
A Rapid Increase in Serum Lactate Levels after Cardiovascular Surgery Is Associated with Postoperative Serious Adverse Events: A Single Center Retrospective Study

Abstract
1. Introduction
2. Materials and Methods
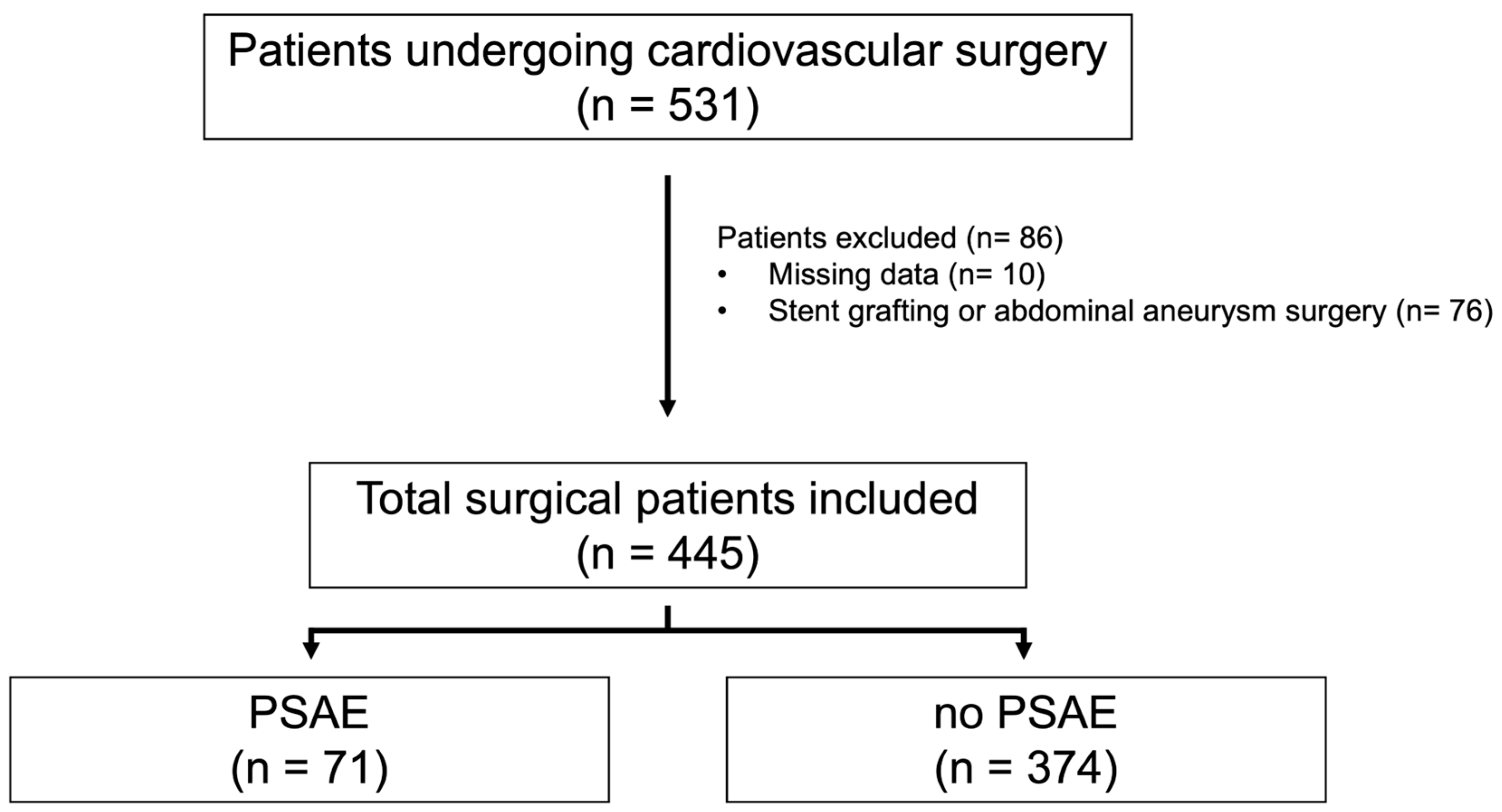
2.1. Patients
2.2. Data Collection
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maillet, J.-M.; Le Besnerais, P.; Cantoni, M.; Nataf, P.; Ruffenach, A.; Lessana, A.; Brodaty, D. Frequency, risk factors, and outcome of hyperlactatemia after cardiac surgery. Chest 2003, 123, 1361–1366. [Google Scholar] [CrossRef] [PubMed]
- Minton, J.; Sidebotham, D.A. Hyperlactatemia and cardiac surgery. J. Extra Corpor. Technol. 2017, 49, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Renew, J.R.; Barbara, D.W.; Hyder, J.A.; Dearani, J.A.; Rivera, M.; Pulido, J.N. Frequency and outcomes of severe hyperlactatemia after elective cardiac surgery. J. Thorac. Cardiovasc. Surg. 2016, 151, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Kraut, J.A.; Madias, N.E. Lactic acidosis. N. Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef] [PubMed]
- Nichol, A.; Bailey, M.; Egi, M.; Pettila, V.; French, C.; Stachowski, E.; Reade, M.C.; Cooper, D.J.; Bellomo, R. Dynamic lactate indices as predictors of outcome in critically ill patients. Crit. Care 2011, 15, R242. [Google Scholar] [CrossRef] [PubMed]
- Bakker, J.; Gris, P.; Coffernils, M.; Kahn, R.J.; Vincent, J.L. Serial blood lactate levels can predict the development of multiple organ failure following septic shock. Am. J. Surg. 1996, 171, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, L.A.; Almeida, J.P.; Fukushima, J.T.; Rhodes, A.; Vincent, J.-L.; Osawa, E.A.; Galas, F.R.B.G. High lactate levels are predictors of major complications after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2013, 146, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Mak, N.T.J.J.; Iqbal, S.; de Varennes, B.; Khwaja, K. Outcomes of post-cardiac surgery patients with persistent hyperlactatemia in the intensive care unit: A matched cohort study. J. Cardiothorac. Surg. 2016, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, T.; Egi, M.; Shimizu, K.; Toda, Y.; Iwasaki, T.; Morimatsu, H. Intraoperative change of lactate level is associated with postoperative outcomes in pediatric cardiac surgery patients: Retrospective observational study. BMC Anesthesiol. 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Suistomaa, M.; Ruokonen, E.; Kari, A.; Takala, J. Time-pattern of lactate and lactate to pyruvate ratio in the first 24 hours of intensive care emergency admissions. Shock 2000, 14, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Desebbe, O.; Montemont, C.; Gibot, S. Increased aerobic glycolysis through beta2 stimulation is a common mechanism involved in lactate formation during shock states. Shock 2008, 30, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Blohm, E.; Lai, J.; Neavyn, M. Drug-induced hyperlactatemia. Clin. Toxicol. 2017, 55, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Haanschoten, M.C.; Kreeftenberg, H.G.; Arthur Bouwman, R.; van Straten, A.H.M.; Buhre, W.F.; Soliman Hamad, M.A. Use of postoperative peak arterial lactate level to predict outcome after cardiac surgery. J. Cardiothorac. Vasc. Anesth 2017, 31, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, K.; Suzuki, M.; Yonemoto, N.; Hori, S.; Tamura, T.; Sakurai, A.; Tahara, Y.; Nagao, K.; Yaguchi, A.; Morimura, N.; et al. Early lactate clearance is associated with improved outcomes in patients with postcardiac arrest syndrome: A prospective, multicenter observational study (SOS-KANTO 2012 study). Crit. Care Med. 2017, 45, e559–e566. [Google Scholar] [CrossRef] [PubMed]
- Donnino, M.W.; Andersen, L.W.; Giberson, T.; Gaieski, D.F.; Abella, B.S.; Peberdy, M.A.; Rittenberger, J.C.; Callaway, C.W.; Ornato, J.; Clore, J.; et al. Initial lactate and lactate change in post-cardiac arrest: A multicenter validation study. Crit. Care Med. 2014, 42, 1804–1811. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Quintairos, E.; Silva, A.; Couto, L.; Taccone, F.S. The value of blood lactate kinetics in critically ill patients: A systematic review. Crit. Care 2016, 20, 257. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | PSAEs (n = 71) | No PSAEs (n = 374) | p |
|---|---|---|---|
| Preoperative | |||
| Sex (% male) | 60.6 | 60.4 | >0.99 |
| Age (y) (IQR) | 70 (62–77) | 71 (64–76) | 0.94 |
| Hypertension (%) | 56.3 | 56.8 | 0.94 |
| Diabetes mellitus (%) | 18.3 | 23.3 | 0.35 |
| Dyslipidemia (%) | 16.9 | 23.8 | 0.20 |
| eGFR (% <60 mL/min/1.73 m2) | 53.5 | 46.8 | 0.30 |
| Hb (g/dL) (IQR) | 12 (10.9–13.2) | 12.7 (11.5–13.9) | 0.02 |
| Urgent surgery (%) | 39.4 | 13.9 | <0.001 |
| Type of surgery | |||
| Single valve surgery (n) (%) | 7 (9.0) | 71 (91.0) | |
| Single valve surgery + CABG (n) (%) | 6 (18.2) | 27 (81.8) | |
| Multiple valve surgery (n) (%) | 5 (15.6) | 27 (84.4) | |
| Multiple valve surgery + CABG (n) (%) | 3 (33.3) | 6 (66.7) | |
| CABG (n) (%) | 0 (0) | 3 (100) | |
| Thoracic aortic surgery (n) (%) | 45 (19.7) | 183 (80.3) | |
| Other surgery (n) (%) | 5 (8.2) | 56 (91.8) | |
| Intraoperative | |||
| CPB (min) (IQR) | 208 (146–271) | 172 (116–220) | <0.001 |
| Cross-clamp (min) (IQR) | 94 (40–156) | 93 (0–140) | 0.28 |
| Circulatory arrest (min) (IQR) | 0 (0–57) | 0 (0–49.75) | 0.098 |
| RBC (mL) (IQR) | 1960 (840–3360) | 1120 (560–1820) | <0.001 |
| FFP (mL) (IQR) | 1440 (960–2160) | 960 (480–1440) | <0.001 |
| PC (mL) (IQR) | 250 (250–250) | 250 (0–250) | <0.001 |
| Blood salvage (mL) (IQR) | 0 (0–0) | 0 (0–460) | 0.0073 |
| Albumin (mL) (IQR) | 0 (0–500) | 0 (0–500) | 0.061 |
| Hemorrhage (mL) (IQR) | 2300 (830–3430) | 1535 (565–2500) | 0.0022 |
| Urine (mL) (IQR) | 1100 (475–1800) | 1000 (626–1596) | 0.72 |
| Peak Lac (mmol/L) (IQR) | 3.1 (1.8–5.0) | 2.1 (1.3–3.3) | <0.001 |
| Postoperative | |||
| Lac in ICU admission (mmol/L) (IQR) | 2.7 (1.8–4.3) | 2 (1.2–3.2) | <0.001 |
| ICU peak Lac (mmol/L) (IQR) | 4 (2.9–6.1) | 3.1 (2.3–4.4) | <0.001 |
| ICU ΔLac (mmol/L) (IQR) | 1.0 (0.5–1.6) | 0.8 (0.3–1.3) | 0.02 |
| Mechanical ventilation (d) (IQR) | 2 (2–4) | 1 (1–2) | <0.001 |
| ICU stay (d) (IQR) | 3 (2–5) | 2 (2–2) | <0.001 |
| Hospital stay (d) (IQR) | 35 (24–59) | 22 (18–29) | <0.001 |
| 28 d mortality (%) (n) | 7.3 (5) | 0.3 (1) | <0.001 |
| 90 d mortality (%) (n) | 12.7 (8) | 0.9 (3) | <0.001 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Sex, male | 1.0 (0.60–1.69) | 0.98 | 1.12 (0.64–1.97) | 0.70 |
| Age | 0.99 (0.98–1.02) | 0.94 | 1.00 (0.97–1.02) | 0.83 |
| Urgent surgery | 4.03 (2.31–8.05) | <0.01 | 3.45 (1.84–6.47) | <0.01 |
| Type of surgery, vascular | 2.04 (1.20–3.48) | <0.01 | 1.05 (0.56–1.96) | 0.88 |
| CPB | 1.01 (1.00–1.01) | 0.01 | 1.00 (1.00–1.01) | <0.01 |
| ICU peak Lac ≧ 3 mmol/L | 2.40 (1.36–4.26) | <0.01 | 1.43 (0.75–2.75) | 0.28 |
| ΔLac ≧ 2 mmol/L | 2.61 (1.25–5.45) | 0.01 | 2.35 (1.04–5.31) | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikuchi, K.; Kazuma, S.; Masuda, Y. A Rapid Increase in Serum Lactate Levels after Cardiovascular Surgery Is Associated with Postoperative Serious Adverse Events: A Single Center Retrospective Study. Diagnostics 2024, 14, 2082. https://doi.org/10.3390/diagnostics14182082
Kikuchi K, Kazuma S, Masuda Y. A Rapid Increase in Serum Lactate Levels after Cardiovascular Surgery Is Associated with Postoperative Serious Adverse Events: A Single Center Retrospective Study. Diagnostics. 2024; 14(18):2082. https://doi.org/10.3390/diagnostics14182082
Chicago/Turabian StyleKikuchi, Kenichiro, Satoshi Kazuma, and Yoshiki Masuda. 2024. "A Rapid Increase in Serum Lactate Levels after Cardiovascular Surgery Is Associated with Postoperative Serious Adverse Events: A Single Center Retrospective Study" Diagnostics 14, no. 18: 2082. https://doi.org/10.3390/diagnostics14182082
APA StyleKikuchi, K., Kazuma, S., & Masuda, Y. (2024). A Rapid Increase in Serum Lactate Levels after Cardiovascular Surgery Is Associated with Postoperative Serious Adverse Events: A Single Center Retrospective Study. Diagnostics, 14(18), 2082. https://doi.org/10.3390/diagnostics14182082