
Intramuscular Neural Distribution of the Gluteus Maximus Muscle: Diagnostic Electromyography and Injective Treatments



Abstract
1. Introduction
2. Materials and Methods
2.1. Modified Sihler Staining Procedure
- Fixation: The Gmax specimens were placed in a 10% formalin solution (for one week for fixation).
- Maceration and Depigmentation: After fixation, the specimens were soaked in running tap water for one hour and then submerged in a 3% aqueous potassium hydroxide and 0.01% hydrogen peroxide solution for 3 to 4 weeks for maceration and depigmentation. We monitored the solution closely and replaced it whenever it became cloudy, which is essential for subsequent staining. Because of the substantial thickness of the Gmax muscle belly, we applied manual manipulation such as gentle kneading to ensure effective maceration.
- Decalcification: For whitening and decalcification, the specimens were soaked in Sihler 1 solution (10% glycerin and 7% glacial acetic acid) for a week.
- Staining: The specimens were soaked in Sihler 2 solution (10% glycerin and 10% Ehrlich’s hematoxylin) for one week to stain the neural structures.
- Destaining: The stained muscle specimens were re-immersed in Sihler 1 solution to remove excess staining. This step ensures that only neural structures retain the stain for clear visualization.
- Neutralization: After destaining, the specimens were rinsed in flowing water for 40 min and then soaked in 0.05% lithium carbonate solution for 50 min to intensify the nerve color.
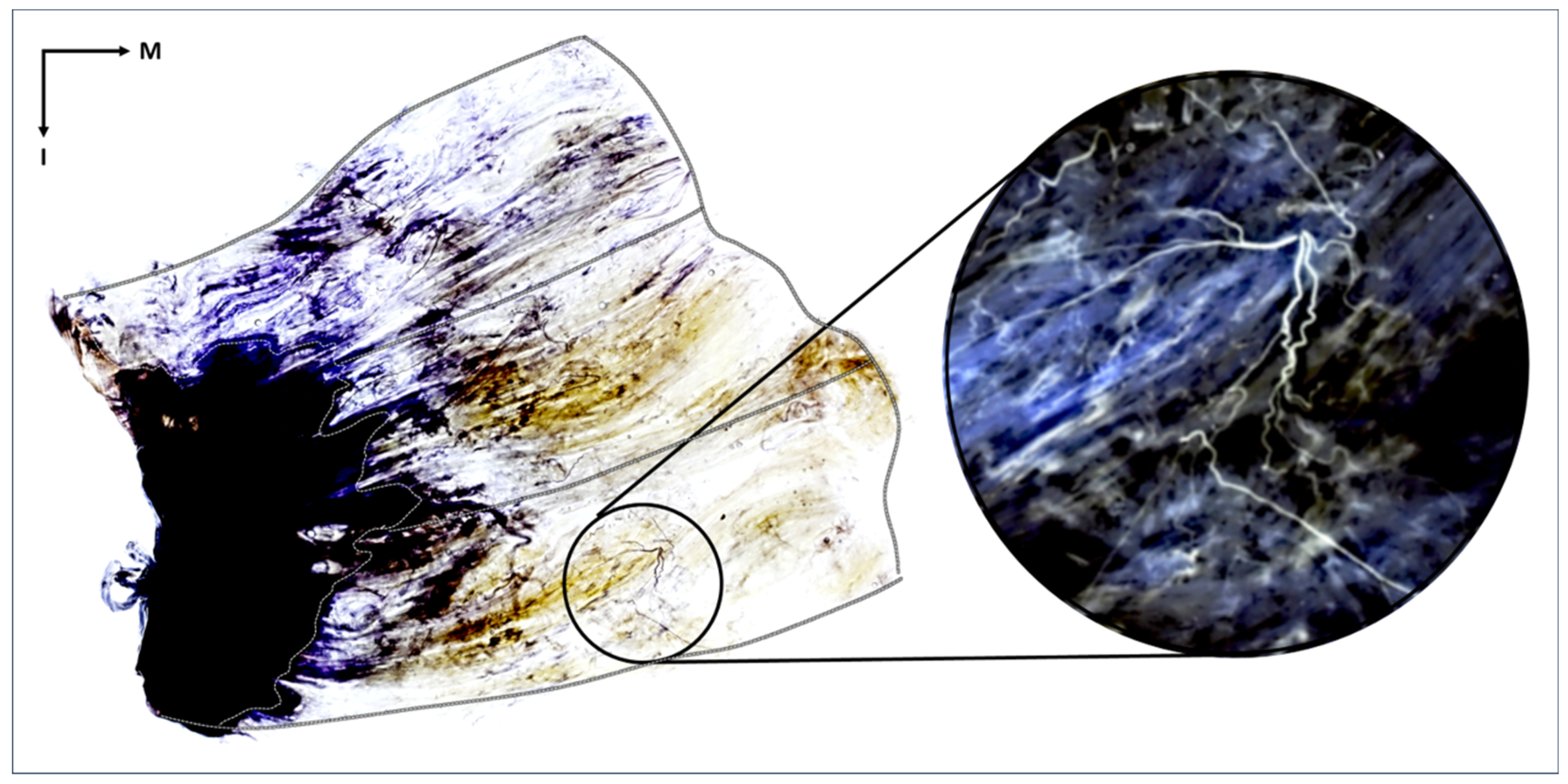
- Clearing: In the final stage, the neutralized Gmax specimens were gradually brought to transparency using a cleaning solution of 1:1 glycerin and formamide. The concentration of the solution was increased from 70% to 100% in 10% increments as the solution was changed daily for several days. This process makes the muscle tissue transparent and emphasizes the stained nerves (Figure 1).
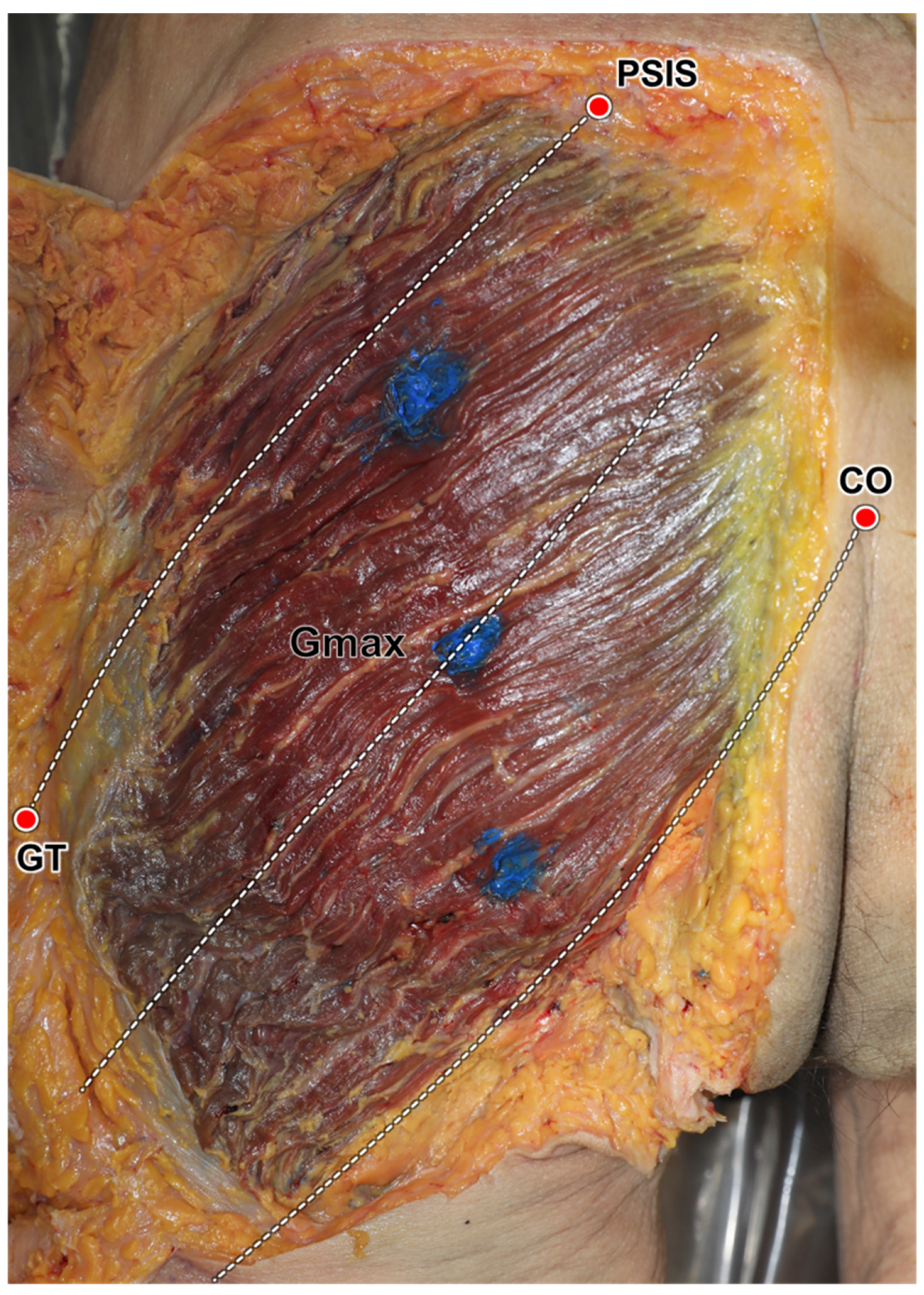
- Identification and Analysis of Neural Distribution Patterns: After Sihler staining was complete, each stained Gmax was placed on a vinyl-wrapped LED view box. The distribution of nerves was observed using a magnifying glass. Each Gmax was divided into three segments, caudal, middle, and cranial, each of which was further divided into ten equal parts based on the width from the muscle origin to its insertion. The presence and distribution of nerve endings in each part were examined. Then, the proportion of each area containing nerve endings was calculated to determine the intramuscular neural distribution ratio across the entire muscle.
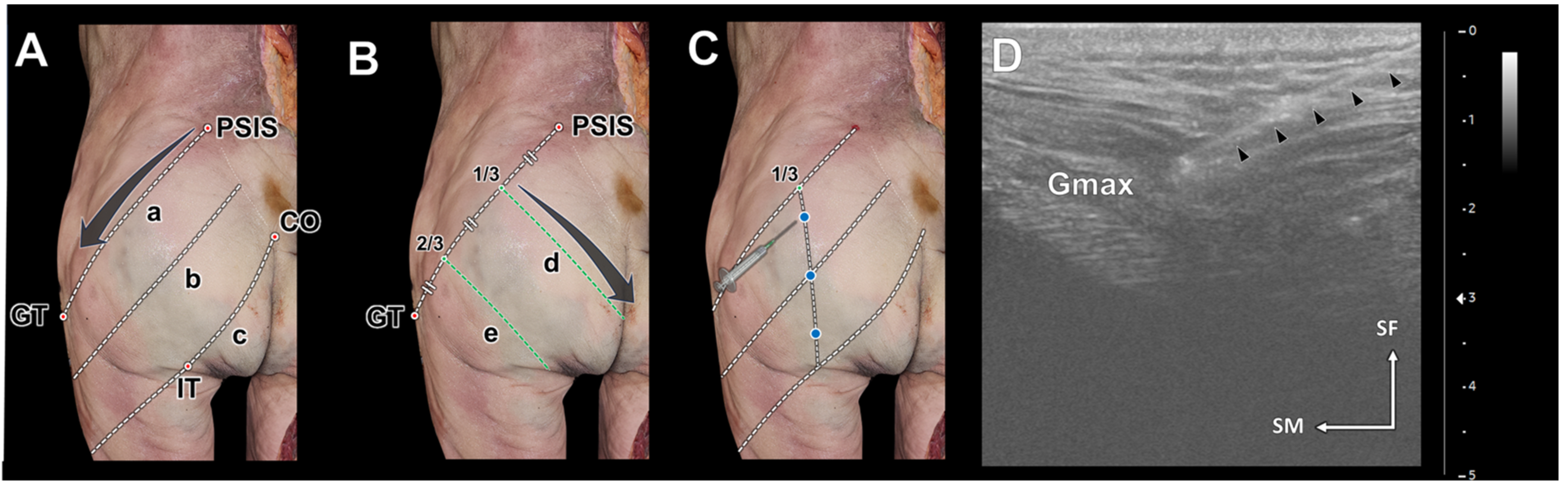
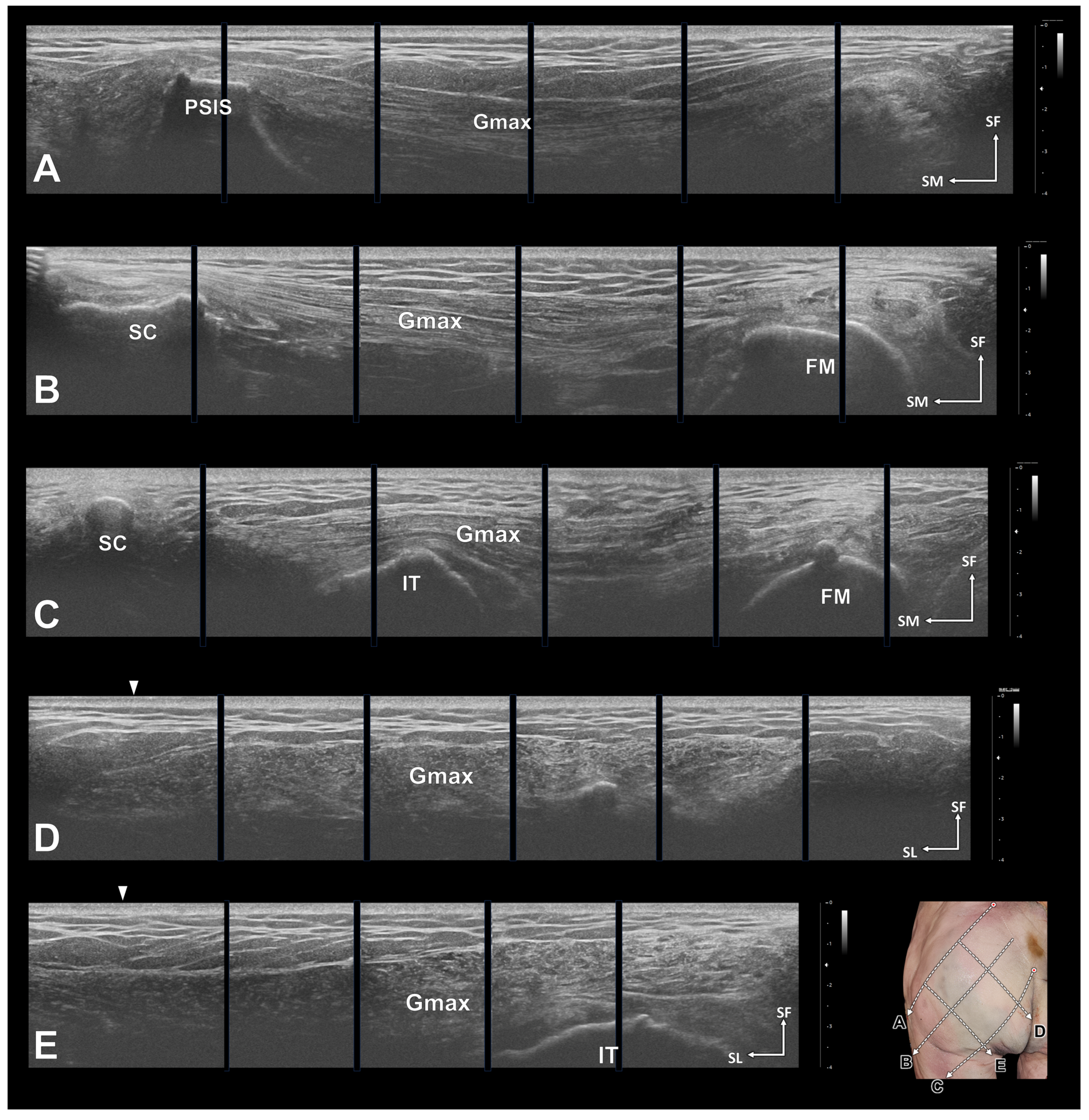
2.2. Ultrasonography and Ultrasound-Guided Injections
3. Results
3.1. Neural Distribution Patterns in the Gmax
3.2. Cranial Segment
3.3. Middle Segment
3.4. Caudal Segment
3.5. Ultrasonography and Ultrasound-Guided Injections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barnes, M.P.; Kent, R.M.; Semlyen, J.K.; McMullen, K.M. Spasticity in multiple sclerosis. Neurorehabilit. Neural Repair 2003, 17, 66–70. [Google Scholar] [CrossRef]
- Standring, S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Tugui, R.D.; Antonescu, D. Cerebral palsy gait, clinical importance. Maedica 2013, 8, 388–393. [Google Scholar]
- Rosales, R.L.; Kong, K.H.; Goh, K.J.; Kumthornthip, W.; Mok, V.C.; Delgado-De Los Santos, M.M.; Chua, K.S.; Abdullah, S.J.; Zakine, B.; Maisonobe, P.; et al. Botulinum toxin injection for hypertonicity of the upper extremity within 12 weeks after stroke: A randomized controlled trial. Neurorehabilit. Neural Repair 2012, 26, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Rameckers, E.A.; Speth, L.A.; Duysens, J.; Vles, J.S.; Smits-Engelsman, B.C. Botulinum toxin-a in children with congenital spastic hemiplegia does not improve upper extremity motor-related function over rehabilitation alone: A randomized controlled trial. Neurorehabilit. Neural Repair 2009, 23, 218–225. [Google Scholar] [CrossRef]
- Lam, T.I.; Bingham, D.; Chang, T.J.; Lee, C.C.; Shi, J.; Wang, D.; Massa, S.; Swanson, R.A.; Liu, J. Beneficial effects of minocycline and botulinum toxin-induced constraint physical therapy following experimental traumatic brain injury. Neurorehabilit. Neural Repair 2013, 27, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.F.; Hsu, C.W.; Sun, H.P.; Hwang, C.W.; Yang, C.L.; Wang, J.L. Combined botulinum toxin type A with modified constraint-induced movement therapy for chronic stroke patients with upper extremity spasticity: A randomized controlled study. Neurorehabilit. Neural Repair 2010, 24, 34–41. [Google Scholar] [CrossRef]
- Diserens, K.; Ruegg, D.; Kleiser, R.; Hyde, S.; Perret, N.; Vuadens, P.; Fornari, E.; Vingerhoets, F.; Seitz, R.J. Effect of repetitive arm cycling following botulinum toxin injection for poststroke spasticity: Evidence from FMRI. Neurorehabilit. Neural Repair 2010, 24, 753–762. [Google Scholar] [CrossRef]
- Won, S.Y.; Rha, D.W.; Kim, H.S.; Jung, S.H.; Park, E.S.; Hu, K.S.; Kim, H.J. Intramuscular nerve distribution pattern of the adductor longus and gracilis muscles demonstrated with Sihler staining: Guidance for botulinum toxin injection. Muscle Nerve 2012, 46, 80–85. [Google Scholar] [CrossRef]
- Hsu, T.S.; Dover, J.S.; Arndt, K.A. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch. Dermatol. 2004, 140, 1351–1354. [Google Scholar] [CrossRef]
- Kinnett, D. Botulinum toxin A injections in children: Technique and dosing issues. Am. J. Phys. Med. Rehabil. 2004, 83, S59–S64. [Google Scholar] [CrossRef]
- Lepage, D.; Parratte, B.; Tatu, L.; Vuiller, F.; Monnier, G. Extra- and intramuscular nerve supply of the muscles of the anterior antebrachial compartment: Applications for selective neurotomy and for botulinum toxin injection. Surg. Radiol. Anat. 2005, 27, 420–430. [Google Scholar] [CrossRef] [PubMed]
- De Andrés, J.; Adsuara, V.M.; Palmisani, S.; Villanueva, V.; López-Alarcón, M.D. A double-blind, controlled, randomized trial to evaluate the efficacy of botulinum toxin for the treatment of lumbar myofascial pain in humans. Reg. Anesth. Pain Med. 2010, 35, 255–260. [Google Scholar] [CrossRef]
- Stecco, A.; Gesi, M.; Stecco, C.; Stern, R. Fascial components of the myofascial pain syndrome. Curr. Pain Headache Rep. 2013, 17, 352. [Google Scholar] [CrossRef]
- Akamatsu, F.E.; Yendo, T.M.; Rhode, C.; Itezerote, A.M.; Hojaij, F.; Andrade, M.; Hsing, W.T.; Jacomo, A.L. Anatomical Basis of the Myofascial Trigger Points of the Gluteus Maximus Muscle. BioMed Res. Int. 2017, 2017, 4821968. [Google Scholar] [CrossRef] [PubMed]
- Van Campenhout, A.; Hubens, G.; Fagard, K.; Molenaers, G. Localization of motor nerve branches of the human psoas muscle. Muscle Nerve 2010, 42, 202–207. [Google Scholar] [CrossRef]
- Sheverdin, V.A.; Hur, M.S.; Won, S.Y.; Song, W.C.; Hu, K.S.; Koh, K.S.; Kim, H.J. Extra- and intramuscular nerves distributions of the triceps surae muscle as a basis for muscle resection and botulinum toxin injections. Surg. Radiol. Anat. 2009, 31, 615–621. [Google Scholar] [CrossRef]
- Won, S.Y.; Hur, M.S.; Rha, D.W.; Park, H.D.; Hu, K.S.; Fontaine, C.; Kim, H.J. Extra- and intramuscular nerve distribution patterns of the muscles of the ventral compartment of the forearm. Am. J. Phys. Med Rehabil. 2010, 89, 644–652. [Google Scholar] [CrossRef]
- Gracies, J.M.; Lugassy, M.; Weisz, D.J.; Vecchio, M.; Flanagan, S.; Simpson, D.M. Botulinum toxin dilution and endplate targeting in spasticity: A double-blind controlled study. Arch. Phys. Med. Rehabil. 2009, 90, 9–16.e2. [Google Scholar] [CrossRef]
- Van Campenhout, A.; Verhaegen, A.; Pans, S.; Molenaers, G. Botulinum toxin type A injections in the psoas muscle of children with cerebral palsy: Muscle atrophy after motor end plate-targeted injections. Res. Dev. Disabil. 2013, 34, 1052–1058. [Google Scholar] [CrossRef]
- Chantelot, C.; Feugas, C.; Guillem, P.; Chapnikoff, D.; Remy, F.; Fontaine, C. Innervation of the medial epicondylar muscles: An anatomic study in 50 cases. Surg. Radiol. Anat. 1999, 21, 165–168. [Google Scholar] [CrossRef]
- Hwang, K.; Jin, S.; Hwang, S.H.; Lee, K.M.; Han, S.H. Location of nerve entry points of flexor digitorum profundus. Surg. Radiol. Anat. 2007, 29, 617–621. [Google Scholar] [CrossRef]
- Roberts, C.; Crystal, R.; Eastwood, D.M. Optimal injection points for the neuromuscular blockade of forearm flexor muscles: A cadaveric study. J. Pediatr. Orthop. B 2006, 15, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Verschuuren, J.; Strijbos, E.; Vincent, A. Neuromuscular junction disorders. Handb. Clin. Neurol. 2016, 133, 447–466. [Google Scholar] [CrossRef]
- Elgellaie, A.; Ashcroft, E.; Larkin, T.A. Morphology and anatomical relations of iliac and femoral bony landmarks, gluteal muscles and the sciatic nerve: Sex differences and clinical implications. Eur. J. Anat. 2019, 23, 377–382. [Google Scholar]
- McAndrew, D.; Gorelick, M.; Brown, J.M.M. Muscles within Muscles: A Mechanomyographic Analysis of Muscle Segment Contractile Properties within Human Gluteus Maximus. J. Musculoskelet. Res. 2006, 10, 23–35. [Google Scholar] [CrossRef]
- Reiman, M.P.; Bolgla, L.A.; Loudon, J.K. A literature review of studies evaluating gluteus maximus and gluteus medius activation during rehabilitation exercises. Physiother. Theory Pract. 2012, 28, 257–268. [Google Scholar] [CrossRef]
- Semciw, A.I.; Pizzari, T.; Murley, G.S.; Green, R.A. Gluteus medius: An intramuscular EMG investigation of anterior, middle and posterior segments during gait. J. Electromyogr. Kinesiol. 2013, 23, 858–864. [Google Scholar] [CrossRef]
- Yang, H.M.; Won, S.Y.; Lee, Y.I.; Kim, H.J.; Hu, K.S. The Sihler staining study of the infraorbital nerve and its clinical complication. J. Craniofac. Surg. 2014, 25, 2209–2213. [Google Scholar] [CrossRef]
- Wu, J.; Cai, Y.; Cao, A.; Bi, Y.; Hu, X.; Yang, S. Recommendation of the Best Site Based on the Distribution Pattern of Extramuscular and Intramusular Nerves for Gluteal Muscle Injection. Int. J. Morphol. 2020, 38, 975–982. [Google Scholar] [CrossRef]
- Sadikoglu, F.; Kavalcioglu, C.; Dagman, B. Electromyogram (EMG) signal detection, classification of EMG signals and diagnosis of neuropathy muscle disease. Procedia Comput. Sci. 2017, 120, 422–429. [Google Scholar] [CrossRef]
- Boon, A.J.; Oney-Marlow, T.M.; Murthy, N.S.; Harper, C.M.; McNamara, T.R.; Smith, J. Accuracy of electromyography needle placement in cadavers: Non-guided vs. ultrasound guided. Muscle Nerve 2011, 44, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Jin, T.G.; D’Andrea, D.; Ajroud-Driss, S.; Franz, C.K. The accuracy of needle electrode placement by trainees in selected forearm muscles using verification by neuromuscular ultrasound. J. Electromyogr. Kinesiol. 2021, 60, 102573. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Santamato, A.; Chemello, E.; Cinone, N.; Cisari, C.; Gandolfi, M.; Ranieri, M.; Smania, N.; Baricich, A. Adjuvant treatments associated with botulinum toxin injection for managing spasticity: An overview of the literature. Ann. Phys. Rehabil. Med. 2019, 62, 291–296. [Google Scholar] [CrossRef]
- Balasubramanian, C.K.; Boulias, C.; Davidson, C.; Holz, A.; Ismail, F.; Phadke, C.P. Adverse Clinical Effects of Botulinum Toxin Intramuscular Injections for Spasticity. Can. J. Neurol. Sci./J. Can. Des Sci. Neurol. 2016, 43, 298–310. [Google Scholar] [CrossRef]
- Ondo, W.G.; Vuong, K.D.; Derman, H.S. Botulinum toxin A for chronic daily headache: A randomized, placebo-controlled, parallel design study. Cephalalgia 2004, 24, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Chuang, F.C.; Yang, T.H.; Kuo, H.C. Botulinum toxin A injection in the treatment of chronic pelvic pain with hypertonic pelvic floor in women: Treatment techniques and results. Low. Urin. Tract Symptoms 2021, 13, 5–12. [Google Scholar] [CrossRef]
- Roldán-Chicano, M.T.; Rodríguez-Tello, J.; Cebrián-López, R.; Moore, J.R.; Del Mar García-López, M. Adverse effects of dorsogluteal intramuscular injection versus ventrogluteal intramuscular injection: A systematic review and meta-analysis. Nurs. Open 2023, 10, 5975–5988. [Google Scholar] [CrossRef]
- Koscielniak-Nielsen, Z.J. Ultrasound-guided peripheral nerve blocks: What are the benefits? Acta Anaesthesiol. Scand. 2008, 52, 727–737. [Google Scholar] [CrossRef]
- Chang, K.V.; Mezian, K.; Naňka, O.; Wu, W.T.; Lou, Y.M.; Wang, J.C.; Martinoli, C.; Özçakar, L. Ultrasound Imaging for the Cutaneous Nerves of the Extremities and Relevant Entrapment Syndromes: From Anatomy to Clinical Implications. J. Clin. Med. 2018, 7, 457. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Proportion within the Gluteus Maximus | Cranial Segment | Middle Segment | Caudal Segment |
|---|---|---|---|
| 0–10% | 4/20 (20%) | 0/20 (0%) | 4/20 (20%) |
| 10–20% | 8/20 (40%) | 0/20 (0%) | 4/20 (20%) |
| 20–30% | 20/20 (100%) | 12/20 (60%) | 16/20 (80%) |
| 30–40% | 20/20 (100%) | 16/20 (80%) | 20/20 (100%) |
| 40–50% | 20/20 (100%) | 20/20 (100%) | 20/20 (100%) |
| 50–60% | 20/20 (100%) | 20/20 (100%) | 20/20 (100%) |
| 60–70% | 20/20 (100%) | 20/20 (100%) | 20/20 (100%) |
| 70–80% | 8/20 (40%) | 12/20 (60%) | 12/20 (60%) |
| 80–90% | 8/20 (40%) | 4/20 (20%) | 8/20 (40%) |
| 90–100% | 4/20 (20%) | 4/20 (20%) | 0/20 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, K.-H.; Kim, D.C.; Lee, S.; Lee, H.-J.; Lee, J.-H. Intramuscular Neural Distribution of the Gluteus Maximus Muscle: Diagnostic Electromyography and Injective Treatments. Diagnostics 2024, 14, 140. https://doi.org/10.3390/diagnostics14020140
Yi K-H, Kim DC, Lee S, Lee H-J, Lee J-H. Intramuscular Neural Distribution of the Gluteus Maximus Muscle: Diagnostic Electromyography and Injective Treatments. Diagnostics. 2024; 14(2):140. https://doi.org/10.3390/diagnostics14020140
Chicago/Turabian StyleYi, Kyu-Ho, Dong Chan Kim, Siyun Lee, Hyung-Jin Lee, and Ji-Hyun Lee. 2024. "Intramuscular Neural Distribution of the Gluteus Maximus Muscle: Diagnostic Electromyography and Injective Treatments" Diagnostics 14, no. 2: 140. https://doi.org/10.3390/diagnostics14020140
APA StyleYi, K.-H., Kim, D. C., Lee, S., Lee, H.-J., & Lee, J.-H. (2024). Intramuscular Neural Distribution of the Gluteus Maximus Muscle: Diagnostic Electromyography and Injective Treatments. Diagnostics, 14(2), 140. https://doi.org/10.3390/diagnostics14020140