
Serum Interleukin-17 and Its Association with Inflammation and Bone Remodeling in Rheumatoid Arthritis and Hand Osteoarthritis: Insights from Musculoskeletal Ultrasound

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Subjects
2.3. Clinical History and Health Assessment
2.4. Physical Examination
2.5. Musculoskeletal Ultrasound Examination
2.6. Blood Sampling
2.7. Quantitation of IL-17A Serum Level
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, S.H.; Dong, C. Signaling of interleukin-17 family cytokines in immunity and inflammation. Cell Signal 2011, 23, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Huangfu, L.; Li, R.; Huang, Y.; Wang, S. The IL-17 family in diseases: From bench to bedside. Signal Transduct. Target. Ther. 2023, 8, 402. [Google Scholar] [CrossRef] [PubMed]
- Hemdan, N.Y.A.; Birkenmeier, G.; Wichmann, G.; Abu El-Saad, A.M.; Krieger, T.; Conrad, K.; Sack, U. Interleukin-17-producing T helper cells in autoimmunity. Autoimmun. Rev. 2010, 9, 785–792. [Google Scholar] [CrossRef]
- McGeachy, M.J.; Cua, D.J.; Gaffen, S.L. The IL-17 Family of Cytokines in Health and Disease. Immunity 2019, 50, 892–906. [Google Scholar] [CrossRef]
- Robert, M.; Miossec, P. IL-17 in Rheumatoid Arthritis and Precision Medicine: From Synovitis Expression to Circulating Bioactive Levels. Front. Med. 2018, 5, 364. [Google Scholar] [CrossRef] [PubMed]
- Tsukazaki, H.; Kaito, T. The Role of the IL-23/IL-17 Pathway in the Pathogenesis of Spondyloarthritis. Int. J. Mol. Sci. 2020, 21, 6401. [Google Scholar] [CrossRef]
- Blauvelt, A.; Chiricozzi, A. The Immunologic Role of IL-17 in Psoriasis and Psoriatic Arthritis Pathogenesis. Clin. Rev. Allergy Immunol. 2018, 55, 379–390. [Google Scholar] [CrossRef]
- Zhang, X.; Yuan, Y.; Pan, Z.; Ma, Y.; Wu, M.; Yang, J.; Han, R.; Chen, M.; Hu, X.; Liu, R.; et al. Elevated circulating IL-17 level is associated with inflammatory arthritis and disease activity: A meta-analysis. Clin. Chim. Acta 2019, 496, 76–83. [Google Scholar] [CrossRef]
- Afzali, B.; Lombardi, G.; Lechler, R.I.; Lord, G.M. The role of T helper 17 (Th17) and regulatory T cells (Treg) in human organ transplantation and autoimmune disease. Clin. Exp. Immunol. 2007, 148, 32–46. [Google Scholar] [CrossRef]
- Kamel, S.; Khalaf, R.; Moness, H.; Ahmed, S. Serum and Synovial Fluid Levels of Interleukin-17A in Primary Knee Osteoarthritis Patients: Correlations with Functional Status, Pain, and Disease Severity. Arch. Rheumatol. 2022, 37, 187–194. [Google Scholar] [CrossRef]
- van Baarsen, L.G.M.; Lebre, M.C.; van der Coelen, D.; Aarrass, S.; Tang, M.W.; Ramwadhdoebe, T.H.; Gerlag, D.M.; Tak, P.P. Heterogeneous expression pattern of interleukin 17A (IL-17A), IL-17F and their receptors in synovium of rheumatoid arthritis, psoriatic arthritis and osteoarthritis: Possible explanation for nonresponse to anti-IL-17 therapy? Arthritis Res. Ther. 2014, 16, 426. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, G.; Puig, L. Pathogenic Role of IL-17 and Therapeutic Targeting of IL-17F in Psoriatic Arthritis and Spondyloarthropathies. Int. J. Mol. Sci. 2023, 24, 10305. [Google Scholar] [CrossRef] [PubMed]
- Sapundzhieva, T.L.; Karalilova, R.; Batalov, A. Musculoskeletal Ultrasound in Rheumatology—New Horizons. Folia Medica 2020, 62, 7–16. [Google Scholar] [CrossRef]
- Perricone, C.; Ceccarelli, F.; Modesti, M.; Vavala, C.; Di Franco, M.; Valesini, G.; Iagnocco, A. The 6-joint ultrasonographic assessment: A valid, sensitive-to-change and feasible method for evaluating joint inflammation in RA. Rheumatology 2011, 51, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, M.; Kamradt, T.; Sandrock, D.; Loreck, D.; Fritz, J.; Wolf, K.J.; Raber, H.; Hamm, B.; Burmester, G.R.; Bollow, M. Arthritis of the finger joints: A comprehensive approach comparing conventional radiography, scintigraphy, ultrasound, and contrast-enhanced magnetic resonance imaging. Arthritis Rheum. 1999, 42, 1232–1245. [Google Scholar] [CrossRef]
- Bruyn, G.A.; Iagnocco, A.; Naredo, E.; Balint, P.V.; Gutierrez, M.; Hammer, H.B.; Collado, P.; Filippou, G.; Schmidt, W.A.; Jousse-Joulin, S.; et al. OMERACT Definitions for Ultrasonographic Pathologies and Elementary Lesions of Rheumatic Disorders 15 Years On. J. Rheumatol. 2019, 46, 1388–1393. [Google Scholar] [CrossRef]
- Di Matteo, A.; Mankia, K.; Azukizawa, M.; Wakefield, R.J. The role of musculoskeletal ultrasound in the rheumatoid arthritis continuum. Curr. Rheumatol. Rep. 2020, 22, 41. [Google Scholar] [CrossRef]
- Quesada-Masachs, E.; Lopez-Corbeto, M.; Moreno-Ruzafa, E. Ultrasound in pediatric rheumatology: Highlighting the differences with adults. Eur. J. Rheumatol. 2022, 11, S348–S357. [Google Scholar] [CrossRef]
- Al-Saadany, H.M.; Hussein, M.S.; Gaber, R.A.; Zaytoun, H.A. Th-17 cells and serum IL-17 in rheumatoid arthritis patients: Correlation with disease activity and severity. Egypt. Rheumatol. 2016, 38, 1–7. [Google Scholar] [CrossRef]
- Abood, A.; Sabbar, H.R. Study the Association of IL-21, IL-17, CD163, and hs-CRP with Activity of Knee Osteoarthritis Among Iraqi Patients. Egypt. Acad. J. Biol. Sci. C Physiol. Mol. Biol. 2023, 15, 713–722. [Google Scholar] [CrossRef]
- Aletaha, D.; Ward, M.M.; Machold, K.P.; Nell, V.P.K.; Stamm, T.; Smolen, J.S. Remission and active disease in rheumatoid arthritis: Defining criteria for disease activity states. Arthritis Rheum. 2005, 52, 2625–2636. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Alarcon, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Gray, R.; et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum. 1990, 33, 1601–1610. [Google Scholar] [CrossRef] [PubMed]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Campbell, J.; Haraoui, B.; Buchbinder, R.; Hobby, K.; Roth, J.H.; MacDermid, J.C. Dimensionality and clinical importance of pain and disability in hand osteoarthritis: Development of the Australian/Canadian (AUSCAN) Osteoarthritis Hand Index. Osteoarthr. Cartil. 2002, 10, 855–862. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, S240–S252. [Google Scholar]
- Aletaha, D.; Nell, V.P.; Stamm, T.; Uffmann, M.; Pflugbeil, S.; Machold, K.; Smolen, J.S. Acute phase reactants add little to composite disease activity indices for rheumatoid arthritis: Validation of a clinical activity score. Arthritis Res. Ther. 2005, 7, R796. [Google Scholar] [CrossRef]
- Martinoli, C. Musculoskeletal ultrasound: Technical guidelines. Insights Imaging 2010, 1, 99–141. [Google Scholar] [CrossRef]
- Zhang, X.; Angkasekwinai, P.; Dong, C.; Tang, H. Structure and function of interleukin-17 family cytokines. Protein Cell 2011, 2, 26–40. [Google Scholar] [CrossRef]
- Kuwabara, T.; Ishikawa, F.; Kondo, M.; Kakiuchi, T. The Role of IL-17 and Related Cytokines in Inflammatory Autoimmune Diseases. Mediators Inflamm. 2017, 2017, 3908061. [Google Scholar] [CrossRef]
- Schinocca, C.; Rizzo, C.; Fasano, S.; Grasso, G.; La Barbera, L.; Ciccia, F.; Guggino, G. Role of the IL-23/IL-17 Pathway in Rheumatic Diseases: An Overview. Front. Immunol. 2021, 12, 637829. [Google Scholar] [CrossRef]
- Kim, J.; Kang, S.; Kim, J.; Kwon, G.; Koo, S. Elevated levels of T helper 17 cells are associated with disease activity in patients with rheumatoid arthritis. Ann. Lab. Med. 2013, 33, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Al-Zifzaf, D.S.; El Bakry, S.A.; Mamdouh, R.; Shawarby, L.A.; Ghaffar, A.Y.A.; Amer, H.A.; Alim, A.A.; Sakr, H.M.; Rahman, R.A. FoxP3+T regulatory cells in Rheumatoid arthritis and the imbalance of the Treg/TH17 cytokine axis. Egypt. Rheumatol. 2015, 37, 7–15. [Google Scholar] [CrossRef]
- Hussein, M.R.; Fathi, N.A.; El-Din, A.M.E.; Hassan, H.I.; Abdullah, F.; AL-Hakeem, E.; Backer, E.A. Alterations of the CD4+, CD8+ T Cell Subsets, Interleukins-1β, IL-10, IL-17, Tumor Necrosis Factor-α and Soluble Intercellular Adhesion Molecule-1 in Rheumatoid Arthritis and Osteoarthritis: Preliminary Observations. Pathol. Oncol. Res. 2008, 14, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Samaan, S.F.; Taha, S.I.; Mahmoud, F.A.; Elsaadawy, Y.; Khalil, S.A.; Gamal, D.M. Role of Interleukin-17 in Predicting Activity of Rheumatoid Arthritis and Systemic Lupus Erythematosus. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2024, 17, 11795441241276880. [Google Scholar] [CrossRef]
- Mohamed, S.A.; Neseem, N.O.; Metwally, S.S.; Dein M Farag, S.E. IL-17 in primary knee osteoarthritis and its relation with severity of the disease. Int. J. Clin. Rheumatol. 2018, 13, hcae175.981. [Google Scholar] [CrossRef]
- Miller, R.E.; Miller, R.J.; Malfait, A.-M. Osteoarthritis joint pain: The cytokine connection. Cytokine 2014, 70, 185–193. [Google Scholar] [CrossRef]
- Mathiessen, A.; Conaghan, P.G. Synovitis in osteoarthritis: Current understanding with therapeutic implications. Arthritis Res. Ther. 2017, 19, 18. [Google Scholar] [CrossRef]
- Torres, L.; Dunlop, D.D.; Peterfy, C.; Guermazi, A.; Prasad, P.; Hayes, K.W.; Song, J.; Cahue, S.; Chang, A.; Marshall, M.; et al. The relationship between specific tissue lesions and pain severity in persons with knee osteoarthritis. Osteoarthr. Cartil. 2006, 14, 1033–1040. [Google Scholar] [CrossRef]
- Lubberts, E. The role of IL-17 and family members in the pathogenesis of arthritis. Curr. Opin. Investig. Drugs 2003, 4, 572–577. [Google Scholar]
- Lubberts, E.; Joosten, L.A.B.; Oppers, B.; van den Bersselaar, L.; Coenen-de Roo, C.J.J.; Kolls, J.K.; Schwarzenberger, P.; van de Loo, F.A.J.; van den Berg, W.B. IL-1-Independent Role of IL-17 in Synovial Inflammation and Joint Destruction During Collagen-Induced Arthritis. J. Immunol. 2001, 167, 1004–1013. [Google Scholar] [CrossRef]
- Elhewala, A.E.I.; Soliman, S.G.; Labeeb, A.A.-A.; Mousa, W.A.; Salah, D. Interleukin-17 level in rheumatoid arthritis patients and its relation to disease activity: A clinical and ultrasound study. Egypt. Rheumatol. Rehabil. 2015, 42, 183–187. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Groups | Control | RA Group | OA Group | Test of Significance | p-Value | |
|---|---|---|---|---|---|---|
| Parameter | ||||||
| Age (years) -Mean ± SD -Range | 42.2 ± 7.82 24–53 | 45.2 ± 9.33 29–61 | 46.3 ± 7.72 24–62 | F test | 0.07 | |
| Sex -Male = n (%) -Female = n (%) | 10 (25.0) 30 (75.0) | 2 (5.0) 38 (95.0) | 12 (30.0) 28 (70.0) | χ2 test | 0.013 * | |
| IL-17 (pg/mL) -Mean ± SD -Range | 32.46 ± 20.7 8.3–75.0 | 141.37 ± 51.9 85.2–312.8 | 151.69 ± 23.11 6.3–221.5 | F test | <0.0001 * | |
| Variable | IL-17 in RA Group | IL-17 in OA Group | ||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| AUSCAN | NA | NA | 0.124 | 0.46 |
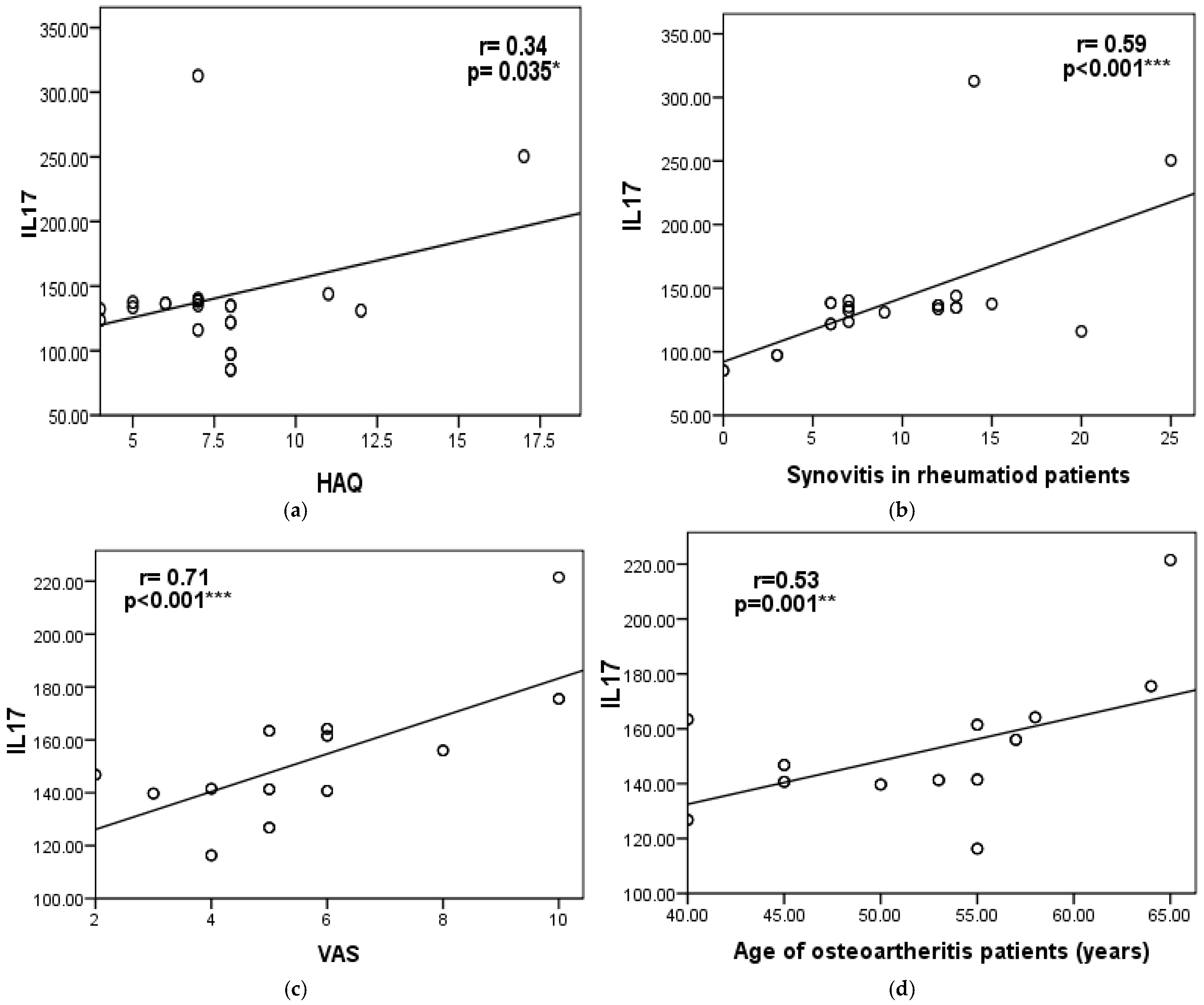
| CDAS | 0.4 | 0.02 * | NA | NA |
| Erosions | 0.25 | 0.12 | −0.23 | 0.19 |
| Effusion | 0.06 | 0.72 | −0.23 | 0.19 |
| Osteophytes | 0.006 | 0.97 | −0.34 | 0.84 |
| Disease Duration | 0.37 | 0.018 * | 0.26 | 0.13 |
| Groups | RA Group Mean ± SD | OA Group Mean ± SD | Test of Significance | p-Value | |
|---|---|---|---|---|---|
| Parameter | |||||
| IL-17 (pg/mL) | 141.37 ± 51.09 | 151.69 ± 23.13 | t test | 0.26 | |
| VAS | 5.12 ± 1.79 | 5.7 ± 2.29 | t test | 0.21 | |
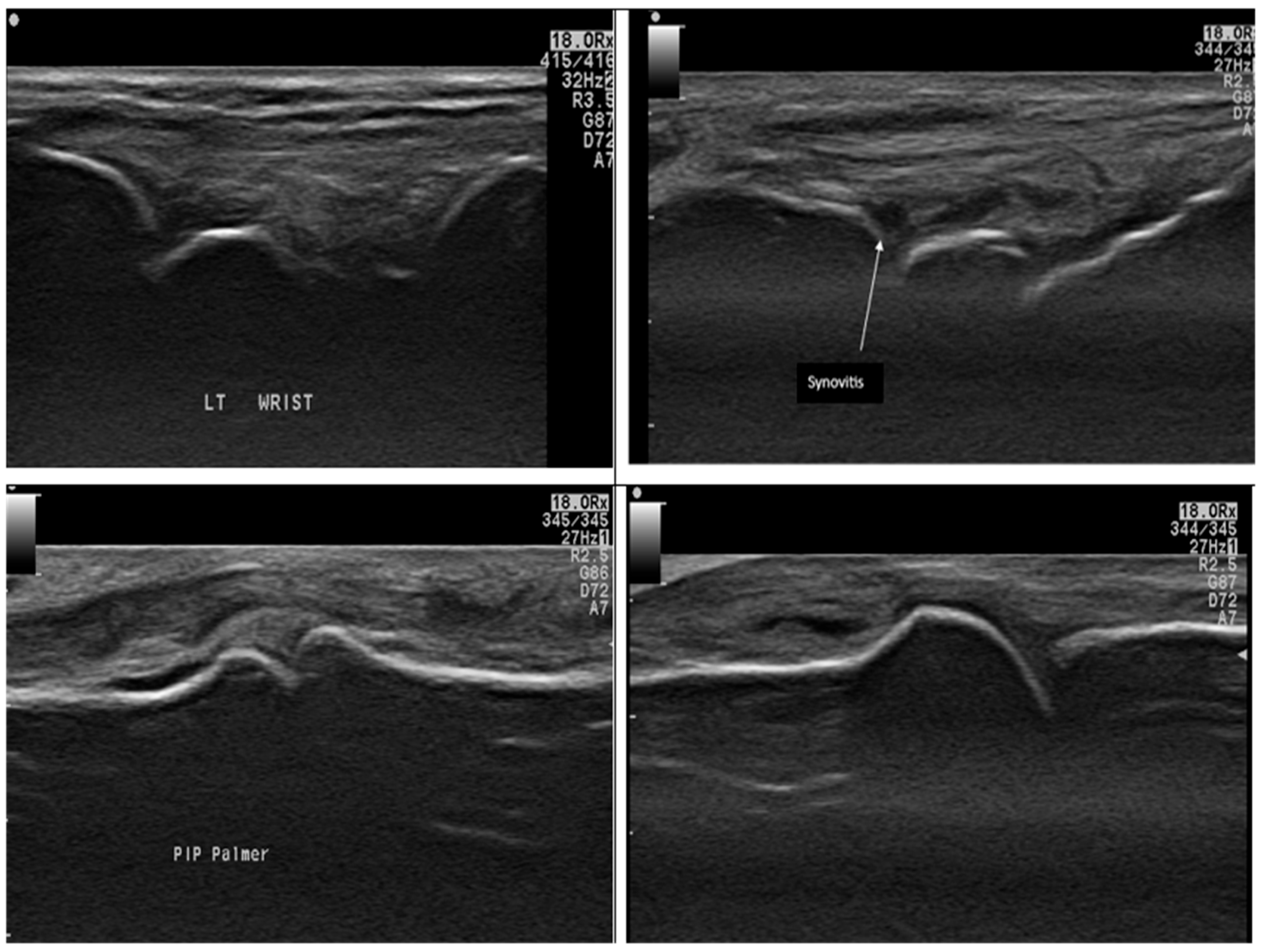
| Synovitis | 9.8 ± 6.02 | 5.18 ± 2.37 | t test | <0.0001 * | |
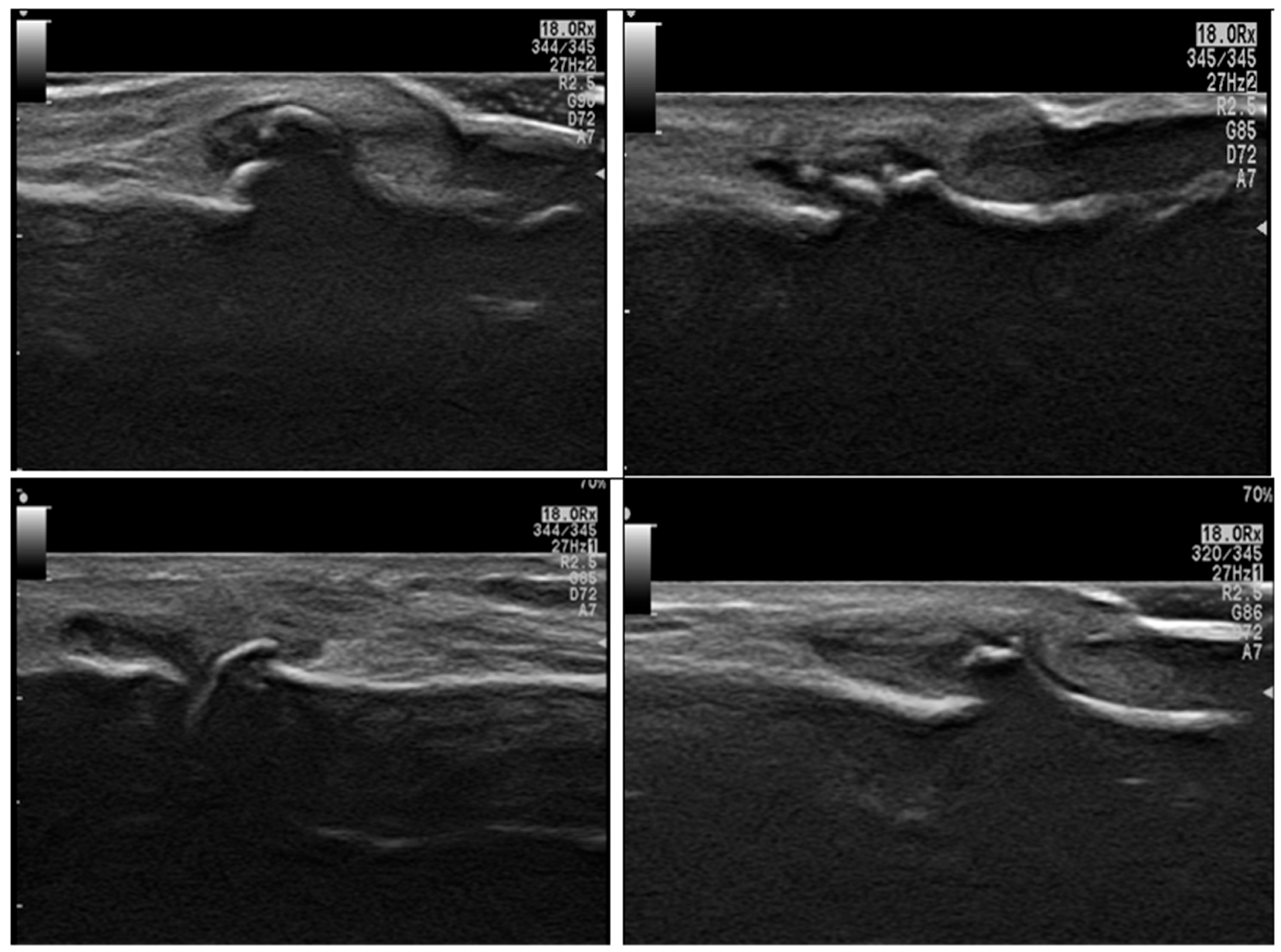
| Erosions | 1.42 ± 0.16 | 1.57 ± 0.37 | t test | <0.0001 * | |
| Effusion | 1.24 ± 1.82 | 1.24 ± 2.61 | MW | 0.25 | |
| Osteophytes | 6.58 ± 5.79 | 11.78 ± 6.68 | MW | <0.0001 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebaid, A.M.; Atwa, E.; Mortada, M.A.; Bahri, H.A.; Almadani, N.; Hammad, N.M. Serum Interleukin-17 and Its Association with Inflammation and Bone Remodeling in Rheumatoid Arthritis and Hand Osteoarthritis: Insights from Musculoskeletal Ultrasound. Diagnostics 2025, 15, 1335. https://doi.org/10.3390/diagnostics15111335
Ebaid AM, Atwa E, Mortada MA, Bahri HA, Almadani N, Hammad NM. Serum Interleukin-17 and Its Association with Inflammation and Bone Remodeling in Rheumatoid Arthritis and Hand Osteoarthritis: Insights from Musculoskeletal Ultrasound. Diagnostics. 2025; 15(11):1335. https://doi.org/10.3390/diagnostics15111335
Chicago/Turabian StyleEbaid, Amany M., Essam Atwa, Mohamed A. Mortada, Hibah Abdulrahim Bahri, Noura Almadani, and Noha M. Hammad. 2025. "Serum Interleukin-17 and Its Association with Inflammation and Bone Remodeling in Rheumatoid Arthritis and Hand Osteoarthritis: Insights from Musculoskeletal Ultrasound" Diagnostics 15, no. 11: 1335. https://doi.org/10.3390/diagnostics15111335
APA StyleEbaid, A. M., Atwa, E., Mortada, M. A., Bahri, H. A., Almadani, N., & Hammad, N. M. (2025). Serum Interleukin-17 and Its Association with Inflammation and Bone Remodeling in Rheumatoid Arthritis and Hand Osteoarthritis: Insights from Musculoskeletal Ultrasound. Diagnostics, 15(11), 1335. https://doi.org/10.3390/diagnostics15111335