1. Introduction
Intraocular pressure (IOP) measurement remains a fundamental component in the diagnosis, monitoring, and treatment of glaucoma, a chronic and progressive optic neuropathy that represents a major global cause of irreversible blindness. The timely detection and accurate assessment of IOP are crucial, as it is the most significant modifiable risk factor for glaucomatous damage. For this reason, IOP evaluation is routinely included in comprehensive ophthalmic examinations and is critical for assessing disease progression and treatment efficacy.
Over the decades, numerous technologies and methods have been developed to measure intraocular pressure (IOP), reflecting the clinical importance of accurate and reliable tonometry. These include a wide range of contact and non-contact devices such as pneumotonometry, rebound tonometry (iCare), non-contact tonometry (NCT or “air puff”), Tono-Pen applanation tonometry, dynamic contour tonometry (Pascal), transpalpebral tonometry (e.g., Diaton), and ocular response analyzers (ORA), each with unique mechanisms, advantages, and limitations. Despite the growing diversity and sophistication of these alternatives, Goldmann applanation tonometry (GAT), originally introduced by Goldmann and Schmidt in 1957, has withstood the test of time and remains widely regarded as the clinical gold standard for IOP measurement [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21]. Its well-established reliability, reproducibility, and extensive validation in both clinical and research settings have made it the benchmark against which newer tonometry methods are compared. GAT’s consistent performance and central role in major glaucoma studies continue to support its prominence in ophthalmic practice.
In recent years, technological advances have led to the development of digital adaptations of the classic GAT, aiming to modernize IOP measurement while maintaining clinical accuracy. The first digital version of the traditional Goldmann tonometer, and to date still one of the very few, is the AT900D, introduced in the early 2010s by Haag-Streit (Köniz, Switzerland). This model features a digital backlit readout and improved visualization while preserving the mechanical design and user experience of the original device.
Several studies have evaluated the AT900D and confirmed its high level of accuracy and reproducibility. Comparative analyses between the AT900D and the classic mechanical Goldmann tonometer have consistently shown excellent agreement in IOP measurements, with strong inter-device correlation and low variability, supporting its clinical reliability and the possibility of routine use as a digital alternative [
22,
23,
24,
25].
Despite differences in display and data interface, both the AT900D and its mechanical predecessor are based on the same underlying physical principle—the Imbert–Fick law [
26]. This law, which relates the internal pressure of a sphere to the external force required to flatten its surface, remains the cornerstone of applanation tonometry and ensures methodological continuity across both device types.
Following the introduction of the AT900D, the Huvitz HT5000 (Huvitz, Dongan-gu, Anyang-si, Gyeonggi-do, Republic of Korea) emerged as an additional digital Goldmann-type applanation tonometer. Like the AT900D and the classic mechanical GAT, it is based on the Imbert–Fick principle. A key differentiator of the HT5000 is its substantially lower cost compared to the AT900D, making it a practical choice for ophthalmic clinics aiming to modernize equipment on a limited budget.
Despite being commercially available for over a decade, to the best of our knowledge, no peer-reviewed study has yet directly compared IOP measurements obtained with the Huvitz HT5000 and those of the gold-standard mechanical GAT. This notable gap in the literature raises important clinical questions about the interchangeability and reliability of the HT5000.
The aim of the present study was therefore to compare the performance of the Huvitz HT5000 digital applanation tonometer (dGAT) with that of the conventional Haag-Streit AT900 mechanical GAT (mGAT), focusing on the level of agreement, correlation, and potential differences across various IOP ranges. By analyzing the relationship between the two instruments, this study seeks to clarify whether this digital device can serve as a reliable substitute for the mechanical GAT in routine ophthalmologic settings.
2. Materials and Methods
This retrospective comparative study was conducted at a tertiary ophthalmology center and was based on a chart review of patients who underwent routine comprehensive ocular examinations. Eligible records were identified from the clinic database over a defined study period and included adult patients (aged ≥ 18 years) who had undergone IOP measurement using both mGAT and dGAT, as part of standard clinical care.
Inclusion criteria required complete and reliable IOP readings with both devices, along with a recorded measurement of central corneal thickness (CCT). Eyes with known corneal pathology (e.g., corneal scarring, dystrophies, edema, or prior refractive surgery) that could influence applanation accuracy were excluded. When both eyes met the inclusion criteria, they were included in the analysis.
Sample size estimation was based on previously published epidemiological data, which report an average IOP of approximately 15 mmHg with a standard deviation of 4 mmHg in populations similar to ours [
27]. With an alpha level (α) of 0.05, a power (1 − β) of 0.80, and an anticipated clinically relevant difference of 1.6 mmHg, the minimum required sample size was calculated to be 49 eyes. To ensure adequate statistical power and account for possible exclusions, data from 53 eyes were ultimately included.
All measurements had been previously performed by a single experienced glaucoma specialist (AK) as part of routine care. Each patient had undergone full ophthalmic examination, including best-corrected visual acuity assessment, slit-lamp biomicroscopy, gonioscopy, indirect ophthalmoscopy, and pachymetry using ultrasound for CCT determination.
Intraocular pressure was measured using both the Haag-Streit AT900 mechanical Goldmann applanation tonometer (mGAT; Haag-Streit, Bern, Switzerland) and the Huvitz HT5000 digital Goldmann tonometer (dGAT; Huvitz, Dongan-gu, Anyang-si, Gyeonggi-do, Republic of Korea). Devices were calibrated regularly in accordance with manufacturer recommendations. The order of tonometry (mGAT vs. dGAT) had been randomly assigned at the time of the clinical visit to minimize measurement order bias. IOP was measured twice with each device per eye, and the average value was used for analysis.
To minimize the influence of repeated applanation on IOP measurements, a five-minute interval was observed between the two measurements [
28]. To preserve examiner masking, the LED readout on the dGAT and the dial on the mGAT were concealed during measurement, and readings were recorded by an assistant. mGAT readings were rounded to the nearest whole mmHg in accordance with standard clinical conventions (even numbers when near a gauge mark; odd when between marks).
The reproducibility of each tonometer’s readings was assessed using the coefficient of variation (CV) from the paired measurements. Statistical analyses were performed using MedCalc version 20.110 (MedCalc Software, Mariakerke, Belgium). Paired Student’s t-tests were used to compare IOP means between devices, while Pearson’s correlation coefficient evaluated the linear relationship between paired readings. Agreement was assessed via Bland–Altman analysis. Linear regression models were employed to examine the association between inter-device IOP differences and CCT.
The study protocol was reviewed and approved by the institutional ethics committee and adhered to the principles of the Declaration of Helsinki (as revised in 2013).
3. Results
3.1. Demographics, IOP Results and Reproducibility
A total of 53 eyes from 28 patients were included in the final analysis. An initial review identified 56 eligible eyes, but three were excluded: one due to documented corneal irregularities that could interfere with applanation tonometry, and two due to insufficient patient cooperation during IOP measurement, which rendered the data unreliable.
Demographic characteristics and the distribution of ocular comorbidities are summarized in
Table 1. The mean age of patients was 62.6 ± 21.3 years, and 15 (54%) were male. The mean central corneal thickness (CCT) was 549 ± 48 µm, and mean visual acuity was 0.3 ± 0.1 LogMAR. Common ocular conditions included cataract (in 35 eyes), glaucoma (25 eyes), and age-related macular degeneration (dry form: 13 eyes; wet form: 5 eyes).
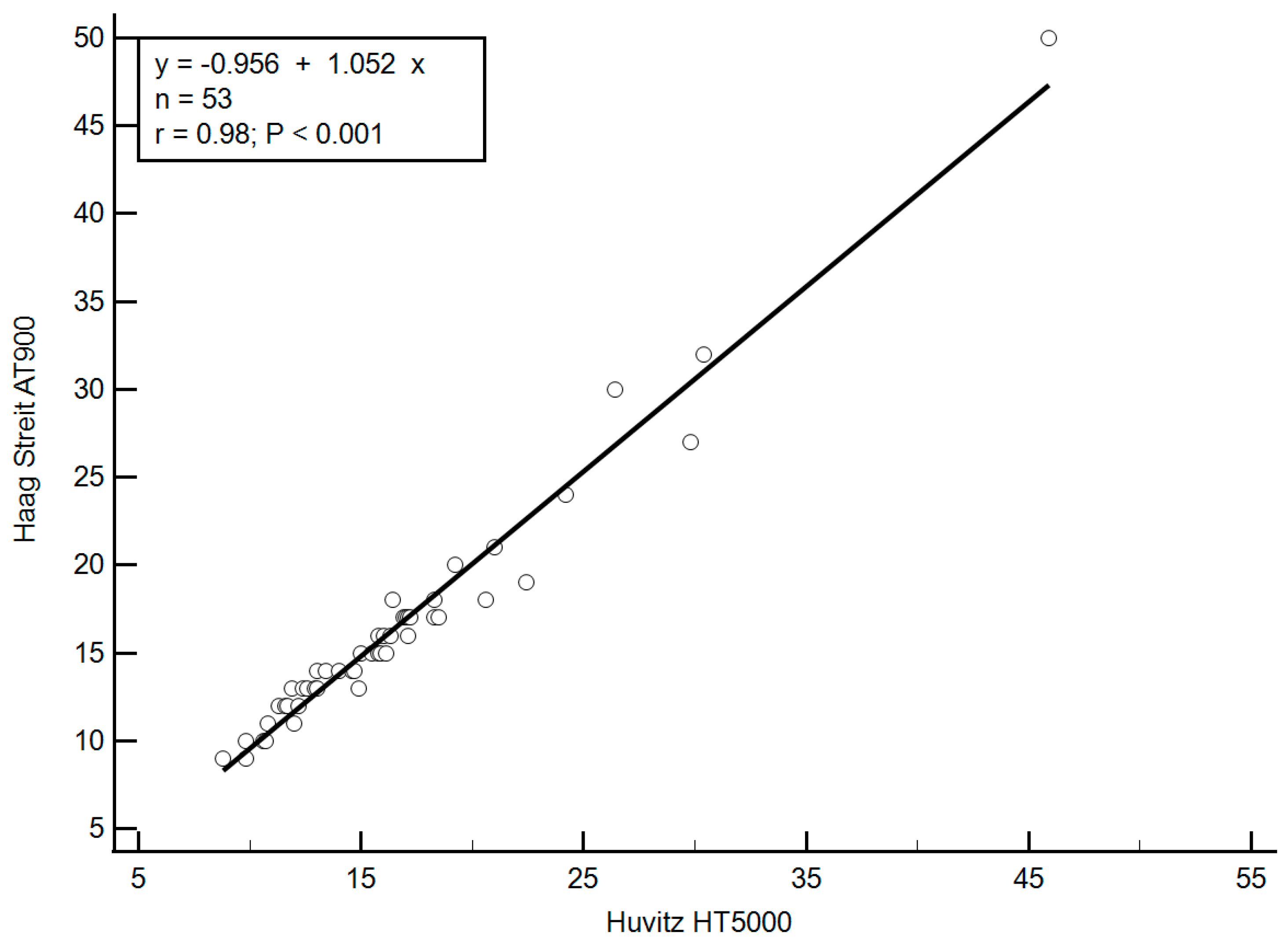
Mean intraocular pressure (IOP) values obtained with mGAT and the digital dGAT were 16.3 ± 6.6 mmHg (range: 9–50 mmHg) and 16.4 ± 6.2 mmHg (range: 8.8–45.9 mmHg), respectively. The difference between these mean values was not statistically significant (p = 0.53), suggesting a high level of agreement between the devices across the studied population.
To evaluate intra-device reproducibility, the coefficient of variation (CV) was calculated based on the paired IOP readings obtained with each tonometer. The CV for the mGAT was 3.97% (95% confidence interval [CI]: 3.36–4.49%), while the CV for the dGAT was 4.59% (95% CI: 3.95–5.15%). No statistically significant difference was observed between the CVs of the two devices (p = 0.299), indicating comparable measurement repeatability under routine clinical conditions.
3.2. Correlation and Analysis of Differences Between Measurements
A strong and statistically significant correlation was observed between IOP values measured by the mGAT and dGAT. The Pearson correlation coefficient was r = 0.98 (
p < 0.001), indicating excellent agreement between the two devices across the entire IOP range. This correlation is illustrated in
Figure 1.
In terms of absolute clinical agreement, 91% of all paired measurements fell within ±2 mmHg, and 96% were within ±3 mmHg, suggesting that in most cases, the difference between instruments was within a clinically acceptable margin (
Table 2).
To further evaluate inter-device agreement, a Bland–Altman plot was constructed by plotting the difference between mGAT and dGAT measurements against the average of the two readings (
Figure 2). The 95% limits of agreement ranged from −2.5 mmHg to +2.3 mmHg, reflecting the distribution of differences. The plot revealed a weak but statistically significant proportional bias, as demonstrated by a positive correlation between the average IOP and the inter-device difference (r = 0.35,
p = 0.011). This indicates that the difference in IOP readings increased slightly with higher IOP values.
A linear regression analysis was conducted to quantify this bias. The regression equation was as follows: Difference = (0.0679 × mean IOP) − 1.216. Based on this model, an “equilibrium point” of 17.9 mmHg was identified—the value at which both instruments were expected to yield the same IOP reading. For IOP values above 17.9 mmHg, mGAT tended to report slightly higher IOP than dGAT, increasing by approximately 0.0679 mmHg for every 1 mmHg increase in pressure. Conversely, below this point, mGAT reported slightly lower IOP values compared to dGAT.
The potential influence of central corneal thickness (CCT) on the discrepancy between instruments was also evaluated. A weak, non-significant positive correlation was found between CCT and the difference in IOP readings (r = 0.13,
p = 0.61), as shown in
Figure 3. The regression equation describing this relationship was: Difference = (0.0021 × CCT) − 1.505. This model suggests that mGAT tended to yield higher IOP readings than dGAT in eyes with thicker corneas, and vice versa for thinner corneas. The theoretical crossover, or equilibrium point, occurred at a CCT value of 717 µm. For each additional 1 µm above this point, the mGAT was expected to read approximately 0.0021 mmHg higher than the dGAT, while for each µm below this threshold, mGAT readings would be lower by the same magnitude.
4. Discussion
GAT remains the gold standard for IOP measurement due to its long-standing clinical validation, reproducibility, and widespread use [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21]. However, it is not without limitations. Both mechanical and digital GAT instruments operate according to the Imbert–Fick principle [
26], which assumes that the eye behaves as a thin-walled sphere with a perfectly flexible and dry surface—conditions not met in vivo. As a result, GAT is affected by several physiological and technical factors including CCT, corneal curvature, corneal hysteresis, the volume and concentration of fluorescein used, the impact of consecutive measurements, accommodation, and even examiner viewing angle [
5,
12,
29,
30,
31,
32]. These sources of error are equally applicable to digital tonometry platforms that retain the same underlying physical principle, such as the Huvitz HT5000 and the Haag-Streit AT900D.
Digital GAT instruments offer several practical advantages. One major improvement is the ability to display IOP values in increments of 0.1 mmHg, in contrast to the 2 mmHg scale divisions on traditional mechanical devices. This refinement eliminates the well-documented “hedgehog effect”—the digit preference toward even-numbered readings observed in mechanical tonometry [
33,
34]. Nevertheless, while the increased numerical resolution may convey an impression of superior precision, clinicians should remain mindful that the inherent accuracy of applanation tonometry is still limited to approximately ±1.5 mmHg [
4,
5,
13,
14,
15,
35,
36].
Other benefits of digital GAT devices include improved display visibility in low-light conditions, easier readability, and digital data recording capabilities.
However, these enhancements come with trade-offs. Digital tonometers such as the HT5000 and AT900D have a narrower measurable IOP range (3–75 mmHg), as compared to the 0–80 mmHg range of mechanical GAT [
37,
38]. In clinical practice, this means that IOP readings below 3 mmHg or above 75 mmHg are displayed as “Lo” or “Hi,” respectively. While measurements above 75 mmHg are seldom required in routine ophthalmic practice, accurate assessment of very low IOP is essential in specific clinical scenarios, particularly in the early postoperative period following glaucoma filtration surgery. In such cases, differentiating between an IOP of 3 mmHg, 1 mmHg, or even 0 mmHg may carry significant therapeutic implications. Digital applanation tonometers, which may lack sufficient accuracy in the low-pressure range, are therefore not suitable for use in these critical postoperative settings.
Another practical limitation of digital applanation tonometers is their dependence on battery power (four AAA batteries per unit). In high-volume clinical settings, this may necessitate more frequent battery replacements, potentially resulting in increased operational costs and workflow disruptions, particularly if battery depletion occurs during a patient examination. Although these events are uncommon, they highlight a logistical consideration that distinguishes digital tonometers from their mechanical counterparts.
As with the classic mechanical Goldmann tonometer, the accuracy and routine calibration of digital applanation devices are essential for obtaining reliable IOP measurements. Both the Haag-Streit AT900 and the Huvitz HT-5000 utilize manufacturer-supplied calibration weights for checking device accuracy at two reference points: 20 mmHg and 60 mmHg. Calibration is verified by applying the appropriate weight and confirming the corresponding IOP reading. According to manufacturer recommendations, calibration checks should be performed monthly [
37,
38]. A deviation exceeding ±0.5 mmHg at 20 mmHg or ±1.0 mmHg at 60 mmHg is considered out of tolerance and requires recalibration or servicing. These shared calibration standards underscore the similar maintenance and quality assurance protocols required for both mechanical and digital Goldmann-based tonometers.
In the present study, IOP values measured using the mechanical GAT and the digital HT5000 showed excellent agreement. The mean difference between the two instruments was only 0.11 mmHg. Bland–Altman analysis demonstrated narrow 95% limits of agreement (−2.5 to +2.3 mmHg), and 91% of paired measurements were within ±2 mmHg, a difference considered clinically insignificant by most standards.
A weak but statistically significant proportional bias was identified, wherein the mGAT tended to report slightly higher IOP values at higher IOP ranges, with a crossover or “equilibrium point” at 17.9 mmHg. For example, at IOP levels of 30 or 40 mmHg, the HT5000 would read approximately 0.8 and 1.5 mmHg lower than the mechanical GAT, respectively. However, these deviations remain well within the expected variability range of applanation techniques and are unlikely to influence clinical decision-making in most cases.
Regarding the effect of central corneal thickness, we found only a weak, non-significant correlation between CCT and inter-device differences (r = 0.13, p = 0.61). The regression model revealed a theoretical inflection point at 717 µm. For the actual CCT values in our sample—ranging from 474 µm to 648 µm—the expected IOP difference between devices remained negligible (from −0.51 to −0.14 mmHg). This suggests that, while CCT is a known confounder in applanation tonometry, its impact on the relative performance of these two instruments is minimal.
This study has several methodological strengths, including its real-world clinical setting, consistent examiner technique, and appropriate statistical analysis. However, limitations should be acknowledged. The retrospective design introduces inherent selection bias, as data were collected from patients who had both tonometers used in routine practice rather than through controlled randomization. The sample size, while numerically modest, was statistically sufficient to address the primary endpoints, as determined by formal power analysis. Nevertheless, the study may not fully capture device performance in subpopulations with extreme IOP values. Further studies with larger cohorts may help validate and extend these findings. Furthermore, the study excluded patients with corneal abnormalities, limiting generalizability to those with altered biomechanics.
5. Conclusions
In summary, the Huvitz HT5000 digital Goldmann tonometer demonstrated excellent agreement with the traditional mechanical GAT across a wide IOP range. The minimal differences observed were both statistically and clinically insignificant, supporting the device’s interchangeability in most clinical settings. While the HT5000 offers operational advantages such as enhanced digital readout and improved ergonomics, clinicians should remain aware of its limitations, particularly its inability to register extreme IOP values and its dependence on battery power. Further prospective studies involving larger and more diverse populations, including patients with corneal pathology or undergoing IOP-lowering interventions, are warranted to confirm and extend these findings.
Author Contributions
Conceptualization, A.K. and R.Y.; methodology, A.K. and R.Y.; software, A.K.; validation, A.I., A.B., M.G., A.Z. and I.G.; formal analysis, A.K. and I.G.; investigation, A.K. and R.Y.; resources, A.K. and R.Y.; data curation, A.K.; writing—original draft preparation, A.K.; writing—review and editing, A.K., R.Y., A.I., A.B., M.G., A.Z. and I.G.; visualization, A.K.; supervision, A.K.; project administration, A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Soroka Medical Center (protocol code 0396-21-SOR; approved on 27 February 2022).
Informed Consent Statement
The need for informed consent in this retrospective study was waived by the Institutional Review Board in accordance with their established guidelines and regulations.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to patient confidentiality and institutional restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Goldmann, H.; Schmidt, T.H. Über applanation tonometrie. Ophthalmologica 1957, 134, 221–242. [Google Scholar] [CrossRef] [PubMed]
- Brusini, P.; Salvetat, M.L.; Zeppieri, M.; Tosoni, C.; Parisi, L. Comparison of ICare tonometer with Goldmann applanation tonometer in glaucoma patients. J. Glaucoma 2006, 15, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Spaide, T.; Wu, Y.; Yanagihara, R.T.; Feng, S.; Ghabra, O.; Yi, J.S.; Chen, P.P.; Moses, F.; Lee, A.Y.; Wen, J.C. Using deep learning to automate Goldmann applanation tonometry Readings. Ophthalmology 2020, 127, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Sun, Z.; Li, L.; Sun, R.; Zhang, H. Comparison of intraocular pressure measured by Ocular Response Analyzer and Goldmann applanation tonometry in patients after corneal refractive surgery: A meta-analysis. BMC Ophthalmol. 2020, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Osmers, J.; Langenbucher, A.; Nguyen, N.X.; Fischer, A. Adaptive finite element eye model for the compensation of biometric influences on acoustic tonometry. Comput. Methods Programs Biomed. 2021, 200, 105930. [Google Scholar] [CrossRef] [PubMed]
- Szurman, P.; Mansouri, K.; Tanner, V.; Dick, H.B.; Hoffmann, E.M.; Mermoud, A.; Mackert, M.J.; Weinreb, R.N.; Rao, H.L.; Mansouri, K.; et al. EYEMATE-SC trial: Twelve-month safety, performance, and accuracy of a suprachoroidal sensor for telemetric measurement of intraocular pressure. Ophthalmology 2023, 130, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Choritz, L.; Mansouri, K.; van den Bosch, J.; Weigel, M.; Dick, H.B.; Wagner, M.; Thieme, H.; ARGOS Study Group. Telemetric measurement of intraocular pressure via an implantable pressure sensor: 12-month results from the ARGOS-02 trial. Am. J. Ophthalmol. 2020, 209, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.T.; Kanaster, K.; Kaizer, A.M.; Young, C.C.; Pantcheva, M.B.; Ertel, M.K.; Kahook, M.Y.; Seibold, L.K. The utility of iCare HOME tonometry for detection of therapy-related intraocular pressure changes in glaucoma and ocular hypertension. Ophthalmol. Glaucoma 2022, 5, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Kuo, D.S.; Rahimy, E. Agreement of serial iCare HOME2 and Goldmann applanation tonometry. Ophthalmol. Glaucoma 2024, 7, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Badakere, S.V.; Chary, R.; Choudhari, N.S.; Rao, H.L.; Garudadri, C.; Senthil, S. Agreement of intraocular pressure measurement of Icare ic200 with Goldmann applanation tonometer in adult eyes with normal cornea. Ophthalmol. Glaucoma 2021, 4, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Aceituno Paredes, S.C.; Asturias de León, A.L.; Barnoya Pérez, J. Rebound tonometry with re-sterilised tips versus Goldmann applanation tonometry in children. Arch. Soc. Esp. Oftalmol. Engl. Ed. 2020, 95, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Kouassi Rebours, A.C.; Kouassi, F.X.; Soumahoro, M.; Koman Chiatse Ellalie, C.E.; Alla Ngoran Siméon, K.R.A.; Agbohoun, R.P. Comparison of Goldmann tonometry with air-puff tonometry. A study of 159 patients in Abidjan. J. Fr. Ophtalmol. 2021, 44, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.W.; Wang, J.J.; Lai, C.H.; Chen, C.Y.; Lai, I.C. Assessing agreement and variability among alternative devices for intraocular pressure measurement. Clin. Ophthalmol. 2023, 17, 3453–3461. [Google Scholar] [CrossRef] [PubMed]
- Strzalkowska, A.; Pirlich, N.; Stingl, J.V.; Schuster, A.K.; Rezapour, J.; Wagner, F.M.; Buse, J.; Hoffmann, E.M. Intraocular Pressure Measurement in Childhood Glaucoma under Standardized General Anaesthesia: The Prospective EyeBIS Study. J. Clin. Med. 2022, 11, 2846. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, O.M.; Istrate, S.; Macovei, M.L.; Gheorghe, A.G. Intraocular pressure measurement after penetrating keratoplasty. Diagnostics 2022, 12, 234. [Google Scholar] [CrossRef] [PubMed]
- Gedde, S.J.; Lind, J.T.; Wright, M.M.; Chen, P.P.; Muir, K.W.; Vinod, K.; Li, T.; Mansberger, S.L. Primary Open-Angle Glaucoma Suspect Preferred Practice Pattern. Ophthalmology 2021, 128, 151–192. [Google Scholar] [CrossRef] [PubMed]
- Porwal, A.C.; Shrishrimal, M.; Punamia, R.P.; Mathew, B.C. Assessment of Intraocular Pressure Measurement Between Goldman Applanation Tonometer, Rebound Tonometer, Non-Contact Tonometer, and Its Correlation With Central Corneal Thickness. Indian J. Ophthalmol. 2023, 71, 1927–1931. [Google Scholar] [CrossRef] [PubMed]
- Stock, R.A.; Ströher, C.; Sampaio, R.R.; Mergener, R.A.; Bonamigo, E.L. A Comparative Study Between the Goldmann Applanation Tonometer and the Non-Contact Air-Puff Tonometer (Huvitz HNT 7000) in Normal Eyes. Clin. Ophthalmol. 2021, 15, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Nam, J.W.; Sung, M.S.; Park, S.W. Factors Influencing Discrepancies in Intraocular Pressure Measurements Between iCare IC200 and Goldmann Tonometer. J. Glaucoma 2025. [Google Scholar] [CrossRef] [PubMed]
- Keller, W.J. International Comparisons of Intraocular Pressures, as Measured by Tono-Pen and Goldmann Applanation Tonometry, in Healthy Adults: A Meta-Analysis. Medicine 2023, 102, e33078. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, I.; Altan, C.; Çakmak, S.; Yildirim, Y.M.; Genc, S.; Agca, A. Comparison of Intraocular Pressure Measurements With Goldmann Applanation Tonometry, Tonopen XL, and Pascal Dynamic Contour Tonometry in Patients With Descemet Membrane Endothelial Keratoplasty. J. Glaucoma 2022, 31, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Morales-Fernandez, L.; Martinez-de-la-Casa, J.M.; Garcia-Feijoo, J.; Saenz-Frances, F.; Santos, E.; Garcia-Sanchez, J. Reproducibility of the New Goldmann AT900D Digital Tonometer. J. Glaucoma 2012, 21, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Egli, M.; Goldblum, D.; Kipfer, A.; Rohrer, K.; Tappeiner, C.; Abegg, M.; Berger, L.; Schoetzau, A.; Iliev, M.E. Assessment of a new Goldmann applanation tonometer. Br. J. Ophthalmol. 2012, 96, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Sakaue, Y.; Ueda, J.; Seki, M.; Tanaka, T.; Togano, T.; Yoshino, T.; Fukuchi, T. Evaluation of the new digital Goldmann applanation tonometer for measuring intraocular pressure. J. Ophthalmol. 2014, 2014, 461681. [Google Scholar] [CrossRef] [PubMed]
- Brusini, P.; Salvetat, M.L.; Zeppieri, M. How to Measure Intraocular Pressure: An Updated Review of Various Tonometers. J. Clin. Med. 2021, 10, 3860. [Google Scholar] [CrossRef] [PubMed]
- Imbert, A. Theorie ophthalmotonometres. Arch. Ophthalmol. 1885, 5, 358–363. [Google Scholar]
- David, R.; Zangwill, L.; Stone, D.; Yassur, Y. Epidemiology of intraocular pressure in a population screened for glaucoma. Br. J. Ophthalmol. 1987, 71, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Almubrad, T.M.; Ogbuehi, K.C. The effect of repeated applanation on subsequent IOP measurements. Clin. Exp. Optom. 2008, 91, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Poostchi, A.; Mitchell, R.; Nicholas, S.; Purdie, G.; Wells, A. The iCare rebound tonometer: Comparisons with Goldmann tonometry, and influence of central corneal thickness. Clin. Exp. Ophthalmol. 2009, 37, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Whitacre, M.M.; Stein, R. Sources of error with use of Goldman-type tonometers. Surv. Ophthalmol. 1993, 38, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Lester, M.; Mete, M.; Figus, M.; Frezzotti, P. Incorporating corneal pachymetry into the management of glaucoma. J. Cataract. Refract. Surg. 2009, 35, 1623–1628. [Google Scholar] [CrossRef] [PubMed]
- Holladay, J.T.; Allison, M.E.; Prager, T.C. Goldmann applanation tonometry in patients with regular corneal astigmatism. Am. J. Ophthalmol. 1983, 96, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Buller, A.J.; Chatzinikolas, K.; Giannopoulos, N.; Nair, J.; Kelleher, S.; Raj, S.; Roy, K.; Naylor, G. Digit preference in Goldmann applanation tonometry: The hedgehog effect. Am. J. Ophthalmol. 2005, 140, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Rozwat, A.; Roberts, D.K. Even-number Measurement Bias with Goldmann Applanation Tonometry. J. Glaucoma 2020, 29, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Ogbuehi, K.C. Assessment of the accuracy and reliability of the Topcon CT80 non-contact tonometer. Clin. Exp. Optom. 2006, 89, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Dielemans, I.; Vingerling, J.R.; Hofman, A.; Grobbee, D.E.; de Jong, P.T. Reliability of intraocular pressure measurement with the Goldmann applanation tonometer in epidemiological studies. Graefe’s Arch. Clin. Exp. Ophthalmol. 1994, 232, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Haag-Streit International. Instructions for Use Manual, Applanation Tonometer AT 900D, 13th ed.; Internal Document Information: HS-Doc. No. 1500.7220067.04130; Haag-Streit, AG: Koeniz, Switzerland, 2011. [Google Scholar]
- Huvitz. Huvitz HT5000 User’s Manual. Version 1.0.; 2011 Edition; Huvitz Co., Ltd.: Anyang-si, Republic of Korea, 2011. [Google Scholar]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}
{kind=link}