


Radioactive Seed Localization for Nonpalpable Breast Lesions: Systematic Review and Meta-Analysis
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Methods to Identify and Select Studies
- Databases: The searches were performed in the following databases: Embase, LILACS, PubMed, SciELO, Web of Science, and clinicaltrials.gov. In addition, a manual search was performed in reference lists. Studies published in languages other than English, Portuguese, and Spanish were excluded. The search was performed to include studies published during the researched period. The search was performed again before the final analysis to include possible recent eligible studies.
- Search strategy: The identification scope of relevant studies was as wide as possible according to the inclusion criteria. Based on this, the search strategy was to write with controlled and free vocabulary, respecting the syntax of each database. Exclusion filters, including the publication year, were not used. The database search strategy can be found in the Supporting Information.
- Outcomes: Positive surgical margins, intraoperative re-excision, reoperation, recurrence, failed identification of SLNB, specimen volume, complications, patient assessment of intervention, medical team assessment of intervention, localization time, operative time, and time between site and surgery.
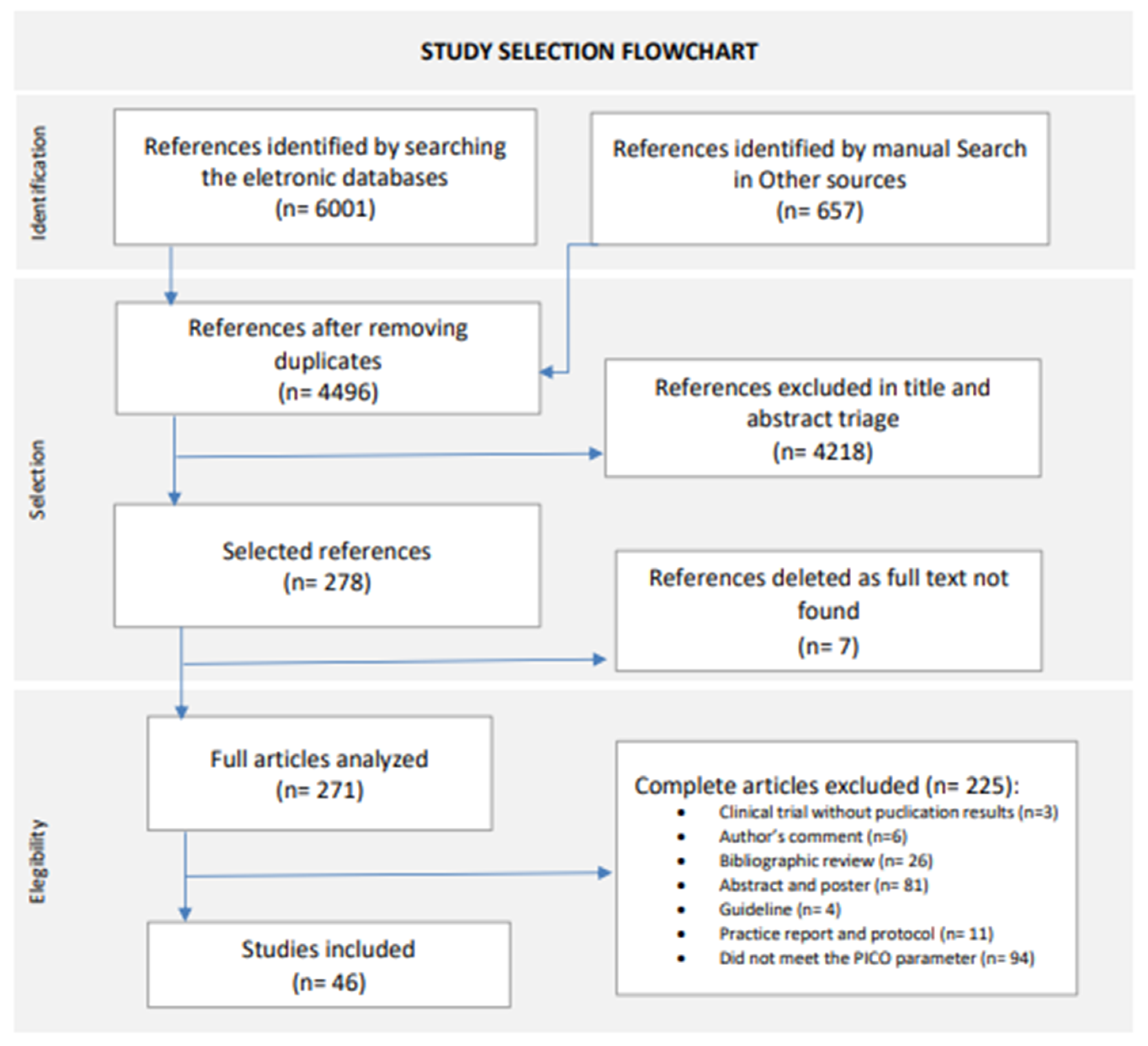
- Two-step triage: Studies identified through the search strategy were exported to Mendeley [21] for managing references and removing duplicates. The study selection was performed through a two-step triage process, performed independently by two of the authors (Ferreira, Rostelato). Any discrepancies regarding eligibility were resolved by discussion among all authors. In the first step, the triage was performed by reading the title and abstract, to select all studies that potentially met the inclusion criteria. In the second step, the full text of all studies selected in step one was analyzed to confirm eligibility or exclusion from the study. The research results, including the studies’ selection and justified exclusion, were organized in a selection flowchart, according to the guidelines presented in “Preferred Reporting Items for Systematic review and Meta-analysis Protocols” (PRISMA-P) [21].
2.2. Eligibility Criteria of Studies for Review
- PopulationInclusion: women, of any age over eighteen years old, diagnosed with a nonpalpable breast lesion, eligible for surgical intervention.Exclusion: age under 18, pregnancy, men.
- InterventionInclusion: RSL with iodine-125 for nonpalpable breast lesion conservative surgery.Exclusion: RSL for regions other than the breast.
- ComparatorInclusion: WGL and ROLL for nonpalpable breast lesion conservative surgery.Exclusion: WGL and ROLL for regions other than the breast.
- Study designInclusion: randomized clinical trial and cohort study with more than 10 patients, comparing RSL against ROLL and/or WGL.Exclusion: reviews, letters, abstracts, comments, in vitro assays
2.3. Data Analysis
- Data extraction: Data from all studies included were collected independently by two of the authors (Ferreira, Rostelato). Any discrepancies regarding the collected data were resolved by discussion among all authors. A standard form created by the authors was used in this process to collect the following data: study information (authors, title, year of publication, country, type of study); population characteristics (number of participants, age, clinical and pathological information about the lesion); methodology (assessed interventions, procedure description, assessed outcomes); results (description of results by outcome).
- Risk of bias assessment: The risk of bias assessment was performed independently by two authors (Ferreira, Rostelato). Any discrepancies regarding the critical assessment were resolved by discussion among all authors. The evaluation was performed for all included studies, using its specific tool for each study design. The risk of bias assessment results was illustrated in graphs with the most important points that could add bias to the review, using the Robvis tool [22]. Risk of bias assessment tools are structured with fixed bias domains, focusing on different aspects of study design, conduct, and reporting. Within each domain, there is a series of questions that aim to obtain information about study characteristics that are relevant to the risk of bias.
- ○
- Randomized clinical trials were evaluated according to ROB 2, which is the Cochrane risk of bias tool for randomized trials [23]. The domains evaluated with this tool are random generation and allocation; blinding of participants, professionals, and outcome evaluators; incomplete outcomes; outcome measurement; and selective outcome reporting.
- ○
- Observational studies were evaluated according to ROBINS I [24], which is the Cochrane risk of bias tool for evaluating non-randomized studies of interventions. With this tool, the domains evaluated were confusion; study participants selection; intervention classification; deviations from the intended interventions; incomplete outcomes; outcome measurement; and selective outcome reporting.
- Measures of treatment effectiveness: A combined estimate for effect size and 95% confidence interval (CI = ) was calculated by combining all studies to determine the likely beneficial therapeutic outcome between treatment approaches. Dichotomous data were measured using the relative risk (RR) for SLNB identification failure rate, complication rate, positive resection margin rate, intraoperative re-excision rate, reoperation rate, recurrence rate, and intervention evaluation by the patient. Mean difference (MD) was calculated to measure continuous data such as localization time, time between localization and surgery, operating time, and specimen volume. The relative risk (RR) or odds ratio is the ratio of the probability that an individual in the exposed group will develop the condition studied to the probability that an individual in the comparator group will develop the same condition.
- Lost data: This was an available case analysis, where data were analyzed for known cases only. To solve the missing data problem, all data were obtained whenever possible by contacting the correspondent author. In cases where data were found to be randomly lost, only existing data were analyzed. All known missing data occurrences will be presented and explored in the Section 4.
- Assessment of heterogeneity: A statistical heterogeneity test was conducted to detect any differences in effects between the studies. This was performed by reviewing the confidence intervals (CI) for each of the individual studies in the systematic review to assess overlap; and formally conducting a statistical test for heterogeneity using the I2 statistical test. An I2 greater than 50% indicates substantial heterogeneity, and above 75% considerable heterogeneity. The analyzed results were organized into forest plots using the Review Manager software, version 5.4, Cochrane Library, Hoboken, NJ, USA [25].
- Assessment of publication bias: To analyze the issue of publication bias, risk assessment forms were used to determine the level and type of risk of bias. This information was then entered into the Review Manager 5 software, where the results were summarized in funnel plots, except for outcomes that had less than 10 studies grouped together, because the test’s power is too low to determine symmetry.
- Data synthesis: The random effects model was chosen to group the data by outcome, using the Review Manager 5 software. Results were reported in forest plots presenting the effect estimate. For quantitative data that were not considered appropriate for grouping due to heterogeneity or missing data, the synthesis was performed qualitatively with a narrative description.
- Evidence quality: The evidence quality was evaluated for each of the outcomes independently according to the orientations present in the GRADE tool, which is a system for grading evidence and strength of recommendations [26]. The level of evidence represents the confidence level in estimating the effects presented in support of a particular recommendation and can be classified into four levels: high, moderate, low, and very low. The factors responsible for classifying the evidence are related to methodological quality, inconsistency, imprecision, indirect evidence, and publication bias.
3. Results
3.1. RSL and ROLL
3.1.1. Comparative Analysis by Outcome
3.1.2. Positive Surgical Margins
3.1.3. Reoperation
3.1.4. Recurrence
3.1.5. Time between Localization and Surgery
3.1.6. Risk of Bias Assessment
3.1.7. Evidence Quality Assessment
3.2. RSL and WGL
3.2.1. Comparative Analysis by Outcome
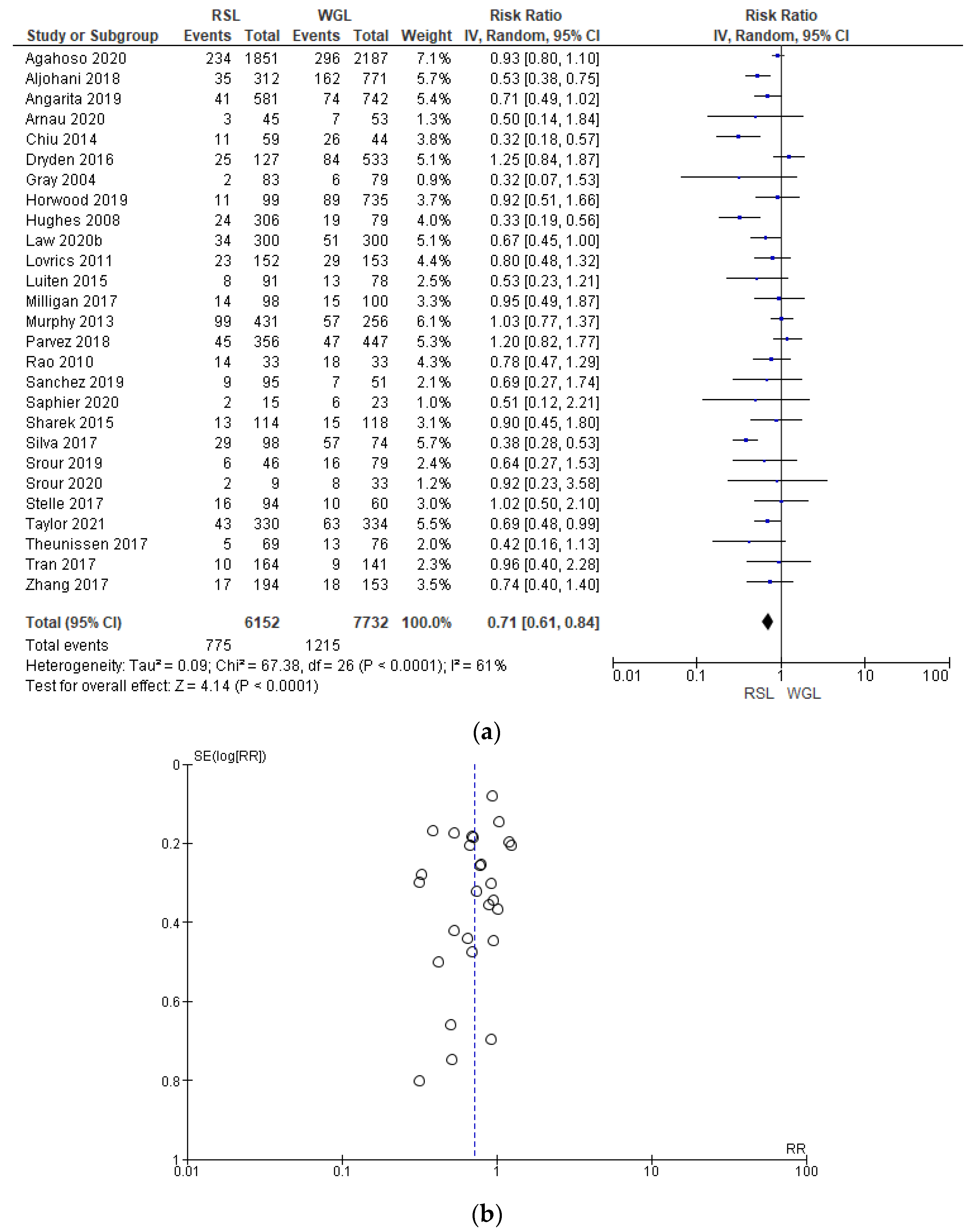
3.2.2. Positive Surgical Margins
3.2.3. Intraoperative Re-Excision
3.2.4. Reoperation
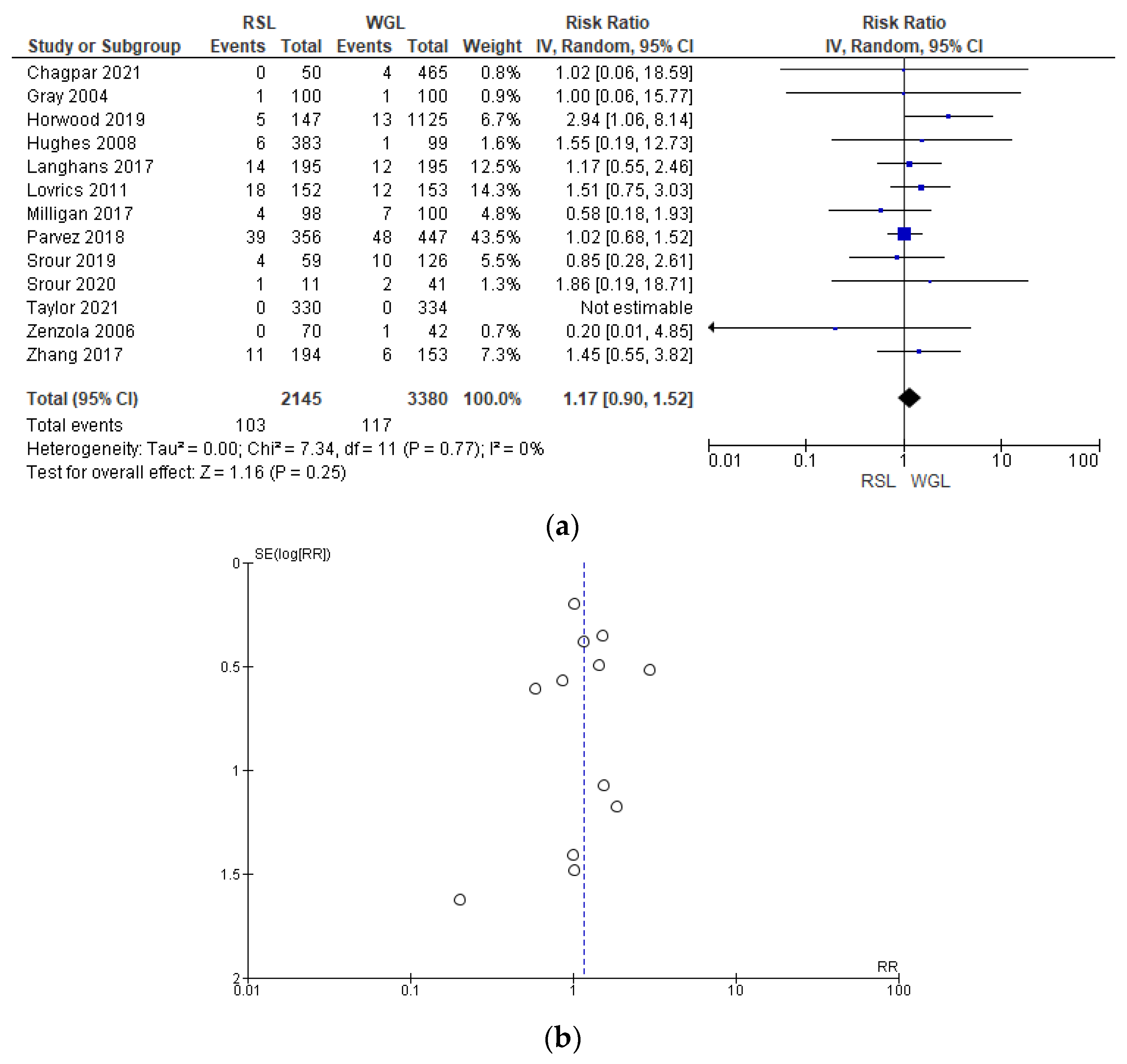
3.2.5. Recurrence
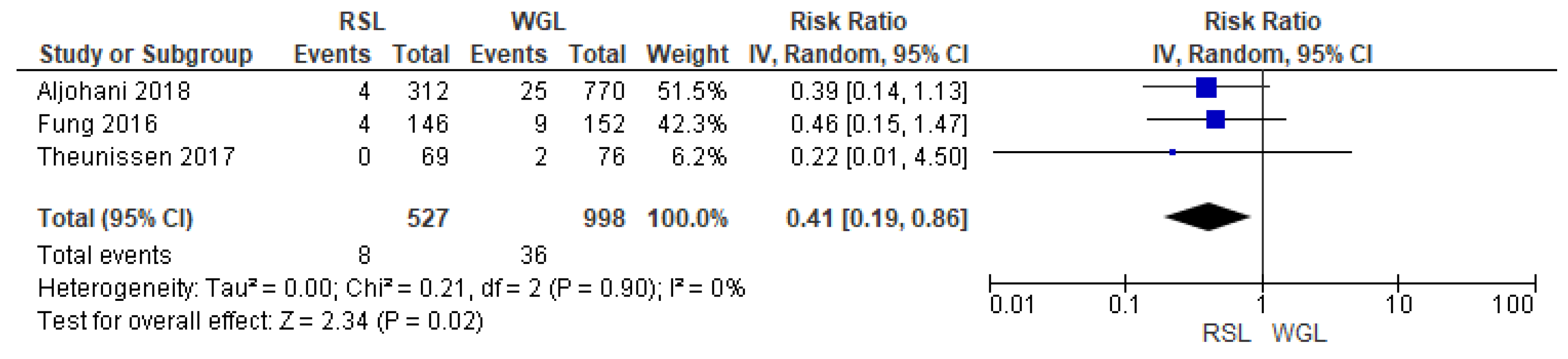
3.2.6. Sentinel Lymph Node Biopsy Failure Identification Rate
3.2.7. Complications
3.2.8. Time between Localization and Surgery
3.2.9. Risk of Bias Assessment
3.2.10. Evidence Quality Assessment
4. Discussion
4.1. Key Findings and Explanations
4.2. Strengths and Limitations
4.3. Comparison with Similar Researches
4.4. Implications and Actions Needed
4.5. Costs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, C.; Kuusk, U.; Dingee, C.; McKevitt, E. Coordination of radiological and clinical care for breast cancer diagnosis in BC. Br. Columbia Med. J. 2018, 60, 33–39. [Google Scholar]
- World Heath Organization. Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer#:~:text=In%202020%2C%20there%20were%202.3,the%20world’s%20most%20prevalent%20cancer2021 (accessed on 18 August 2022).
- Scully, O.J.; Bay, B.-H.; Yip, G.; Yu, Y. Breast Cancer Metastasis. Cancer Genom.—Proteom. 2012, 9, 311–320. [Google Scholar]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubini, E. Twenty-Year Follow-up of a Randomized Study Comparing Breast-Conserving Surgery with Radical Mastectomy for Early Breast Cancer. N. Engl. J. Med. 2002, 347, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Apantaku, L.M. Breast-conserving surgery for breast cancer. Am. Fam. Physician 2002, 66, 2271–2278. [Google Scholar]
- Xiang, J.; Huang, S.; Tuo, Y.; Wang, Y. Effect of breast-conserving surgery combined with sentinel lymph node biopsy and axillary preservation on the recurrence, metastasis, complications and cosmetic results of early breast cancer patients. Gland. Surg. 2020, 9, 1019–1025. [Google Scholar] [CrossRef]
- Weber, W.P.; Soysal, S.D.; Fulco, I.; Barandun, M.; Babst, D.; Kalbermatten, D.; Schaefer, D.J.; Oertli, D.; Kappos, E.A.; Haug, M. Standardization of oncoplastic breast conserving surgery. Eur. J. Surg. Oncol. 2017, 43, 1236–1243. [Google Scholar] [CrossRef]
- Skinner, K.A.; Silberman, H.; Sposto, R.; Silverstein, M.J. Palpable breast cancers are inherently different from nonpalpable breast cancers. Ann. Surg. Oncol. 2001, 8, 705–710. [Google Scholar] [CrossRef]
- Ahmed, M.; Douek, M. ROLL versus RSL: Toss of a coin? Breast Cancer Res. Treat. 2013, 140, 213–217. [Google Scholar] [CrossRef]
- Ernst, M.F.; Avenarius, J.K.; Schuur, K.H.; Roukema, J.A. Wire localization of non-palpable breast lesions: Out of date? Breast 2002, 11, 408–413. [Google Scholar] [CrossRef]
- National Nuclear Data Center. Brookhaven National Laboratory. NuDAT 2.7. Available online: https://www.nndc.bnl.gov/nudat2 (accessed on 10 June 2019).
- Penna, A.C.; Franca, C.A.S.; Oliveira MVFTd Fonseca LMBd Saldanha, P.d.A.B.; Costa, M.M.; Balen, J.; Rocha, A.C.P.; Pereira, F.P.A.; Andrade, V.C.; Calas, M.J.G. Uso de sementes de iodo-125 (ROLLIS) para localização intraoperatória de lesões impalpáveis da mama: Análise do implante de 338 sementes em 284 pacientes. Mastology 2017, 27, 117–123. [Google Scholar] [CrossRef]
- Bourke, A.G.; Taylor, D.B.; Westcott, E.; Hobbs, M.; Saunders, C. Iodine-125 seeds to guide removal of impalpable breast lesions: Radio-guided occult lesion localization—A pilot study. ANZ J. Surg. 2017, 87, E178–E182. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.B.; Bourke, A.G.; Westcott, E.; Burrage, J.; Latham, B.; Riley, P.; Ballal, H.; Kamyab, R.; Frost, F.; Dissanayake, D.; et al. Radioguided occult lesion localisation using iodine-125 seeds (‘ROLLIS’) for removal of impalpable breast lesions: First Australian experience. J. Med. Imaging Radiat. Oncol. 2015, 59, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Reed, A.J.; Kim, J.H.; Burrage, J.W. Development and application of a simple method for calculating breast dose from radio-guided occult lesion localisation using iodine-125 seeds (ROLLIS). Phys. Med. Biol. 2019, 64, 075020. [Google Scholar] [CrossRef]
- Dua, S.M.; Gray, R.J.; Keshtgar, M. Strategies for localisation of impalpable breast lesions. Breast 2011, 20, 246–253. [Google Scholar] [CrossRef]
- Rostelato, M.E.C.M. Estudo e Desenvolvimento de uma nova Metodologia para Confecção de Sementes de Iodo-125 para Aplicação em Braquiterapia. IPEN-CNEN/SP; Instituto de Pesquisas Energéticas e Nucleares: São Paulo, Brazil, 2006. [Google Scholar]
- Cardoso, R.M.; de Souza, C.D.; Rostelato, M.E.C.M.; Araki, K. Highly efficient method for production of radioactive silver seed cores for brachytherapy. Appl. Radiat. Isot. 2017, 120, 76–81. [Google Scholar] [CrossRef]
- van der Noordaa, M.E.; Pengel, K.E.; Groen, E.; van Werkhoven, E.; Rutgers, E.J.; Loo, C.E.; Vogel, W.; Vrancken Peeters, M.J.T.F.D. The use of radioactive iodine-125 seed localization in patients with non-palpable breast cancer: A comparison with the radioguided occult lesion localization with 99m technetium. Eur. J. Surg. Oncol. 2015, 41, 553–558. [Google Scholar] [CrossRef]
- Elsevier. Mendeley [Computer Program]. Available online: https://www.mendeley.com/2021 (accessed on 10 January 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias visualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Syn. Meth. 2020, 12, 55–61. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- The Cochrane Library. Review Manager Version 5.4 [Computer Program]. Available online: https://training.cochrane.org/online-learning/core-software/revman2020 (accessed on 5 January 2021).
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Donker, M.; Drukker, C.A.; Valdés Olmos, R.A.; Rutgers, E.J.T.T.; Loo, C.E.; Sonke, G.S.; Wesseling, J.; Alderliesten, T.; Marie-Jeanne, T.F.D.; Peeters, V. Guiding breast-conserving surgery in patients after neoadjuvant systemic therapy for breast cancer: A comparison of radioactive seed localization with the ROLL technique. Ann. Surg. Oncol. 2013, 20, 2569–2575. [Google Scholar] [CrossRef]
- Niinikoski, L.; Hukkinen, K.; Leidenius, M.H.K.; Vaara, P.; Voynov, A.; Heikkilä, P.; Mattson, J.; Meretoja, T.J. Resection margins and local recurrences of impalpable breast cancer: Comparison between radioguided occult lesion localization (ROLL) and radioactive seed localization (RSL). Breast 2019, 47, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Theunissen, C.I.J.M.; Rust, E.A.Z.; Edens, M.A.; Bandel, C.; Van’t Ooster-van den Berg, J.G.; Jager, P.L.; Noorda, E.M.; Francken, A.B. Radioactive seed localization is the preferred technique in nonpalpable breast cancer compared with wire-guided localization and radioguided occult lesion localization. Nucl. Med. Commun. 2017, 38, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Bloomquist, E.V.; Ajkay, N.; Patil, S.; Collett, A.E.; Frazier, T.G.; Barrio, A.V. A randomized prospective comparison of patient-assessed satisfaction and clinical outcomes with radioactive seed localization versus wire localization. Breast J. 2016, 22, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Chagpar, A.B.; Garcia-Cantu, C.; Howard-McNatt, M.M.; Gass, J.S.; Levine, E.A.; Chiba, A.; Lum, S.; Martinez, R.; Brown, E.; Dupont, E. Does Localization Technique Matter for Non-palpable Breast Cancers? Am. Surg. 2022, 88, 2871–2876. [Google Scholar] [CrossRef] [PubMed]
- Fung, F.; Cornacchi, S.D.; Reedijk, M.; Hodgson, N.; Goldsmith, C.H.; McCready, D.; Gohla, G.; Boylan, C.; Lovrics, P.J. Breast cancer recurrence following radioguided seed localization and standard wire localization of nonpalpable invasive and in situ breast cancers: 5-Year follow-up from a randomized controlled trial. Am. J. Surg. 2017, 213, 798–804. [Google Scholar] [CrossRef]
- Gray, R.J.; Salud, C.; Nguyen, K.; Dauway, E.; Friedland, J.; Berman, C.; Peltz, E.; Whitehead, G.; Cox, C.E. Randomized prospective evaluation of a novel technique for biopsy or lumpectomy of nonpalpable breast lesions: Radioactive seed versus wire localization. Ann. Surg. Oncol. 2001, 8, 711–715. [Google Scholar] [CrossRef]
- Langhans, L.; Tvedskov, T.F.; Klausen, T.L.; Jensen, M.-B.B.; Talman, M.-L.L.; Vejborg, I.; Benian, C.; Roslind, A.; Hermansen, J.; Oturai, P.S.; et al. Radioactive Seed Localization or Wire-guided Localization of Nonpalpable Invasive and In Situ Breast Cancer: A Randomized, Multicenter, Open-label Trial. Ann. Surg. 2017, 266, 29–35. [Google Scholar] [CrossRef]
- Lovrics, P.J.; Goldsmith, C.H.; Hodgson, N.; McCready, D.; Gohla, G.; Boylan, C.; Cornacchi, S.; Reedijk, M. A multicentered, randomized, controlled trial comparing radioguided seed localization to standard wire localization for nonpalpable, invasive and in situ breast carcinomas. Ann. Surg. Oncol. 2011, 18, 3407–3414. [Google Scholar] [CrossRef]
- Ong, J.S.L.; Teh, J.; Saunders, C.; Bourke, A.G.; Lizama, C.; Newton, J.; Phillips, M.; Taylor, D.B. Patient satisfaction with Radioguided Occult Lesion Localisation using iodine-125 seeds (‘ROLLIS’) versus conventional hookwire localisation. Eur. J. Surg. Oncol. 2017, 43, 2261–2269. [Google Scholar] [CrossRef]
- Parvez, E.; Cornacchi, S.D.; Hodgson, N.; Thoma, A.; Kong, I.; Foster, G.; Cheng, J.; Goldsmith, C.H.; Dao, D.; Lovrics, P.J. A cosmesis outcome substudy in a prospective, randomized trial comparing radioguided seed localization with standard wire localization for nonpalpable, invasive, and in situ breast carcinomas. Am. J. Surg. 2014, 208, 711–718. [Google Scholar] [CrossRef]
- Agahozo, M.C.; Berghuis, S.A.M.; van den Broek, E.; Koppert, L.B.; Obdeijn, I.-M.; van Deurzen, C.H.M. Radioactive Seed Versus Wire-Guided Localization for Ductal Carcinoma in Situ of the Breast: Comparable Resection Margins. Ann. Surg. Oncol. 2020, 27, 5296–5302. [Google Scholar] [CrossRef] [PubMed]
- Aljohani, B.; Jumaa, K.; Kornecki, A.; Brackstone, M. Clinical utility of radioactive seed localization in nonpalpable breast cancer: A retrospective single institutional cohort study. Int. J. Surg. 2018, 60, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Angarita, F.A.; Acuna, S.A.; Down, N.; Leung, C.S.; Pirmoradi, F.; Osman, F. Comparison of Radioactive Seed Localized Excision and Wire Localized Excision of Breast Lesions: A Community Hospital’s Experience. Clin. Breast Cancer 2019, 19, e364–e369. [Google Scholar] [CrossRef]
- Mendoza Arnau, I.; Sánchez Sánchez, R.; Culiáñez Casas, M.; Rebollo Aguirre, Á.C.; González Jiménez, A.D.; Martínez Meca, S. Surgical clips vs. iodine-125 (125I) seeds for marking the location of nonpalpable malignant breast lesions: Preliminary results. Radiologia 2020, 62, 38–45. [Google Scholar] [CrossRef]
- Chiu, J.C.; Ajmal, S.; Zhu, X.; Griffith, E.; Encarnacion, T.; Barr, L. Radioactive seed localization of nonpalpable breast lesions in an academic comprehensive cancer program community hospital setting. Am. Surg. 2014, 80, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Diego, E.J.; Soran, A.; McGuire, K.P.; Costellic, C.; Johnson, R.R.; Bonaventura, M.; Ahrendt, G.M.; McAuliffe, P.F. Localizing High-Risk Lesions for Excisional Breast Biopsy: A Comparison Between Radioactive Seed Localization and Wire Localization. Ann. Surg. Oncol. 2014, 21, 3268–3272. [Google Scholar] [CrossRef]
- Dryden, M.J.; Dogan, B.E.; Fox, P.; Wang, C.; Black, D.M.; Hunt, K.; Yang, W.T. Imaging factors that influence surgical margins after preoperative 125I radioactive seed localization of breast lesions: Comparison with wire localization. Am. J. Roentgenol. 2016, 206, 1112–1118. [Google Scholar] [CrossRef]
- Gray, R.J.; Pockaj, B.A.; Karstaedt, P.J.; Roarke, M.C. Radioactive seed localization of nonpalpable breast lesions is better than wire localization. Am. J. Surg. 2004, 188, 377–380. [Google Scholar] [CrossRef]
- Horwood, C.R.; Grignol, V.; Lahey, S.; Pemmaraju, V.; Schafer, A.; Terando, A.M.; Agnese, D.M. Radioactive seed vs wire localization for nonpalpable breast lesions: A single institution review. Breast J. 2019, 25, 282–285. [Google Scholar] [CrossRef]
- Hout, B.A.; Schenk, K.E.; van der Linden, A.N.; Roumen, R.M.H. Efficacy of localization of non-palpable, invasive breast cancer: Wire localization vs. Iodine-125 seed: A historical comparison. Breast 2016, 29, 8–13. [Google Scholar]
- Hughes, J.H.; Mason, M.C.; Gray, R.J.; McLaughlin, S.A.; Degnim, A.C.; Fulmer, J.T.; Pockaj, B.A.; Karstaedt, P.J.; Roarke, M.C. A multi-site validation trial of radioactive seed localization as an alternative to wire localization. Breast J. 2008, 14, 153–157. [Google Scholar] [CrossRef]
- Jumaa, K.; Johani, B.A.; Brackstone, M.; Kornecki, A. A Single-Institute Experience with Radioactive Seed Localization of Breast Lesions-A Retrospective Study. Can. Assoc. Radiol. J. J. L’association Can. Des Radiol. 2020, 71, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Law, W.; Cao, X.; Wright, F.C.; Slodkowska, E.; Look Hong, N.; Curpen, B. Adequacy of invasive and in situ breast carcinoma margins in radioactive seed and wire-guided localization lumpectomies. Breast J. 2021, 27, 134–140. [Google Scholar] [CrossRef]
- Luiten, J.D.; Beek, M.A.; Voogd, A.C.; Gobardhan, P.D.; Luiten, E.J.T. Iodine seed versus wire-guided localization in breast-conserving surgery for non-palpable ductal carcinoma in situ. Br. J. Surg. 2015, 102, 1665–1669. [Google Scholar] [CrossRef]
- Milligan, R.; Pieri, A.; Critchley, A.; Peace, R.; Lennard, T.; O’Donoghue, J.M.; Howitt, R.; Nicholson, S.; Cain, H.; Petrides, G.; et al. Radioactive seed localization compared with wire-guided localization of non-palpable breast carcinoma in breast conservation surgery- the first experience in the United Kingdom. Br. J. Radiol. 2018, 91, 20170268. [Google Scholar] [CrossRef]
- Murphy, J.O.; Moo, T.-A.A.; King, T.A.; Van Zee, K.J.; Villegas, K.A.; Stempel, M.; Eaton, A.; St. Germain, J.M.; Morris, E.; Morrow, M. Radioactive seed localization compared to wire localization in breast-conserving surgery: Initial 6-month experience. Ann. Surg. Oncol. 2013, 20, 4121–4127. [Google Scholar] [CrossRef]
- Murphy, B.L.; Boughey, J.C.; Keeney, M.G.; Glasgow, A.E.; Racz, J.M.; Keeney, G.L.; Habermann, E.B. Factors Associated with Positive Margins in Women Undergoing Breast Conservation Surgery. Mayo Clin. Proc. 2018, 93, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Parvez, E.; Cornacchi, S.D.; Fu, E.; Hodgson, N.; Farrokhyar, F.; Reid, S.; Lovrics, P.J. Adoption and outcomes of radioguided seed localization for non-palpable invasive and in-situ breast cancer at three academic tertiary care centers. Am. J. Surg. 2018, 216, 1160–1165. [Google Scholar] [CrossRef]
- Pieri, A.; Milligan, R.; Critchley, A.; O’Donoghue, J.M.; Sibal, N.; Peace, R.; Petrides, G.; Howitt, R.; Nicholson, S.; Cain, H. The introduction of radioactive seed localisation improves the oncological outcome of image guided breast conservation surgery. Breast 2017, 36, 49–53. [Google Scholar] [CrossRef]
- Rao, R.; Moldrem, A.; Sarode, V.; White, J.; Amen, M.; Rao, M.; Andrews, V.; Euhus, D.; Radford, L.; Ulissey, M. Experience with seed localization for nonpalpable breast lesions in a public health care system. Ann. Surg. Oncol. 2010, 17, 3241–3246. [Google Scholar] [CrossRef]
- Rarick, J.; Kimler, B.F.; Tawfik, O. Comparison of margin status and lesional size between radioactive seed localized vs conventional wire localized breast lumpectomy specimens. Ann. Diagn. Pathol. 2016, 21, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Romanoff, A.; Schmidt, H.; McMurray, M.; Burnett, A.; Condren, A.; Port, E. Physician preference and patient satisfaction with radioactive seed versus wire localization. J. Surg. Res. 2017, 210, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Sanchez, R.; Gonzalez Jimenez, A.D.; Rebollo Aguirre, A.C.; Mendoza Arnau, I.; Menjon Beltran, S.; Vergara Alcaide, M.E.; Osorio Ceballos, J.L.; Llamas Elvira, J.M. I-125 radioactive seed localization for non-palpable lesions in breast cancer. Rev. Esp. Med. Nucl. E Imagen Mol. 2019, 38, 343–347. [Google Scholar]
- Saphier, N.; Kondraciuk, J.; Morris, E.; Bernard-Davila, B.; Mango, V. Preoperative Localization of Breast MRI Lesions: MRI-guided Marker Placement with Radioactive Seed Localization as an Alternative to MRI-guided Wire Localization. J. Breast Imaging 2020, 2, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Sharek, D.; Zuley, M.L.; Zhang, J.Y.; Soran, A.; Ahrendt, G.M.; Ganott, M.A. Radioactive seed localization versus wire localization for lumpectomies: A comparison of outcomes. AJR Am. J. Roentgenol. 2015, 204, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, M.; Porembka, J.; Mokdad, A.A.; Seiler, S.; Huth, J.; Rivers, A.; Wooldridge, R.; Chu, A.; Brown, E.; Bao, J.; et al. Bracketed radioactive seed localization vs bracketed wire-localization in breast surgery. Breast J. 2018, 24, 161–166. [Google Scholar] [CrossRef]
- Srour, M.K.; Kim, S.; Amersi, F.; Giuliano, A.E.; Chung, A. Comparison of wire localization, radioactive seed, and Savi scout(®) radar for management of surgical breast disease. Breast J. 2020, 26, 406–413. [Google Scholar] [CrossRef]
- Srour, M.K.; Kim, S.; Amersi, F.; Giuliano, A.E.; Chung, A. Comparison of Multiple Wire, Radioactive Seed, and Savi Scout(®) Radar Localizations for Management of Surgical Breast Disease. Ann. Surg. Oncol. 2020, 28, 2212–2218. [Google Scholar] [CrossRef]
- Stelle, L.; Schoenheit, T.; Brubaker, A.; Tang, X.; Qu, P.; Cradock, K.; Higham, A. Radioactive Seed Localization Versus Wire Localization for Nonpalpable Breast Lesions: A Two-Year Initial Experience at a Large Community Hospital. Ann. Surg. Oncol. 2018, 25, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Tran, V.T.; David, J.; Patocskai, E.; Zummo-Soucy, M.; Younan, R.; Lalonde, L.; Labelle, M.; El Khoury, M.; Robidoux, A.; Trop, I. Comparative Evaluation of Iodine-125 Radioactive Seed Localization and Wire Localization for Resection of Breast Lesions. Can. Assoc. Radiol. J. J. L’association Can. Des Radiol. 2017, 68, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Zénzola, V.; Hidalgo, F.; Paredtes, R.; Betancourt, L.; Mattar, D.; Andrade, A. Estudio comparativo entre radiolocalización con aguja arpón: Y uso de semillas radioactivas de yodo 125 en lesiones subclínicas de mama TT—Comparative study between radiolocation with needle harpoon and use of radioactive iodine seeds in 125 subclinica. Rev. Venez. Oncol. 2006, 18, 136–143. [Google Scholar]
- Zhang, Y.; Seely, J.; Cordeiro, E.; Hefler, J.; Thavorn, K.; Mahajan, M.; Domina, S.; Aro, J.; Ibrahim, A.M.; Arnaout, A.; et al. Radioactive Seed Localization Versus Wire-Guided Localization for Nonpalpable Breast Cancer: A Cost and Operating Room Efficiency Analysis. Ann. Surg. Oncol. 2017, 24, 3567–3573. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.B.; Bourke, A.G.; Westcott, E.J.; Marinovich, M.L.; Chong, C.Y.L.; Liang, R.; Hughes, R.L.; Elder, E.; Saunders, C.M. Surgical outcomes after radioactive 125I seed versus hookwire localization of non-palpable breast cancer: A multicentre randomized clinical trial. Br. J. Surg. 2021, 108, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.K.Y.; Wiseberg-Firtell, J.A.; Jois, R.H.S.; Jensen, K.; Audisio, R.A. Localization techniques for guided surgical excision of non-palpable breast lesions. Cochrane Database Syst. Rev. 2015, 2015, CD009206. [Google Scholar]
- Moreira, I.C.; Ventura, S.R.; Ramos, I.; Fougo, J.L.; Rodrigues, P.P. Preoperative localisation techniques in breast conservative surgery: A systematic review and meta-analysis. Surg. Oncol. 2020, 35, 351–373. [Google Scholar] [CrossRef]
- Ahmed, M.; Douek, M. Radioactive seed localisation (RSL) in the treatment of non-palpable breast cancers: Systematic review and meta-analysis. Breast 2013, 22, 383–388. [Google Scholar] [CrossRef]
- Barentsz, M.W.; van den Bosch, M.A.A.J.; Veldhuis, W.B.; van Diest, P.J.; Pijnappel, R.M.; Witkamp, A.J.; Verkooijen, H.M. Radioactive seed localization for non-palpable breast cancer. Br. J. Surg. 2013, 100, 582–588. [Google Scholar] [CrossRef]
- Gray, R.J.; Pockaj, B.A.; Garvey, E.; Blair, S. Intraoperative Margin Management in Breast-Conserving Surgery: A Systematic Review of the Literature. Ann. Surg. Oncol. 2018, 25, 18–27. [Google Scholar] [CrossRef]
- Fusco, R.; Petrillo, A.; Catalano, O.; Sansone, M.; Granata, V.; Filice, S.; D’aiuto, M.; Pankhurst, Q.; Douek, M. Procedures for location of non-palpable breast lesions: A systematic review for the radiologist. Breast Cancer 2014, 21, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Pouw, B.; Veen, L.J.d.W.v.d.; Stokkel, M.P.; Loo, C.E.; Peeters, M.-J.T.V.; Olmos, R.A.V. Heading toward radioactive seed localization in non-palpable breast cancer surgery? A meta-analysis. J. Surg. Oncol. 2015, 111, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.-L.; Tsikouras, P.; Zuo, H.-Q.; Huang, M.-Q.; Peng, L.; Bothou, A.; Zervoudis, S.; Teichmann, A.T. Radioactive seed localization and wire guided localization in breast cancer: A systematic review and meta-analysis. JBUON 2019, 24, 48–60. [Google Scholar] [PubMed]
- Xu, X.J.; Li, J.J.; Bin Ji, W. An updated Meta-Analysis of radioactive seed localization versus wire-guided localization in the treatment of nonpalpable breast lesions. Breast J. 2018, 24, 673–675. [Google Scholar] [CrossRef]
- Aetna. Breast Biopsy Procedures. In Medical Clinical Policy Bulletins; Aetna: Hartford, CT, USA, 2020. [Google Scholar]
- CADTH. Preoperative Seed Placement for Breast Cancer Surgery: Clinical Effectiveness, Cost-Efectiveness, and Guidelines; CADTH: Ottawa, ON, Canada, 2019. [Google Scholar]
- INESSS. Utilization de la bille radioactive pour la localisation preoperatoire de tumeurs mammaires non palpables. In Note Informative; INESSS: Montreal, QC, Canada, 2016. [Google Scholar]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | RSL | ROLL |
|---|---|---|
| Age | 28–91 | |
| Number of participants | 724 | 826 |
| Carcinoma ductal in situ | 117 | 106 |
| Carcinoma invasive | 607 | 720 |
| Neoadjuvant chemotherapy | 71 | 83 |
| Bracketing localization | 2 | 0 |
| Unknown bracketing localization | 69 | - |
| Data | RSL | WGL |
|---|---|---|
| Number of participants | 8670 | 11,150 |
| Age 20–92 years old | 6986 | 7990 |
| Unknown age | 1684 | 3160 |
| Carcinoma ductal in situ | 2917 | 3593 |
| Carcinoma invasive | 4432 | 4481 |
| Other pathologies 1 | 1321 | 3076 |
| Neoadjuvant chemotherapy | 161 | 77 |
| Unknown neoadjuvant chemotherapy | 418 | 839 |
| Bracketing localization | 479 | 577 |
| Unknown bracketing localization | 1059 | 2579 |
| Excisional biopsy | 112 | 177 |
| Unknown excisional biopsy | 1607 | 2556 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, H.H.J.; de Souza, C.D.; Pozzo, L.; Ribeiro, M.S.; Rostelato, M.E.C.M. Radioactive Seed Localization for Nonpalpable Breast Lesions: Systematic Review and Meta-Analysis. Diagnostics 2024, 14, 441. https://doi.org/10.3390/diagnostics14040441
Ferreira HHJ, de Souza CD, Pozzo L, Ribeiro MS, Rostelato MECM. Radioactive Seed Localization for Nonpalpable Breast Lesions: Systematic Review and Meta-Analysis. Diagnostics. 2024; 14(4):441. https://doi.org/10.3390/diagnostics14040441
Chicago/Turabian StyleFerreira, Hortência H. J., Carla Daruich de Souza, Lorena Pozzo, Martha S. Ribeiro, and Maria Elisa C. M. Rostelato. 2024. "Radioactive Seed Localization for Nonpalpable Breast Lesions: Systematic Review and Meta-Analysis" Diagnostics 14, no. 4: 441. https://doi.org/10.3390/diagnostics14040441
APA StyleFerreira, H. H. J., de Souza, C. D., Pozzo, L., Ribeiro, M. S., & Rostelato, M. E. C. M. (2024). Radioactive Seed Localization for Nonpalpable Breast Lesions: Systematic Review and Meta-Analysis. Diagnostics, 14(4), 441. https://doi.org/10.3390/diagnostics14040441