
Duodenal Biopsy Audit: Relative Frequency of Diagnoses, Key Words on Request Forms Indicating Severe Pathology, and Potential Diagnoses for Intraepithelial Lymphocytosis, as a Foundation for Developing Artificial Intelligence Diagnostic Approaches

 , ,
, ,  , and
, and 
Abstract
1. Introduction
1.1. Biopsy Reporting Processes in Histopathology
1.2. Global Shortage of Pathologists
1.3. Effect on Endoscopic Duodenal Biopsies
1.4. Diagnosing Coeliac Disease in Endoscopic Duodenal Biopsies
1.5. Pathologists’ Discordance in Biopsy-Based Coeliac Disease Diagnosis
1.6. The UK Biobank
1.7. Digital Pathology
1.8. Rationale for Audit
2. Materials and Methods
2.1. Duodenal Biopsy Case Identification
2.2. Analysis of the Duodenal Biopsy Cases Identified
2.3. Identification of Key Words Indicative of Serious Pathology
2.4. Demographic and Clinical Features Associated with Isolated Intraepithelial Lymphocytosis
2.5. Attempted Refinement of Diagnosis in Cases of Isolated Intraepithelial Lymphocytosis
2.6. Calculated of Expected UK Population Frequency of Coeliac-Risk HLA Types Using the UK Biobank
2.7. Determination of Conditions Associated with Isolated Intraepithelial Lymphocytosis
2.8. Literature Review of Conditions Associated with Isolated Intraepithelial Lymphocytosis
2.9. Recording of Other Abnormal Laboratory Investigations in Patients with Isolated Intraepithelial Lymphocytosis
3. Results
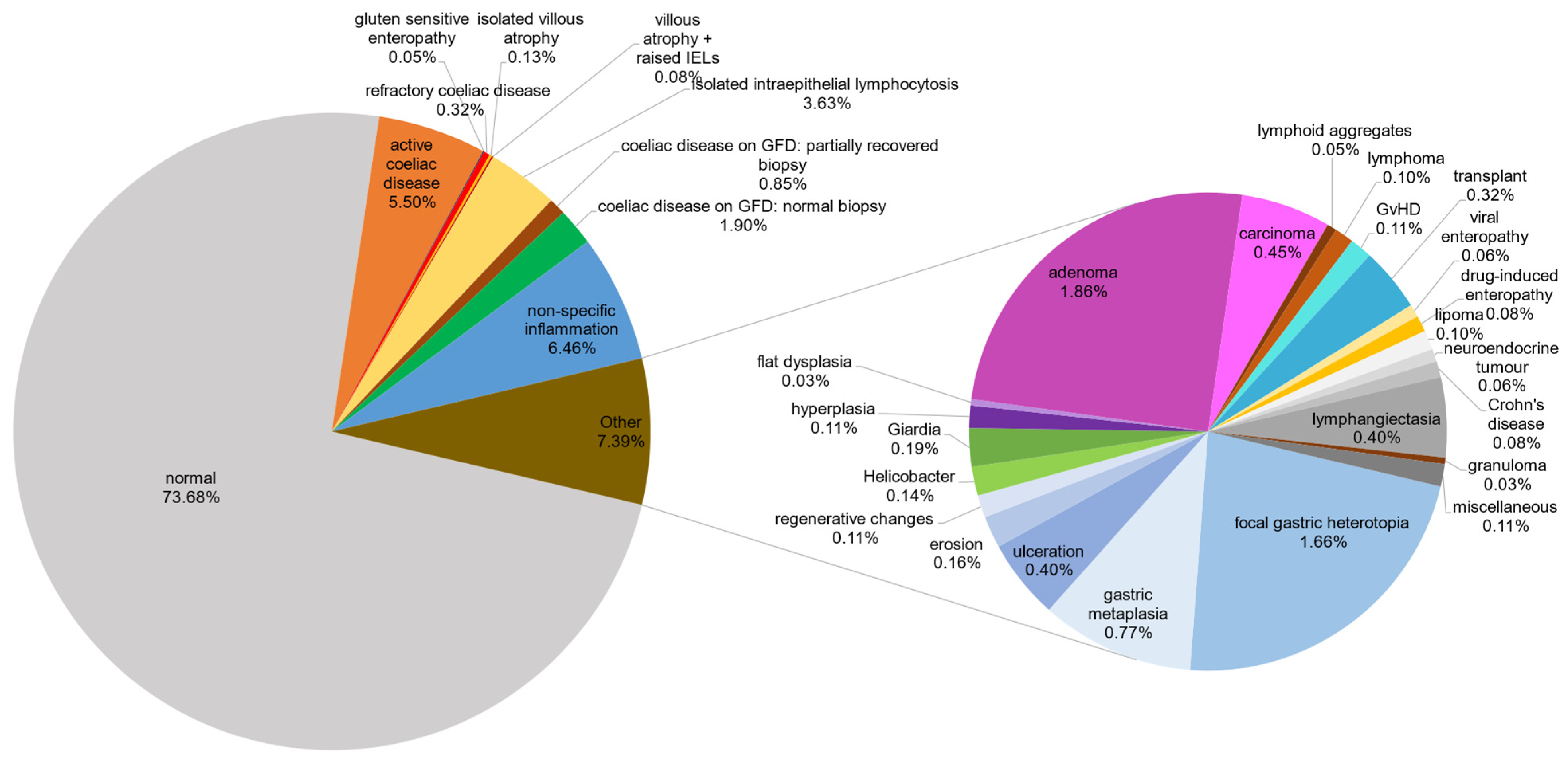
3.1. Summary of Biopsy Diagnostic Categories
3.2. Key Words for Minor Diagnostic Categories
3.3. Isolated Intraepithelial Lymphocytosis
4. Discussion
5. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hayat, M.; Cairns, A.; Dixon, M.F.; O’Mahony, S. Quantitation of Intraepithelial Lymphocytes in Human Duodenum: What Is Normal? J. Clin. Pathol. 2002, 55, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Marsh, M.N.; Rostami, K. What Is A Normal Intestinal Mucosa? Gastroenterology 2016, 151, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Oberhuber, G. Histopathology of Celiac Disease. Biomed. Pharmacother. 2000, 54, 368–372. [Google Scholar] [CrossRef]
- Tsung, J.S.H. Institutional Pathology Consultation. Am. J. Surg. Pathol. 2004, 28, 399. [Google Scholar] [CrossRef]
- Frable, W.J. Surgical Pathology—Second Reviews, Institutional Reviews, Audits, and Correlations: What’s Out There? Error or Diagnostic Variation? Arch. Pathol. Lab. Med. 2006, 130, 620–625. [Google Scholar] [CrossRef]
- Ordi, J.; Castillo, P.; Saco, A.; del Pino, M.; Ordi, O.; Rodríguez-Carunchio, L.; Ramírez, J. Validation of Whole Slide Imaging in the Primary Diagnosis of Gynaecological Pathology in a University Hospital. J. Clin. Pathol. 2015, 68, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Metter, D.M.; Colgan, T.J.; Leung, S.T.; Timmons, C.F.; Park, J.Y. Trends in the US and Canadian Pathologist Workforces From 2007 to 2017. JAMA Netw. Open 2019, 2, e194337. [Google Scholar] [CrossRef]
- The Royal College of Pathologists of Australia. Australian Pathologists Workforce Study 2018. Available online: https://www.rcpa.edu.au/getattachment/4a38b4f9-5f6a-45eb-8947-dfa072797685/APW.aspx (accessed on 22 January 2024).
- Märkl, B.; Füzesi, L.; Huss, R.; Bauer, S.; Schaller, T. Number of Pathologists in Germany: Comparison with European Countries, USA, and Canada. Virchows Arch. 2021, 478, 335–341. [Google Scholar] [CrossRef]
- Robboy, S.J.; Weintraub, S.; Horvath, A.E.; Jensen, B.W.; Alexander, C.B.; Fody, E.P.; Crawford, J.M.; Clark, J.R.; Cantor-Weinberg, J.; Joshi, M.G.; et al. Pathologist Workforce in the United States: I. Development of a Predictive Model to Examine Factors Influencing Supply. Arch. Pathol. Lab. Med. 2013, 137, 1723–1732. [Google Scholar] [CrossRef]
- Mudenda, V.; Malyangu, E.; Sayed, S.; Fleming, K. Addressing the Shortage of Pathologists in Africa: Creation of a MMed Programme in Pathology in Zambia. Afr. J. Lab. Med. 2020, 9, 974. [Google Scholar] [CrossRef]
- Bychkov, A.; Schubert, M. Constant Demand, Patchy Supply. Pathologist 2023, 88, 18–27. [Google Scholar]
- Martin, J. Meeting Pathology Demand: Histopathology Workforce Census. 2018. Available online: https://www.rcpath.org/static/952a934d-2ec3-48c9-a8e6e00fcdca700f/Meeting-Pathology-Demand-Histopathology-Workforce-Census-2018.pdf (accessed on 27 May 2025).
- The Royal College of Pathologists. Head Count of Histopathologists in the UK—By Region and Devolved Nation. Available online: https://www.rcpath.org/static/797e5533-d718-442a-be4ee7e695a5550e/Histopathologists.pdf (accessed on 27 May 2025).
- Adesina, A.; Chumba, D.; Nelson, A.M.; Orem, J.; Roberts, D.J.; Wabinga, H.; Wilson, M.; Rebbeck, T.R. Improvement of Pathology in Sub-Saharan Africa. Lancet Oncol. 2013, 14, e152–e157. [Google Scholar] [CrossRef] [PubMed]
- Coeliac UK. Diagnosis of Coeliac Disease. Available online: https://www.coeliac.org.uk/healthcare-professionals/diagnosis/ (accessed on 23 January 2024).
- Downey, L.; Houten, R.; Murch, S.; Longson, D. Recognition, Assessment, and Management of Coeliac Disease: Summary of Updated NICE Guidance. Bmj 2015, 351, h4513. [Google Scholar] [CrossRef] [PubMed]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac Disease: A Comprehensive Current Review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Coeliac Disease: Recognition, Assessment and Management. 2024. Available online: https://www.nice.org.uk/guidance/ng20/evidence/full-guideline-pdf-438530077 (accessed on 23 January 2024).
- Denholm, J.; Schreiber, B.A.; Jaeckle, F.; Wicks, M.N.; Benbow, E.W.; Bracey, T.S.; Chan, J.Y.; Farkas, L.; Fryer, E.; Gopalakrishnan, K. CD, or Not CD, That Is the Question: A Digital Interobserver Agreement Study in Coeliac Disease. BMJ Open Gastroenterol. 2024, 11, e001252. [Google Scholar] [CrossRef]
- Villanacci, V.; Lorenzi, L.; Donato, F.; Auricchio, R.; Dziechciarz, P.; Gyimesi, J.; Koletzko, S.; Mišak, Z.; Laguna, V.M.; Polanco, I.; et al. Histopathological Evaluation of Duodenal Biopsy in the PreventCD Project. An Observational Interobserver Agreement Study. APMIS 2018, 126, 208–214. [Google Scholar] [CrossRef]
- Picarelli, A.; Borghini, R.; Donato, G.; Di Tola, M.; Boccabella, C.; Isonne, C.; Giordano, M.; Di Cristofano, C.; Romeo, F.; Di Cioccio, G.; et al. Weaknesses of Histological Analysis in Celiac Disease Diagnosis: New Possible Scenarios. Scand. J. Gastroenterol. 2014, 49, 1318–1324. [Google Scholar] [CrossRef]
- Arguelles-Grande, C.; Tennyson, C.A.; Lewis, S.K.; Green, P.H.R.; Bhagat, G. Variability in Small Bowel Histopathology Reporting between Different Pathology Practice Settings: Impact on the Diagnosis of Coeliac Disease. J. Clin. Pathol. 2012, 65, 242. [Google Scholar] [CrossRef]
- Alessio, M.G.; Tonutti, E.; Brusca, I.; Radice, A.; Licini, L.; Sonzogni, A.; Florena, A.; Schiaffino, E.; Marus, W.; Sulfaro, S.; et al. Correlation between IgA Tissue Transglutaminase Antibody Ratio and Histological Finding in Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 44–49. [Google Scholar] [CrossRef]
- Corazza, G.R.; Villanacci, V.; Zambelli, C.; Milione, M.; Luinetti, O.; Vindigni, C.; Chioda, C.; Albarello, L.; Bartolini, D.; Donato, F. Comparison of the Interobserver Reproducibility with Different Histologic Criteria Used in Celiac Disease. Clin. Gastroenterol. Hepatol. 2007, 5, 838–843. [Google Scholar] [CrossRef]
- Montén, C.; Bjelkenkrantz, K.; Gudjonsdottir, A.H.; Browaldh, L.; Arnell, H.; Naluai, Å.T.; Agardh, D. Validity of Histology for the Diagnosis of Paediatric Coeliac Disease: A Swedish Multicentre Study. Scand. J. Gastroenterol. 2016, 51, 427–433. [Google Scholar] [CrossRef]
- Collin, P.; Wahab, P.J.; Murray, J.A. Intraepithelial Lymphocytes and Coeliac Disease. Best Pract. Res. Clin. Gastroenterol. 2005, 19, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Hammer, S.T.G.; Greenson, J.K. The Clinical Significance of Duodenal Lymphocytosis with Normal Villus Architecture. Arch. Pathol. Lab. Med. 2013, 137, 1216–1219. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.M.; Papanicolas, I.N. Impact of Symptoms on Quality of Life before and after Diagnosis of Coeliac Disease: Results from a UK Population Survey. BMC Health Serv. Res. 2010, 10, 105. [Google Scholar] [CrossRef]
- Watts, G. UK Biobank Opens Its Data Vaults to Researchers. 2012. Available online: https://www.bmj.com/content/344/bmj.e2459.full (accessed on 19 February 2025).
- Bahcall, O.G. UK Biobank–a New Era in Genomic Medicine. Nat. Rev. Genet. 2018, 19, 737–738. [Google Scholar] [CrossRef]
- UK Biobank. Imputation of Classical HLA Types. 2016. Available online: https://biobank.ctsu.ox.ac.uk/crystal/refer.cgi?id=182 (accessed on 27 May 2025).
- Ting, Y.T.; Dahal-Koirala, S.; Kim, H.S.K.; Qiao, S.-W.; Neumann, R.S.; Lundin, K.E.A.; Petersen, J.; Reid, H.H.; Sollid, L.M.; Rossjohn, J. A Molecular Basis for the T Cell Response in HLA-DQ2.2 Mediated Celiac Disease. Proc. Natl. Acad. Sci. USA 2020, 117, 3063. [Google Scholar] [CrossRef]
- Holten-Rossing, H.; Talman, M.-L.M.; Jylling, A.M.B.; Lænkholm, A.-V.; Kristensson, M.; Vainer, B. Application of Automated Image Analysis Reduces the Workload of Manual Screening of Sentinel Lymph Node Biopsies in Breast Cancer. Histopathology 2017, 71, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Ström, P.; Kartasalo, K.; Olsson, H.; Solorzano, L.; Delahunt, B.; Berney, D.M.; Bostwick, D.G.; Evans, A.J.; Grignon, D.J.; Humphrey, P.A.; et al. Artificial Intelligence for Diagnosis and Grading of Prostate Cancer in Biopsies: A Population-Based, Diagnostic Study. Lancet Oncol. 2020, 21, 222–232. [Google Scholar] [CrossRef]
- Brodsky, V.; Levine, L.; Solans, E.P.; Dola, S.; Chervony, L.; Polak, S. Performance of Automated Classification of Diagnostic Entities in Dermatopathology Validated on Multisite Data Representing the Real-World Variability of Pathology Workload. Arch. Pathol. Lab. Med. 2023, 147, 1093–1098. [Google Scholar] [CrossRef]
- Al-Janabi, S.; Huisman, A.; Van Diest, P.J. Digital Pathology: Current Status and Future Perspectives. Histopathology 2012, 61, 1–9. [Google Scholar] [CrossRef]
- Jahn, S.W.; Plass, M.; Moinfar, F. Digital Pathology: Advantages, Limitations and Emerging Perspectives. J. Clin. Med. 2020, 9, 3697. [Google Scholar] [CrossRef] [PubMed]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A. International Evaluation of an AI System for Breast Cancer Screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef]
- Denholm, J.; Schreiber, B.A.; Evans, S.C.; Crook, O.M.; Sharma, A.; Watson, J.L.; Bancroft, H.; Langman, G.; Gilbey, J.D.; Schönlieb, C.-B.; et al. Multiple-Instance-Learning-Based Detection of Coeliac Disease in Histological Whole-Slide Images. J. Pathol. Inform. 2022, 13, 100151. [Google Scholar] [CrossRef]
- Jaeckle, F.; Bryant, R.; Denholm, J.; Romero Diaz, J.; Schreiber, B.; Shenoy, V.; Ekundayomi, D.; Evans, S.; Arends, M.; Soilleux, E. Interpretable Machine Learning Based Detection of Coeliac Disease. medRxiv 2025. [Google Scholar] [CrossRef]
- Jaeckle, F.; Denholm, J.; Schreiber, B.; Evans, S.C.; Wicks, M.N.; Chan, J.Y.H.; Bateman, A.C.; Natu, S.; Arends, M.J.; Soilleux, E. Machine Learning Achieves Pathologist-Level Celiac Disease Diagnosis. NEJM AI 2025, 2, AIoa2400738. [Google Scholar] [CrossRef] [PubMed]
- Torres-Bondia, F.; de Batlle, J.; Galván, L.; Buti, M.; Barbé, F.; Piñol-Ripoll, G. Evolution of the Consumption Trend of Proton Pump Inhibitors in the Lleida Health Region between 2002 and 2015. BMC Public Health 2022, 22, 818. [Google Scholar] [CrossRef]
- Brennan, R.; Wazaify, M.; Shawabkeh, H.; Boardley, I.; McVeigh, J.; Van Hout, M.C. A Scoping Review of Non-Medical and Extra-Medical Use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). Drug Saf. 2021, 44, 917–928. [Google Scholar] [CrossRef]
- Hackett, R.J.; Preston, S.L. H. pylori Infection, Part I: Clinical Burden and Diagnosis. Trends Urol. Men’s Health 2021, 12, 13–19. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Quality Standards and Indicators—Irritable Bowel Syndrome. 2015. Available online: https://www.nice.org.uk/guidance/QS114/documents/irritable-bowel-syndrome-in-adults-qs-briefing-paper2 (accessed on 27 May 2025).
- National Institute for Health and Care Excellence. Thyroid Disease: Assessment and Management. 2023. Available online: https://www.nice.org.uk/guidance/ng145/chapter/Context (accessed on 27 May 2025).
- National Institute for Health and Care Excellence. Hyperthyroidism. Available online: https://cks.nice.org.uk/topics/hyperthyroidism/background-information/prevalence/ (accessed on 27 May 2025).
- Green, H.D.; Beaumont, R.N.; Thomas, A.; Hamilton, B.; Wood, A.R.; Sharp, S.; Jones, S.E.; Tyrrell, J.; Walker, G.; Goodhand, J.; et al. Genome-Wide Association Study of Microscopic Colitis in the UK Biobank Confirms Immune-Related Pathogenesis. J Crohn’s Colitis 2019, 13, 1578–1582. [Google Scholar] [CrossRef]
- Mohamed, M.; Thio, J.; Thomas, R.S.; Phillips, J. Pernicious Anaemia. BMJ 2020, 369, m1319. [Google Scholar] [CrossRef]
- Pasvol, T.J.; Horsfall, L.; Bloom, S.; Segal, A.W.; Sabin, C.; Field, N.; Rait, G. Incidence and Prevalence of Inflammatory Bowel Disease in UK Primary Care: A Population-Based Cohort Study. BMJ Open 2020, 10, e036584. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Rheumatoid Arthritis. 2025. Available online: https://cks.nice.org.uk/topics/rheumatoid-arthritis/background-information/prevalence-incidence/ (accessed on 27 May 2025).
- National Institute for Health and Care Excellence. Axial Spondyloarthritis (Including Ankylosing Spondylitis). 2024. Available online: https://cks.nice.org.uk/topics/axial-spondyloarthritis-including-ankylosing-spondylitis/background-information/prevalence/ (accessed on 27 May 2025).
- National Institute for Health and Care Excellence. Gastrointestinal Tract (Lower) Cancers—Recognition and Referral. 2025. Available online: https://cks.nice.org.uk/topics/gastrointestinal-tract-lower-cancers-recognition-referral/background-information/prevalence/ (accessed on 27 May 2025).
- National Institute for Health and Care Excellence. Gastrointestinal Tract (Upper) Cancers—Recognition and Referral. 2025. Available online: https://cks.nice.org.uk/topics/gastrointestinal-tract-upper-cancers-recognition-referral/ (accessed on 27 May 2025).
- Sen, R.; Goyal, A.; Hurley, J.A. Seronegative Spondyloarthropathy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Burton, C.; Cottrell, E.; Edwards, J. Addison’s Disease: Identification and Management in Primary Care. Br. J. Gen. Pract. 2015, 65, 488–490. [Google Scholar] [CrossRef] [PubMed]
- NHS Blood and Transplant. Annual Report on Intestine Transplantation. 2022. Available online: https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/27817/nhsbt-annual-report-on-intestine-transplantation-202122.pdf (accessed on 27 May 2025).
- Delle Fave, G.; Kwekkeboom, D.J.; Van Cutsem, E.; Rindi, G.; Kos-Kudla, B.; Knigge, U.; Sasano, H.; Tomassetti, P.; Salazar, R.; Ruszniewski, P.; et al. ENETS Consensus Guidelines for the Management of Patients with Gastroduodenal Neoplasms. Neuroendocrinology 2011, 95, 74–87. [Google Scholar] [CrossRef] [PubMed]
- NICE. How Should I Assess a Person with Suspected Coeliac Disease? Available online: https://cks.nice.org.uk/topics/coeliac-disease/diagnosis/assessment/#:~:text=Consider%20checking%20serum%20IgG%20EMA,care%20to%20diagnose%20coeliac%20disease (accessed on 19 February 2025).


{kind=link}
{kind=link}
| Classification | Total (n) | Percentage (%) |
|---|---|---|
| Normal | 4606 | 73.76 |
| Coeliac-associated diagnoses | 552 | 8.84 |
| Active coeliac disease | 344 | 5.50 |
| Coeliac disease on GFD 1: normal biopsy | 119 | 1.90 |
| Coeliac disease on GFD: partially recovered biopsy | 53 | 0.85 |
| Refractory coeliac disease | 20 | 0.32 |
| Isolated villous atrophy | 8 | 0.13 |
| Villous atrophy + raised IELs 2 | 5 | 0.08 |
| Gluten-sensitive enteropathy | 3 | 0.05 |
| Isolated intraepithelial lymphocytosis | 227 | 3.63 |
| Non-specific inflammation | 404 | 6.46 |
| Neoplastic changes | ||
| Adenoma | 116 | 1.86 |
| Carcinoma | 28 | 0.45 |
| Lymphoma | 6 | 0.10 |
| Lipoma | 6 | 0.10 |
| Neuroendocrine tumour | 4 | 0.06 |
| Flat dysplasia | 2 | 0.03 |
| Infections | ||
| Giardiasis | 12 | 0.19 |
| Helicobacter pylori infection | 9 | 0.14 |
| Viral enteropathy | 4 | 0.06 |
| Benign gastric epithelium-related changes | ||
| Focal gastric heterotopia | 104 | 1.66 |
| Gastric metaplasia | 48 | 0.77 |
| Duodenal mucosal surface changes | ||
| Ulceration | 25 | 0.40 |
| Lymphangiectasia | 25 | 0.40 |
| Erosion | 10 | 0.16 |
| Regenerative changes | 7 | 0.11 |
| Hyperplasia | 7 | 0.11 |
| Autoimmune/Inflammatory conditions | ||
| Crohn’s disease | 5 | 0.08 |
| Drug-induced enteropathy | 5 | 0.08 |
| Lymphoid aggregates | 3 | 0.05 |
| Granuloma | 2 | 0.03 |
| Transplant-related diagnoses | ||
| Transplant | 20 | 0.32 |
| Graft versus host disease (GvHD) | 7 | 0.11 |
| Miscellaneous | 7 | 0.11 |
| Total | 6245 | 100 |
| Biopsy Diagnostic Category * | Clinical Key Words |
|---|---|
| Adenoma | Gastrointestinal bleeding, familial adenomatous polyposis (FAP), and polyp or papillary tumours on endoscopy |
| Amyloidosis | Systemic infiltrative disease |
| Carcinoma | Jaundice, gastrointestinal bleeding, bowel obstruction, mass or dilated bile duct on imaging or endoscopic examination, and previous diagnosis of malignancy of any organ |
| Common variable immunodeficiency | Background of immunodeficiency syndrome, opportunistic infections (norovirus in our data) |
| Crohn’s disease | Previous diagnosis of Crohn’s disease, stricture, and fistula |
| Drug-induced enteropathy | Established autoimmune disease on immunomodulators/NSAIDs † |
| Flat (non-adenoma) dysplasia | Gastrointestinal bleeding, necrotic ulcer |
| Focal gastric heterotopia | Polyp on endoscopy |
| Gastric metaplasia | Polyp on endoscopy |
| Giardia | Iron deficiency anaemia, weight loss, and abdominal pain |
| Granuloma | History of tuberculosis or Crohn’s disease |
| Hyperplasia without dysplasia | Polyp on endoscopy |
| Lipoma | Nodule on endoscopy |
| Lymphangiectasia | Gastrointestinal bleeding, ill-defined mass on endoscopy |
| Lymphoid aggregates | Mass on endoscopy |
| Lymphoma | Duodenal mass, gastrointestinal bleeding, and previous diagnosis of lymphoma |
| Neuroendocrine tumour | Nodule/polyp |
| Ulceration | Gastrointestinal bleeding, abnormal barium study, and relevant drug history (NSAIDs †) |
| Viral enteropathy | Immune suppression |
| Characteristic | Finding (n = 227) |
|---|---|
| Median age in years (standard deviation) | 49 (17.7) |
| Female sex (%) | 163 (71.8) |
| Male sex (%) | 64 (28.2) |
| Indications for Biopsy (%) | |
| Iron deficiency anaemia | 108 (47.6) |
| Diarrhoea | 44 (19.4) |
| Abdominal pain | 32 (14.1) |
| Weight loss | 33 (14.5) |
| Dyspepsia | 24 (10.6) |
| Reflux | 16 (7.1) |
| Nausea or vomiting | 9 (4.0) |
| Folate deficiency | 9 (4.0) |
| Non-specific altered bowel movements | 8 (3.5) |
| Dysphagia | 8 (3.5) |
| Bloating | 7 (3.1) |
| Constipation | 4 (1.8) |
| Vitamin B12 deficiency | 4 (1.8) |
| No information provided | 23 (10.1) |
| Characteristic | Finding (n = 33) |
|---|---|
| Median age in years (standard deviation) | 48 (16.6) |
| Female sex (%) | 23 (69.7) |
| Male sex (%) | 10 (30.3) |
| Integrated clinical diagnosis of coeliac disease (%) | n = 24 |
| Prior to biopsy | 9 (27.3) |
| Subsequent to biopsy | 13 (39.4) |
| After further biopsy | 2 (6.1) |
| Features strongly suspicious for coeliac disease (%) | n = 9 |
| Positive IgA(tTG) and positive EMA | 5 (15.2) |
| Positive IgA(tTG) and negative/missing EMA | 4 (12.1) |
| Associated Condition | Number of Cases, n (%) (N = 227) | Prevalence in UK Population (From Published Studies) |
|---|---|---|
| Proton pump inhibitor use | 26 (11.45) | 18.04% [43] |
| NSAID 1 use | 18 (7.93) | Variable [44] |
| Helicobacter pylori infection | 12 (5.29) | Up to 35% [45] |
| Irritable bowel syndrome | 9 (3.96) | 10–20% [46] |
| Hypothyroidism | 8 (3.52) | 2% [47] |
| Graves’ disease | 6 (2.64) | 0.75% [48] |
| Microscopic colitis | 4 (1.76) | 0.1% [49] |
| Pernicious anaemia | 3 (1.32) | 0.05–0.2% [50] |
| Crohn’s disease | 3 (1.32) | 0.27% [51] |
| Rheumatoid arthritis | 3 (1.32) | 1% [52] |
| Ankylosing spondylitis | 3 (1.32) | 0.05–0.2% [53] |
| Gastrointestinal adenocarcinoma | 3 (1.32) | Variable [54,55] |
| Ulcerative colitis | 2 (0.88) | 0.39% [51] |
| Seronegative spondyloarthropathy | 2 (0.88) | 0.5–1.9% [56] |
| Addison’s disease | 2 (0.88) | 0.01% [57] |
| Transplanted ileum and colon | 1 (0.44) | 19 cases in 2018–19 [58] |
| Duodenal neuroendocrine tumour | 1 (0.44) | 0.00017% [59] |
| Abnormal Laboratory Test | Likely Significance of Test | Number of Cases, n (%) |
|---|---|---|
| Elevated faecal calprotectin | Raised in inflammatory bowel disease (e.g., Crohn’s disease, ulcerative colitis), but can be raised in many inflammatory gastrointestinal conditions, including coeliac disease and infection | 37 (16.3) |
| Elevated ESR 1 | Raised in many inflammatory and autoimmune conditions, but also in infections and cancer | 17 (7.5) |
| Elevated CRP 2 | Raised in many inflammatory and autoimmune conditions, but also in infections and tissue injury | 15 (6.6) |
| IgA 3 deficiency | A common immunodeficiency, which may be asymptomatic, or associated with recurrent respiratory infections, allergies, and autoimmune conditions | 10 (4.4) |
| Elevated ANA 4 | A relatively non-specific marker of autoimmune disease | 8 (3.5) |
| Elevated rheumatoid factor | A relatively non-specific marker of autoimmune disease, particularly rheumatoid arthritis | 7 (3.1) |
| Elevated p-ANCA 5 | A marker of autoimmune disease, particularly, but not exclusively, those affecting blood vessels (vasculitis) and the kidney (glomerulonephritis) | 3 (1.3) |
| Elevated anti-cyclic citrullinated protein | A highly specific marker for rheumatoid arthritis | 2 (0.9) |
| Elevated c-ANCA 6 | A marker of autoimmune disease, particularly, but not exclusively, those affecting blood vessels (vasculitis) and the kidney (glomerulonephritis) | 1 (0.4) |
| Elevated anti-U1 RNP 7 | A marker strongly associated with a group of autoimmune conditions, known as mixed connective tissue disease | 1 (0.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shenoy, V.; James, J.L.; Williams-Walker, A.B.; Madhan Mohan, N.P.R.; Luu Hoang, K.N.; Williams, J.; Jaeckle, F.; Evans, S.C.; Soilleux, E.J. Duodenal Biopsy Audit: Relative Frequency of Diagnoses, Key Words on Request Forms Indicating Severe Pathology, and Potential Diagnoses for Intraepithelial Lymphocytosis, as a Foundation for Developing Artificial Intelligence Diagnostic Approaches. Diagnostics 2025, 15, 1483. https://doi.org/10.3390/diagnostics15121483
Shenoy V, James JL, Williams-Walker AB, Madhan Mohan NPR, Luu Hoang KN, Williams J, Jaeckle F, Evans SC, Soilleux EJ. Duodenal Biopsy Audit: Relative Frequency of Diagnoses, Key Words on Request Forms Indicating Severe Pathology, and Potential Diagnoses for Intraepithelial Lymphocytosis, as a Foundation for Developing Artificial Intelligence Diagnostic Approaches. Diagnostics. 2025; 15(12):1483. https://doi.org/10.3390/diagnostics15121483
Chicago/Turabian StyleShenoy, Vrinda, Jessica L. James, Amelia B. Williams-Walker, Nasyen P. R. Madhan Mohan, Kim N. Luu Hoang, Josephine Williams, Florian Jaeckle, Shelley C. Evans, and Elizabeth J. Soilleux. 2025. "Duodenal Biopsy Audit: Relative Frequency of Diagnoses, Key Words on Request Forms Indicating Severe Pathology, and Potential Diagnoses for Intraepithelial Lymphocytosis, as a Foundation for Developing Artificial Intelligence Diagnostic Approaches" Diagnostics 15, no. 12: 1483. https://doi.org/10.3390/diagnostics15121483
APA StyleShenoy, V., James, J. L., Williams-Walker, A. B., Madhan Mohan, N. P. R., Luu Hoang, K. N., Williams, J., Jaeckle, F., Evans, S. C., & Soilleux, E. J. (2025). Duodenal Biopsy Audit: Relative Frequency of Diagnoses, Key Words on Request Forms Indicating Severe Pathology, and Potential Diagnoses for Intraepithelial Lymphocytosis, as a Foundation for Developing Artificial Intelligence Diagnostic Approaches. Diagnostics, 15(12), 1483. https://doi.org/10.3390/diagnostics15121483