
Daily Measurements from Cardiac Implantable Electronic Devices to Assess Health Status



Abstract
1. Introduction
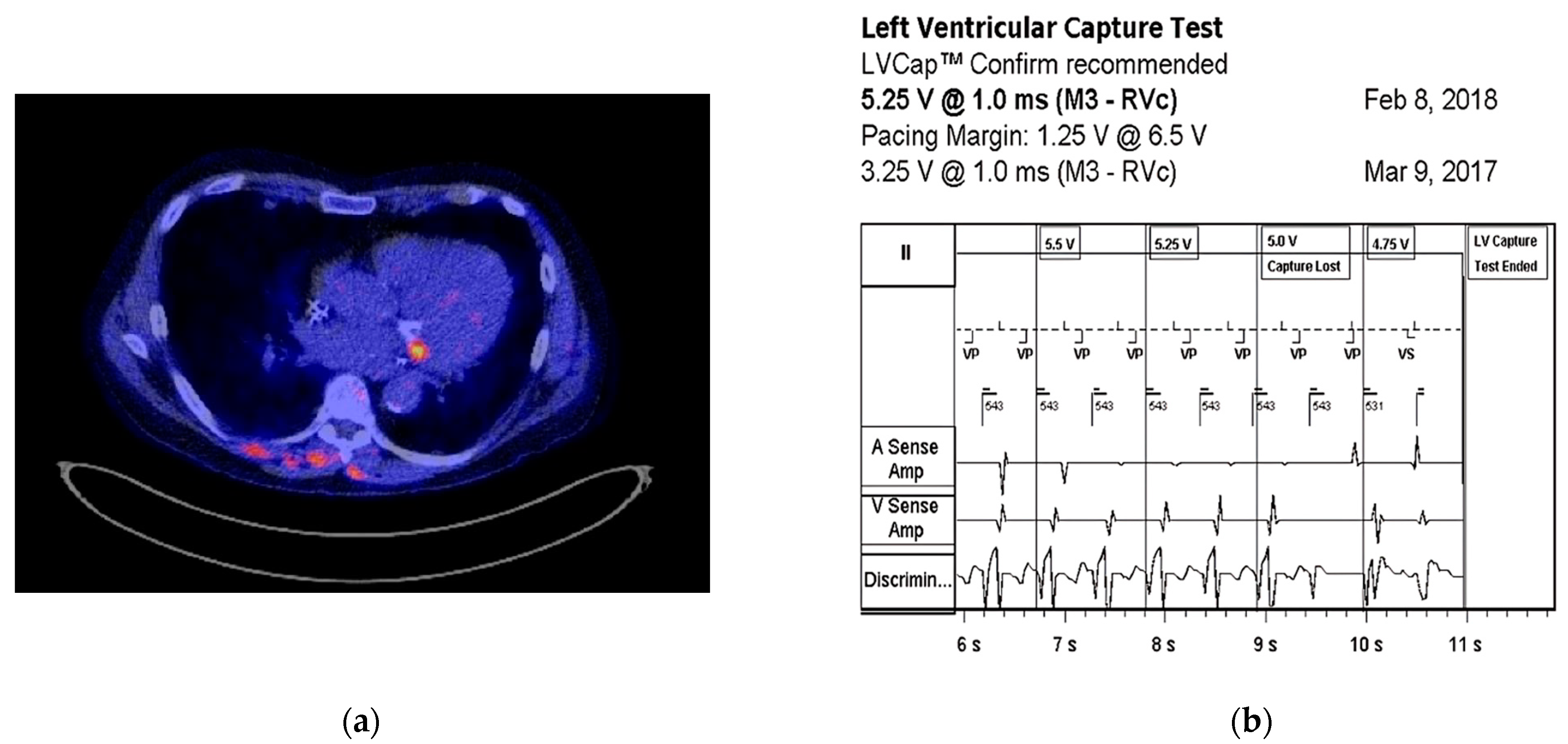
2. Pacing Threshold
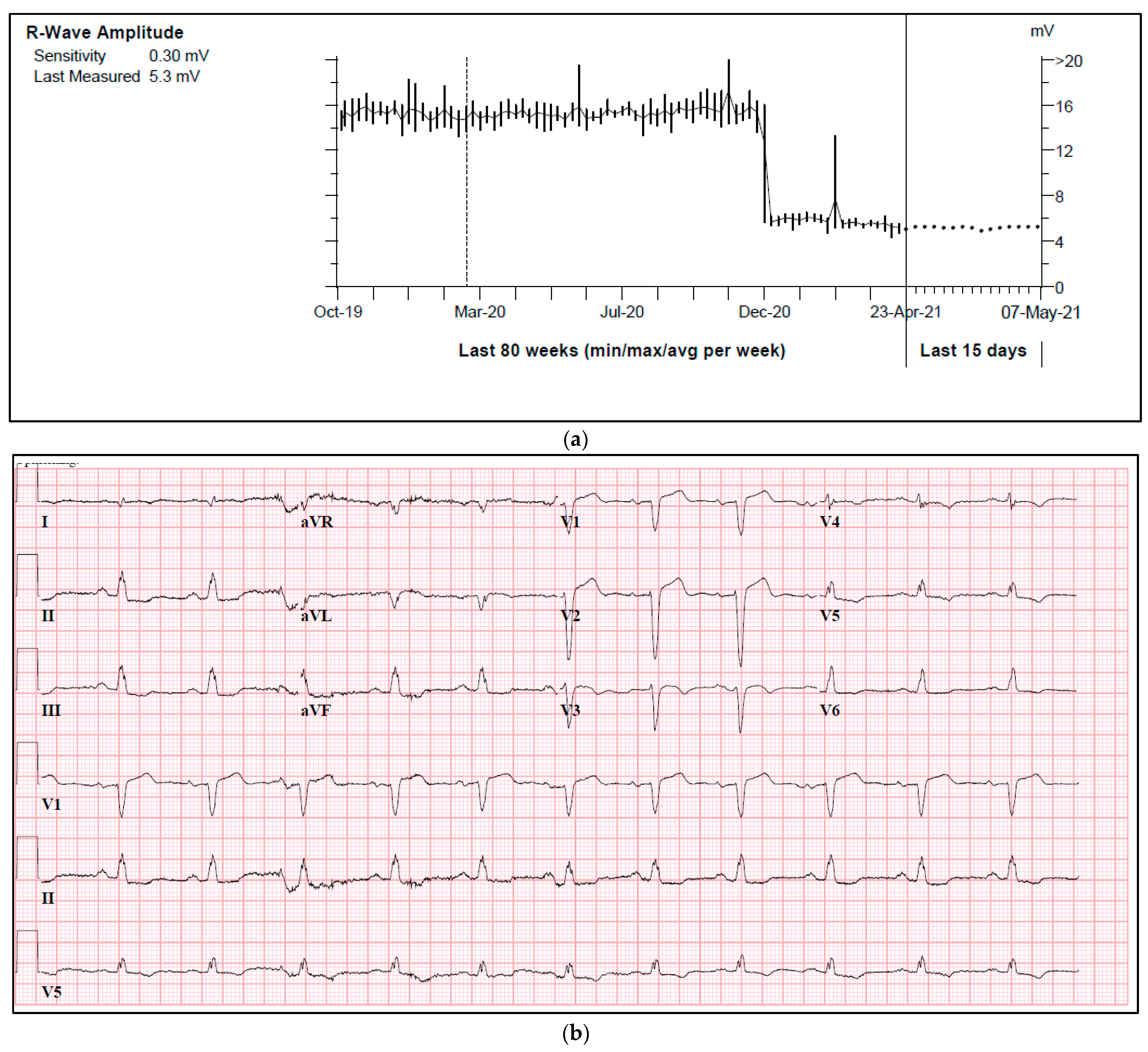
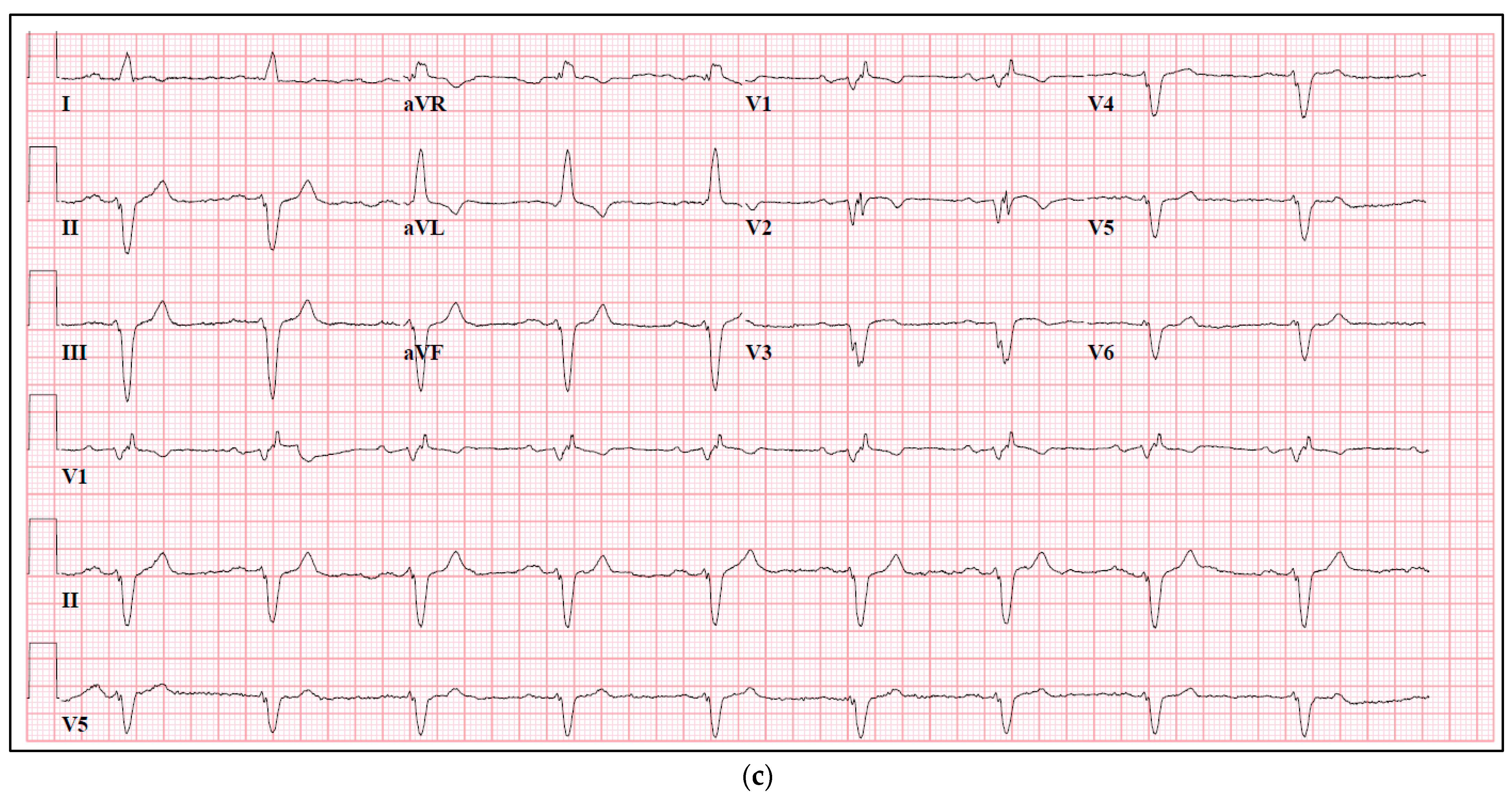
3. Intracardiac Signals
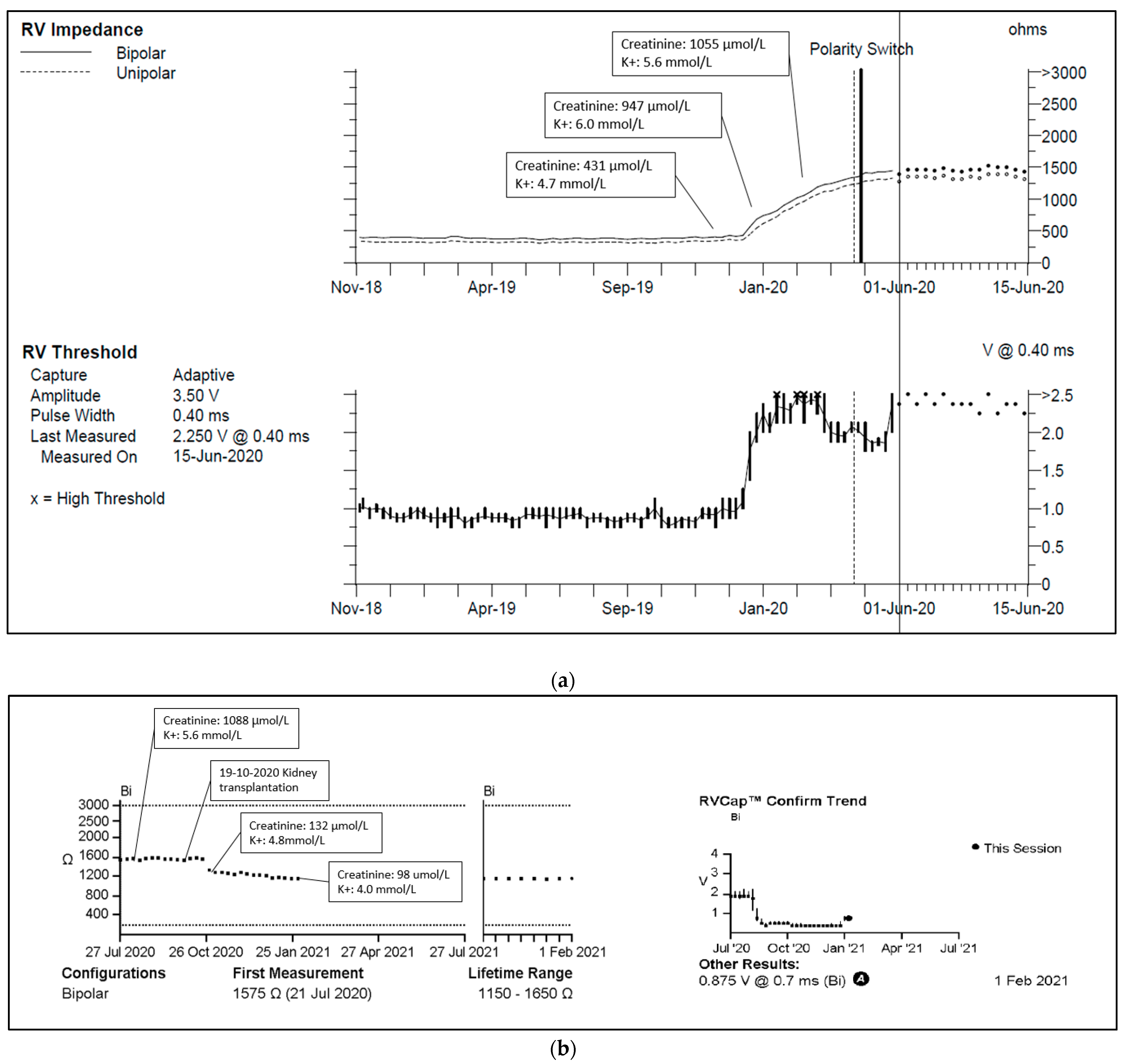
4. Pacing Impedance
5. Thoracic Impedance
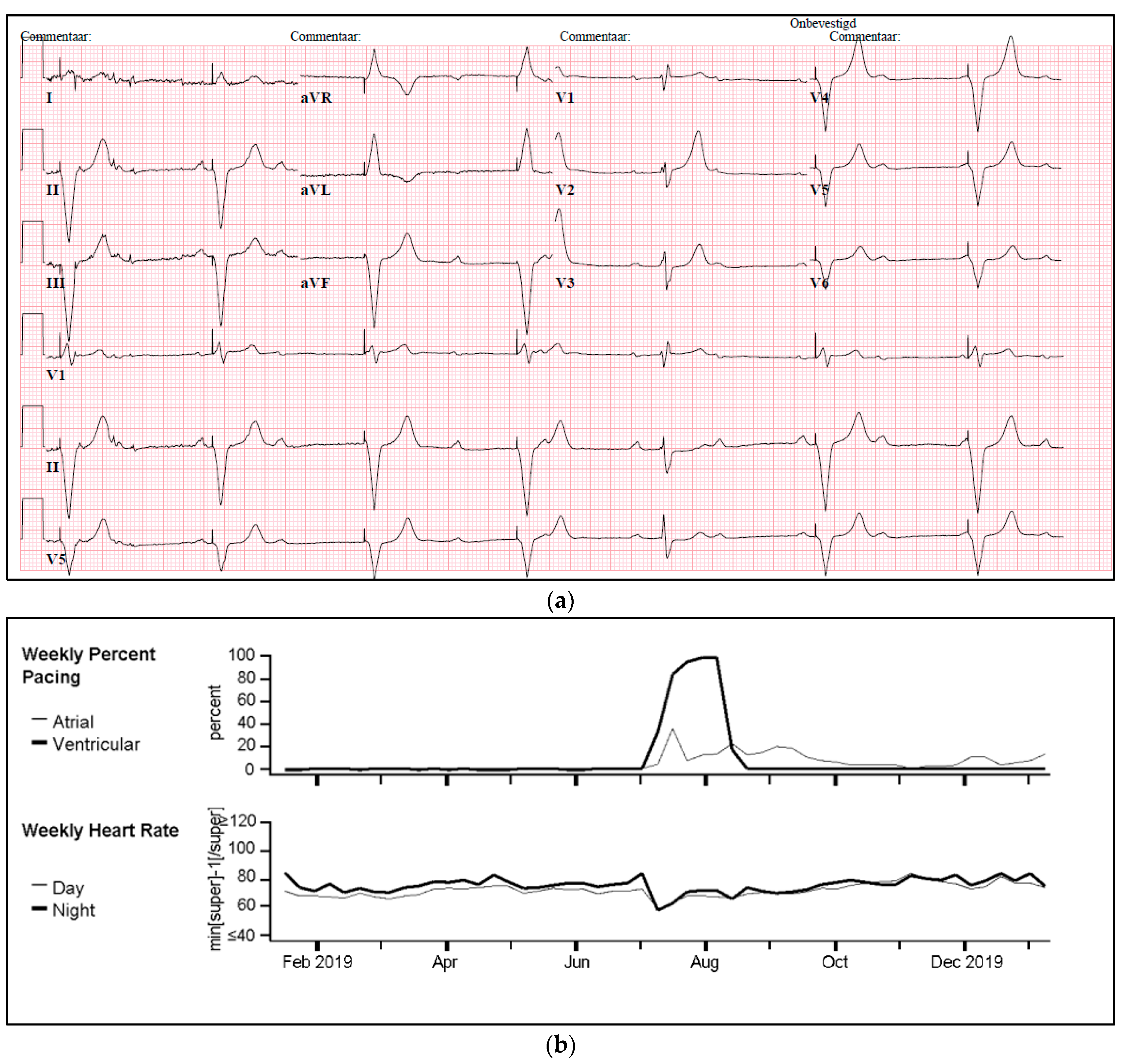
6. Pacing Percentage
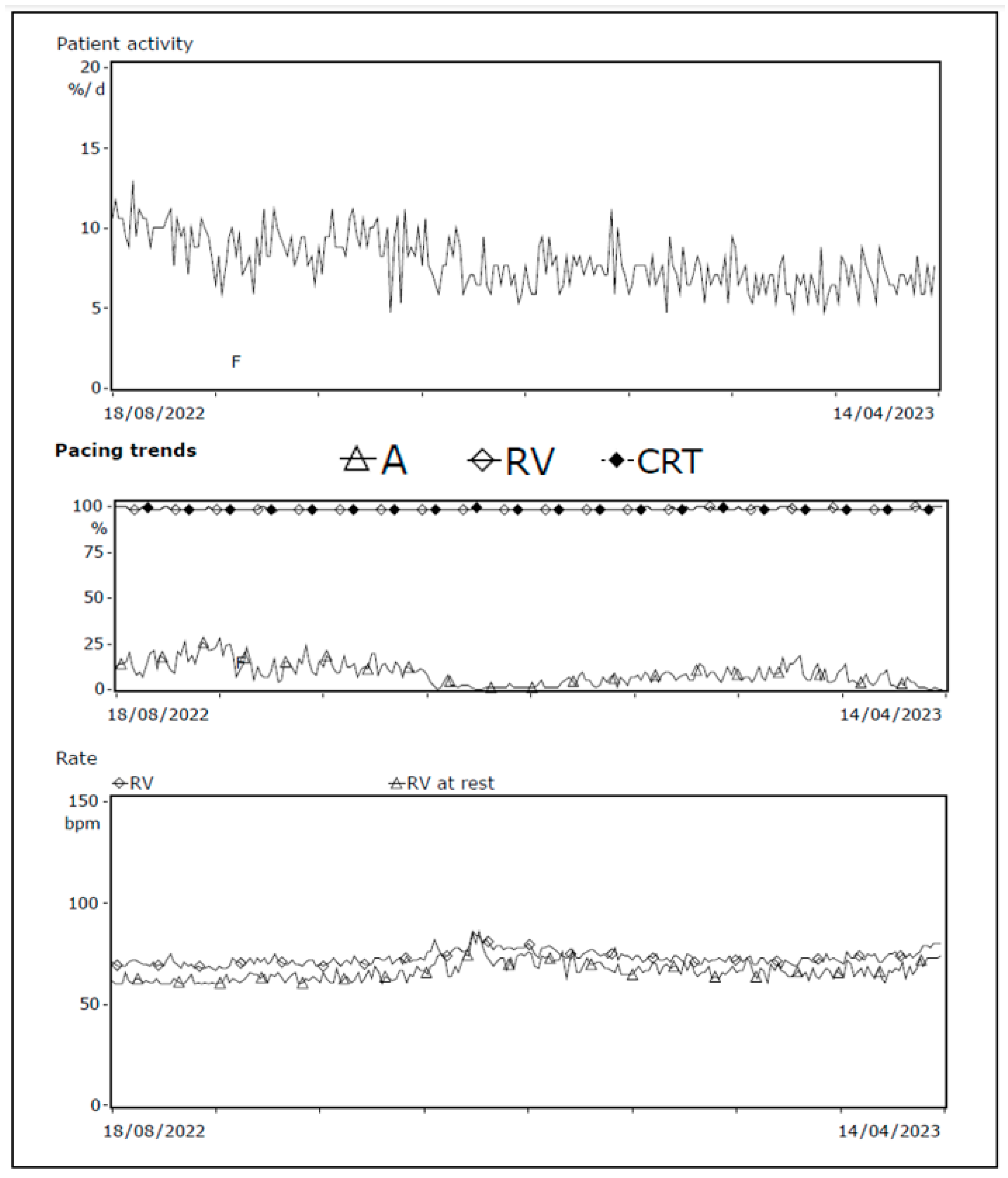
7. Patient Activity
8. Arrhythmia Episodes
9. Discussion
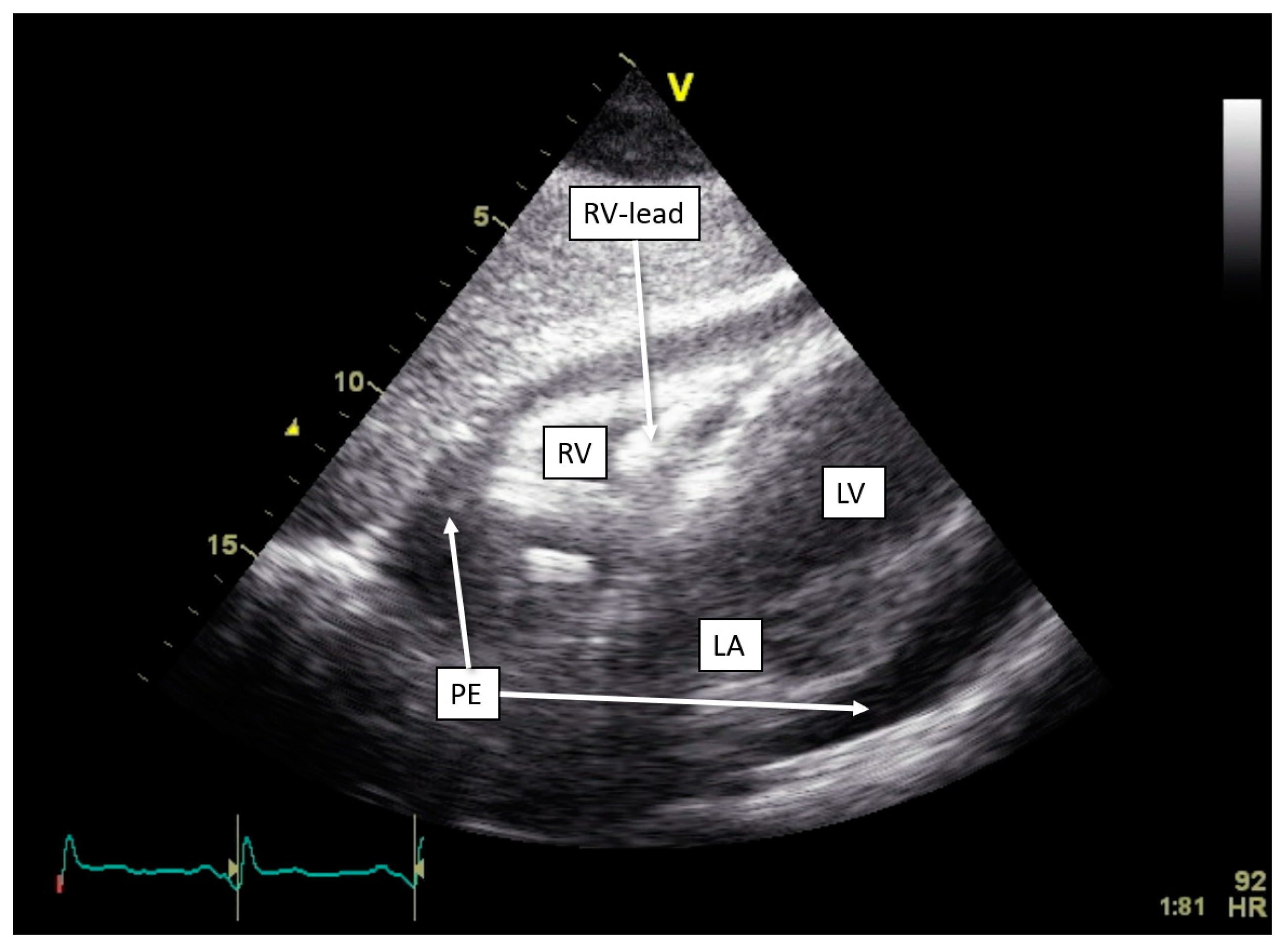
9.1. Pericardial Disease
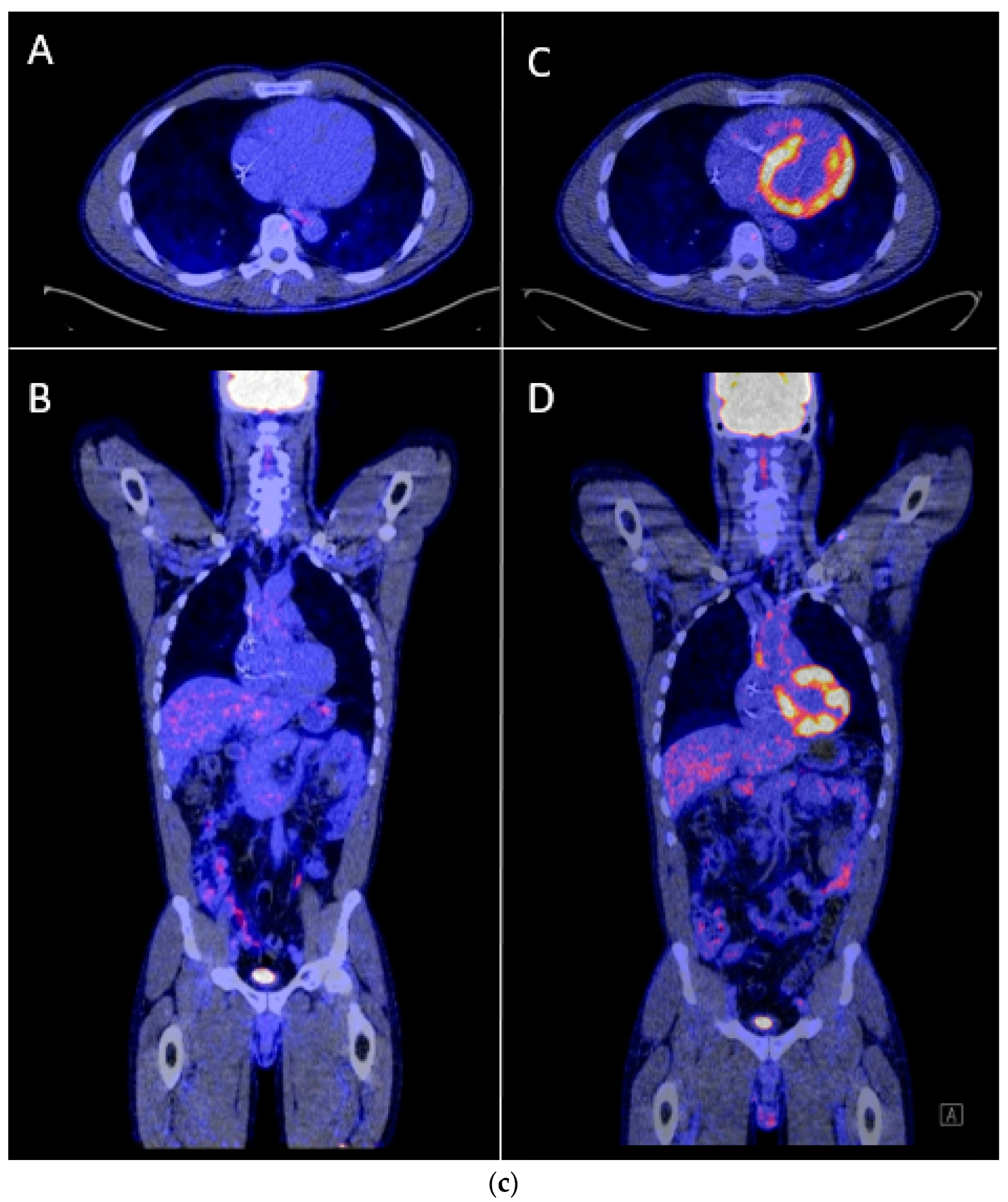
9.2. Myocardial Disease
9.3. Infectious Disease
9.4. Extracardiac Disease
10. Future Directions
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Kusumoto, F.M.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. Circulation 2019, 140, e333–e381. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Taborsky, M.; Glikson, M.; Heinrich, U.; Schumacher, B.; Katz, A.; Brachmann, J.; Lewalter, T.; Goette, A.; Block, M.; et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): A randomised controlled trial. Lancet 2014, 384, 583–590. [Google Scholar] [CrossRef]
- Scholte, N.T.B.; Gürgöze, M.T.; Aydin, D.; Theuns, D.A.M.J.; Brugts, J.J. Telemonitoring for heart failure: A meta-analysis. Eur. Heart J. 2023, 44, 2911–2926. [Google Scholar] [CrossRef] [PubMed]
- Zeppenfeld, K.; Tfelt-Hansen, J.; De Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; De Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Ferrick, A.M.; Raj, S.R.; Deneke, T.; Kojodjojo, P.; Lopez-Cabanillas, N.; Abe, H.; Boveda, S.; Chew, D.S.; Choi, J.I.; Dagres, N.; et al. 2023 HRS/EHRA/APHRS/LAHRS Expert Consensus Statement on Practical Management of the Remote Device Clinic. Europace 2023, 25, euad123. [Google Scholar] [CrossRef]
- Safavi-Naeini, P.; Saeed, M. Pacemaker troubleshooting: Common clinical scenarios. Tex. Heart Inst. J. 2016, 43, 415–418. [Google Scholar] [CrossRef]
- Swerdlow, C.D.; Koneru, J.N.; Gunderson, B.; Kroll, M.W.; Ploux, S.; Ellenbogen, K.A. Impedance in the Diagnosis of Lead Malfunction. Circ. Arrhythm. Electrophysiol. 2020, 13, E008092. [Google Scholar] [CrossRef]
- Alonso, P.; Lopez, R.; Sancho Tello, M.J.; Andres, A. Failure of ventricular capture and pacemaker exit block secondary to moderate hyperkalemia. Interv. Cardiol. 2016, 8, 591–593. [Google Scholar] [CrossRef]
- Barold, S.S.; Herweg, B. The effect of hyperkalaemia on cardiac rhythm devices. Europace 2014, 16, 467–476. [Google Scholar] [CrossRef]
- Kübler, W.; Sowton, E. Influence of beta-blockade on myocardial threshold in patients with pacemakers. Lancet 1970, 11, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Mohan, J.; Kaul, U.; Bhatia, M. Acute effects of anti-arrhythmic drugs on cardiac pacing threshold. Acta Cardiol. 1984, 39, 191–201. [Google Scholar] [PubMed]
- Varela, D.L.; Ayinapudi, K.; Ahmed, B.; Groh, C.A.; Freedman, R.A. Increasing pacemaker lead impedance and pacing threshold after initiation of chemotherapy with doxorubicin and cyclophosphamide. Hear. Case Rep. 2022, 8, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.L.; Bridge, B.; Wang, J.; Jovin, I.S. Mycobacterium fortuitum causing infection of a biventricular pacemaker/implantable cardioverter defibrillator. Int. J. Mycobacteriol. 2012, 1, 221–223. [Google Scholar] [CrossRef]
- Gao, Y.; Lan, R.F.; Zhang, N.; Wang, S.X.; Han, Z.L.; Xu, W. Aspergillus infection of pacemaker in an immunocompetent host: A case report. J. Geriatr. Cardiol. 2020, 17, 58–60. [Google Scholar] [CrossRef]
- Veldkamp, M.W.; Verkerk, A.O.; Van Ginneken, A.C.G.; Baartscheer, A.; Schumacher, C.; De Jonge, N.; De Bakker, J.M.T.; Opthof, T. Norepinephrine induces action potential prolongation and early afterdepolarizations in ventricular myocytes isolated from human end-stage failing hearts. Eur. Heart J. 2001, 22, 955–963. [Google Scholar] [CrossRef]
- Beanlands, D.; Akyurekli, Y.; Keon, W. Prednisone in the management of exit block. In Proceedings of the VIthWorld Symposium on Cardiac Pacing Vienna; Steinkopff: Dresden, Germany, 1979. [Google Scholar]
- Sagawa, Y.; Nagata, Y.; Yamaguchi, T.; Mitsui, K.; Nagamine, T.; Yamaguchi, J.; Hijikata, S.; Watanabe, K.; Masuda, R.; Miyazaki, R.; et al. Long-term performance of right ventricular implantable cardioverter-defibrillator leads in arrhythmogenic right ventricular cardiomyopathy and hypertrophic cardiomyopathy. Int. Heart J. 2020, 61, 39–45. [Google Scholar] [CrossRef]
- McVenes, R.; Hansen, N.; Lahtinen, S.P.; Stokes, K. The salty dog: Serum sodium and potassium effects on modern pacing electrodes. PACE-Pacing Clin. Electrophysiol. 2007, 30, 4–11. [Google Scholar] [CrossRef]
- Hauser, R.G.; Sengupta, J.; Casey, S.; Tang, C.; Stanberry, L.I.; Abdelhadi, R. High shocking and pacing impedances due to defibrillation lead calcification. J. Interv. Card. Electrophysiol. 2020, 58, 253–259. [Google Scholar] [CrossRef]
- Kuriachan, V.; Tedrow, U.; Antman, E.; Epstein, L.M. Acute hyperkalemia detected by alert from implantable cardioverter- defibrillator. PACE-Pacing Clin. Electrophysiol. 2012, 35, e276–e279. [Google Scholar] [CrossRef]
- Abraham, W.T.; Compton, S.; Haas, G.; Foreman, B.; Canby, R.C.; Fishel, R.; Mcrae, S.; Toledo, G.B.; Sarkar, S.; Hettrick, D.A. Intrathoracic Impedance vs. Daily Weight Monitoring for Predicting Worsening Heart Failure Events: Results of the Fluid Accumulation Status Trial (FAST). Congest. Heart Fail. 2011, 17, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Barth, C.; Kindermann, I.; Mahfoud, F.; Buob, A.; Böhm, M. Intrathoracic impedance monitoring detecting pneumonia. Clin. Res. Cardiol. 2010, 99, 333–335. [Google Scholar] [CrossRef] [PubMed]
- Diercks, D.B.; Shumaik, G.M.; Harrigan, R.A.; Brady, W.J.; Chan, T.C. Electrocardiographic manifestations: Electrolyte abnormalities. J. Emerg. Med. 2004, 27, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Ho, F.K.; Zhou, Z.; Petermann-Rocha, F.; Para-Soto, S.; Boonpor, J.; Welsh, P.; Gill, J.M.R.; Gray, S.R.; Sattar, N.; Pell, J.P.; et al. Association between Device-Measured Physical Activity and Incident Heart Failure: A Prospective Cohort Study of 94 739 UK Biobank Participants. Circulation 2022, 146, 883–891. [Google Scholar] [CrossRef]
- Hayes, D.L.; Vlietstra, R.E. Pacemaker Malfunction. Ann. Intern. Med. 1993, 119, 828–835. [Google Scholar] [CrossRef]
- Mond, H.G.; Helland, J.R.; Stokes, K.; Bornzin, G.A.; McVENES, R. The electrode-tissue interface: The revolutionary role of steroid-elution. Pacing Clin. Electrophysiol. 2014, 37, 1232–1249. [Google Scholar] [CrossRef]
- Breivik, K.; Ohm, O.-J.; Engedal, H. Long-term Comparison of Unipolar and Bipolar Pacing and Sensing, Using a New Multiprogrammable Pacemaker System. Pacing Clin. Electrophysiol. 1983, 6, 592–600. [Google Scholar] [CrossRef]
- Chatterjee, K.; Sutton, R.; Davies, J. Low intracardiac potentials in myocardial infaction as a cause of failure of inhibition of demand pacemakers. Lancet 1968, 291, 511. [Google Scholar] [CrossRef]
- Seegers, J.; Zabel, M.; Lüthje, L.; Vollmann, D. Ventricular oversensing due to manufacturer-related differences in implantable cardioverter-defibrillator signal processing and sensing lead properties. Europace 2010, 12, 1460–1466. [Google Scholar] [CrossRef]
- Verga, T.A.; Gillberg, J.M.; Greenberg, R.M.; Deger, F.T. True bipolar and integrated bipolar sensing and detection by implantable defibrillators. Pacing Clin. Electrophysiol. 2011, 34, 1561–1568. [Google Scholar] [CrossRef]
- Ellenbogen, K.A.; Gunderson, B.D.; Stromberg, K.D.; Swerdlow, C.D. Performance of lead integrity alert to assist in the clinical diagnosis of implantable cardioverter defibrillator lead failures analysis of different implantable cardioverter defibrillator leads. Circ. Arrhythmia Electrophysiol. 2013, 6, 1169–1177. [Google Scholar] [CrossRef]
- Zhang, J.; Goode, K.M.; Cuddihy, P.E.; Cleland, J.G.F. Predicting hospitalization due to worsening heart failure using daily weight measurement: Analysis of the Trans-European Network-Home-Care Management System (TEN-HMS) study. Eur. J. Heart Fail. 2009, 11, 420–427. [Google Scholar] [CrossRef] [PubMed]
- van Veldhuisen, D.J.; Braunschweig, F.; Conraads, V.; Ford, I.; Cowie, M.R.; Jondeau, G.; Kautzner, J.; Muñoz Aguilera, R.; Lunati, M.; Man Yu, C.; et al. Impedance Monitoring, Audible Patient Alerts, and Outcome in Patients with Heart Failure 2011. Circulation 2011, 124, 1719–1726. [Google Scholar] [CrossRef]
- Boehmer, J.P.; Hariharan, R.; Devecchi, F.G.; Smith, A.L.; Molon, G.; Capucci, A.; An, Q.; Averina, V.; Stolen, C.M.; Thakur, P.H.; et al. Multisensor Algorithm Predicts Heart Failure Events in Patients with Implanted Devices: Results From the MultiSENSE Study. JACC Heart Fail. 2017, 5, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.D.; Rizo-Patron, C.; Hallstrom, A.P.; O’neill, G.P.; Rothbart, S.; Martins, J.B.; Roelke, M.; Steinberg, J.S.; Greene, H.L. Percent right ventricular pacing predicts outcomes in the DAVID trial. Heart Rhythm. 2005, 2, 830–834. [Google Scholar] [CrossRef]
- Belardinelli, R.; Georgiou, D.; Cianci, G.; Purcaro, A. 10-Year Exercise Training in Chronic Heart Failure: A Randomized Controlled Trial. J. Am. Coll. Cardiol. 2012, 60, 1521–1528. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, P.; D’Aloia, A.; Gualeni, A.; Brentana, L.; Cas, L.D. The 6 minute walking test in chronic heart failure: Indications, interpretation and limitations from a review of the literature. Eur. J. Heart Fail. 2004, 6, 687–691. [Google Scholar] [CrossRef]
- Van Gelder, I.C.; Healey, J.S.; Crijns, H.J.G.M.; Wang, J. Duration of device-detected subclinical atrial fibrillation and occurrence of stroke in ASSERT. Eur. Heart J. 2017, 38, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.S.; Lopes, R.D.; Granger, C.B.; Alings, M.; Rivard, L.; McIntyre, W.F.; Atar, D.; Birnie, D.H.; Boriani, G.; Camm, A.J.; et al. Apixaban for Stroke Prevention in Subclinical Atrial Fibrillation. N. Engl. J. Med. 2024, 390, 107–117. [Google Scholar] [CrossRef]
- Kirchhof, P.; Toennis, T.; Goette, A.; Camm, A.J.; Diener, H.C.; Becher, N.; Bertaglia, E.; Lundqvist, C.B.; Borlich, M.; Brandes, A.; et al. Anticoagulation with Edoxaban in Patients with Atrial High-Rate Episodes. N. Engl. J. Med. 2023, 389, 1167–1179. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, J.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Covino, S.; Russo, V. Future perspectives and challenges of artificial intelligence implementation in remote monitoring of cardiologic implantable electronic devices. Expert Rev. Med. Devices 2024, 21, 887–888. [Google Scholar] [CrossRef] [PubMed]
- Neiman, Z.M.; Raitt, M.H.; Rohrbach, G.; Dhruva, S.S. Monitoring of Remotely Reprogrammable Implantable Loop Recorders with Algorithms to Reduce False-Positive Alerts. J. Am. Heart Assoc. 2024, 13, e032890. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurements | Reference Values | Factors Affecting Measurements and Literature References |
|---|---|---|
| Pacing threshold (V) | 0.5–2.0 V | Increase: lead dislodgment [7], fibrosis surrounding the tip [8], hypokalemia [9,10] propranolol [11], verapamil [12], quinidine [12], ajmaline [12], mexelitine [12], doxorubicin [13], cyclophosphamide [13], and CIED infection [14,15]. Decrease: epinephrine [16], norepinephrine [16], and glucocorticoids [17]. |
| Intracardiac signals (mV) | Atrial lead > 0.5 mV Ventricular lead > 2–3 mV | Decrease: fibrosis [7], arrhythmogenic cardiomyopathy [18], hyperkalemia [19], and left anterior fascicular block (this review). |
| Lead Impedance (Ohms) | 200–1000 Ohms | Increase: conductor fracture [8], calcium deposition on the tip [20], hyperkalemia, and renal failure [21]. Decrease: insulation breach [8]. |
| Thoracic impedance alert | Pulmonary edema [22], pneumonia [23], and pericardial effusion (this review). | |
| Pacing percentage | Patient specific | Increase: conduction deterioration, negative chronotropic/dromotropic drugs, hyperkalemia [24], and hypokalemia [24]. |
| Patient activity | Heart failure [25] and severe anemia (this review). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roseboom, E.; Daniëls, F.; Rienstra, M.; Maass, A.H. Daily Measurements from Cardiac Implantable Electronic Devices to Assess Health Status. Diagnostics 2024, 14, 2752. https://doi.org/10.3390/diagnostics14232752
Roseboom E, Daniëls F, Rienstra M, Maass AH. Daily Measurements from Cardiac Implantable Electronic Devices to Assess Health Status. Diagnostics. 2024; 14(23):2752. https://doi.org/10.3390/diagnostics14232752
Chicago/Turabian StyleRoseboom, Eva, Fenna Daniëls, Michiel Rienstra, and Alexander H. Maass. 2024. "Daily Measurements from Cardiac Implantable Electronic Devices to Assess Health Status" Diagnostics 14, no. 23: 2752. https://doi.org/10.3390/diagnostics14232752
APA StyleRoseboom, E., Daniëls, F., Rienstra, M., & Maass, A. H. (2024). Daily Measurements from Cardiac Implantable Electronic Devices to Assess Health Status. Diagnostics, 14(23), 2752. https://doi.org/10.3390/diagnostics14232752