
Impact of Point-of-Care Testing on Diagnosis, Treatment, and Surveillance of Vaccine-Preventable Viral Infections



Abstract
1. Introduction
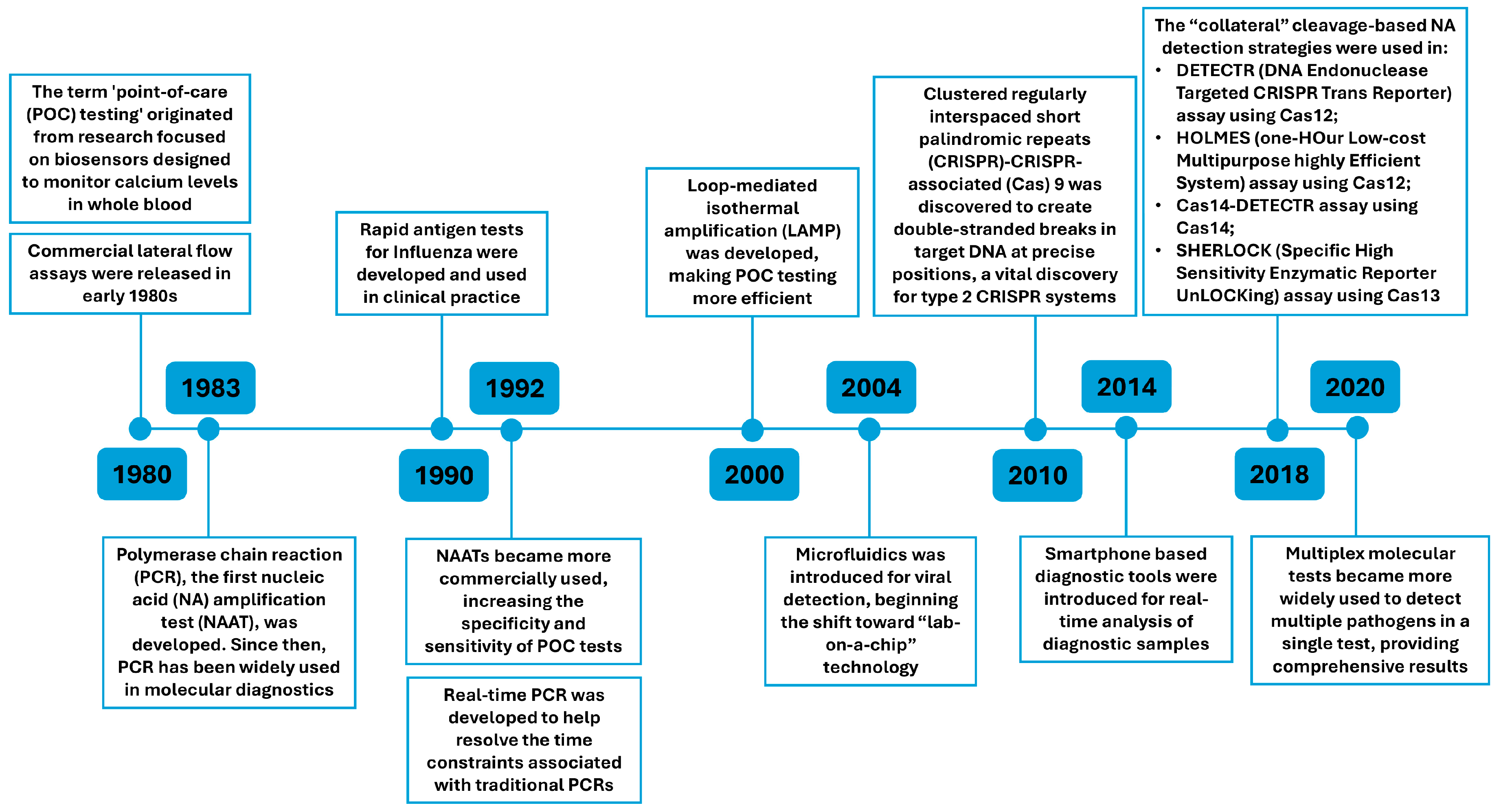
2. Progress in POC Technologies
2.1. Advancements in Nucleic Acid Amplification Tests (NAATs)
2.2. Biosensors
2.3. CRISPR-Cas
3. Impact of Viral POC Testing on Diagnosis and Treatment of VPVIs
3.1. Mpox
3.2. HBV
3.3. Respiratory Viruses
3.4. Flaviviruses: Dengue, Zika and Yellow Fever Virus
4. Impact of Viral POC Testing on Surveillance
4.1. Mpox
4.2. HBV
4.3. Respiratory Viruses
4.4. Flaviviruses: Dengue, Zika and Yellow Fever Virus
5. Conclusions
6. Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brenzel, L.; Wolfson, L.J.; Fox-Rushby, J.; Miller, M.; Halsey, N.A. Vaccine-preventable Diseases. In Disease Control Priorities in Developing Countries, 2nd ed.; Jamison, D.T., Breman, J.G., Measham, A.R., Alleyne, G., Claeson, M., Evans, D.B., Jha, P., Mills, A., Musgrove, P., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA; Oxford University Press: New York, NY, USA, 2006; Chapter 20. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11768/ (accessed on 31 December 2024).
- Hotez, P.J. Vaccine Preventable Disease and Vaccine Hesitancy. Med. Clin. N. Am. 2023, 107, 979–987. [Google Scholar] [CrossRef]
- Liu, B.M.; Li, T.; Xu, J.; Li, X.G.; Dong, J.P.; Yan, P.; Yang, J.X.; Yan, L.; Gao, Z.Y.; Li, W.P.; et al. Characterization of potential antiviral resistance mutations in hepatitis B virus reverse transcriptase sequences in treatment-naïve Chinese patients. Antivir. Res. 2010, 85, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.X.; Liu, B.M.; Li, X.G.; Yan, C.H.; Xu, J.; Sun, X.W.; Wang, Y.H.; Jiao, X.J.; Yan, L.; Dong, J.P.; et al. Profile of HBV antiviral resistance mutations with distinct evolutionary pathways against nucleoside/nucleotide analogue treatment among Chinese chronic hepatitis B patients. Antivir. Ther. 2010, 15, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Li, X.G.; Liu, B.M.; Xu, J.; Liu, X.E.; Ding, H.; Li, T. Discrepancy of potential antiviral resistance mutation profiles within the HBV reverse transcriptase between nucleos(t)ide analogue-untreated and -treated patients with chronic hepatitis B in a hospital in China. J. Med. Virol. 2012, 84, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Yang, J.X.; Yan, L.; Zhuang, H.; Li, T. Novel HBV recombinants between genotypes B and C in 3′-terminal reverse transcriptase (RT) sequences are associated with enhanced viral DNA load, higher RT point mutation rates and place of birth among Chinese patients. Infect. Genet. Evol. 2018, 57, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Liu, B.; Zhao, C.; Yang, J.; Yan, C.; Yan, L.; Zhuang, H.; Li, T. Amino acid similarities and divergences in the small surface proteins of genotype C hepatitis B viruses between nucleos(t)ide analogue-naïve and lamivudine-treated patients with chronic hepatitis B. Antivir. Res. 2014, 102, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Liu, B.; Hou, J.; Sun, J.; Hao, R.; Xiang, K.; Yan, L.; Zhang, J.; Zhuang, H.; Li, T. Naturally occurring deletions/insertions in HBV core promoter tend to decrease in hepatitis B e antigen-positive chronic hepatitis B patients during antiviral therapy. Antivir. Ther. 2015, 20, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Kayser, V.; Ramzan, I. Vaccines and vaccination: History and emerging issues. Hum. Vaccines Immunother. 2021, 17, 5255–5268. [Google Scholar] [CrossRef]
- Pollard, A.J.; Bijker, E.M. A guide to vaccinology: From basic principles to new developments. Nat. Rev. Immunol. 2021, 21, 83–100. [Google Scholar] [CrossRef] [PubMed]
- Laboratory Diagnosis of Viral Infections. In Fenner’s Veterinary Virology; Academic Press: Cambridge, MA, USA, 2017; pp. 105–129. [CrossRef]
- Larkins, M.C.; Thombare, A. Point-of-Care Testing. [Updated 2023 May 29]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, January 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK592387/ (accessed on 31 December 2024).
- Basharat, S.; Horton, J. An Overview of Emerging Point-of-Care Tests for Differentiating Bacterial and Viral Infections: CADTH Horizon Scan [Internet]; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, USA, December 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK594330/ (accessed on 31 December 2024).
- Xiao, Y.; Thompson, A.J.; Howell, J. Point-of-Care Tests for Hepatitis B: An Overview. Cells 2020, 9, 2233. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.L. Quality control issues in point of care testing. Clin. Biochem. Rev. 2008, 29 (Suppl. S1), S79–S82. [Google Scholar] [PubMed]
- Zhang, Z.; Ma, P.; Ahmed, R.; Wang, J.; Akin, D.; Soto, F.; Liu, B.; Li, P.; Demirci, U. Advanced Point-of-Care Testing Technologies for Human Acute Respiratory Virus Detection. Adv. Mater. 2022, 34, e2103646. [Google Scholar] [CrossRef] [PubMed]
- Xiao, M.; Tian, F.; Liu, X.; Zhou, Q.; Pan, J.; Luo, Z.; Yang, M.; Yi, C. Virus Detection: From State-of-the-Art Laboratories to Smartphone-Based Point-of-Care Testing. Adv. Sci. 2022, 9, e2105904. [Google Scholar] [CrossRef]
- Gronowski, A.M. Who or What is SHERLOCK? eJIFCC 2018, 29, 201–204. [Google Scholar]
- Kaunitz, J.D. The Discovery of PCR: ProCuRement of Divine Power. Dig. Dis. Sci. 2015, 60, 2230–2231. [Google Scholar] [CrossRef] [PubMed]
- Ongaro, A.E.; Ndlovu, Z.; Sollier, E.; Otieno, C.; Ondoa, P.; Street, A.; Kersaudy-Kerhoas, M. Engineering a sustainable future for point-of-care diagnostics and single-use microfluidic devices. Lab Chip 2022, 22, 3122–3137. [Google Scholar] [CrossRef]
- Banik, S.; Melanthota, S.K.; Arbaaz; Vaz, J.M.; Kadambalithaya, V.M.; Hussain, I.; Dutta, S.; Mazumder, N. Recent trends in smartphone-based detection for biomedical applications: A review. Anal. Bioanal. Chem. 2021, 413, 2389–2406. [Google Scholar] [CrossRef]
- Shinoda, H.; Taguchi, Y.; Nakagawa, R.; Makino, A.; Okazaki, S.; Nakano, M.; Muramoto, Y.; Takahashi, C.; Takahashi, I.; Ando, J.; et al. Amplification-free RNA detection with CRISPR–Cas13. Commun. Biol. 2021, 4, 476. [Google Scholar] [CrossRef]
- Liu, B.M. Isothermal nucleic acid amplification technologies and CRISPR-Cas based nucleic acid detection strategies for infectious disease diagnostics. In Manual of Molecular Microbiology; ASM Press: Washington, DC, USA, 2026. [Google Scholar]
- Liu, B.M.; Beck, E.M.; Fisher, M.A. The Brief Case: Ventilator-Associated Corynebacterium accolens Pneumonia in a Patient with Respiratory Failure Due to COVID-19. J. Clin. Microbiol. 2021, 59, e0013721. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kang, T.; Lu, J.; Yu, T.; Long, Y.; Liu, G. Advances in nucleic acid amplification techniques (NAATs): COVID-19 point-of-care diagnostics as an example. Biosens. Bioelectron. 2022, 206, 114109. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.M.; Carlisle, C.P.; Fisher, M.A.; Shakir, S.M. The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Bronchopneumonia. J. Clin. Microbiol. 2021, 59, e0247220. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xiao, Z.; Liu, X.; Kang, X.; Feng, Y.; Zheng, L.; Chen, C. Rapid and accurate detection of SARS-CoV-2 using the RHAM technology. Sci. Rep. 2023, 13, 22798. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, B.M. History of global food safety, foodborne illness, and risk assessment. In History of Food and Nutrition Toxicology; Academic Press: Washington, DC, USA, 2023; pp. 301–316. [Google Scholar]
- Lewinski, M.A.; Alby, K.; Babady, N.E.; Butler-Wu, S.M.; Bard, J.D.; Greninger, A.L.; Hanson, K.; Naccache, S.N.; Newton, D.; Temple-Smolkin, R.L.; et al. Exploring the Utility of Multiplex Infectious Disease Panel Testing for Diagnosis of Infection in Different Body Sites: A Joint Report of the Association for Molecular Pathology, American Society for Microbiology, Infectious Diseases Society of America, and Pan American Society for Clinical Virology. J. Mol. Diagn. 2023, 25, 857–875. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Forman, M.; Valsamakis, A. Optimization and evaluation of a novel real-time RT-PCR test for detection of parechovirus in cerebrospinal fluid. J. Virol. Methods 2019, 272, 113690. [Google Scholar] [CrossRef] [PubMed]
- Nelson, P.P.; Rath, B.A.; Fragkou, P.C.; Antalis, E.; Tsiodras, S.; Skevaki, C. Current and Future Point-of-Care Tests for Emerging and New Respiratory Viruses and Future Perspectives. Front. Cell. Infect. Microbiol. 2020, 10, 181. [Google Scholar] [CrossRef]
- Naresh, V.; Lee, N. A Review on Biosensors and Recent Development of Nanostructured Materials-Enabled Biosensors. Sensors 2021, 21, 1109. [Google Scholar] [CrossRef] [PubMed]
- Manring, N.; Ahmed, M.M.N.; Tenhoff, N.; Smeltz, J.L.; Pathirathna, P. Recent Advances in Electrochemical Tools for Virus Detection. Anal. Chem. 2022, 94, 7149–7157. [Google Scholar] [CrossRef] [PubMed]
- John, P.; Vasa, N.J.; Zam, A. Optical Biosensors for the Diagnosis of COVID-19 and Other Viruses—A Review. Diagnostics 2023, 13, 2418. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Devarakonda, S.; Singh, R.; Bhardwaj, J.; Jang, J. Cost-Effective and Handmade Paper-Based Immunosensing Device for Electrochemical Detection of Influenza Virus. Sensors 2017, 17, 2597. [Google Scholar] [CrossRef]
- Guliy, O.I.; Zaitsev, B.D.; Semyonov, A.P.; Karavaeva, O.A.; Fomin, A.S.; Staroverov, S.A.; Burov, A.M.; Borodina, I.A. Sensor System Based on a Piezoelectric Resonator with a Lateral Electric Field for Virus Diagnostics. Ultrasound Med. Biol. 2022, 48, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, M.; Janani, R.; Deepa, C.; Rajeshkumar, L. Nanotechnology-Enabled Biosensors: A Review of Fundamentals, Design Principles, Materials, and Applications. Biosensors 2022, 13, 40. [Google Scholar] [CrossRef]
- Kobra Salimiyan rizi, The smartphone biosensors for point-of-care detection of human infectious diseases: Overview and perspectives—A systematic review. Curr. Opin. Electrochem. 2022, 32, 100925. [CrossRef]
- Hasan, M.R.; Sharma, P.; Singh, S.; Narang, J. Smartphone-Integrated Wireless Portable Potentiostat to Develop 5th-Generation Dengue Pocket Aptasensor toward Portronicx-Approach. ACS Appl. Bio Mater. 2024, 7, 2299–2308. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhou, X.; Wang, M.; Ren, L. Towards Point of Care CRISPR-Based Diagnostics: From Method to Device. J. Funct. Biomater. 2023, 14, 97. [Google Scholar] [CrossRef]
- van Dongen, J.E.; Berendsen, J.T.W.; Steenbergen, R.D.M.; Wolthuis, R.M.F.; Eijkel, J.C.T.; Segerink, L.I. Point-of-care CRISPR/Cas nucleic acid detection: Recent advances, challenges and opportunities. Biosens. Bioelectron. 2020, 166, 112445. [Google Scholar] [CrossRef]
- Ravichandran, M.; Maddalo, D. Applications of CRISPR-Cas9 for advancing precision medicine in oncology: From target discovery to disease modeling. Front. Genet. 2023, 14, 1273994. [Google Scholar] [CrossRef] [PubMed]
- Luppa, P.B.; Müller, C.; Schlichtiger, A.; Schlebusch, H. Point-of-care testing (POCT): Current techniques and future perspectives. TrAC Trends Anal. Chem. 2011, 30, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.N.A.; Arrowsmith, J.E. Point-of-care testing. Surg.-Oxf. Int. Ed. Vol. 2006, 24, 341. [Google Scholar] [CrossRef]
- Mattila, S.; Paalanne, N.; Honkila, M.; Pokka, T.; Tapiainen, T. Effect of Point-of-Care Testing for Respiratory Pathogens on Antibiotic Use in Children: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2216162. [Google Scholar] [CrossRef]
- Brendish, N.J.; Mills, S.; Ewings, S.; Clark, T.W. Impact of point-of-care testing for respiratory viruses on antibiotic use in adults with exacerbation of airways disease. J. Infect. 2019, 79, 357–362. [Google Scholar] [CrossRef]
- Liu, B.M.; Rakhmanina, N.Y.; Yang, Z.; Bukrinsky, M.I. Mpox (Monkeypox) Virus and Its Co-Infection with HIV, Sexually Transmitted Infections, or Bacterial Superinfections: Double Whammy or a New Prime Culprit? Viruses 2024, 16, 784. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, B.; Panda, D.; Mendez-Rios, J.D.; Ganesan, S.; Wyatt, L.S.; Moss, B. Identification of Poxvirus Genome Uncoating and DNA Replication Factors with Mutually Redundant Roles. J. Virol. 2018, 92, e02152-17. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rani, I.; Goyal, A.; Shamim, M.A.; Satapathy, P.; Pal, A.; Squitti, R.; Goswami, K.; Sah, R.; Barboza, J.J.; Padhi, B.K. Prevalence of mpox viral DNA in cutaneous specimens of monkeypox-infected patients: A systematic review and meta-analysis. Front. Cell. Infect. Microbiol. 2023, 13, 1179885. [Google Scholar] [CrossRef] [PubMed]
- Deputy, N.P.; Deckert, J.; Chard, A.N.; Sandberg, N.; Moulia, D.L.; Barkley, E.; Dalton, A.F.; Sweet, C.; Cohn, A.C.; Little, D.R.; et al. Vaccine Effectiveness of JYNNEOS against Mpox Disease in the United States. N. Engl. J. Med. 2023, 388, 2434–2443. [Google Scholar] [CrossRef] [PubMed]
- World Health Organzation. Surveillance, Case Investigation and Contact Tracing for Mpox (Monkeypox). 20 March 2024. Available online: https://www.who.int/publications/i/item/WHO-MPX-Surveillance-2024.1 (accessed on 31 December 2024).
- Cepheid Mpox Package Insert. Available online: https://web-support.cepheid.com/Package%20Insert%20Files/302-9630%20Rev.%20A%20Xpert%20Mpox%20IFU%20Xpress%20POC.pdf (accessed on 25 November 2024).
- Li, D.; Wilkins, K.; McCollum, A.M.; Osadebe, L.; Kabamba, J.; Nguete, B.; Likafi, T.; Balilo, M.P.; Lushima, R.S.; Malekani, J.; et al. Evaluation of the GeneXpert for Human Monkeypox Diagnosis. Am. J. Trop. Med. Hyg. 2017, 96, 405–410. [Google Scholar] [CrossRef]
- Damhorst, G.; McLendon, K.; Morales, E.; Solis, Z.; Fitts, E.; Bowers, H.; Sabino, C.; Sullivan, J.; Greenleaf, M.; Colasanti, J.; et al. 1022. Detection of Mpox virus with the Cepheid Xpert Mpox assay in oropharyngeal, anorectal and cutaneous lesion swab specimens. Open Forum Infect. Dis. 2023, 10 (Suppl. S2), ofad500-053. [Google Scholar] [CrossRef]
- Suñer, C.; Ubals, M.; Tarín-Vicente, E.J.; Mendoza, A.; Alemany, A.; Hernández-Rodríguez, Á.; Casañ, C.; Descalzo, V.; Ouchi, D.; Marc, A.; et al. Viral dynamics in patients with monkeypox infection: A prospective cohort study in Spain. Lancet Infect. Dis. 2023, 23, 445–453. [Google Scholar] [CrossRef]
- Thompson, P.; Morgan, C.E.; Ngimbi, P.; Mwandagalirwa, K.; Ravelomanana, N.L.R.; Tabala, M.; Fathy, M.; Kawende, B.; Muwonga, J.; Misingi, P.; et al. Arresting vertical transmission of hepatitis B virus (AVERT-HBV) in pregnant women and their neonates in the Democratic Republic of the Congo: A feasibility study. Lancet Glob. Health 2021, 9, e1600–e1609, Erratum in Lancet Glob. Health 2021, 9, e1507. [Google Scholar] [CrossRef]
- Ioannou, G.N. Hepatitis B virus in the United States: Infection, exposure, and immunity rates in a nationally representative survey. Ann. Intern. Med. 2011, 154, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Chahal, H.S.; Peters, M.G.; Harris, A.M.; McCabe, D.; Volberding, P.; Kahn, J.G. Cost-effectiveness of Hepatitis B Virus Infection Screening and Treatment or Vaccination in 6 High-risk Populations in the United States. Open Forum Infect. Dis. 2018, 6, ofy353. [Google Scholar] [CrossRef] [PubMed]
- Marcuccilli, F.; Chevaliez, S.; Muller, T.; Colagrossi, L.; Abbondanza, G.; Beyser, K.; Wlassow, M.; Ortonne, V.; Perno, C.F.; Ciotti, M. Multicenter Evaluation of the Cepheid Xpert® HBV Viral Load Test. Diagnostics 2021, 11, 297. [Google Scholar] [CrossRef]
- Jackson, K.; Tekoaua, R.; Li, X.; Locarnini, S. Real-world application of the Xpert® HBV viral load assay on serum and dried blood spots. J. Med. Virol. 2021, 93, 3707–3713. [Google Scholar] [CrossRef] [PubMed]
- Khounvisith, V.; Saysouligno, S.; Souvanlasy, B.; Billamay, S.; Mongkhoune, S.; Vongphachanh, B.; Snoeck, C.J.; Black, A.P.; Muller, C.P.; Hübschen, J.M. Hepatitis B virus and other transfusion-transmissible infections in child blood recipients in Lao People’s Democratic Republic: A hospital-based study. Arch. Dis. Child. 2023, 108, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States. Recommendations of the Advisory Committee on Immunization Practices (ACIP) Part 1 Immunization of Infants, Children, and Adolescents. MMWR Morb. Mortal. Wkly. Rep. 2005, 54, 1–23. [Google Scholar]
- Liu, B.M.; Martins, T.B.; Peterson, L.K.; Hill, H.R. Clinical significance of measuring serum cytokine levels as inflammatory biomarkers in adult and pediatric COVID-19 cases: A review. Cytokine 2021, 142, 155478. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- LeMessurier, K.S.; Rooney, R.; Ghoneim, H.E.; Liu, B.; Li, K.; Smallwood, H.S.; Samarasinghe, A.E. Influenza A virus directly modulates mouse eosinophil responses. J. Leucoc. Biol. 2020, 108, 151–168. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, B.M.; Hill, H.R. Role of Host Immune and Inflammatory Responses in COVID-19 Cases with Underlying Primary Immunodeficiency: A Review. J. Interferon Cytokine Res. 2020, 40, 549–554. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, B.M.; Mulkey, S.B.; Campos, J.M.; DeBiasi, R.L. Laboratory diagnosis of CNS infections in children due to emerging and re-emerging neurotropic viruses. Pediatr. Res. 2024, 95, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Liu, B. Universal PCR Primers Are Critical for Direct Sequencing-Based Enterovirus Genotyping. J. Clin. Microbiol. 2016, 55, 339–340. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, B.; Li, N.L.; Shen, Y.; Bao, X.; Fabrizio, T.; Elbahesh, H.; Webby, R.J.; Li, K. The C-Terminal Tail of TRIM56 Dictates Antiviral Restriction of Influenza A and B Viruses by Impeding Viral RNA Synthesis. J. Virol. 2016, 90, 4369–4382. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ribeiro, B.V.; Cordeiro, T.A.R.; e Freitas, G.R.O.; Ferreira, L.F.; Franco, D.L. Biosensors for the detection of respiratory viruses: A review. Talanta Open 2020, 2, 100007. [Google Scholar] [CrossRef] [PubMed]
- Stamm, B.D.; Tamerius, J.; Reddy, S.; Barlow, S.; Hamer, C.; Kempken, A.; Goss, M.; He, C.; Bell, C.; Arnold, M.; et al. The Influence of Rapid Influenza Diagnostic Testing on Clinician Decision-Making for Patients With Acute Respiratory Infection in Urgent Care. Clin. Infect. Dis. 2023, 76, 1942–1948. [Google Scholar] [CrossRef] [PubMed]
- Jian, M.J.; Chung, H.Y.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Li, S.Y.; Hsieh, S.S.; Liu, M.T.; Yang, J.R.; et al. Clinical Comparison of Three Sample-to-Answer Systems for Detecting SARS-CoV-2 in B.1.1.7 Lineage Emergence. Infect. Drug Resist. 2021, 14, 3255–3261. [Google Scholar] [CrossRef] [PubMed]
- Fjelltveit, E.B.; Cox, R.J.; Østensjø, J.; Blomberg, B.; Ebbesen, M.H.; Langeland, N.; Mohn, K.G. Point-of-Care Influenza Testing Impacts Clinical Decision, Patient Flow, and Length of Stay in Hospitalized Adults. J. Infect. Dis. 2022, 226, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, H.; van Genne, M.; Lizarazo-Forero, E.; Niesters, H.G.M.; Gard, L. Evaluation of the QIAstat-Dx RP2.0 and the BioFire FilmArray RP2.1 for the Rapid Detection of Respiratory Pathogens Including SARS-CoV-2. Front. Microbiol. 2022, 13, 854209. [Google Scholar] [CrossRef] [PubMed]
- Contes, K.; Liu, B.M. Epidemiology, clinical significance and diagnosis of respiratory viruses and their co-infections in the post-COVID era. Preprints 2024, 2024120268. [Google Scholar] [CrossRef]
- Fistera, D.; Kikull, K.; Risse, J.; Herrmann, A.; Brachmann, M.; Kill, C. Point-of-care PCR testing of SARS-CoV-2 in the emergency department: Influence on workflow and efficiency. PLoS ONE 2023, 18, e0288906. [Google Scholar] [CrossRef]
- Larkin, H.D. NIH Pilots Telehealth Program for COVID-19. JAMA 2023, 329, 363–364. [Google Scholar] [CrossRef]
- González-Parra, G.; Mahmud, M.S.; Kadelka, C. Learning from the COVID-19 pandemic: A systematic review of mathematical vaccine prioritization models. Infect. Dis. Model. 2024, 9, 1057–1080. [Google Scholar] [CrossRef]
- Loeffelholz, M.J.; Alland, D.; Butler-Wu, S.M.; Pandey, U.; Perno, C.F.; Nava, A.; Carroll, K.C.; Mostafa, H.; Davies, E.; McEwan, A.; et al. Multicenter Evaluation of the Cepheid Xpert Xpress SARS-CoV-2 Test. J. Clin. Microbiol. 2020, 58, e00926-20. [Google Scholar] [CrossRef] [PubMed]
- Barker, K.R.; Small, L.N.; Thai, D.V.; Sohn, K.Y.; Rosella, L.C. Evaluating the Ability to ID (COVID-19) NOW: A Large Real-World Prospective Evaluation of the Abbott ID NOW COVID-19 Assay. Microbiol. Spectr. 2022, 10, e0051322. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Sharma, P.; Berhane, S.; van Wyk, S.S.; Nyaaba, N.; Domen, J.; Taylor, M.; Cunningham, J.; Davenport, C.; Dittrich, S.; et al. Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2022, 7, CD013705. [Google Scholar] [CrossRef] [PubMed]
- Chong, Z.-S.; Wright, G.J.; Sharma, S. Investigating Cellular Recognition Using CRISPR/Cas9 Genetic Screening. Trends Cell Biol. 2020, 30, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, W.; Omar, M. Enterovirus. [Updated 2023 Jul 31]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK562330/ (accessed on 31 December 2024).
- Cong, L.; Ran, F.A.; Cox, D.; Lin, S.; Barretto, R.; Habib, N.; Hsu, P.D.; Wu, X.; Jiang, W.; Marraffini, L.A.; et al. Multiplex Genome Engineering Using CRISPR/Cas Systems. Science 2013, 339, 819–823. [Google Scholar] [CrossRef]
- Schechter, M. Prioritization of antiretroviral therapy in patients with high CD4 counts, and retention in care: Lessons from the START and Temprano trials. J. Int. AIDS Soc. 2018, 21, e25077. [Google Scholar] [CrossRef]
- Jallow, M.M.; Mendy, M.P.; Barry, M.A.; Diagne, M.M.; Sagne, S.N.; Tall, F.; Diouf, J.B.N.; Ndiaye, N.K.; Kiori, D.; Sy, S.; et al. Real-Time Enterovirus D68 Outbreak Detection through Hospital Surveillance of Severe Acute Respiratory Infection, Senegal, 2023. Emerg. Infect. Dis. 2024, 30, 1687–1691. [Google Scholar] [CrossRef]
- Kabir, M.A.; Zilouchian, H.; Younas, M.A.; Asghar, W. Dengue Detection: Advances in Diagnostic Tools from Conventional Technology to Point of Care. Biosensors 2021, 11, 206. [Google Scholar] [CrossRef]
- Liu, B.; Li, N.L.; Wang, J.; Shi, P.Y.; Wang, T.; Miller, M.A.; Li, K. Overlapping and distinct molecular determinants dictating the antiviral activities of TRIM56 against flaviviruses and coronavirus. J. Virol. 2014, 88, 13821–13835. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, D.; Li, N.L.; Wei, D.; Liu, B.; Guo, F.; Elbahesh, H.; Zhang, Y.; Zhou, Z.; Chen, G.Y.; Li, K. The E3 ligase TRIM56 is a host restriction factor of Zika virus and depends on its RNA-binding activity but not miRNA regulation, for antiviral function. PLoS Negl. Trop. Dis. 2019, 13, e0007537. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pang, J.; Chia, P.Y.; Lye, D.C.; Leo, Y.S. Progress and Challenges towards Point-of-Care Diagnostic Development for Dengue. J. Clin. Microbiol. 2017, 55, 3339–3349. [Google Scholar] [CrossRef] [PubMed]
- Laboratory Diagnosis and Diagnostic Tests. In Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition; World Health Organization: Geneva, Switzerland, 2009. Available online: https://www.ncbi.nlm.nih.gov/books/NBK143156/ (accessed on 1 January 2020).
- Ooi, E.E. Challenges in prevaccination screening for previous dengue infection. Lancet Glob. Health 2021, 9, e4–e5. [Google Scholar] [CrossRef]
- World Health Organization. Disease Outbreak News; Mpox in African Region. 22 August 2024. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2024-DON528 (accessed on 31 December 2024).
- Chou, R.; Dana, T.; Bougatsos, C.; Blazina, I.; Khangura, J.; Zakher, B. Screening for Hepatitis B Virus Infection in Adolescents and Adults: A Systematic Review to Update the U.S. Preventive Services Task Force Recommendation. Ann. Intern. Med. 2014, 161, 31–45. [Google Scholar] [CrossRef]
- Servant-Delmas, A.; Ly, T.D.; Hamon, C.; Houdah, A.K.; Laperche, S. Comparative Performance of Three Rapid HBsAg Assays for Detection of HBs Diagnostic Escape Mutants in Clinical Samples. J. Clin. Microbiol. 2015, 53, 3954–3955. [Google Scholar] [CrossRef]
- Liu, B.M.; Hayes, A.W. Mechanisms and Assessment of Genotoxicity of Metallic Engineered Nanomaterials in the Human Environment. Biomedicines 2024, 12, 2401. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, B.M. Epidemiological and clinical overview of the 2024 Oropouche virus disease outbreaks, an emerging/re-emerging neurotropic arboviral disease and global public health threat. J. Med. Virol. 2024, 96, e29897. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Breckenridge, A.J.; Garcia-Alcalde, F.; Wildum, S.; Smits, S.L.; de Man, R.A.; van Campenhout, M.J.H.; Brouwer, W.P.; Niu, J.; Young, J.A.T.; Najera, I.; et al. Machine-learning based patient classification using Hepatitis B virus full-length genome quasispecies from Asian and European cohorts. Sci. Rep. 2019, 9, 18892. [Google Scholar] [CrossRef] [PubMed]
- Piermatteo, L.; D’Anna, S.; Bertoli, A.; Bellocchi, M.; Carioti, L.; Fabeni, L.; Alkhatib, M.; Frazia, S.L.; Lichtner, M.; Mastroianni, C.; et al. Unexpected rise in the circulation of complex HBV variants enriched of HBsAg vaccine-escape mutations in HBV genotype-D: Potential impact on HBsAg detection/quantification and vaccination strategies. Emerg. Microbes Infect. 2023, 12, 2219347. [Google Scholar] [CrossRef]
- Tshiabuila, D.; Choga, W.; James, S.E.; Maponga, T.; Preiser, W.; van Zyl, G.; Moir, M.; van Wyk, S.; Giandhari, J.; Pillay, S.; et al. An Oxford Nanopore Technology-Based Hepatitis B Virus Sequencing Protocol Suitable For Genomic Surveillance Within Clinical Diagnostic Settings. Int. J. Mol. Sci. 2024, 25, 11702. [Google Scholar] [CrossRef]
- Geyer, R.E.; Kotnik, J.H.; Lyon, V.; Brandstetter, E.; Suchsland, M.Z.; Han, P.D.; Graham, C.; Ilcisin, M.; Kim, A.E.; Chu, H.Y.; et al. Diagnostic Accuracy of an At-Home, Rapid Self-test for Influenza: Prospective Comparative Accuracy Study. JMIR Public Health Surveill. 2022, 8, e28268. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Evaluation of rapid influenza diagnostic tests for influenza A (H3N2)v virus and updated case count—United States, 2012. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 619–621. [Google Scholar]
- Harper, S.A.; Bradley, J.S.; Englund, J.A.; File, T.M.; Gravenstein, S.; Hayden, F.G.; McGeer, A.J.; Neuzil, K.M.; Pavia, A.T.; Tapper, M.L.; et al. Seasonal Influenza in Adults and Children—Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management: Clinical Practice Guidelines of the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 48, 1003–1032. [Google Scholar] [CrossRef]
- Iliescu, F.S.; Ionescu, A.M.; Gogianu, L.; Simion, M.; Dediu, V.; Chifiriuc, M.C.; Pircalabioru, G.G.; Iliescu, C. Point-of-Care Testing-The Key in the Battle against SARS-CoV-2 Pandemic. Micromachines 2021, 12, 1464. [Google Scholar] [CrossRef] [PubMed]
- Sakthivel, D.; Delgado-Diaz, D.; McArthur, L.; Hopper, W.; Richards, J.S.; Narh, C.A. Point-of-Care Diagnostic Tools for Surveillance of SARS-CoV-2 Infections. Front. Public Health 2021, 9, 766871. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.M.; Yao, Q.; Cruz-Cosme, R.; Yarbrough, C.; Draper, K.; Suslovic, W.; Muhammad, I.; Contes, K.M.; Hillyard, D.R.; Teng, S.; et al. Genetic conservation and diversity of SARS-CoV-2 Envelope gene across variants of concern. J. Med. Virol. 2025, 97, e70136. [Google Scholar] [CrossRef] [PubMed]
- Hirano, J.; Murakami, K.; Hayashi, T. CRISPR-Cas9-Based Technology for Studying Enteric Virus Infection. Front. Genome Ed. 2022, 4, 888878. [Google Scholar] [CrossRef]
- Abedi, G.R.; Watson, J.T.; Nix, W.A.; Oberste, M.S.; Gerber, S.I. Enterovirus and Parechovirus Surveillance—United States, 2014–2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 515–518. [Google Scholar] [CrossRef]
- Wang, J.; Liu, B.; Wang, N.; Lee, Y.M.; Liu, C.; Li, K. TRIM56 is a virus- and interferon-inducible E3 ubiquitin ligase that restricts pestivirus infection. J. Virol. 2011, 85, 3733–3745. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Raafat, N.; Blacksell, S.D.; Maude, R.J. A review of dengue diagnostics and implications for surveillance and control. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 653–660. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakshmanan, K.; Liu, B.M. Impact of Point-of-Care Testing on Diagnosis, Treatment, and Surveillance of Vaccine-Preventable Viral Infections. Diagnostics 2025, 15, 123. https://doi.org/10.3390/diagnostics15020123
Lakshmanan K, Liu BM. Impact of Point-of-Care Testing on Diagnosis, Treatment, and Surveillance of Vaccine-Preventable Viral Infections. Diagnostics. 2025; 15(2):123. https://doi.org/10.3390/diagnostics15020123
Chicago/Turabian StyleLakshmanan, Kirthika, and Benjamin M. Liu. 2025. "Impact of Point-of-Care Testing on Diagnosis, Treatment, and Surveillance of Vaccine-Preventable Viral Infections" Diagnostics 15, no. 2: 123. https://doi.org/10.3390/diagnostics15020123
APA StyleLakshmanan, K., & Liu, B. M. (2025). Impact of Point-of-Care Testing on Diagnosis, Treatment, and Surveillance of Vaccine-Preventable Viral Infections. Diagnostics, 15(2), 123. https://doi.org/10.3390/diagnostics15020123