
Systemic Implications of Bullous Pemphigoid: Bridging Dermatology and Internal Medicine

{kind=link}
{kind=link}
{kind=link}
Abstract
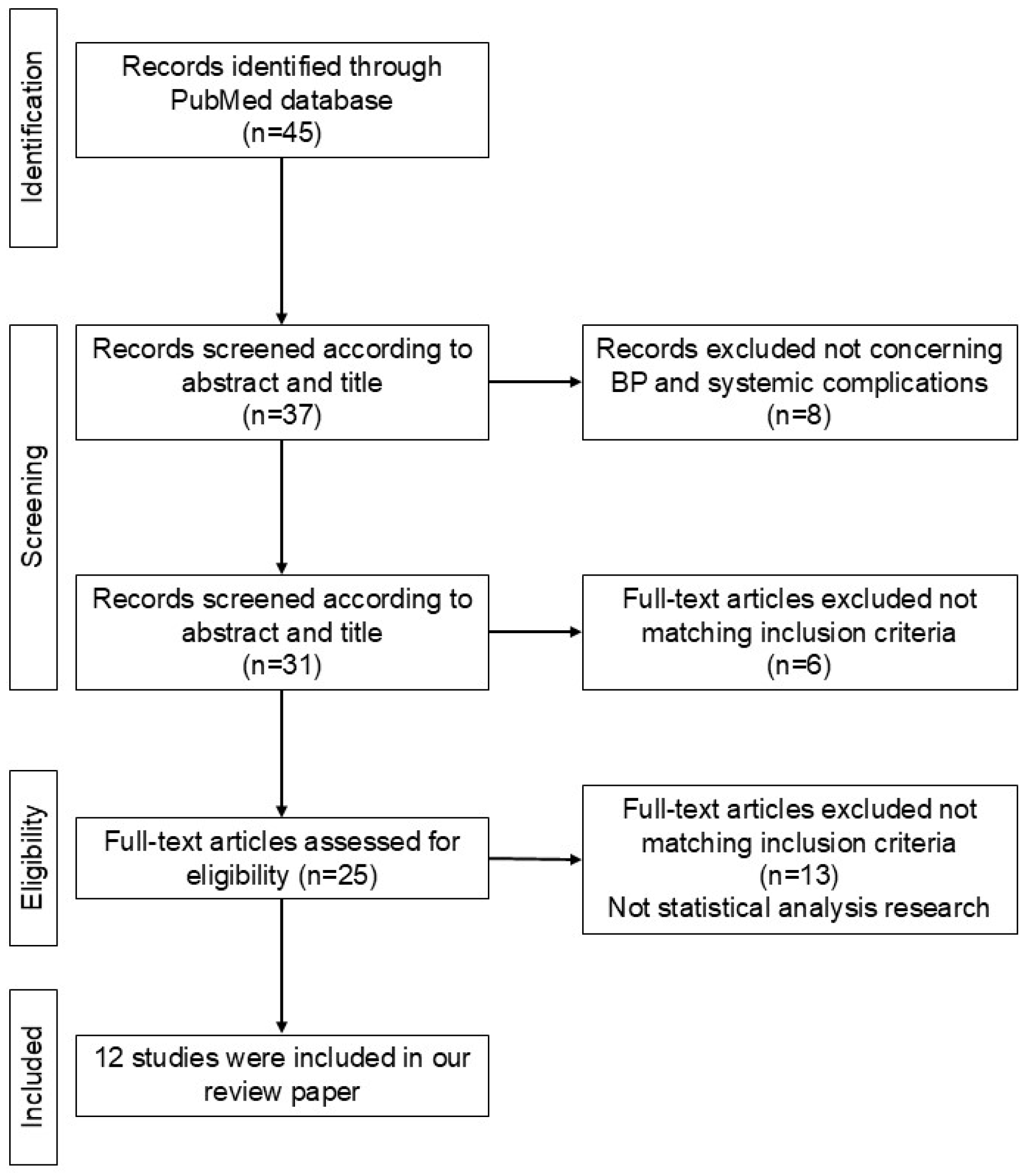
1. Introduction
2. Pathogenesis
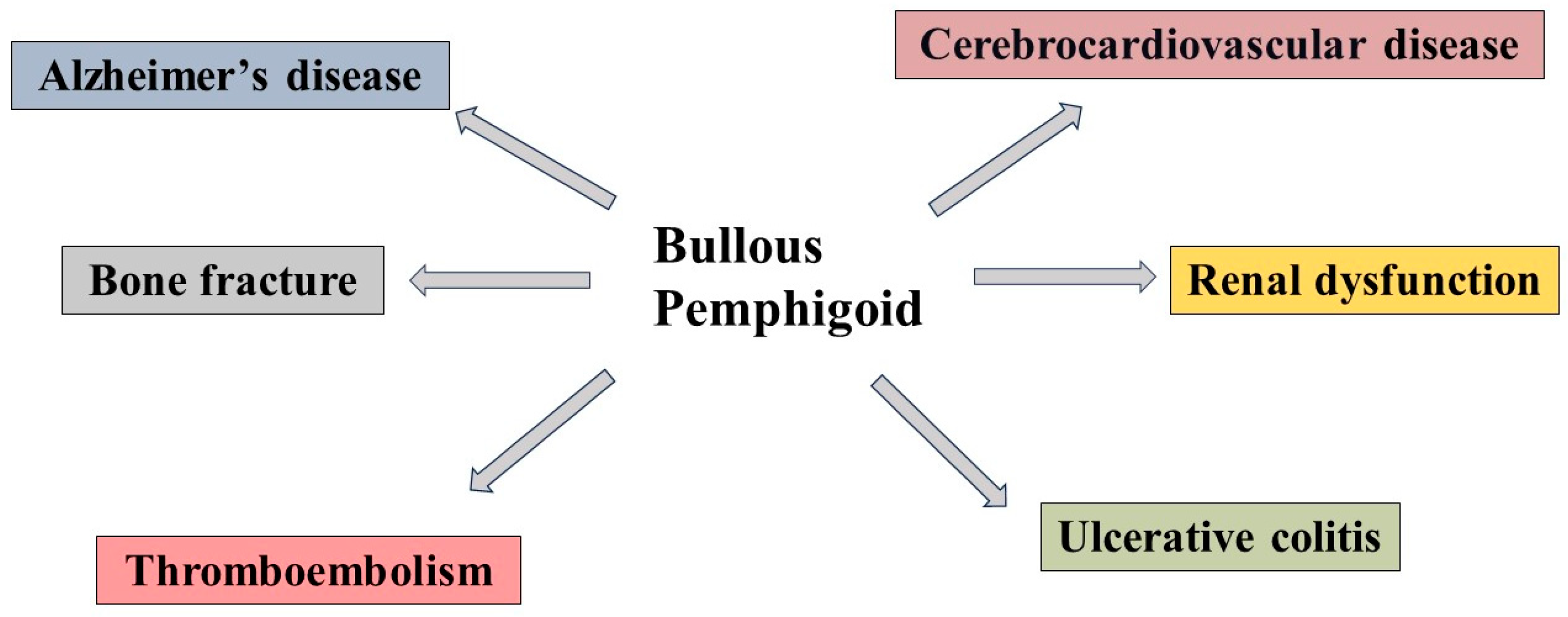
3. BP and Systemic Organ Diseases
4. Bullous Pemphigoid and Cardiovascular Disease
5. Renal Dysfunction
6. Alzheimer’s Disease and BP
7. Ulcerative Colitis and BP
8. Thromboembolism and BP
9. Bone Fracture
10. Whole Interaction of BP with Systemic Organ Inflammation
11. Conclusions
Funding
Conflicts of Interest
References
- Kabashima, K.; Honda, T.; Ginhoux, F.; Egawa, G. The immunological anatomy of the skin. Nat. Rev. Immunol. 2019, 19, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Harris-Tryon, T.A.; Grice, E.A. Microbiota and maintenance of skin barrier function. Science 2022, 376, 940–945. [Google Scholar] [CrossRef] [PubMed]
- Dainichi, T.; Kitoh, A.; Otsuka, A.; Nakajima, S.; Nomura, T.; Kaplan, D.H.; Kabashima, K. The epithelial immune microenvironment (EIME) in atopic dermatitis and psoriasis. Nat. Immunol. 2018, 19, 1286–1298. [Google Scholar] [CrossRef] [PubMed]
- Sawada, Y.; Saito-Sasaki, N.; Mashima, E.; Nakamura, M. Daily Lifestyle and Inflammatory Skin Diseases. Int. J. Mol. Sci. 2021, 22, 5204. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, A.E.; Giai, C.; Gómez, M.I. Staphylococcus aureus Adaptation to the Skin in Health and Persistent/Recurrent Infections. Antibiotics 2023, 12, 1520. [Google Scholar] [CrossRef]
- Luger, T.; Amagai, M.; Dreno, B.; Dagnelie, M.A.; Liao, W.; Kabashima, K.; Schikowski, T.; Proksch, E.; Elias, P.M.; Simon, M.; et al. Atopic dermatitis: Role of the skin barrier, environment, microbiome, and therapeutic agents. J. Dermatol. Sci. 2021, 102, 142–157. [Google Scholar] [CrossRef]
- Zaniboni, M.C.; Samorano, L.P.; Orfali, R.L.; Aoki, V. Skin barrier in atopic dermatitis: Beyond filaggrin. An. Bras. De Dermatol. 2016, 91, 472–478. [Google Scholar] [CrossRef]
- Goad, N.; Gawkrodger, D.J. Ambient humidity and the skin: The impact of air humidity in healthy and diseased states. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1285–1294. [Google Scholar] [CrossRef]
- Fairley, J.A.; Heintz, P.W.; Neuburg, M.; Diaz, L.A.; Giudice, G.J. Expression pattern of the bullous pemphigoid-180 antigen in normal and neoplastic epithelia. Br. J. Dermatol. 1995, 133, 385–391. [Google Scholar] [CrossRef]
- Yamada, T.; Endo, R.; Tsukagoshi, K.; Fujita, S.; Honda, K.; Kinoshita, M.; Hasebe, T.; Hirohashi, S. Aberrant expression of a hemidesmosomal protein, bullous pemphigoid antigen 2, in human squamous cell carcinoma. Lab. Investig. 1996, 75, 589–600. [Google Scholar]
- Bédane, C.; McMillan, J.R.; Balding, S.D.; Bernard, P.; Prost, C.; Bonnetblanc, J.M.; Diaz, L.A.; Eady, R.A.; Giudice, G.J. Bullous pemphigoid and cicatricial pemphigoid autoantibodies react with ultrastructurally separable epitopes on the BP180 ectodomain: Evidence that BP180 spans the lamina lucida. J. Investig. Dermatol. 1997, 108, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, E.; Zillikens, D. Pemphigoid diseases. Lancet 2013, 381, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, T.; Sawada, Y. Psoriasis and Systemic Inflammatory Disorders. Int. J. Mol. Sci. 2022, 23, 4457. [Google Scholar] [CrossRef] [PubMed]
- Itamura, M.; Sawada, Y. Involvement of Atopic Dermatitis in the Development of Systemic Inflammatory Diseases. Int. J. Mol. Sci. 2022, 23, 13445. [Google Scholar] [CrossRef] [PubMed]
- Frezzolini, A.; Teofoli, P.; Cianchini, G.; Barduagni, S.; Ruffelli, M.; Ferranti, G.; Puddu, P.; De Pita, O. Increased expression of eotaxin and its specific receptor CCR3 in bullous pemphigoid. Eur. J. Dermatol. 2002, 12, 27–31. [Google Scholar]
- Gounni Abdelilah, S.; Wellemans, V.; Agouli, M.; Guenounou, M.; Hamid, Q.; Beck, L.A.; Lamkhioued, B. Increased expression of Th2-associated chemokines in bullous pemphigoid disease. Role of eosinophils in the production and release of these chemokines. Clin. Immunol. 2006, 120, 220–231. [Google Scholar] [CrossRef]
- Günther, C.; Carballido-Perrig, N.; Kopp, T.; Carballido, J.M.; Pfeiffer, C. CCL18 is expressed in patients with bullous pemphigoid and parallels disease course. Br. J. Dermatol. 2009, 160, 747–755. [Google Scholar] [CrossRef]
- Feliciani, C.; Toto, P.; Mohammad Pour, S.; Coscione, G.; Amerio, P.; Amerio, P. A Th2-like cytokine response is involved in bullous pemphigoid. the role of IL-4 and IL-5 in the pathogenesis of the disease. Int. J. Immunopathol. Pharmacol. 1999, 12, 55–61. [Google Scholar] [CrossRef]
- Wang, Y.; Mao, X.; Liu, Y.; Yang, Y.; Jin, H.; Li, L. IL-13 Genetic Susceptibility to Bullous Pemphigoid: A Potential Target for Treatment and a Prognostic Marker. Front. Immunol. 2022, 13, 824110. [Google Scholar] [CrossRef]
- Xiong, H.; Dolpady, J.; Wabl, M.; Curotto de Lafaille, M.A.; Lafaille, J.J. Sequential class switching is required for the generation of high affinity IgE antibodies. J. Exp. Med. 2012, 209, 353–364. [Google Scholar] [CrossRef]
- D’Auria, L.; Bonifati, C.; Cordiali-Fei, P.; Leone, G.; Picardo, M.; Pietravalle, M.; Giacalone, B.; Ameglio, F. Increased serum interleukin-15 levels in bullous skin diseases: Correlation with disease intensity. Arch. Dermatol. Res. 1999, 291, 354–356. [Google Scholar] [CrossRef] [PubMed]
- Freire, P.C.; Muñoz, C.H.; Stingl, G. IgE autoreactivity in bullous pemphigoid: Eosinophils and mast cells as major targets of pathogenic immune reactants. Br. J. Dermatol. 2017, 177, 1644–1653. [Google Scholar] [CrossRef] [PubMed]
- Giang Pham, N.; Thi Ha Nguyen, V.; Le Huu, D. High serum total IgE levels correlate with urticarial lesions and IgE deposition in perilesional skin of bullous pemphigoid patients: An observational study. Indian. J. Dermatol. Venereol. Leprol. 2023, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Iryo, K.; Tsuda, S.; Sasai, Y. Ultrastructural aspects of infiltrated eosinophils in bullous pemphigoid. J. Dermatol. 1992, 19, 393–399. [Google Scholar] [CrossRef]
- Ståhle-Bäckdahl, M.; Inoue, M.; Guidice, G.J.; Parks, W.C. 92-kD gelatinase is produced by eosinophils at the site of blister formation in bullous pemphigoid and cleaves the extracellular domain of recombinant 180-kD bullous pemphigoid autoantigen. J. Clin. Investig. 1994, 93, 2022–2030. [Google Scholar] [CrossRef]
- Ishiura, N.; Fujimoto, M.; Watanabe, R.; Nakashima, H.; Kuwano, Y.; Yazawa, N.; Echigo, T.; Okochi, H.; Tamaki, K. Serum levels of IgE anti-BP180 and anti-BP230 autoantibodies in patients with bullous pemphigoid. J. Dermatol. Sci. 2008, 49, 153–161. [Google Scholar] [CrossRef]
- Farnaghi, F.; Ehsani, A.H.; Kamyab-Hesary, K.; Abbasian, S.; Seirafi, H.; Nasimi, M. Correlation of dermal and blood eosinophilia with bullous pemphigoid disease severity. Int. J. Womens Dermatol. 2020, 6, 171–175. [Google Scholar] [CrossRef]
- Jovanovic, D.V.; Martel-Pelletier, J.; Di Battista, J.A.; Mineau, F.; Jolicoeur, F.C.; Benderdour, M.; Pelletier, J.P. Stimulation of 92-kd gelatinase (matrix metalloproteinase 9) production by interleukin-17 in human monocyte/macrophages: A possible role in rheumatoid arthritis. Arthritis Rheum. 2000, 43, 1134–1144. [Google Scholar] [CrossRef]
- Huang, R.; Hu, L.; Jiang, F. Study of cytokine-induced immunity in bullous pemphigoid: Recent developments. Ann. Med. 2023, 55, 2280991. [Google Scholar] [CrossRef]
- Giusti, D.; Bini, E.; Terryn, C.; Didier, K.; Le Jan, S.; Gatouillat, G.; Durlach, A.; Nesmond, S.; Muller, C.; Bernard, P.; et al. NET Formation in Bullous Pemphigoid Patients With Relapse Is Modulated by IL-17 and IL-23 Interplay. Front. Immunol. 2019, 10, 701. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, C.; Wang, Y.; Mo, B.; Wei, J.; Ma, L.; Rao, L.; Wang, J.; Yao, D.; Huang, J.; et al. E4BP4 facilitates glucocorticoid sensitivity of human bronchial epithelial cells via down-regulation of glucocorticoid receptor-beta. Cell Immunol. 2018, 334, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Emson, C.L.; Bell, S.E.; Jones, A.; Wisden, W.; McKenzie, A.N. Interleukin (IL)-4-independent induction of immunoglobulin (Ig)E, and perturbation of T cell development in transgenic mice expressing IL-13. J. Exp. Med. 1998, 188, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Wang, Y.; Chen, X.; Yang, N.; Li, L. Targeting interleukin 4 and interleukin 13: A novel therapeutic approach in bullous pemphigoid. Ann. Med. 2023, 55, 1156–1170. [Google Scholar] [CrossRef] [PubMed]
- Borrego, L.; Maynard, B.; Peterson, E.A.; George, T.; Iglesias, L.; Peters, M.S.; Newman, W.; Gleich, G.J.; Leiferman, K.M. Deposition of eosinophil granule proteins precedes blister formation in bullous pemphigoid. Comparison with neutrophil and mast cell granule proteins. Am. J. Pathol. 1996, 148, 897–909. [Google Scholar] [PubMed]
- Ujiie, H. IgE autoantibodies in bullous pemphigoid: Supporting role, or leading player? J. Dermatol. Sci. 2015, 78, 5–10. [Google Scholar] [CrossRef]
- Mills, K.H.G. IL-17 and IL-17-producing cells in protection versus pathology. Nat. Rev. Immunol. 2023, 23, 38–54. [Google Scholar] [CrossRef]
- McDermott, A.J.; Falkowski, N.R.; McDonald, R.A.; Pandit, C.R.; Young, V.B.; Huffnagle, G.B. Interleukin-23 (IL-23), independent of IL-17 and IL-22, drives neutrophil recruitment and innate inflammation during Clostridium difficile colitis in mice. Immunology 2016, 147, 114–124. [Google Scholar] [CrossRef]
- Anderson, J.L.; Morrow, D.A. Acute Myocardial Infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef]
- Yang, Y.W.; Chen, Y.H.; Xirasagar, S.; Lin, H.C. Increased risk of stroke in patients with bullous pemphigoid: A population-based follow-up study. Stroke 2011, 42, 319–323. [Google Scholar] [CrossRef]
- Cai, S.C.; Allen, J.C.; Lim, Y.L.; Chua, S.H.; Tan, S.H.; Tang, M.B. Mortality of bullous pemphigoid in Singapore: Risk factors and causes of death in 359 patients seen at the National Skin Centre. Br. J. Dermatol. 2014, 170, 1319–1326. [Google Scholar] [CrossRef]
- Shen, W.C.; Chiang, H.Y.; Chen, P.S.; Lin, Y.T.; Kuo, C.C.; Wu, P.Y. Risk of All-Cause Mortality, Cardiovascular Disease Mortality, and Cancer Mortality in Patients With Bullous Pemphigoid. JAMA Dermatol. 2022, 158, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Försti, A.K.; Jokelainen, J.; Timonen, M.; Tasanen, K. Risk of Death in Bullous Pemphigoid: A Retrospective Database Study in Finland. Acta Derm. Venereol. 2016, 96, 758–761. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.N.; Teague, H.L.; Swindell, W.R.; Baumer, Y.; Ward, N.L.; Xing, X.; Baugous, B.; Johnston, A.; Joshi, A.A.; Silverman, J.; et al. IFN-γ and TNF-α synergism may provide a link between psoriasis and inflammatory atherogenesis. Sci. Rep. 2017, 7, 13831. [Google Scholar] [CrossRef]
- Eid, R.E.; Rao, D.A.; Zhou, J.; Lo, S.F.; Ranjbaran, H.; Gallo, A.; Sokol, S.I.; Pfau, S.; Pober, J.S.; Tellides, G. Interleukin-17 and interferon-gamma are produced concomitantly by human coronary artery-infiltrating T cells and act synergistically on vascular smooth muscle cells. Circulation 2009, 119, 1424–1432. [Google Scholar] [CrossRef] [PubMed]
- Karbach, S.; Croxford, A.L.; Oelze, M.; Schüler, R.; Minwegen, D.; Wegner, J.; Koukes, L.; Yogev, N.; Nikolaev, A.; Reißig, S.; et al. Interleukin 17 drives vascular inflammation, endothelial dysfunction, and arterial hypertension in psoriasis-like skin disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2658–2668. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.P.; Pavel, A.B.; Wu, J.; Fernandes, M.; Maari, C.; Saint-Cyr Proulx, E.; Jack, C.; Glickman, J.; Choi, S.; He, H.; et al. Vascular inflammation in moderate-to-severe atopic dermatitis is associated with enhanced Th2 response. Allergy 2021, 76, 3107–3121. [Google Scholar] [CrossRef]
- D’Agostino, G.M.; Rizzetto, G.; Marani, A.; Marasca, S.; Candelora, M.; Gambini, D.; Gioacchini, H.; De Simoni, E.; Maurizi, A.; Campanati, A.; et al. Bullous Pemphygoid and Novel Therapeutic Approaches. Biomedicines 2022, 10, 2844. [Google Scholar] [CrossRef]
- Romagnani, P.; Remuzzi, G.; Glassock, R.; Levin, A.; Jager, K.J.; Tonelli, M.; Massy, Z.; Wanner, C.; Anders, H.J. Chronic kidney disease. Nat. Rev. Dis. Primers 2017, 3, 17088. [Google Scholar] [CrossRef]
- Lee, S.; Rastogi, S.; Hsu, D.Y.; Nardone, B.; Silverberg, J.I. Association of bullous pemphigoid and comorbid health conditions: A case-control study. Arch. Dermatol. Res. 2021, 313, 327–332. [Google Scholar] [CrossRef]
- Morimoto, K.; Yoshida, T.; Washida, N.; Uchiyama, K.; Nakayama, T.; Itoh, H.; Oya, M. Bullous pemphigoid in patients receiving peritoneal dialysis: A case series and a literature survey. Ren. Fail. 2021, 43, 651–657. [Google Scholar] [CrossRef]
- Osipowicz, K.; Kalinska-Bienias, A.; Kowalewski, C.; Wozniak, K. Development of bullous pemphigoid during the haemodialysis of a young man: Case report and literature survey. Int. Wound J. 2017, 14, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; You, R.; Yu, N.; Gong, Y.; Qu, C.; Zhang, Y.; Lu, G.; Huang, Y.; Zhang, H.; Gao, Y.; et al. Increased proportions of Tc17 cells and NK cells may be risk factors for disease progression in Hashimoto’s thyroiditis. Int. Immunopharmacol. 2016, 40, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Lavoz, C.; Matus, Y.S.; Orejudo, M.; Carpio, J.D.; Droguett, A.; Egido, J.; Mezzano, S.; Ruiz-Ortega, M. Interleukin-17A blockade reduces albuminuria and kidney injury in an accelerated model of diabetic nephropathy. Kidney Int. 2019, 95, 1418–1432. [Google Scholar] [CrossRef] [PubMed]
- Odobasic, D.; Gan, P.Y.; Summers, S.A.; Semple, T.J.; Muljadi, R.C.; Iwakura, Y.; Kitching, A.R.; Holdsworth, S.R. Interleukin-17A promotes early but attenuates established disease in crescentic glomerulonephritis in mice. Am. J. Pathol. 2011, 179, 1188–1198. [Google Scholar] [CrossRef]
- Liu, B.; Jiang, J.; Liang, H.; Xiao, P.; Lai, X.; Nie, J.; Yu, W.; Gao, Y.; Wen, S. Natural killer T cell/IL-4 signaling promotes bone marrow-derived fibroblast activation and M2 macrophage-to-myofibroblast transition in renal fibrosis. Int. Immunopharmacol. 2021, 98, 107907. [Google Scholar] [CrossRef] [PubMed]
- Braga, T.T.; Correa-Costa, M.; Guise, Y.F.; Castoldi, A.; de Oliveira, C.D.; Hyane, M.I.; Cenedeze, M.A.; Teixeira, S.A.; Muscara, M.N.; Perez, K.R.; et al. MyD88 signaling pathway is involved in renal fibrosis by favoring a TH2 immune response and activating alternative M2 macrophages. Mol. Med. 2012, 18, 1231–1239. [Google Scholar] [CrossRef] [PubMed]
- Gungor, O.; Unal, H.U.; Guclu, A.; Gezer, M.; Eyileten, T.; Guzel, F.B.; Altunoren, O.; Erken, E.; Oguz, Y.; Kocyigit, I.; et al. IL-33 and ST2 levels in chronic kidney disease: Associations with inflammation, vascular abnormalities, cardiovascular events, and survival. PLoS ONE 2017, 12, e0178939. [Google Scholar] [CrossRef]
- Masters, C.L.; Bateman, R.; Blennow, K.; Rowe, C.C.; Sperling, R.A.; Cummings, J.L. Alzheimer’s disease. Nat. Rev. Dis. Primers 2015, 1, 15056. [Google Scholar] [CrossRef]
- Brick, K.E.; Weaver, C.H.; Savica, R.; Lohse, C.M.; Pittelkow, M.R.; Boeve, B.F.; Gibson, L.E.; Camilleri, M.J.; Wieland, C.N. A population-based study of the association between bullous pemphigoid and neurologic disorders. J. Am. Acad. Dermatol. 2014, 71, 1191–1197. [Google Scholar] [CrossRef]
- Kokkonen, N.; Herukka, S.K.; Huilaja, L.; Kokki, M.; Koivisto, A.M.; Hartikainen, P.; Remes, A.M.; Tasanen, K. Increased Levels of the Bullous Pemphigoid BP180 Autoantibody Are Associated with More Severe Dementia in Alzheimer’s Disease. J. Investig. Dermatol. 2017, 137, 71–76. [Google Scholar] [CrossRef]
- Kibsgaard, L.; Rasmussen, M.; Lamberg, A.; Deleuran, M.; Olesen, A.B.; Vestergaard, C. Increased frequency of multiple sclerosis among patients with bullous pemphigoid: A population-based cohort study on comorbidities anchored around the diagnosis of bullous pemphigoid. Br. J. Dermatol. 2017, 176, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Kridin, K.; Hübner, F.; Recke, A.; Linder, R.; Schmidt, E. The burden of neurological comorbidities in six autoimmune bullous diseases: A population-based study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2074–2078. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.N.; Hammers, C.M.; Mao, X.; Jin, H.Z.; Yuan, J.; Li, L. Analysis of the autoimmune response against BP180 in patients with Alzheimer’s disease. Ann. Transl. Med. 2021, 9, 107. [Google Scholar] [CrossRef] [PubMed]
- Oberstein, T.J.; Taha, L.; Spitzer, P.; Hellstern, J.; Herrmann, M.; Kornhuber, J.; Maler, J.M. Imbalance of Circulating T(h)17 and Regulatory T Cells in Alzheimer’s Disease: A Case Control Study. Front. Immunol. 2018, 9, 1213. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ke, K.F.; Liu, Z.; Qiu, Y.H.; Peng, Y.P. Th17 cell-mediated neuroinflammation is involved in neurodegeneration of aβ1-42-induced Alzheimer’s disease model rats. PLoS ONE 2013, 8, e75786. [Google Scholar] [CrossRef]
- Cristiano, C.; Volpicelli, F.; Lippiello, P.; Buono, B.; Raucci, F.; Piccolo, M.; Iqbal, A.J.; Irace, C.; Miniaci, M.C.; Perrone Capano, C.; et al. Neutralization of IL-17 rescues amyloid-β-induced neuroinflammation and memory impairment. Br. J. Pharmacol. 2019, 176, 3544–3557. [Google Scholar] [CrossRef]
- Xu, J.J.; Guo, S.; Xue, R.; Xiao, L.; Kou, J.N.; Liu, Y.Q.; Han, J.Y.; Fu, J.J.; Wei, N. Adalimumab ameliorates memory impairments and neuroinflammation in chronic cerebral hypoperfusion rats. Aging 2021, 13, 14001–14014. [Google Scholar] [CrossRef]
- Barth, J.H.; Kelly, S.E.; Wojnarowska, F.; Savin, J.A.; Whittaker, S.; Cream, J.J.; White, J.E. Pemphigoid and ulcerative colitis. J. Am. Acad. Dermatol. 1988, 19 Pt 1, 303–308. [Google Scholar] [CrossRef]
- Kaplan, R.P. Bullous pemphigoid and ulcerative colitis. Arch. Dermatol. 1991, 127, 1728–1729. [Google Scholar] [CrossRef]
- Chen, Y.J.; Juan, C.K.; Chang, Y.T.; Wu, C.Y.; Ho, H.J.; Tseng, H.C. Association between inflammatory bowel disease and bullous pemphigoid: A population-based case-control study. Sci. Rep. 2020, 10, 12727. [Google Scholar] [CrossRef]
- Leppkes, M.; Becker, C.; Ivanov, I.I.; Hirth, S.; Wirtz, S.; Neufert, C.; Pouly, S.; Murphy, A.J.; Valenzuela, D.M.; Yancopoulos, G.D.; et al. RORgamma-expressing Th17 cells induce murine chronic intestinal inflammation via redundant effects of IL-17A and IL-17F. Gastroenterology 2009, 136, 257–267. [Google Scholar] [CrossRef]
- OuYang, Z.; Hirota, Y.; Osuga, Y.; Hamasaki, K.; Hasegawa, A.; Tajima, T.; Hirata, T.; Koga, K.; Yoshino, O.; Harada, M.; et al. Interleukin-4 stimulates proliferation of endometriotic stromal cells. Am. J. Pathol. 2008, 173, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.L.; Wu, C.Y.; Lyu, Y.S.; Chou, Y.J.; Chang, Y.T.; Wu, C.Y. Association between bullous pemphigoid and risk of venous thromboembolism: A nationwide population-based cohort study. J. Dermatol. 2022, 49, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Cugno, M.; Marzano, A.V.; Bucciarelli, P.; Balice, Y.; Cianchini, G.; Quaglino, P.; Calzavara Pinton, P.; Caproni, M.; Alaibac, M.; De Simone, C.; et al. Increased risk of venous thromboembolism in patients with bullous pemphigoid. The INVENTEP (INcidence of VENous ThromboEmbolism in bullous Pemphigoid) study. Thromb. Haemost. 2016, 115, 193–199. [Google Scholar] [PubMed]
- Mo, J.W.; Zhang, D.F.; Ji, G.L.; Liu, X.Z.; Fan, B. Detection of targets and their mechanisms for early diagnosis of traumatic deep vein thrombosis. Genet. Mol. Res. 2015, 14, 2413–2421. [Google Scholar] [CrossRef] [PubMed]
- Ding, P.; Zhang, S.; Yu, M.; Feng, Y.; Long, Q.; Yang, H.; Li, J.; Wang, M. IL-17A promotes the formation of deep vein thrombosis in a mouse model. Int. Immunopharmacol. 2018, 57, 132–138. [Google Scholar] [CrossRef]
- Eastell, R.; O’Neill, T.W.; Hofbauer, L.C.; Langdahl, B.; Reid, I.R.; Gold, D.T.; Cummings, S.R. Postmenopausal osteoporosis. Nat. Rev. Dis. Primers 2016, 2, 16069. [Google Scholar] [CrossRef]
- Chovatiya, R.; Silverberg, J.I. Association of pemphigus and pemphigoid with osteoporosis and pathological fractures. Arch. Dermatol. Res. 2020, 312, 263–271. [Google Scholar] [CrossRef]
- Marzano, A.V.; Trevisan, V.; Eller-Vainicher, C.; Cairoli, E.; Marchese, L.; Morelli, V.; Beck-Peccoz, P.; Crosti, C.; Chiodini, I. Evidence for vitamin D deficiency and increased prevalence of fractures in autoimmune bullous skin diseases. Br. J. Dermatol. 2012, 167, 688–691. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Y.; Luo, Z.; Wu, Y.; Niu, T.; Zheng, J.; Xie, Y. Prognostic factors for mortality in bullous pemphigoid: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0264705. [Google Scholar] [CrossRef]
- Guo, W.; Rathi, S.; Marquez, J.; Smith, H.; Kuruvilla, A.; Tonnesen, M.G.; Salvemini, J.N. Prevalence of diabetes mellitus in bullous pemphigoid patients in the absence of dipeptidyl peptidase-4 inhibitors: A systematic review and meta-analysis. Arch. Dermatol. Res. 2023, 315, 2207–2213. [Google Scholar] [CrossRef] [PubMed]
- Patton, T.; Korman, N.J. Bullous pemphigoid treatment review. Expert Opin. Pharmacother. 2006, 7, 2403–2411. [Google Scholar] [CrossRef] [PubMed]
- Bağcı, I.S.; Horváth, O.N.; Ruzicka, T.; Sárdy, M. Bullous pemphigoid. Autoimmun. Rev. 2017, 16, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Kubin, M.E.; Hellberg, L.; Palatsi, R. Glucocorticoids: The mode of action in bullous pemphigoid. Exp. Dermatol. 2017, 26, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.C.; Wojnarowska, F.; Kirtschig, G.; Mason, J.; Godec, T.R.; Schmidt, E.; Chalmers, J.R.; Childs, M.; Walton, S.; Harman, K.; et al. Doxycycline versus prednisolone as an initial treatment strategy for bullous pemphigoid: A pragmatic, non-inferiority, randomised controlled trial. Lancet 2017, 389, 1630–1638. [Google Scholar] [CrossRef]
- Żychowska, M. Dapsone: A forgotten and underestimated treatment option for bullous pemphigoid? Br. J. Dermatol. 2017, 177, 1156–1157. [Google Scholar] [CrossRef]
- Cardones, A.R.; Hall, R.P. Doxycycline and the treatment for bullous pemphigoid: What outcomes are most important to our patients? Br. J. Dermatol. 2017, 177, 1145–1147. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, Q.; Chen, L.; Chen, J.; Zhang, J.; Zou, Y.; Gong, T.; Ji, C. Efficacy and Safety of Dupilumab in Moderate-to-Severe Bullous Pemphigoid. Front. Immunol. 2021, 12, 738907. [Google Scholar] [CrossRef]
- Zhao, L.; Wang, Q.; Liang, G.; Zhou, Y.; Yiu, N.; Yang, B.; Zhang, G.; Li, W.; Feng, S.; Shang, P.; et al. Evaluation of Dupilumab in Patients With Bullous Pemphigoid. JAMA Dermatol. 2023, 159, 953–960. [Google Scholar] [CrossRef]
- Chebani, R.; Lombart, F.; Chaby, G.; Dadban, A.; Debarbieux, S.; Viguier, M.A.; Ingen-Housz-Oro, S.; Pham-Ledard, A.; Bedane, C.R.; Picard-Dahan, C.; et al. Omalizumab in the treatment of bullous pemphigoid resistant to first-line therapy: A French national multicentre retrospective study of 100 patients. Br. J. Dermatol. 2024, 190, 258–265. [Google Scholar] [CrossRef]
- Granados-Betancort, E.; Sánchez-Díaz, M.; Muñoz-Barba, D.; Arias-Santiago, S. Omalizumab and Dupilumab for the Treatment of Bullous Pemphigoid: A Systematic Review. J. Clin. Med. 2024, 13, 4844. [Google Scholar] [CrossRef] [PubMed]
- Cao, P.; Xu, W.; Zhang, L. Rituximab, Omalizumab, and Dupilumab Treatment Outcomes in Bullous Pemphigoid: A Systematic Review. Front. Immunol. 2022, 13, 928621. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.; Ahmed, A.R. Treatment of bullous pemphigoid with rituximab: Critical analysis of the current literature. J. Drugs Dermatol. 2013, 12, 672–677. [Google Scholar] [PubMed]
- Kremer, N.; Snast, I.; Cohen, E.S.; Hodak, E.; Mimouni, D.; Lapidoth, M.; Mazor, S.; Levi, A. Rituximab and Omalizumab for the Treatment of Bullous Pemphigoid: A Systematic Review of the Literature. Am. J. Clin. Dermatol. 2019, 20, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Terui, H.; Asano, Y. Biologics for Reducing Cardiovascular Risk in Psoriasis Patients. J. Clin. Med. 2023, 12, 1162. [Google Scholar] [CrossRef]
- Wang, R.; Wang, A.; Wang, M. Two cases with bullous pemphigoid relapsed after using interleukin-17A inhibitors for psoriasis: A paradoxical reaction. J. Dermatol. 2023, 50, 956–959. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mashima, E.; Saito-Sasaki, N.; Sawada, Y. Systemic Implications of Bullous Pemphigoid: Bridging Dermatology and Internal Medicine. Diagnostics 2024, 14, 2272. https://doi.org/10.3390/diagnostics14202272
Mashima E, Saito-Sasaki N, Sawada Y. Systemic Implications of Bullous Pemphigoid: Bridging Dermatology and Internal Medicine. Diagnostics. 2024; 14(20):2272. https://doi.org/10.3390/diagnostics14202272
Chicago/Turabian StyleMashima, Emi, Natsuko Saito-Sasaki, and Yu Sawada. 2024. "Systemic Implications of Bullous Pemphigoid: Bridging Dermatology and Internal Medicine" Diagnostics 14, no. 20: 2272. https://doi.org/10.3390/diagnostics14202272
APA StyleMashima, E., Saito-Sasaki, N., & Sawada, Y. (2024). Systemic Implications of Bullous Pemphigoid: Bridging Dermatology and Internal Medicine. Diagnostics, 14(20), 2272. https://doi.org/10.3390/diagnostics14202272