
The Mechanical Power in Patients with Acute Respiratory Distress Syndrome Undergoing Prone Positioning Can Predict Mortality

 , , , , , ,
, , , , , ,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Ventilator Settings
2.3. Prone Positioning
2.4. Definition of MP Derivation
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Ventilator Parameters
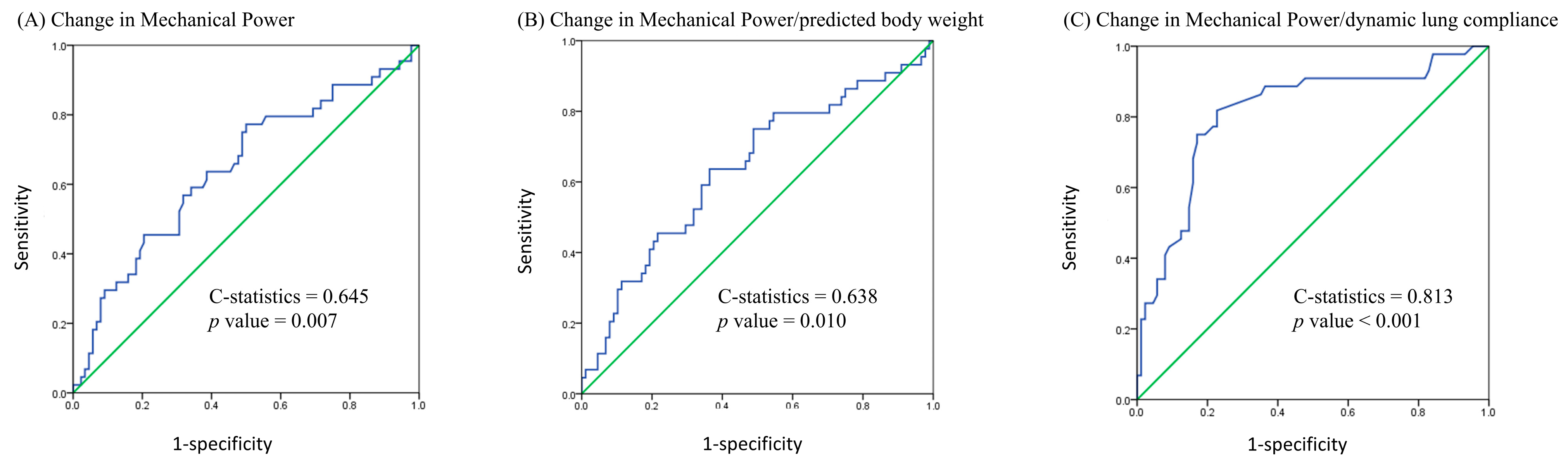
3.3. MP Derivation
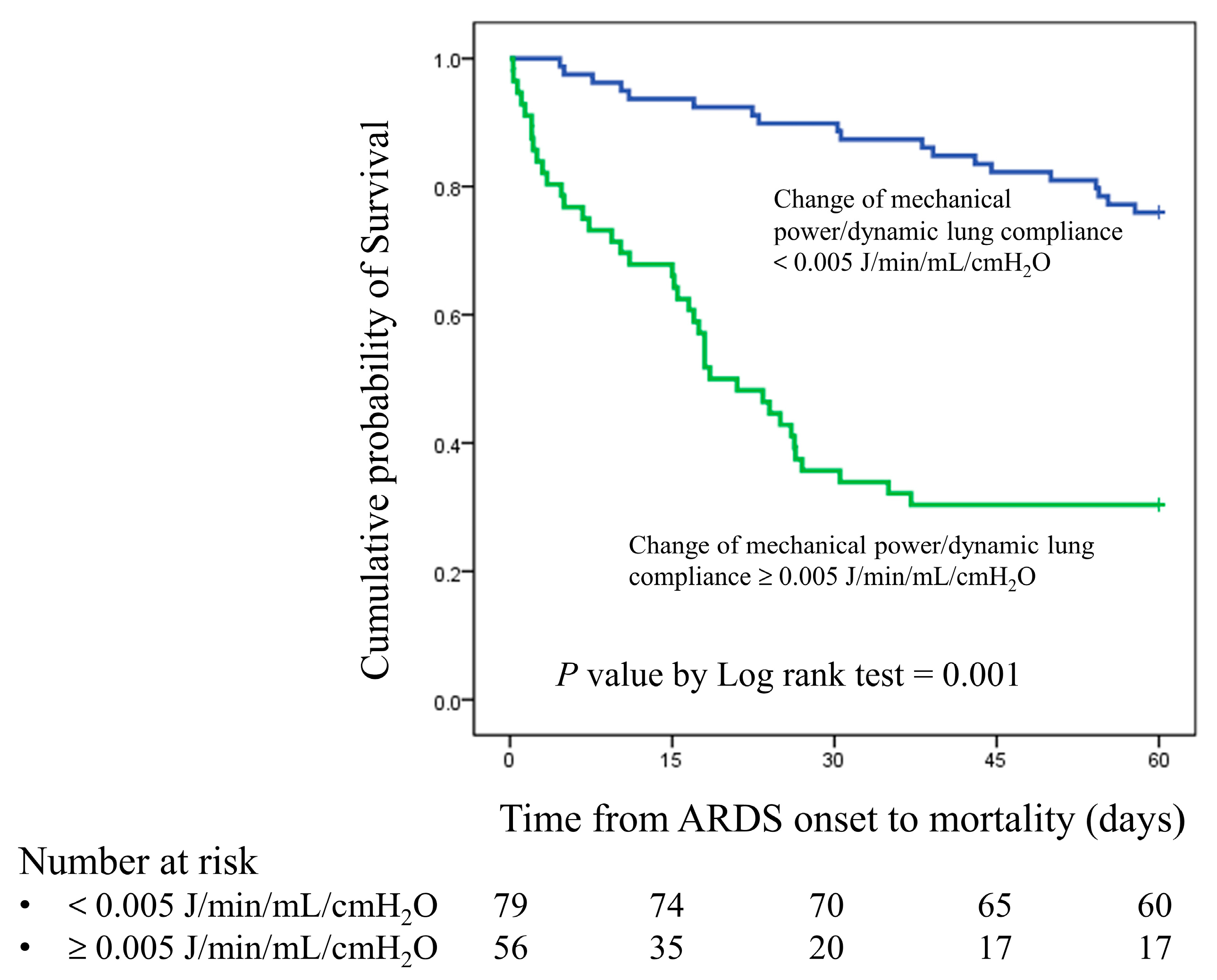
3.4. Univariate and Multivariate Cox Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-related causes of lung injury: The mechanical power. Intensive Care Med. 2016, 42, 1567–1575. [Google Scholar] [CrossRef]
- Guerin, C.; Papazian, L.; Reignier, J.; Ayzac, L.; Loundou, A.; Forel, J.M.; Investigators of the Acurasys and Proseva Trials. Effect of driving pressure on mortality in ARDS patients during lung protective mechanical ventilation in two randomized controlled trials. Crit. Care 2016, 20, 384. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zheng, B.; Liu, N.; Ge, H.; Hong, Y. Mechanical power normalized to predicted body weight as a predictor of mortality in patients with acute respiratory distress syndrome. Intensive Care Med. 2019, 45, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Serpa Neto, A.; Deliberato, R.O.; Johnson, A.E.W.; Bos, L.D.; Amorim, P.; Pereira, S.M.; Cazati, D.C.; Cordioli, R.L.; Correa, T.D.; Pollard, T.J.; et al. Mechanical power of ventilation is associated with mortality in critically ill patients: An analysis of patients in two observational cohorts. Intensive Care Med. 2018, 44, 1914–1922. [Google Scholar] [CrossRef]
- Chiu, L.C.; Lin, S.W.; Chuang, L.P.; Li, H.H.; Liu, P.H.; Tsai, F.C.; Chang, C.H.; Hung, C.Y.; Lee, C.S.; Leu, S.W.; et al. Mechanical power during extracorporeal membrane oxygenation and hospital mortality in patients with acute respiratory distress syndrome. Crit. Care 2021, 25, 13. [Google Scholar] [CrossRef] [PubMed]
- Coppola, S.; Caccioppola, A.; Froio, S.; Formenti, P.; De Giorgis, V.; Galanti, V.; Consonni, D.; Chiumello, D. Effect of mechanical power on intensive care mortality in ARDS patients. Crit. Care 2020, 24, 246. [Google Scholar] [CrossRef]
- The Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]
- Guerin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Bryan, A.C. Conference on the scientific basis of respiratory therapy. Pulmonary physiotherapy in the pediatric age group. Comments of a devil’s advocate. Am. Rev. Respir. Dis. 1974, 110, 143–144. [Google Scholar] [PubMed]
- Boesing, C.; Krebs, J.; Conrad, A.M.; Otto, M.; Beck, G.; Thiel, M.; Rocco, P.R.M.; Luecke, T.; Schaefer, L. Effects of prone positioning on lung mechanical power components in patients with acute respiratory distress syndrome: A physiologic study. Crit. Care 2024, 28, 82. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T.; National Heart, L.; Blood Institute, A.C.T.N. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar] [CrossRef]
- Schmidt, M.; Pham, T.; Arcadipane, A.; Agerstrand, C.; Ohshimo, S.; Pellegrino, V.; Vuylsteke, A.; Guervilly, C.; McGuinness, S.; Pierard, S.; et al. Mechanical Ventilation Management during Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. An International Multicenter Prospective Cohort. Am. J. Respir. Crit. Care Med. 2019, 200, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Urner, M.; Juni, P.; Hansen, B.; Wettstein, M.S.; Ferguson, N.D.; Fan, E. Time-varying intensity of mechanical ventilation and mortality in patients with acute respiratory failure: A registry-based, prospective cohort study. Lancet Respir. Med. 2020, 8, 905–913. [Google Scholar] [CrossRef]
- Richter, T.; Bellani, G.; Scott Harris, R.; Vidal Melo, M.F.; Winkler, T.; Venegas, J.G.; Musch, G. Effect of prone position on regional shunt, aeration, and perfusion in experimental acute lung injury. Am. J. Respir. Crit. Care Med. 2005, 172, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Cornejo, R.A.; Diaz, J.C.; Tobar, E.A.; Bruhn, A.R.; Ramos, C.A.; Gonzalez, R.A.; Repetto, C.A.; Romero, C.M.; Galvez, L.R.; Llanos, O.; et al. Effects of prone positioning on lung protection in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2013, 188, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Prisk, G.K.; Yamada, K.; Henderson, A.C.; Arai, T.J.; Levin, D.L.; Buxton, R.B.; Hopkins, S.R. Pulmonary perfusion in the prone and supine postures in the normal human lung. J. Appl. Physiol. 2007, 103, 883–894. [Google Scholar] [CrossRef]
- Galiatsou, E.; Kostanti, E.; Svarna, E.; Kitsakos, A.; Koulouras, V.; Efremidis, S.C.; Nakos, G. Prone position augments recruitment and prevents alveolar overinflation in acute lung injury. Am. J. Respir. Crit. Care Med. 2006, 174, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Gainnier, M.; Marin, V.; Donati, S.; Arnal, J.M.; Demory, D.; Roch, A.; Forel, J.M.; Bongrand, P.; Bregeon, F.; et al. Comparison of prone positioning and high-frequency oscillatory ventilation in patients with acute respiratory distress syndrome. Crit. Care Med. 2005, 33, 2162–2171. [Google Scholar] [CrossRef]
- Albert, R.K.; Hubmayr, R.D. The prone position eliminates compression of the lungs by the heart. Am. J. Respir. Crit. Care Med. 2000, 161, 1660–1665. [Google Scholar] [CrossRef] [PubMed]
- Mure, M.; Glenny, R.W.; Domino, K.B.; Hlastala, M.P. Pulmonary gas exchange improves in the prone position with abdominal distension. Am. J. Respir. Crit. Care Med. 1998, 157, 1785–1790. [Google Scholar] [CrossRef]
- Li Bassi, G.; Zanella, A.; Cressoni, M.; Stylianou, M.; Kolobow, T. Following tracheal intubation, mucus flow is reversed in the semirecumbent position: Possible role in the pathogenesis of ventilator-associated pneumonia. Crit. Care Med. 2008, 36, 518–525. [Google Scholar] [CrossRef]
- Cressoni, M.; Gotti, M.; Chiurazzi, C.; Massari, D.; Algieri, I.; Amini, M.; Cammaroto, A.; Brioni, M.; Montaruli, C.; Nikolla, K.; et al. Mechanical Power and Development of Ventilator-induced Lung Injury. Anesthesiology 2016, 124, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.L.V.; Slutsky, A.; Brochard, L.J.; Brower, R.; Serpa-Neto, A.; Cavalcanti, A.B.; Mercat, A.; Meade, M.; Morais, C.C.A.; Goligher, E.; et al. Ventilatory Variables and Mechanical Power in Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2021, 204, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Beitler, J.R.; Walkey, A.J. The Staying Power of Pressure- and Volume-limited Ventilation in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2021, 204, 247–249. [Google Scholar] [CrossRef]
- Kao, K.C.; Chang, K.W.; Chan, M.C.; Liang, S.J.; Chien, Y.C.; Hu, H.C.; Chiu, L.C.; Chen, W.C.; Fang, W.F.; Chen, Y.M.; et al. Predictors of survival in patients with influenza pneumonia-related severe acute respiratory distress syndrome treated with prone positioning. Ann. Intensive Care 2018, 8, 94. [Google Scholar] [CrossRef]
- Chiumello, D.; Carlesso, E.; Brioni, M.; Cressoni, M. Airway driving pressure and lung stress in ARDS patients. Crit. Care 2016, 20, 276. [Google Scholar] [CrossRef]
- Gattinoni, L.; Marini, J.J.; Pesenti, A.; Quintel, M.; Mancebo, J.; Brochard, L. The “baby lung” became an adult. Intensive Care Med. 2016, 42, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Tojo, K.; Yoshida, T.; Yazawa, T.; Goto, T. Driving-pressure-independent protective effects of open lung approach against experimental acute respiratory distress syndrome. Crit. Care 2018, 22, 228. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Patients | Survival in 28 Days | Nonsurvival in 28 Days | p Value |
|---|---|---|---|---|
| (n = 135) | (n = 91) | (n = 44) | ||
| Age (years) | 58.2 ± 13.0 | 57.2 ± 14.2 | 60.1 ± 9.9 | 0.166 |
| Sex (male/female) | 86/49 | 59/32 | 27/17 | 0.694 |
| BMI (kg/m2) | 25.6 ± 5.4 | 26.7 ± 5.8 | 23.4 ± 3.6 | <0.001 * |
| Comorbidity | ||||
| Malignancy | 21 (15.6%) | 8 (8.8%) | 13 (29.5%) | 0.002 * |
| Chronic liver disease | 12 (8.9%) | 8 (8.8%) | 4 (9.1%) | >0.999 |
| Heart failure | 3 (2.2%) | 1 (1.1%) | 2 (4.5%) | 0.248 |
| End-stage renal disease | 10 (7.4%) | 6 (6.6%) | 4 (9.1%) | 0.728 |
| Diabetes Mellitus | 48 (35.6%) | 31 (34.1%) | 17 (38.6%) | 0.603 |
| Chronic lung disease | 4 (3.0%) | 4 (4.4%) | 0 (0.0%) | 0.303 |
| Chronic steroid usage | 8 (5.9%) | 4 (4.4%) | 4 (9.1%) | 0.437 |
| Etiology of ARDS | 0.012 * | |||
| Viral pneumonia | 86 (63.7%) | 63 (69.2%) | 23 (52.3%) | |
| Bacterial pneumonia | 43 (31.9%) | 27 (29.7%) | 16 (36.4%) | |
| Sepsis | 6 (4.4%) | 1 (1.1%) | 5 (11.4%) | |
| Severity index | ||||
| APACHE II score | 26.4 ± 7.2 | 24.9 ± 7.5 | 29.5 ± 5.5 | <0.001 * |
| SOFA score | 12.4 ± 3.1 | 11.9 ± 3.0 | 13.6 ± 2.8 | 0.003 * |
| Laboratory data | ||||
| White blood cell (1000/μL) | 12.0 ± 16.0 | 10.4 ± 6.9 | 15.4 ± 26.2 | 0.264 |
| C-reactive protein (mg/dL) | 17.6 ± 10.6 | 15.4 ± 9.6 | 22.0 ± 11.3 | 0.001 * |
| Lactate (mg/dL) | 24.2 ± 24.3 | 20.6 ± 18.7 | 31.0 ± 31.5 | 0.046 * |
| Albumin (mg/dL) | 2.7 ± 0.6 | 2.8 ± 0.5 | 2.6 ± 0.7 | 0.216 |
| Creatinine (mg/dL) | 2.0 ± 2.5 | 1.6 ± 2.1 | 2.8 ± 3.1 | 0.004 * |
| Total bilirubin (mg/dL) | 0.9 ± 1.2 | 0.9 ± 1.3 | 0.8 ± 0.8 | 0.303 |
| Arterial blood gas | ||||
| pH | 7.3 ± 0.1 | 7.3 ± 0.1 | 7.3 ± 0.1 | 0.701 |
| PaO2/FiO2 ratio (mmHg) | 87.5 ± 42.1 | 93.3 ± 46.4 | 75.4 ± 28.3 | 0.020 * |
| PaCO2 (mmHg) | 51.5 ± 15.8 | 51.7 ± 16.7 | 51.1 ± 13.8 | 0.830 |
| HCO3 (mmol/L) | 25.5 ± 5.3 | 25.8 ± 5.5 | 25.1 ± 4.9 | 0.489 |
| Interventions | ||||
| Period from ARDS onset to prone positioning (days) | 1.7 ± 2.6 | 1.6 ± 2.8 | 2.1 ± 2.3 | 0.070 |
| Duration of prone positioning (days) | 3.5 ± 3.6 | 3.5 ± 3.8 | 3.5 ± 3.0 | 0.751 |
| Fresh hemodialysis | 37 (27.4%) | 18 (19.8%) | 19 (43.2%) | 0.004 * |
| Muscle relaxant usage | 134 (99.3%) | 90 (98.9%) | 44 (100.0%) | 0.485 |
| Vasopressor usage | 91 (67.4%) | 57 (62.6%) | 34 (77.3%) | 0.089 |
| ECMO after prone positioning | 18 (13.3%) | 11 (12.1%) | 7 (15.9%) | 0.540 |
| Characteristics | Survival | Nonsurvival | p Value |
|---|---|---|---|
| (n = 91) | (n = 44) | ||
| Before prone positioning | |||
| PaO2/FiO2 ratio (mmHg) | 93.3 ± 46.4 | 75.4 ± 28.3 | 0.020 * |
| pH | 7.3 ± 0.1 | 7.3 ± 0.1 | 0.793 |
| PaCO2 (mmHg) | 51.7 ± 16.7 | 51.1 ± 13.8 | 0.830 |
| Peak airway pressure (cmH2O) | 31.9 ± 4.4 | 33.5 ± 5.4 | 0.730 |
| Positive end expiratory pressure (cmH2O) | 13.6 ± 3.2 | 13.3 ± 2.5 | 0.590 |
| Tidal volume/predicted body weight (mL/Kg) | 7.4 ± 1.7 | 7.4 ± 1.8 | 0.998 |
| Respiratory rate (/min) | 24.8 ± 4.5 | 24.5 ± 5.1 | 0.710 |
| Dynamic driving pressure (cmH2O) | 18.3 ± 3.9 | 20.2 ± 5.3 | 0.035 * |
| Dynamic compliance (mL/cmH2O) | 24.0 ± 7.5 | 22.6 ± 9.6 | 0.251 |
| Mechanical power (J/min) | 23.3 ± 6.5 | 22.8 ± 5.7 | 0.688 |
| Mechanical power/predicted body weight (10−3 J/min/kg) | 407.0 ± 115.6 | 407.2 ± 121.7 | 0.992 |
| Mechanical power/compliance (J/min/mL/cmH2O) | 1.1 ± 0.4 | 1.2 ± 0.6 | 0.274 |
| After prone positioning | |||
| PaO2/FiO2 ratio (mmHg) | 137.5 ± 64.0 | 108.9 ± 51.9 | 0.013 * |
| pH | 7.4 ± 0.1 | 7.3 ± 0.1 | <0.001 * |
| PaCO2 (mmHg) | 47.2 ± 13.1 | 53.9 ± 15.7 | 0.011 * |
| Peak airway pressure (cmH2O) | 31.0 ± 3.7 | 34.9 ± 5.1 | <0.001 * |
| Positive end expiratory pressure (cmH2O) | 14.2 ± 2.3 | 14.2 ± 2.4 | 0.950 |
| Tidal volume/predicted body weight (mL/Kg) | 7.2 ± 1.6 | 7.0 ± 1.4 | 0.402 |
| Respiratory rate (/min) | 24.9 ± 4.5 | 26.8 ± 4.3 | 0.017 * |
| Dynamic driving pressure (cmH2O) | 16.8 ± 3.7 | 20.7 ± 5.3 | <0.001 * |
| Dynamic compliance (mL/cmH2O) | 25.7 ± 8.1 | 21.0 ± 8.5 | 0.002 * |
| Mechanical power (J/min) | 22.6 ± 6.5 | 25.3 ± 6.2 | 0.024 * |
| Mechanical power/predicted body weight (10−3 J/min/kg) | 396.9 ± 118.9 | 449.3 ± 118.8 | 0.018 * |
| Mechanical power/compliance (J/min/mL/cmH2O) | 0.9 ± 0.3 | 1.4 ± 0.6 | <0.001 * |
| Changes before and after prone positioning | |||
| Change in mechanical power (J/min) | −0.6 ± 5.7 | 2.5 ± 7.4 | 0.007 * |
| Change in mechanical power/predicted body weight (10−3 J/min/kg) | −9.2 ± 97.5 | 42.1 ± 127.9 | 0.010 * |
| Change in mechanical power/compliance (J/min/mL/cmH2O) | −0.1 ± 0.3 | 0.2 ± 0.3 | <0.001 * |
| Univariate Analysis | Multivariate Analysis Model 1 | Multivariate Analysis Model 2 | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| Sex | ||||||
| Female | 1 (reference) | |||||
| Male | 0.875 (0.477–1.606) | 0.667 | ||||
| Age, per 1 year increment | 1.013 (0.991–1.035) | 0.263 | ||||
| Body mass index, per 1 kg/m2 increament | 0.894 (0.837–0.955) | 0.001 * | 0.926 (0.859–0.999) | 0.046 * | 0.928 (0.853–1.009) | 0.081 |
| Cormobidity: malignancy | ||||||
| No | 1 (reference) | |||||
| Yes | 2.758 (1.440–5.281) | 0.002 * | 1.150 (0.472–2.803) | 0.759 | 1.640 (0.786–3.422) | 0.187 |
| APACHE II score, per 1 increment | 1.076 (1.030–1.123) | 0.001 * | 1.025 (0.964–1.089) | 0.428 | 1.033 (0.971–1.099) | 0.301 |
| SOFA score, per 1 increment | 1.171 (1.065–1.287) | 0.001 * | 1.086 (0.955–1.235) | 0.206 | 1.172 (1.012–1.356) | 0.034 * |
| Laboratory data | ||||||
| C-reactive protein, per 1 mg/dL increment | 1.047 (1.021–1.075) | <0.001 * | 1.017 (0.986–1.048) | 0.290 | 1.020 (0.989–1.052) | 0.213 |
| Lactate, per 1 mg/dL increment | 1.010 (1.002–1.018) | 0.020 * | ||||
| Creatinine, per 1 mg/dL increment | 1.125 (1.034–1.225) | 0.006 * | 1.116 (0.983–1.267) | 0.090 | 1.065 (0.939–1.209) | 0.327 |
| Blood gas analysis and respiratory mechanism before prone positioning | ||||||
| PaO2/FiO2 ratio, per 1 mm Hg increment | 0.987 (0.977–0.998) | 0.017 * | ||||
| PaCO2, per 1 mm Hg increment | 0.998 (0.980–1.017) | 0.844 | ||||
| Mechanical power, per 1 J/min increment | 0.994 (0.948–1.042) | 0.804 | ||||
| Mechanical power/predicted body weight, per 1 10−3 J/min/kg increment | 1.000 (0.998–1.003) | 0.835 | ||||
| Mechanical power/compliance, per 1 J/min/mL/cmH2O increment | 1.645 (0.866–3.126) | 0.129 | ||||
| Blood gas analysis and respiratory mechanism after prone positioning for 1 day | ||||||
| PaO2/FiO2 ratio, per 1 mm Hg increment | 0.992 (0.985–0.998) | 0.010 * | 0.991 (0.985–0.998) | 0.015 * | 0.994 (0.987–1.001) | 0.103 |
| PaCO2, per 1 mm Hg increment | 1.027 (1.008–1.047) | 0.004 * | 0.998 (0.972–1.025) | 0.891 | 1.021 (0.998–1.043) | 0.074 |
| Mechanical power, per 1 J/min increment | 1.049 (1.006–1.094) | 0.027 * | ||||
| Mechanical power/predicted body weight, per 1 10−3 J/min/kg increment | 1.003 (1.001–1.005) | 0.017 * | ||||
| Mechanical power/compliance, per 1 J/min/mL/cmH2O increment | 5.209 (2.972–9.129) | <0.001 * | 3.486 (1.422–8.546) | 0.006 * | ||
| Change in mechanical power, per 1 J/min increment | 1.050 (1.010–1.091) | 0.013 * | ||||
| Change in mechanical power/predicted body weight, per 1 10−3 J/min/kg increment | 1.003 (1.000–1.005) | 0.017 * | ||||
| Change in mechanical power/compliance, per 1 J/min/mL/cmH2O increment | 8.231 (3.895–17.395) | <0.001 * | 7.972 (3.071–20.697) | <0.001 * | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, K.-W.; Leu, S.-W.; Hu, H.-C.; Chan, M.-C.; Liang, S.-J.; Yang, K.-Y.; Chiu, L.-C.; Fang, W.-F.; Sheu, C.-C.; Chien, Y.-C.; et al. The Mechanical Power in Patients with Acute Respiratory Distress Syndrome Undergoing Prone Positioning Can Predict Mortality. Diagnostics 2025, 15, 158. https://doi.org/10.3390/diagnostics15020158
Chang K-W, Leu S-W, Hu H-C, Chan M-C, Liang S-J, Yang K-Y, Chiu L-C, Fang W-F, Sheu C-C, Chien Y-C, et al. The Mechanical Power in Patients with Acute Respiratory Distress Syndrome Undergoing Prone Positioning Can Predict Mortality. Diagnostics. 2025; 15(2):158. https://doi.org/10.3390/diagnostics15020158
Chicago/Turabian StyleChang, Ko-Wei, Shaw-Woei Leu, Han-Chung Hu, Ming-Cheng Chan, Shinn-Jye Liang, Kuang-Yao Yang, Li-Chung Chiu, Wen-Feng Fang, Chau-Chyun Sheu, Ying-Chun Chien, and et al. 2025. "The Mechanical Power in Patients with Acute Respiratory Distress Syndrome Undergoing Prone Positioning Can Predict Mortality" Diagnostics 15, no. 2: 158. https://doi.org/10.3390/diagnostics15020158
APA StyleChang, K.-W., Leu, S.-W., Hu, H.-C., Chan, M.-C., Liang, S.-J., Yang, K.-Y., Chiu, L.-C., Fang, W.-F., Sheu, C.-C., Chien, Y.-C., Peng, C.-K., Huang, C.-T., & Kao, K.-C. (2025). The Mechanical Power in Patients with Acute Respiratory Distress Syndrome Undergoing Prone Positioning Can Predict Mortality. Diagnostics, 15(2), 158. https://doi.org/10.3390/diagnostics15020158