
Nationwide Real-World Data of Microsatellite Instability and/or Mismatch Repair Deficiency in Cancer: Prevalence and Testing Patterns

 , , , , ,
, , , , ,  and
and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Patients and Methods
2.1. Participating Centers/Laboratories
2.2. Data Collection
2.3. Statistical Analysis
3. Results
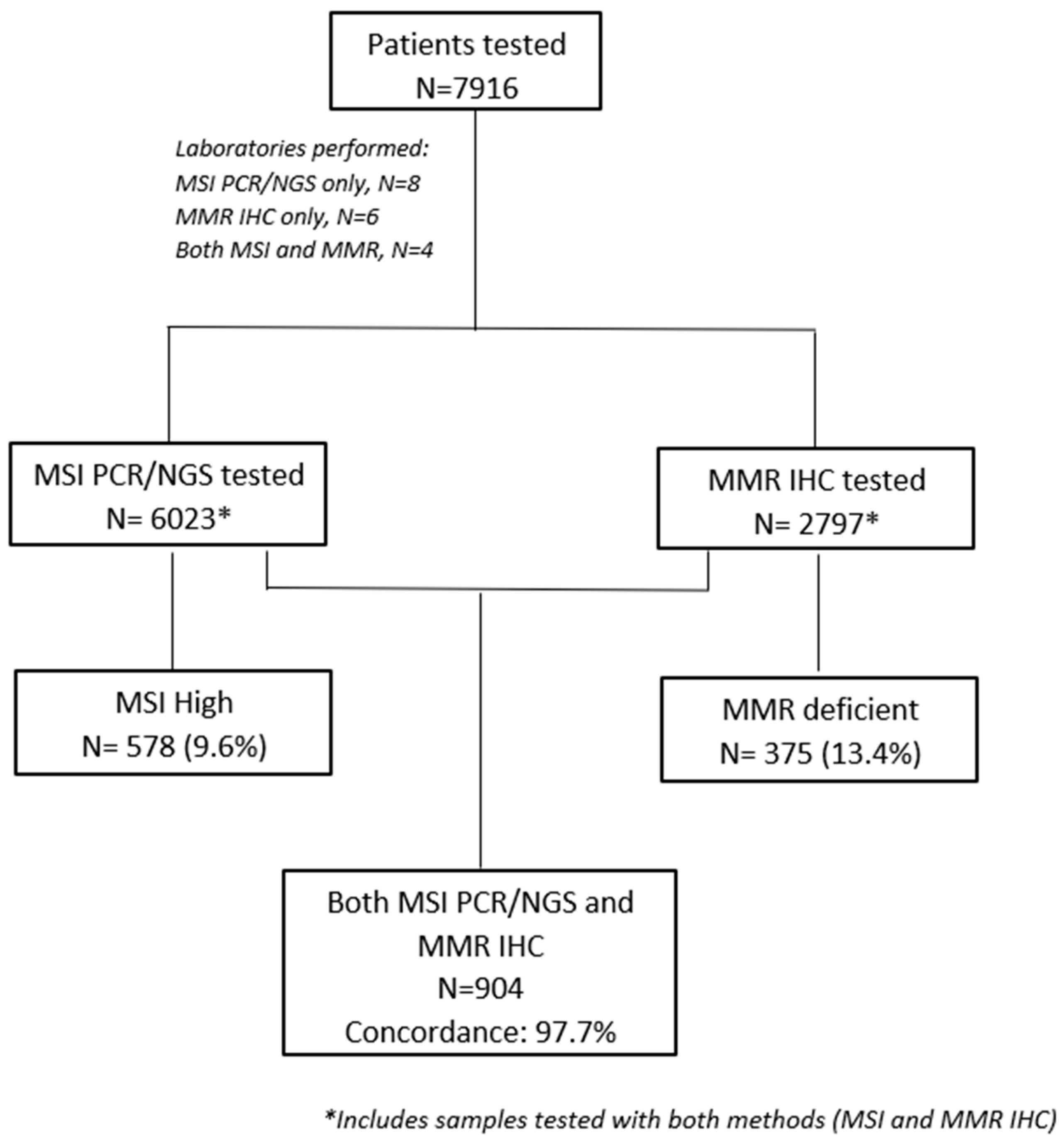
3.1. MSI/MMR Prevalence
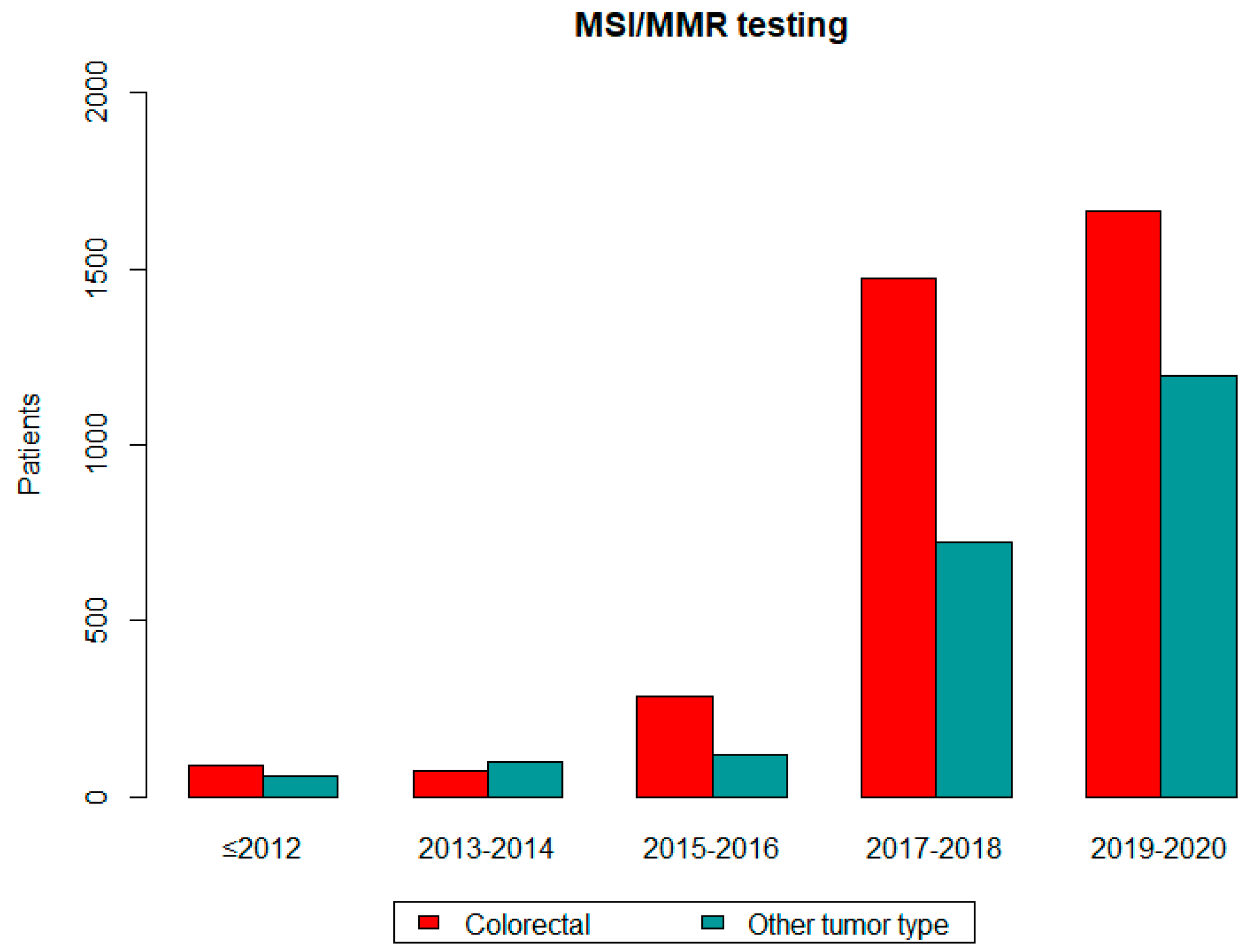
3.2. Referring Patterns
3.3. MSI and MMR Status Concordance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zaanan, A.; Shi, Q.; Taieb, J.; Alberts, S.R.; Meyers, J.P.; Smyrk, T.C.; Julie, C.; Zawadi, A.; Tabernero, J.; Mini, E.; et al. Role of Deficient DNA Mismatch Repair Status in Patients With Stage III Colon Cancer Treated With FOLFOX Adjuvant Chemotherapy: A Pooled Analysis from 2 Randomized Clinical Trials. JAMA Oncol. 2018, 4, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, H.; Zaanan, A.; Sinicrope, F.A. Implications of mismatch repair-deficient status on management of early stage colorectal cancer. J. Gastrointest. Oncol. 2015, 6, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, F.A.; Mahoney, M.R.; Smyrk, T.C.; Thibodeau, S.N.; Warren, R.S.; Bertagnolli, M.M.; Nelson, G.D.; Goldberg, R.M.; Sargent, D.J.; Alberts, S.R. Prognostic impact of deficient DNA mismatch repair in patients with stage III colon cancer from a randomized trial of FOLFOX-based adjuvant chemotherapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 3664–3672. [Google Scholar] [CrossRef] [PubMed]
- Sargent, D.J.; Marsoni, S.; Monges, G.; Thibodeau, S.N.; Labianca, R.; Hamilton, S.R.; French, A.J.; Kabat, B.; Foster, N.R.; Torri, V.; et al. Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3219–3226. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, F.A. DNA mismatch repair and adjuvant chemotherapy in sporadic colon cancer. Nat. Rev. Clin. Oncol. 2010, 7, 174–177. [Google Scholar] [CrossRef]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef]
- André, T.; Shiu, K.K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Oaknin, A.; Gilbert, L.; Tinker, A.V.; Brown, J.; Mathews, C.; Press, J.; Sabatier, R.; O’Malley, D.M.; Samouelian, V.; Boni, V.; et al. Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-H) or proficient/stable (MMRp/MSS) endometrial cancer: Interim results from GARNET-a phase I, single-arm study. J. Immunother. Cancer 2022, 10, e003777. [Google Scholar] [CrossRef]
- Lenz, H.J.; Van Cutsem, E.; Luisa Limon, M.; Wong, K.Y.M.; Hendlisz, A.; Aglietta, M.; García-Alfonso, P.; Neyns, B.; Luppi, G.; Cardin, D.B.; et al. First-Line Nivolumab Plus Low-Dose Ipilimumab for Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: The Phase II CheckMate 142 Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Hampel, H.; Frankel, W.L.; Martin, E.; Arnold, M.; Khanduja, K.; Kuebler, P.; Clendenning, M.; Sotamaa, K.; Prior, T.; Westman, J.A.; et al. Feasibility of screening for Lynch syndrome among patients with colorectal cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 5783–5788. [Google Scholar] [CrossRef]
- Bonneville, R.; Krook, M.A.; Kautto, E.A.; Miya, J.; Wing, M.R.; Chen, H.Z.; Reeser, J.W.; Yu, L.; Roychowdhury, S. Landscape of Microsatellite Instability Across 39 Cancer Types. JCO Precis. Oncol. 2017, 2017, PO.17.00073. [Google Scholar] [CrossRef]
- Kang, Y.J.; O’Haire, S.; Franchini, F.; IJzerman, M.; Zalcberg, J.; Macrae, F.; Canfell, K.; Steinberg, J. A scoping review and meta-analysis on the prevalence of pan-tumour biomarkers (dMMR, MSI, high TMB) in different solid tumours. Sci. Rep. 2022, 12, 20495. [Google Scholar] [CrossRef]
- Latham, A.; Srinivasan, P.; Kemel, Y.; Shia, J.; Bandlamudi, C.; Mandelker, D.; Middha, S.; Hechtman, J.; Zehir, A.; Dubard-Gault, M.; et al. Microsatellite Instability Is Associated With the Presence of Lynch Syndrome Pan-Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 286–295. [Google Scholar] [CrossRef]
- Vilar, E.; Mork, M.E.; Cuddy, A.; Borras, E.; Bannon, S.A.; Taggart, M.W.; Ying, J.; Broaddus, R.R.; Luthra, R.; Rodriguez-Bigas, M.A.; et al. Role of microsatellite instability-low as a diagnostic biomarker of Lynch syndrome in colorectal cancer. Cancer Genet. 2014, 207, 495–502. [Google Scholar] [CrossRef]
- Pearlman, R.; Frankel, W.L.; Swanson, B.J.; Jones, D.; Zhao, W.; Yilmaz, A.; Miller, K.; Bacher, J.; Bigley, C.; Nelsen, L.; et al. Prospective Statewide Study of Universal Screening for Hereditary Colorectal Cancer: The Ohio Colorectal Cancer Prevention Initiative. JCO Precis. Oncol. 2021, 5, PO.20.00525. [Google Scholar] [CrossRef]
- Hampel, H.; Pearlman, R.; de la Chapelle, A.; Pritchard, C.C.; Zhao, W.; Jones, D.; Yilmaz, A.; Chen, W.; Frankel, W.L.; Suarez, A.A.; et al. Double somatic mismatch repair gene pathogenic variants as common as Lynch syndrome among endometrial cancer patients. Gynecol. Oncol. 2021, 160, 161–168. [Google Scholar] [CrossRef]
- Guyot D’Asnières De Salins, A.; Tachon, G.; Cohen, R.; Karayan-Tapon, L.; Junca, A.; Frouin, E.; Godet, J.; Evrard, C.; Randrian, V.; Duval, A.; et al. Discordance between immunochemistry of mismatch repair proteins and molecular testing of microsatellite instability in colorectal cancer. ESMO Open 2021, 6, 100120. [Google Scholar] [CrossRef]
- Mi, M.; Ye, C.; Yuan, Y. Neoadjuvant PD-1 blockade: A promising nonoperative strategy for mismatch repair-deficient, locally advanced rectal cancer. Signal Transduct. Target. Ther. 2022, 7, 361. [Google Scholar] [CrossRef]
- Ryan, N.A.J.; Davison, N.J.; Payne, K.; Cole, A.; Evans, D.G.; Crosbie, E.J. A Micro-Costing Study of Screening for Lynch Syndrome-Associated Pathogenic Variants in an Unselected Endometrial Cancer Population: Cheap as NGS Chips? Front. Oncol. 2019, 9, 61. [Google Scholar] [CrossRef]
- Kang, Y.J.; Killen, J.; Caruana, M.; Simms, K.; Taylor, N.; Frayling, I.M.; Snowsill, T.; Huxley, N.; Coupe, V.M.; Hughes, S.; et al. The predicted impact and cost-effectiveness of systematic testing of people with incident colorectal cancer for Lynch syndrome. Med. J. Aust. 2020, 212, 72–81. [Google Scholar] [CrossRef]
- Gutierrez, C.; Ogino, S.; Meyerhardt, J.A.; Iorgulescu, J.B. The Prevalence and Prognosis of Microsatellite Instability-High/Mismatch Repair-Deficient Colorectal Adenocarcinomas in the United States. JCO Precis. Oncol. 2023, 7, e2200179. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Factor * | Total (N = 7916) | MSS and/or pMMR (N = 7078) | MSI-H and/or dMMR (N = 838) |
|---|---|---|---|
| Age at testing Median (IQR) (N = 5577) | 66.4 (15.9) | 66.3 (15.7) | 67.4 (17.8) |
| Gender (N = 6639) | |||
| Female | 2967 (44.7%) | 2643 (89.1%) | 324 (10.9%) |
| Male | 3672 (55.3%) | 3334 (90.8%) | 338 (9.2%) |
| Cancer type (N = 7820) | |||
| Colorectal | 5068 (64.8%) | 4456 (87.9%) | 612 (12.1%) |
| Endometrial | 225 (2.9%) | 178 (79.1%) | 47 (20.9%) |
| Other tumor type | 2527 (32.3%) | 2362 (93.5%) | 165 (6.5%) |
| Other GI ** | 478 (18.9%) | 440 (92.1%) | 38 (7.9%) |
| Lung | 276 (10.9%) | 268 (97.1%) | 8 (2.9%) |
| Pancreas | 296 (11.7%) | 289 (97.6%) | 7 (2.4%) |
| Other gynecological º | 150 (5.9%) | 145 (96.7%) | 5 (3.3%) |
| Prostate | 91 (3.6%) | 86 (94.5%) | 5 (5.5%) |
| Breast | 93 (3.7%) | 90 (96.8%) | 3 (3.2%) |
| Liver | 49 (1.9%) | 45 (93.8%) | 4 (8.3%) |
| CNS | 25 (1.0%) | 25 (100%) | 0 (0.0%) |
| Genitourinary | 28 (1.1%) | 25 (89.3%) | 3 (10.7%) |
| Melanoma | 12 (0.5%) | 12 (100%) | 0 (0.0%) |
| HNC | 13 (0.5%) | 13 (100%) | 0 (0.0%) |
| Sarcoma | 16 (0.6%) | 15 (93.8%) | 1 (6.3%) |
| Adrenal Gland | 2 (0.1%) | 1 (50.0%) | 1 (50.0%) |
| GIST | 4 (0.2%) | 4 (100%) | 0 (0.0%) |
| Lymphoma | 1 (0.04%) | 1 (100%) | 0 (0.0%) |
| Mesothelioma | 4 (0.2%) | 4 (100%) | 0 (0.0%) |
| Skin | 1 (0.04%) | 1 (100%) | 0 (0.0%) |
| Thymus | 3 (0.1%) | 2 (66.7%) | 1 (33.3%) |
| Thyroid | 7 (0.3%) | 7 (100%) | 0 (0.0%) |
| NET | 1 (0.04%) | 1 (100%) | 0 (0.0%) |
| Primary site not reported | 977 (38.7%) | 888 (90.9%) | 89 (9.1%) |
| Stage at diagnosis (N = 3216) | |||
| I–III | 2878 (89.5%) | 2509 (87.2%) | 369 (12.8%) |
| IV | 338 (10.5%) | 305 (90.2%) | 33 (9.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fountzilas, E.; Papadopoulos, T.; Papadopoulou, E.; Gouedard, C.; Kourea, H.P.; Constantoulakis, P.; Magkou, C.; Sfakianaki, M.; Kotoula, V.; Bantouna, D.; et al. Nationwide Real-World Data of Microsatellite Instability and/or Mismatch Repair Deficiency in Cancer: Prevalence and Testing Patterns. Diagnostics 2024, 14, 1076. https://doi.org/10.3390/diagnostics14111076
Fountzilas E, Papadopoulos T, Papadopoulou E, Gouedard C, Kourea HP, Constantoulakis P, Magkou C, Sfakianaki M, Kotoula V, Bantouna D, et al. Nationwide Real-World Data of Microsatellite Instability and/or Mismatch Repair Deficiency in Cancer: Prevalence and Testing Patterns. Diagnostics. 2024; 14(11):1076. https://doi.org/10.3390/diagnostics14111076
Chicago/Turabian StyleFountzilas, Elena, Theofanis Papadopoulos, Eirini Papadopoulou, Cedric Gouedard, Helen P. Kourea, Pantelis Constantoulakis, Christina Magkou, Maria Sfakianaki, Vassiliki Kotoula, Dimitra Bantouna, and et al. 2024. "Nationwide Real-World Data of Microsatellite Instability and/or Mismatch Repair Deficiency in Cancer: Prevalence and Testing Patterns" Diagnostics 14, no. 11: 1076. https://doi.org/10.3390/diagnostics14111076
APA StyleFountzilas, E., Papadopoulos, T., Papadopoulou, E., Gouedard, C., Kourea, H. P., Constantoulakis, P., Magkou, C., Sfakianaki, M., Kotoula, V., Bantouna, D., Raptou, G., Saetta, A. A., Christopoulou, G., Hatzibougias, D., Michalopoulou-Manoloutsiou, E., Siatra, E., Eleftheriadis, E., Kavoura, E., Kaklamanis, L., ... Saridaki, Z. (2024). Nationwide Real-World Data of Microsatellite Instability and/or Mismatch Repair Deficiency in Cancer: Prevalence and Testing Patterns. Diagnostics, 14(11), 1076. https://doi.org/10.3390/diagnostics14111076