, 18, 1–10. [Google Scholar] [CrossRef]
- Kano, S.; Tanikawa, H.; Mogami, Y.; Shibata, S.I.; Takanashi, S.; Oji, Y.; Aoki, T.; Oba, H.; Ikegami, S.; Takahashi, J. Comparison between Continuous and Discontinuous Multiple Vertebral Compression Fractures. Eur. Spine J. 2012, 21, 1867–1872. [Google Scholar] [CrossRef]
- Langdahl, B.L.; Harsløf, T. Medical Treatment of Osteoporotic Vertebral Fractures. Ther. Adv. Musculoskelet. Dis. 2011, 3, 17–29. [Google Scholar] [CrossRef]
- Jang, H.D.; Kim, E.H.; Lee, J.C.; Choi, S.W.; Kim, H.S.; Cha, J.S.; Shin, B.J. Management of Osteoporotic Vertebral Fracture: Review Update 2022. Asian Spine J. 2022, 16, 934–946. [Google Scholar] [CrossRef]
- Anselmetti, G.C.; Bernard, J.; Blattert, T.; Court, C.; Fagan, D.; Fransen, H.; Fransen, P.; Sabharwal, T.; Schils, F.; Schupfner, R.; et al. Criteria for the Appropriate Treatment of Osteoporotic Vertebral Compression Fractures. Pain. Physician 2013, 16, 519–530. [Google Scholar] [CrossRef]
- Patel, D.; Liu, J.; Ebraheim, N.A. Managements of Osteoporotic Vertebral Compression Fractures: A Narrative Review. World J. Orthop. 2022, 13, 564–573. [Google Scholar] [CrossRef]
- Tu, P.H.; Liu, Z.H.; Lee, S.T.; Chen, J.F. Treatment of Repeated and Multiple New-Onset Osteoporotic Vertebral Compression Fractures with Teriparatide. J. Clin. Neurosci. 2012, 19, 532–535. [Google Scholar] [CrossRef]
- Jang, H.-D.; Kim, E.-H.; Lee, J.C.; Choi, S.-W.; Kim, K.; Shin, B.-J. Current Concepts in the Management of Osteoporotic Vertebral Fractures: A Narrative Review. Asian Spine J. 2020, 14, 898–909. [Google Scholar] [CrossRef] [PubMed]
- Slavici, A.; Rauschmann, M.; Fleege, C. Conservative Management of Osteoporotic Vertebral Fractures: An Update. Eur. J. Trauma. Emerg. Surg. 2017, 43, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Saracen, A.; Kotwica, Z. Treatment of Multiple Osteoporotic Vertebral Compression Fractures by Percutaneous Cement Augmentation. Int. Orthop. 2014, 38, 2309–2312. [Google Scholar] [CrossRef]
- Galibert, P.; Deramond, H.; Rosat, P.; Le Gars, D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie 1987, 33, 166–168. [Google Scholar]
- Kushchayev, S.V.; Wiener, P.C.; Teytelboym, O.M.; Arrington, J.A.; Khan, M.; Preul, M.C. Percutaneous Vertebroplasty: A History of Procedure, Technology, Culture, Specialty, and Economics. Neuroimaging Clin. N. Am. 2019, 29, 481–494. [Google Scholar] [CrossRef]
- Ruiz Santiago, F.; Pérez Abela, A.L.; Almagro Ratia, M.M. El Final de Las Vertebroplastias. Radiologia 2012, 54, 532–538. [Google Scholar] [CrossRef]
- Zhai, W.; Jia, Y.; Wang, J.; Cheng, L.; Zeng, Z.; Yu, Y.; Chen, L. The Clinical Effect of Percutaneous Kyphoplasty for the Treatment of Multiple Osteoporotic Vertebral Compression Fractures and the Prevention of New Vertebral Fractures. Int. J. Clin. Exp. Med. 2015, 8, 13473–13481. [Google Scholar]
- Kallmes, D.F.; Comstock, B.A.; Heagerty, P.J.; Turner, J.A.; Wilson, D.J.; Diamond, T.H.; Edwards, R.; Gray, L.A.; Stout, L.; Owen, S.; et al. A Randomized Trial of Vertebroplasty for Osteoporotic Spinal Fractures. N. Engl. J. Med. 2009, 361, 569–579. [Google Scholar] [CrossRef]
- Buchbinder, R.; Osborne, R.H.; Ebeling, P.R.; Wark, J.D.; Mitchell, P.; Wriedt, C.; Graves, S.; Staples, M.P.; Murphy, B. A Randomized Trial of Vertebroplasty for Painful Osteoporotic Vertebral Fractures. N. Engl. J. Med. 2009, 361, 557–568. [Google Scholar] [CrossRef]
- Dai, C.; Liang, G.; Zhang, Y.; Dong, Y.; Zhou, X. Risk Factors of Vertebral Re-Fracture after PVP or PKP for Osteoporotic Vertebral Compression Fractures, Especially in Eastern Asia: A Systematic Review and Meta-Analysis. J. Orthop. Surg. Res. 2022, 17, 161. [Google Scholar] [CrossRef]
- Zhang, Z.L.; Yang, J.S.; Hao, D.J.; Liu, T.J.; Jing, Q.M. Risk Factors for New Vertebral Fracture after Percutaneous Vertebroplasty for Osteoporotic Vertebral Compression Fractures. Clin. Interv. Aging 2021, 16, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, R.; Johnston, R.V.; Rischin, K.J.; Homik, J.; Jones, C.A.; Golmohammadi, K.; Kallmes, D.F. Percutaneous Vertebroplasty for Osteoporotic Vertebral Compression Fracture. Cochrane Database Syst. Rev. 2018, 2018, CD006349. [Google Scholar]
- Clark, W.; Bird, P.; Gonski, P.; Diamond, T.H.; Smerdely, P.; McNeil, H.P.; Schlaphoff, G.; Bryant, C.; Barnes, E.; Gebski, V. Safety and Efficacy of Vertebroplasty for Acute Painful Osteoporotic Fractures (VAPOUR): A Multicentre, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2016, 388, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Carli, D.; Venmans, A.; Lodder, P.; Donga, E.; van Oudheusden, T.; Boukrab, I.; Schoemaker, K.; Smeets, A.; Schonenberg, C.; Hirsch, J.; et al. Vertebroplasty versus Active Control Intervention for Chronic Osteoporotic Vertebral Compression Fractures: The VERTOS V Randomized Controlled Trial. Radiology 2023, 308, e222535. [Google Scholar] [CrossRef]
- Láinez Ramos-Bossini, A.J.; López Zúñiga, D.; Ruiz Santiago, F. Percutaneous Vertebroplasty versus Conservative Treatment and Placebo in Osteoporotic Vertebral Fractures: Meta-Analysis and Critical Review of the Literature. Eur. Radiol. 2021, 31, 8542–8553. [Google Scholar] [CrossRef]
- Papanastassiou, I.D.; Filis, A.; Aghayev, K.; Kokkalis, Z.T.; Gerochristou, M.A.; Vrionis, F.D. Adverse Prognostic Factors and Optimal Intervention Time for Kyphoplasty/Vertebroplasty in Osteoporotic Fractures. Biomed. Res. Int. 2014, 2014, 925683. [Google Scholar] [CrossRef]
- Gazzotti, M.R.; Roco, C.M.; Pradella, C.O.; Nascimento, O.A.; Porto, E.F.; Adas, M.; Lazaretti-Castro, M.; Jardim, J.R. Frequency of Osteoporosis and Vertebral Fractures in Chronic Obstructive Pulmonary Disease (COPD) Patients. Arch. Bronconeumol. 2019, 55, 252–257. [Google Scholar] [CrossRef]
- Gifre, L.; Massó, E.; Fusaro, M.; Haarhaus, M.; Ureña, P.; Cozzolino, M.; Mazzaferro, S.; Calabia, J.; Peris, P.; Bover, J. Vertebral Fractures in Patients with CKD and the General Population: A Call for Diagnosis and Action. Clin. Kidney J. 2024, 17, sfae191. [Google Scholar] [CrossRef]
- Ruiz Santiago, F.; Láinez Ramos-Bossini, A.J.; Wáng, Y.X.J.; López Zúñiga, D. The Role of Radiography in the Study of Spinal Disorders. Quant. Imaging Med. Surg. 2020, 10, 2322–2355. [Google Scholar] [CrossRef]
- Ruiz Santiago, F.; Láinez Ramos-Bossini, A.; Wáng, Y.X.J.; Martínez Barbero, J.; García Espinosa, J.; Martínez Martínez, A. The Value of Magnetic Resonance Imaging and Computed Tomography in the Study of Spinal Disorders. Quant. Imaging Med. Surg. 2022, 12, 3947–3986. [Google Scholar] [CrossRef]
- Muratore, M.; Ferrera, A.; Masse, A.; Bistolfi, A. Osteoporotic Vertebral Fractures: Predictive Factors for Conservative Treatment Failure. A Systematic Review. Eur. Spine J. 2018, 27, 2565–2576. [Google Scholar] [CrossRef] [PubMed]
- Ruiz Santiago, F.; Láinez Ramos-Bossini, A.J.; Moraleda-Cabrera, B. Factors Influencing Vertebral Collapse in Osteoporotic Vertebral Fractures: A Case-Control Study of Symptomatic Patients Attended in the Emergency Department. Arch. Osteoporos. 2023, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Kepler, C.K.; Vaccaro, A.R.; Koerner, J.D.; Dvorak, M.F.; Kandziora, F.; Rajasekaran, S.; Aarabi, B.; Vialle, L.R.; Fehlings, M.G.; Schroeder, G.D.; et al. Reliability Analysis of the AOSpine Thoracolumbar Spine Injury Classification System by a Worldwide Group of Naïve Spinal Surgeons. Eur. Spine J. 2016, 25, 1082–1086. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Oner, C.; Kepler, C.K.; Dvorak, M.; Schnake, K.; Bellabarba, C.; Reinhold, M.; Aarabi, B.; Kandziora, F.; Chapman, J.; et al. AOSpine Thoracolumbar Spine Injury Classification System. Spine (Phila. Pa. 1976) 2013, 38, 2028–2037. [Google Scholar] [CrossRef]
- Hounsfield, G.N. Computed Medical Imaging. J. Comput. Assist. Tomogr. 1980, 4, 665–674. [Google Scholar] [CrossRef]
- Trout, A.T.; Kallmes, D.F. Does Vertebroplasty Cause Incident Vertebral Fractures? A Review of Available Data. AJNR Am. J. Neuroradiol. 2006, 27, 1397–1403. [Google Scholar]
- Wang, J.; Chen, M.; Du, J. Therapeutic effect of conservative treatment of refracture in cemented vertebrae after percutaneous vertebroplasty for osteoporotic vertebral compression fractures. Nan Fang. Yi Ke Da Xue Xue Bao 2016, 36, 277–281. [Google Scholar]
- Okamoto, Y.; Murakami, H.; Demura, S.; Kato, S.; Yoshioka, K.; Hayashi, H.; Sakamoto, J.; Kawahara, N.; Tsuchiya, H. The Effect of Kyphotic Deformity Because of Vertebral Fracture: A Finite Element Analysis of a 10° and 20° Wedge-Shaped Vertebral Fracture Model. Spine J. 2015, 15, 713–720. [Google Scholar] [CrossRef]
- Huang, M.-H.; Barrett-Connor, E.; Greendale, G.A.; Kado, D.M. Hyperkyphotic Posture and Risk of Future Osteoporotic Fractures: The Rancho Bernardo Study. J. Bone Min. Res. 2006, 21, 419–423. [Google Scholar] [CrossRef]
- Ha, K.Y.; Kim, Y.H. Risk Factors Affecting Progressive Collapse of Acute Osteoporotic Spinal Fractures. Osteoporos. Int. 2013, 24, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Tsujio, T.; Nakamura, H.; Terai, H.; Hoshino, M.; Namikawa, T.; Matsumura, A.; Kato, M.; Suzuki, A.; Takayama, K.; Fukushima, W.; et al. Characteristic Radiographic or Magnetic Resonance Images of Fresh Osteoporotic Vertebral Fractures Predicting Potential Risk for Nonunion. Spine (Phila. Pa. 1976) 2011, 36, 1229–1235. [Google Scholar] [CrossRef]
- Farrokhi, M.R.; Alibai, E.; Maghami, Z. Randomized Controlled Trial of Percutaneous Vertebroplasty versus Optimal Medical Management for the Relief of Pain and Disability in Acute Osteoporotic Vertebral Compression Fractures: Clinical Article. J. Neurosurg. Spine 2011, 14, 561–569. [Google Scholar] [CrossRef]
- Láinez Ramos-Bossini, A.J.; Jiménez Gutiérrez, P.M.; Moraleda Cabrera, B.; Bueno Caravaca, L.; González Díez, M.; Ruiz Santiago, F. Risk of New Vertebral Compression Fractures and Serious Adverse Effects after Vertebroplasty: A Critical Review and Meta-Analysis of Randomized Controlled Trials. Quant. Imaging Med. Surg. 2024, 14, 7848–7861. [Google Scholar] [CrossRef]
- Blasco, J.; Martinez-Ferrer, A.; Macho, J.; San Roman, L.; Pomés, J.; Carrasco, J.; Monegal, A.; Guañabens, N.; Peris, P. Effect of Vertebroplasty on Pain Relief, Quality of Life, and the Incidence of New Vertebral Fractures: A 12-Month Randomized Follow-up, Controlled Trial. J. Bone Miner. Res. 2012, 27, 1159–1166. [Google Scholar] [CrossRef]
- Huang, P.-H.; Chen, C.-W.; Hu, M.-H.; Yang, S.-H.; Huang, C.-C. Risk Factors of Failed Conservative Treatment for Adjacent Vertebral Fractures Following Percutaneous Vertebroplasty. Spine (Phila. Pa. 1976) 2024. [Google Scholar] [CrossRef]
- Han, S.L.; Wan, S.L.; Li, Q.T.; Xu, D.T.; Zang, H.M.; Chen, N.J.; Chen, L.Y.; Zhang, W.P.; Luan, C.; Yang, F.; et al. Is Vertebroplasty a Risk Factor for Subsequent Vertebral Fracture, Meta-Analysis of Published Evidence? Osteoporos. Int. 2015, 26, 113–122. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Sample (N = 90) X ± SD/N (%) | Vertebroplasty (n = 45) X ± SD/N (%) | Cons. Management (n = 45) X ± SD/N (%) | p-Value |
|---|---|---|---|---|
| Sex (female) | 67 (74.4) | 31 (68.9) | 36 (80) | 0.227 |
| Age | 72.5 ± 9.5 | 72.6 ± 10.3 | 72.3 ± 8.8 | 0.860 |
| Follow-up | 24.6 ± 20.9 | 27.3 ± 26.3 | 21.9 ± 13.3 | 0.226 |
| Cause of Fracture | 0.629 | |||
| Fall from standing height | 77 (85.6) | 37 (82.2) | 40 (88.9) | |
| Spontaneous | 6 (6.7) | 4 (8.9) | 2 (4.4) | |
| Stress | 7 (7.8) | 4 (8.9) | 3 (6.7) | |
| Fracture Level | 0.315 | |||
| T7 | 3 (3.3) | 2 (4.4) | 1 (2.2) | |
| T8 | 3 (3.3) | 3 (6.7) | 0 (0) | |
| T11 | 8 (8.9) | 4 (8.9) | 4 (8.9) | |
| T12 | 13 (14.4) | 7 (15.6) | 6 (13.3) | |
| L1 | 34 (37.8) | 12 (26.7) | 22 (48.9) | |
| L2 | 13 (14.4) | 8 (17.8) | 5 (11.1) | |
| L3 | 7 (7.8) | 4 (8.9) | 3 (6.7) | |
| L4 | 7 (7.8) | 3 (6.7) | 4 (8.9) | |
| L5 | 2 (2.2) | 2 (4.4) | 0 (0) | |
| Fracture Type AO Spine | 0.446 | |||
| A1 | 47 (52.2) | 23 (51.1) | 24 (53.3) | |
| A2 | 2 (2.2) | 2 (4.4) | 0 (0) | |
| A3 | 29 (32.2) | 13 (28.9) | 16 (35.6) | |
| A4 | 12 (13.3) | 7 (15.6) | 5 (11.1) | |
| Fracture Type DGOU | 0.602 | |||
| OF2 | 67 (74.4) | 33 (73.3) | 34 (75.6) | |
| OF3 | 22 (24.4) | 11 (24.4) | 11 (24.4) | |
| OF4 | 1 (1.1) | 1 (2.2) | 0 (0) | |
| Fracture Type Sugita | 0.381 | |||
| Swelled-front | 19 (21.1) | 13 (28.9) | 6 (13.3) | |
| Bow-shaped | 33 (36.7) | 16 (35.6) | 17 (37.8) | |
| Projecting | 12 (13.3) | 4 (8.9) | 8 (17.8) | |
| Concave | 21 (23.3) | 10 (22.2) | 11 (24.4) | |
| Dented | 5 (5.6) | 2 (4.4) | 3 (6.7) | |
| Fracture Type Genant m. | 0.580 | |||
| Wedge | 42 (46.7) | 21 (46.7) | 23 (51.1) | |
| Biconcave | 44 (48.9) | 21 (46.7) | 21 (46.7) | |
| Crush | 4 (4.4) | 3 (6.7) | 1 (2.2) | |
| Fracture Type Genant n. | <0.001 * | |||
| 0.5 | 23 (25.6) | 1 (2.2) | 22 (48.9) | |
| 1 | 38 (42.2) | 29 (64.4) | 9 (20) | |
| 2 | 29 (32.2) | 15 (33.3) | 14 (31.1) | |
| Metachronous fractures | 20 (22.2) | 5 (11.1) | 15 (33.3) | 0.022 * |
| Variable | Total Sample (N = 90) X ± SD/N (%) | Vertebroplasty (n = 45) X ± SD/N (%) | Cons. Management (n = 45) X ± SD/N (%) | p-Value |
|---|---|---|---|---|
| Intravertebral cleft | 34 (37.8) | 13 (28.9) | 21 (46.7) | 0.082 |
| Healthy vertebra density | 87.3 ± 32.3 | 88.6 ± 33.0 | 86.0 ± 32.0 | 0.703 |
| Fractured vertebra density | 139.6 ± 52.0 | 158.4 ± 54.1 | 120.8 ± 42.7 | <0.001 * |
| Aorta density | 42.3 ± 14.5 | 42.1 ± 8.2 | 39.8 ± 5.0 | 0.124 |
| Fracture/non-fracture density ratio | 1.9 ± 1.5 | 2.1 ± 1.9 | 1.6 ± 0.7 | 0.062 |
| Fracture/aorta density ratio | 3.5 ± 1.5 | 3.8 ± 1.5 | 3.1 ± 1.4 | 0.030 |
| Loss of anterior height (X-rays) | 26.1 ± 15.8 | 29.3 ± 17.8 | 22.9 ± 12.9 | 0.054 |
| Loss of middle height (X-rays) | 29.9 ± 12.3 | 32.4 ± 13.2 | 27.4 ± 11.0 | 0.052 |
| Loss of posterior height (X-rays) | 9.5 ± 10.3 | 12.3 ± 11.1 | 6.7 ± 8.7 | 0.009 * |
| Loss of anterior height (CT) | 19.5 ± 14.1 | 23.5 ± 14.9 | 15.6 ± 12.1 | 0.007 * |
| Loss of middle height (CT) | 25.5 ± 14.1 | 28.1 ± 15.5 | 22.8 ± 12.2 | 0.074 |
| Loss of posterior height (CT) | 7.8 ± 8.5 | 9.7 ± 10.0 | 5.9 ± 6.1 | 0.032 * |
| Loss of anterior height (X-rays–CT) | 6.6 ± 9.2 | 5.9 ± 8.9 | 7.4 ± 9.7 | 0.436 |
| Loss of middle height (X-rays–CT) | 4.4 ± 11.5 | 4.3 ± 11.2 | 4.6 ± 12.0 | 0.912 |
| Loss of posterior height (X-rays–CT) | 1.7 ± 8.2 | 2.6 ± 7.3 | 0.8 ± 8.9 | 0.305 |
| Variable | Total Sample (N = 90) | New Fractures (n = 20) | No New Fractures (n = 70) | p-Value |
|---|---|---|---|---|
| Treatment | 0.022 * | |||
| Percutaneous vertebroplasty | 45 (50) | 5 (25) | 40 (57.1) | |
| Conservative management | 45 (50) | 15 (75) | 30 (42.9) | |
| Sex (Female) | 67 (74.4) | 17 (85) | 50 (71.4) | 0.220 |
| Age | 72.5 ± 9.5 | 71.6 ± 7.3 | 72.7 ± 10.1 | 0.564 |
| Follow-up | 24.6 ± 20.9 | 23.5 ± 15.0 | 24.9 ± 22.4 | 0.784 |
| Cause | 0.380 | |||
| Spontaneous | 6 (6.7) | 0 (0) | 6 (8.6) | |
| Stress | 7 (7.8) | 2 (10) | 5 (7.1) | |
| Fall from standing height | 77 (85.5) | 18 (90) | 59 (84.3) | |
| Fracture Type (AO Spine) | 0.162 | |||
| A1 | 47 (52.2) | 7 (35) | 40 (57.1) | |
| A2 | 2 (2.2) | 0 (0) | 2 (2.9) | |
| A3 | 29 (32.2) | 8 (40) | 21 (30) | |
| A4 | 12 (13.3) | 5 (25) | 7 (7.8) | |
| Fracture Type (DGOU) | 0.057 | |||
| OF2 | 67 (74.4) | 11 (55) | 56 (80) | |
| OF3 | 22 (24.4) | 9 (45) | 13 (18.6) | |
| OF4 | 1 (1.1) | 0 (0) | 1 (1.4) | |
| Fracture Type (Sugita) | 0.501 | |||
| Swelled-front | 19 (21.1) | 3 (15) | 16 (22.9) | |
| Bow-shaped | 33 (36.7) | 9 (45) | 24 (34.3) | |
| Projecting | 12 (13.3) | 4 (20) | 8 (11.4) | |
| Concave | 21 (23.3) | 4 (20) | 17 (24.3) | |
| Dented | 5 (5.6) | 0 (0) | 5 (7.1) | |
| Fracture Type (Genant morphol.) | 0.665 | |||
| Wedge | 42 (46.7) | 11 (55) | 36 (51.4) | |
| Biconcave | 44 (48.9) | 8 (40) | 31 (44.3) | |
| Crush | 4 (4.4) | 1 (5) | 3 (4.3) | |
| Fracture type (Genant numerical) | 0.028 * | |||
| 0.5 | 23 (25.6) | 5 (25) | 18 (25.7) | |
| 1 | 38 (42.2) | 4 (20) | 34 (48.6) | |
| 2 | 29 (32.2) | 11 (55) | 13 (18.6) | |
| Intravertebral cleft | 34 (37.8) | 13 (65) | 21 (30) | 0.004 * |
| Healthy vertebra density | 87.3 ± 32.3 | 89.6 ± 30.5 | 79.2 ± 37.8 | 0.209 |
| Fractured vertebra density | 139.6 ± 52.0 | 136.9 ± 52.1 | 149.1 ± 51.9 | 0.360 |
| Aorta density | 42.3 ± 14.5 | 40.6 ± 5.6 | 42.2 ± 10.2 | 0.378 |
| Fracture-to-healthy vertebra density ratio | 1.9 ± 1.5 | 1.8 ± 1.5 | 2.2 ± 1.2 | 0.205 |
| Fracture-to-aorta density ratio | 3.5 ± 1.5 | 3.4 ± 1.4 | 3.5 ± 1.8 | 0.067 |
| Loss of anterior height (X-rays) | 26.1 ± 15.8 | 24.9 ± 16.5 | 30.5 ± 12.2 | 0.162 |
| Loss of middle height (X-rays) | 29.9 ± 12.3 | 30.2 ± 12.4 | 28.9 ± 12.4 | 0.677 |
| Loss of posterior height (X-rays) | 9.5 ± 10.3 | 9.4 ± 10.4 | 9.5 ± 10.4 | 0.961 |
| Loss of anterior height (CT) | 19.5 ± 14.1 | 18.2 ± 14.8 | 24.2 ± 10.2 | 0.093 |
| Loss of middle height (CT) | 25.5 ± 14.1 | 24.7 ± 14.5 | 28.2 ± 12.7 | 0.329 |
| Loss of posterior height (CT) | 7.8 ± 8.5 | 10.9 ± 7.6 | 6.9 ± 8.5 | 0.058 |
| Loss of anterior height (X-rays–CT) | 6.6 ± 9.2 | 6.7 ± 9.3 | 6.3 ± 9.4 | 0.873 |
| Loss of middle height (X-rays–CT) | 4.4 ± 11.5 | 5.5 ± 11.2 | 0.7 ± 12.1 | 0.100 |
| Loss of posterior height (X-rays–CT) | 1.7 ± 8.2 | −1.5 ± 8.0 | 2.6 ± 8.0 | 0.042 * |
| Variable | cOR [95%CI] | p-Value U | aOR [95%CI] | p-Value M |
|---|---|---|---|---|
| Treatment [Ref: CM] | 0.250 [0.075–0.724] | 0.015 | 0.050 [0.006–0.253] ^ | 0.001 * |
| Genant (numerical) | 1.720 [0.879–3.560] | 0.123 | 1.97 [0.983–4.190] | 0.064 |
| Intravertebral cleft | 4.330 [1.550–13.000] | 0.006 | 5.62 [1.840–19.200] | 0.003 * |
| Loss of posterior height (X-rays–CT) | 0.930 [0.862–0.995] | 0.047 | 0.926 [0.856–0.992] | 0.038 * |
| Variable | AUC [95%CI] | p-Value |
|---|---|---|
| Treatment [Ref: CM] | 0.660 [0.547–0.774] | 0.012 * |
| Genant (numerical) | 0.611 [0.462–0.761] | 0.107 |
| Intravertebral cleft | 0.675 [0.555–0.795] | 0.005 * |
| Loss of posterior height (X-rays–CT) | 0.660 [0.519–0.802] | 0.030 * |
| Combined model (3 variables) | 0.781 [0.672–0.891] | <0.001 * |
| Combined model (4 variables) | 0.828 [0.725–0.930] | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz Santiago, F.; Bueno Caravaca, L.; Garrido Sanz, F.; Jiménez Gutiérrez, P.M.; Luengo Gómez, D.; Rivera Izquierdo, M.; Benítez, J.M.; Láinez Ramos-Bossini, A.J. Factors Influencing the Development of Metachronous Fractures in Patients with Osteoporotic Vertebral Fractures Treated with Conservative Management or Vertebroplasty. Diagnostics 2025, 15, 160. https://doi.org/10.3390/diagnostics15020160
Ruiz Santiago F, Bueno Caravaca L, Garrido Sanz F, Jiménez Gutiérrez PM, Luengo Gómez D, Rivera Izquierdo M, Benítez JM, Láinez Ramos-Bossini AJ. Factors Influencing the Development of Metachronous Fractures in Patients with Osteoporotic Vertebral Fractures Treated with Conservative Management or Vertebroplasty. Diagnostics. 2025; 15(2):160. https://doi.org/10.3390/diagnostics15020160
Chicago/Turabian StyleRuiz Santiago, Fernando, Lucía Bueno Caravaca, Francisco Garrido Sanz, Paula María Jiménez Gutiérrez, David Luengo Gómez, Mario Rivera Izquierdo, José Manuel Benítez, and Antonio Jesús Láinez Ramos-Bossini. 2025. "Factors Influencing the Development of Metachronous Fractures in Patients with Osteoporotic Vertebral Fractures Treated with Conservative Management or Vertebroplasty" Diagnostics 15, no. 2: 160. https://doi.org/10.3390/diagnostics15020160
APA StyleRuiz Santiago, F., Bueno Caravaca, L., Garrido Sanz, F., Jiménez Gutiérrez, P. M., Luengo Gómez, D., Rivera Izquierdo, M., Benítez, J. M., & Láinez Ramos-Bossini, A. J. (2025). Factors Influencing the Development of Metachronous Fractures in Patients with Osteoporotic Vertebral Fractures Treated with Conservative Management or Vertebroplasty. Diagnostics, 15(2), 160. https://doi.org/10.3390/diagnostics15020160