
Trends in the Use of Second-Generation Androgen Receptor Axis Inhibitors for Metastatic Hormone-Sensitive Prostate Cancer and Clinical Factors Predicting Biological Recurrence

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Statistical Analysis
3. Results
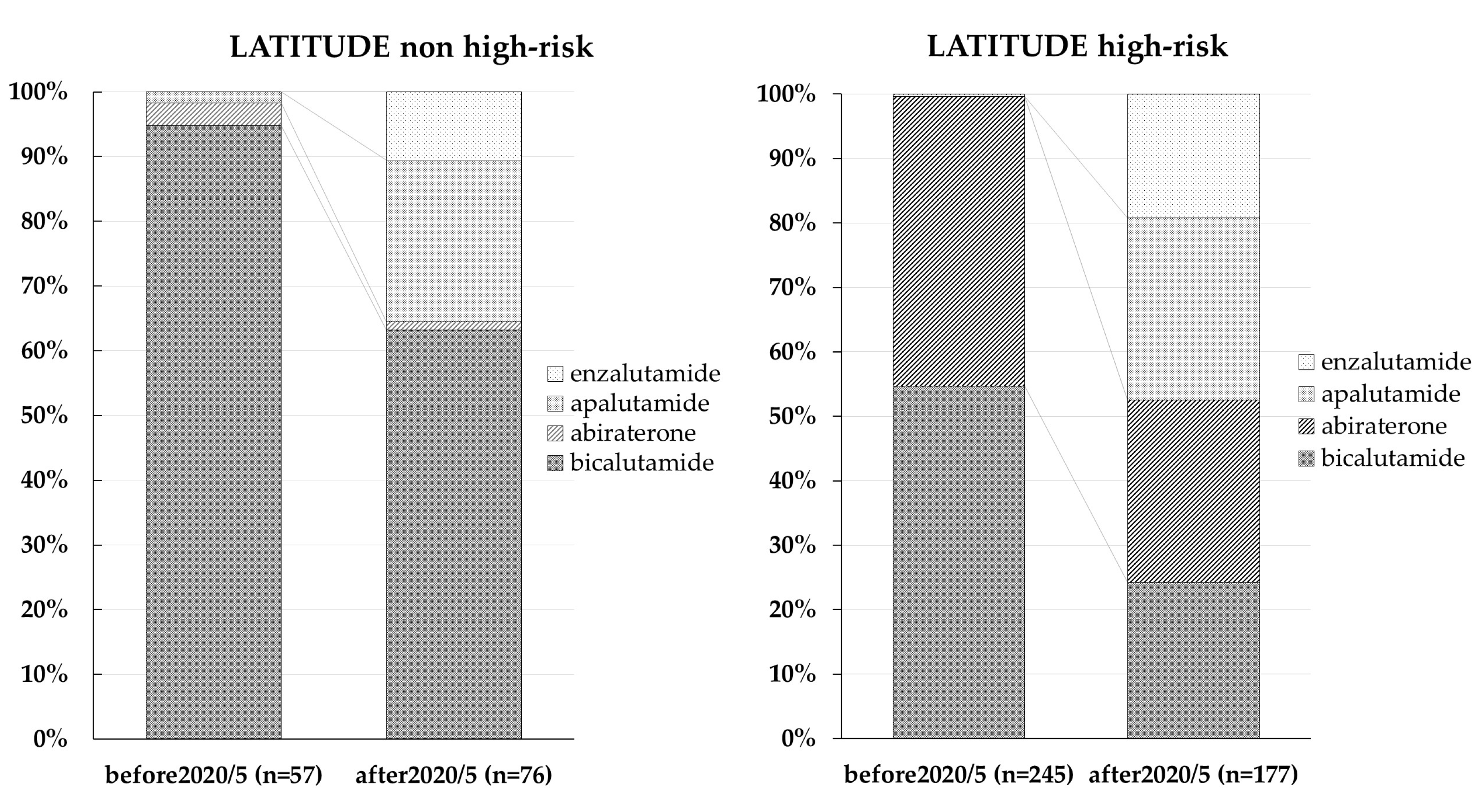
3.1. Trends in ARAT Agent Use
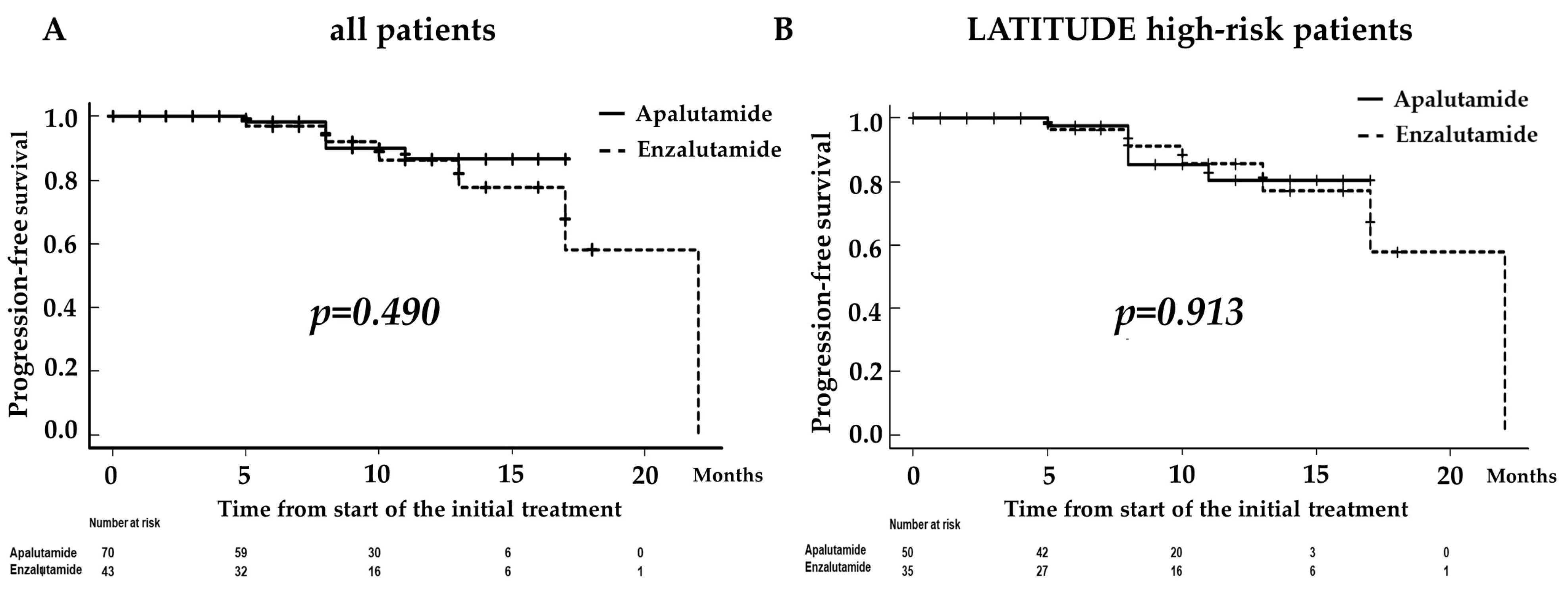
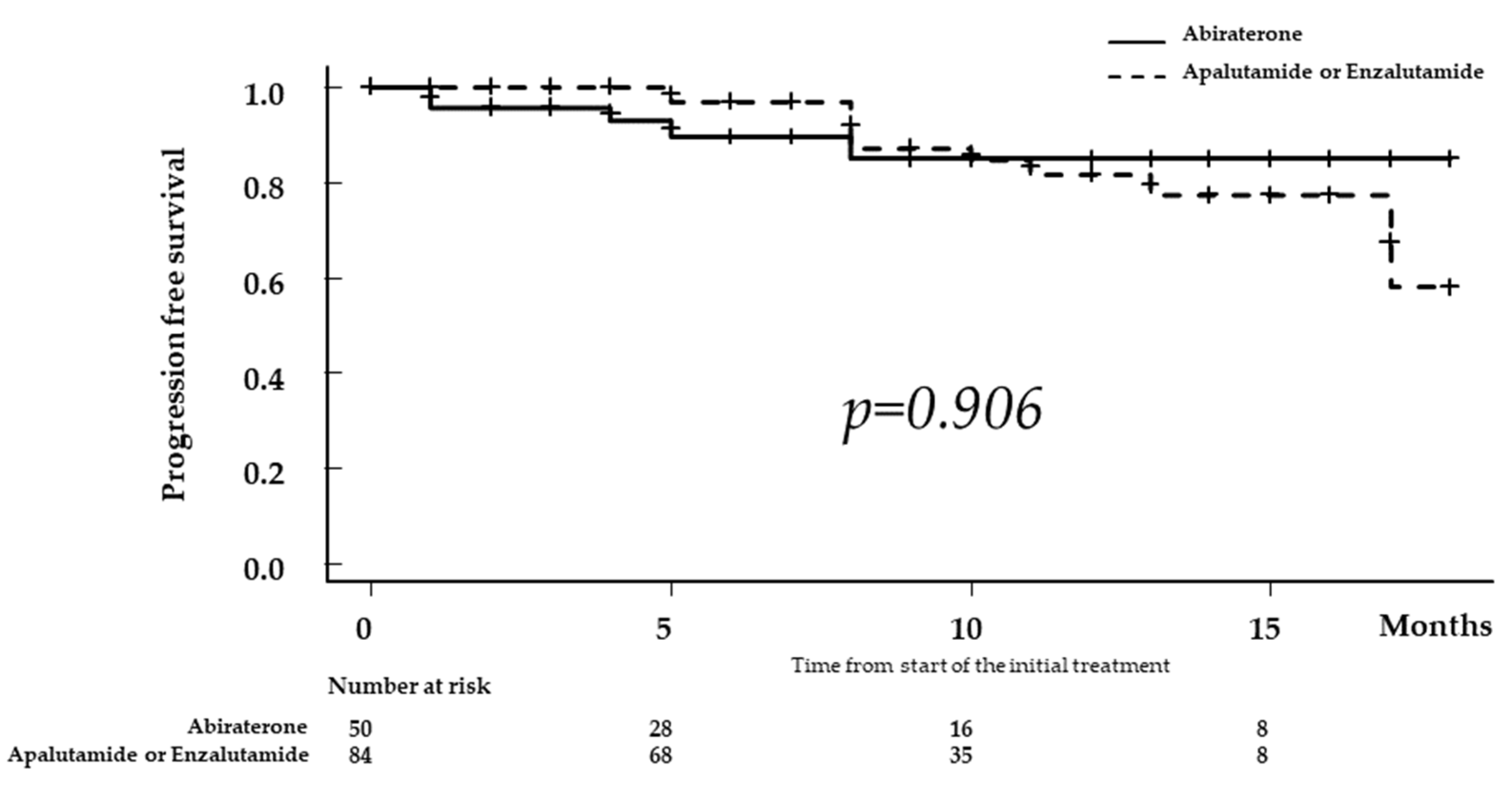
3.2. Comparison of Progression-Free Survival according to ARAT
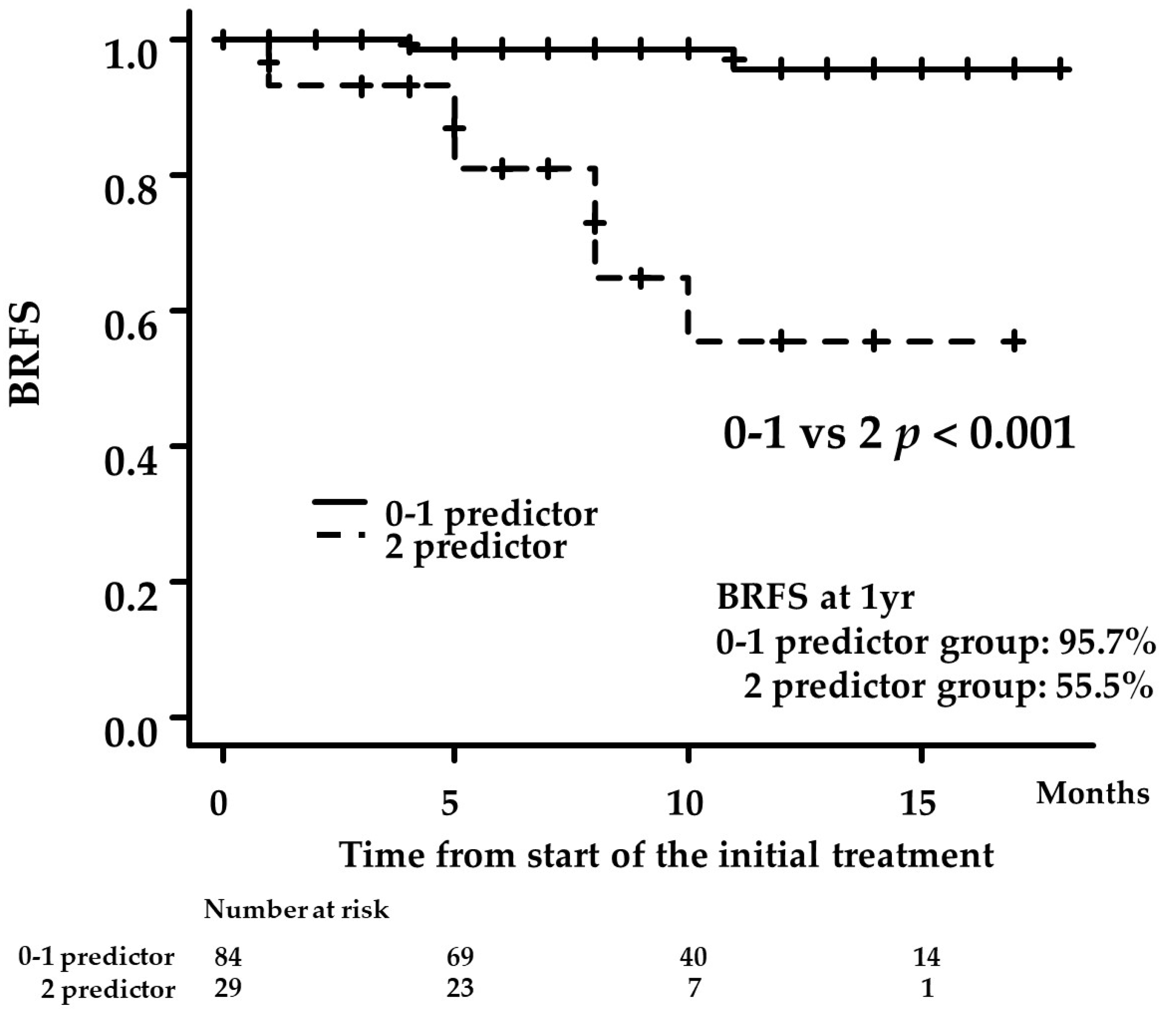
3.3. Uni- and Multivariate Analyses for Factors Predicting BCR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akaza, H.; Hinotsu, S.; Usami, M.; Arai, Y.; Kanetake, H.; Naito, S.; Hirao, Y. Combined androgen blockade with bicalutamide for advanced prostate cancer: Long-term follow-up of a phase 3, double-blind, randomized study for survival. Cancer 2009, 115, 3437–3445. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Jenkins, C.; Tannock, I.F. Should docetaxel be standard of care for patients with metastatic hormone-sensitive prostate cancer? Pro and contra. Ann. Oncol. 2015, 26, 16601667. [Google Scholar] [CrossRef] [PubMed]
- Gravis, G.; Fizazi, K.; Joly, F.; Oudard, S.; Priou, F.; Esterni, B.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): A randomised, open-label, phase 3 trial. Lancet Oncol. 2013, 14, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Miyake, H.; Matsushita, Y.; Watanabe, H.; Tamura, K.; Motoyama, D.; Ito, T.; Sugiyama, T.; Otsuka, A. Prognostic Significance of Time to Castration Resistance in Patients with Metastatic Castration-sensitive Prostate Cancer. Anticancer Res. 2019, 39, 1391–1396. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.E.; Chen, Y.H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J. Clin. Oncol. 2018, 36, 1080–1187. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; de Bono, J.S.; Spears, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Ritchie, A.W.S.; Amos, C.L.; Gilson, C.; Jones, R.J.; et al. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. N. Engl. J. Med. 2017, 377, 338–351. [Google Scholar] [CrossRef]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez Soto, Á.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy with Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations from the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [PubMed]
- Perkins, N.J.; Schisterman, E.F. The inconsistency of “optimal” cutpoints obtained using two criteria based on the receiver operating characteristic curve. Am. J. Epidemiol. 2006, 163, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Takahara, K.; Naiki, T.; Ito, T.; Nakane, K.; Koie, T.; Yasui, T.; Miyake, H.; Shiroki, R. Useful predictors of progression-free survival for Japanese patients with LATITUDE-high-risk metastatic castration-sensitive prostate cancer who received upfront abiraterone acetate. Int. J. Urol. 2022, 29, 229–234. [Google Scholar] [CrossRef]
- Naiki, T.; Takahara, K.; Ito, T.; Nakane, K.; Sugiyama, Y.; Koie, T.; Shiroki, R.; Miyake, H.; Yasui, T. Comparison of clinical outcomes between androgen deprivation therapy with up-front abiraterone and bicalutamide for Japanese patients with LATITUDE high-risk prostate cancer in a real-world retrospective analysis. Int. J. Clin. Oncol. 2022, 27, 592–601. [Google Scholar] [CrossRef] [PubMed]
- Leith, A.; Ribbands, A.; Kim, J.; Clayton, E.; Gillespie-Akar, L.; Yang, L.; Ghate, S.R. Impact of next-generation hormonal agents on treatment patterns among patients with metastatic hormone-sensitive prostate cancer: A real-world study from the United States, five European countries and Japan. BMC Urol. 2022, 22, 33. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Chen, Y.H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef]
- Chi, K.N.; Chowdhury, S.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez, A.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide in Patients with Metastatic Castration-Sensitive Prostate Cancer: Final Survival Analysis of the Randomized, Double-Blind, Phase III TITAN Study. J. Clin. Oncol. 2021, 39, 2294–2303. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef]
- Tang, L.; Li, X.; Wang, B.; Luo, G.; Gu, L.; Chen, L.; Liu, K.; Gao, Y.; Zhang, X. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Localized and Advanced Prostate Cancer: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0153981. [Google Scholar] [CrossRef]
- Tomioka-Inagawa, R.; Nakane, K.; Enomoto, T.; Tomioka, M.; Taniguchi, T.; Ishida, T.; Ozawa, K.; Takagi, K.; Ito, H.; Takeuchi, S.; et al. The Impact of Neutrophil-to-Lymphocyte Ratio after Two Courses of Pembrolizumab for Oncological Outcomes in Patients with Metastatic Urothelial Carcinoma. Biomedicines 2022, 10, 1609. [Google Scholar] [CrossRef] [PubMed]
- Iinuma, K.; Enomoto, T.; Kawada, K.; Fujimoto, S.; Ishida, T.; Takagi, K.; Nagai, S.; Ito, H.; Kawase, M.; Nakai, C.; et al. Utility of Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Systemic Immune Inflammation Index as Prognostic, Predictive Biomarkers in Patients with Metastatic Renal Cell Carcinoma Treated with Nivolumab and Ipilimumab. J. Clin. Med. 2021, 10, 5325. [Google Scholar] [CrossRef] [PubMed]
- Loubersac, T.; Nguile-Makao, M.; Pouliot, F.; Fradet, V.; Toren, P. Neutrophil-to-lymphocyte Ratio as a Predictive Marker of Response to Abiraterone Acetate: A Retrospective Analysis of the COU302 Study. Eur. Urol. Oncol. 2020, 3, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C.J.D.; Shayegan, B.; Morgan, S.C.; Hamilton, R.J.; Cagiannos, I.; Basappa, N.S.; Ferrario, C.; Gotto, G.T.; Fernandes, R.; Roy, S.; et al. Prognostic Association between Common Laboratory Tests and Overall Survival in Elderly Men with De Novo Metastatic Castration Sensitive Prostate Cancer: A Population-Based Study in Canada. Cancers 2021, 13, 2844. [Google Scholar] [CrossRef]
- Salciccia, S.; Frisenda, M.; Bevilacqua, G.; Viscuso, P.; Casale, P.; De Berardinis, E.; Di Pierro, G.B.; Cattarino, S.; Giorgino, G.; Rosati, D.; et al. Comparative Prospective and Longitudinal Analysis on the Platelet-to-Lymphocyte, Neutrophil-to-Lymphocyte, and Albumin-to-Globulin Ratio in Patients with Non-Metastatic and Metastatic Prostate Cancer. Curr. Oncol. 2022, 29, 9474–9500. [Google Scholar] [CrossRef]
- Matsubara, N.; Chi, K.N.; Özgüroğlu, M.; Rodriguez-Antolin, A.; Feyerabend, S.; Fein, L.; Alekseev, B.Y.; Sulur, G.; Protheroe, A.; Li, S.; et al. Correlation of Prostate-specific Antigen Kinetics with Overall Survival and Radiological Progression-free Survival in Metastatic Castration-sensitive Prostate Cancer Treated with Abiraterone Acetate plus Prednisone or Placebos Added to Androgen Deprivation Therapy: Post Hoc Analysis of Phase 3 LATITUDE Study. Eur. Urol. 2020, 77, 494–500. [Google Scholar]
- Tomioka, A.; Tanaka, N.; Yoshikawa, M.; Miyake, M.; Anai, S.; Chihara, Y.; Okajima, E.; Hirayama, A.; Hirao, Y.; Fujimoto, K. Nadir PSA level and time to nadir PSA are prognostic factors in patients with metastatic prostate cancer. BMC Urol. 2014, 14, 33. [Google Scholar] [CrossRef]
- Koo, K.C.; Park, S.U.; Kim, K.H.; Rha, K.H.; Hong, S.J.; Yang, S.C.; Chung, B.H. Predictors of survival in prostate cancer patients with bone metastasis and extremely high prostate-specific antigen levels. Prostate Int. 2015, 3, 10–15. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All | Abiraterone | Apalutamide | Enzalutamide | p-Value |
|---|---|---|---|---|---|
| Number of patients | 276 | 163 | 70 | 43 | |
| Age (years, median, IQR) | 73.0 (68.0–79.0) | 73.0 (68.0–79.0) | 73.5 (69.0–78.7) | 73.0 (65.5–76.0) | 0.575 |
| ECOG-PS (number, %) | 0.792 | ||||
| 0 | 198 (71.7) | 117 (71.8) | 51 (72.9) | 30 (69.8) | |
| 1 | 46 (16.7) | 24 (14.7) | 13 (18.6) | 9 (20.9) | |
| 2 | 27 (9.8) | 19 (11.7) | 5 (7.1) | 3 (7.0) | |
| 3 | 3 (1.1) | 2 (1.2) | 0 (0.0) | 1 (2.3) | |
| 4 | 2 (0.7) | 1 (0.6) | 1 (1.4) | 0 (0.0) | |
| Initial PSA (ng/mL, median, IQR) | 286.5 (68.7–1163.2) | 409.0 (78.8–1656.0) | 185.9 (57.5–598.3) | 380.4 (92.5–1011.9) | 0.05 |
| Gleason score (number, %) | 0.002 | ||||
| ≤6 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| 7 | 12 (4.3) | 1 (0.6) | 8 (11.6) | 3 (7.0) | |
| ≥8 | 262 (95.0) | 161 (99.4) | 61 (88.4) | 40 (93.0) | |
| Clinical T stage (number, %) | 0.927 | ||||
| 1c | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| 2 | 42 (15.2) | 24 (14.7) | 11 (15.7) | 7 (16.3) | |
| 3 | 134 (48.6) | 81 (49.6) | 35 (50.0) | 18 (41.9) | |
| 4 | 92 (33.3) | 55 (33.7) | 21 (30.0) | 16 (37.2) | |
| x | 8 (2.8) | 3 (1.8) | 3 (4.3) | 2 (4.7) | |
| Lymph node involvement (number, %) | 0.461 | ||||
| Negative | 111 (40.2) | 62 (38.0) | 30 (42.9) | 19 (44.2) | |
| positive | 165 (59.8) | 101 (62.0) | 40 (57.1) | 24 (55.8) | |
| Number of bone metastasis (number, %) | <0.001 | ||||
| 1 | 18 (6.5) | 5 (3.1) | 11 (16.2) | 2 (5.0) | |
| 2 | 11 (3.9) | 2 (1.2) | 7 (10.3) | 2 (5.0) | |
| ≥3 | 225 (81.5) | 144 (88.9) | 45 (66.2) | 36 (90.0) | |
| Visceral metastasis (number, %) | 93 (33.7) | 59 (36.2) | 23 (32.9) | 11 (25.6) | 0.418 |
| Patients who met the criteria for high-risk PCa in the LATITTUDE trial (number, %) | 245 (89.2) | 160 (98.2) | 50 (71.4) | 35 (81.4) | <0.001 |
| WBC (count/μL, median, IQR) | 6680 (5500–7860) | 6600 (5470–7810) | 6690 (5500–8280) | 6800 (5800–7800) | 0.668 |
| Neutrophil (count/μL, median, IQR) | 4100 (3235–5311) | 4100 (3200–5140) | 4200 (3235–5444) | 4000 (3373–5587) | 0.816 |
| Lymphocyte (count/μL, median, IQR) | 1500 (1191–1892) | 1500 (1200–1803) | 1400 (1096–1911) | 1440 (1247–2229) | 0.584 |
| NLR | 2.74 (2.00– 3.90) | 2.73 (2.00–3.82) | 2.77 (1.76–4.49) | 2.54 (1.92–3.38) | 0.860 |
| ALP (U/L, median, IQR) | 275 (174– 605) | 401 (235–923) | 213 (101–310) | 158 (102–299) | <0.001 |
| LDH (U/L, median, IQR) | 204 (178– 243) | 205 (178–248) | 198 (169–229) | 206 (182–242) | 0.397 |
| Albumin (g/dL, median, IQR) | 4.0 (3.6– 4.3) | 3.9 (3.5–4.2) | 4.1 (3.7–4.3) | 4.0 (3.8–4.3) | 0.099 |
| CRP (mg/dL, median, IQR) | 0.23 (0.06–1.06) | 0.26 (0.08–1.27) | 0.20 (0.04–1.15) | 0.19 (0.06–0.81) | 0.487 |
| Follow-up period(months, median, IQR) | 12.0 (6.0–22.5) | 19.0 (8.5–27.0) | 9.0 (7.0–12.0) | 7.0 (4.5–12.5) | <0.001 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (≥73 vs. <73 years) | 3.040 | 0.847–10.900 | 0.087 | - | - | - |
| ECOG-PS (≥1 vs. 0) | 2.140 | 0.741–6.176 | 0.159 | - | - | - |
| Albumin (≥3.8 vs. <3.8 g/dL) | 0.351 | 0.120–1.077 | 0.068 | - | - | - |
| NLR (≥2.76 vs. <2.76) | 11.690 | 1.495–91.480 | 0.019 | 9.700 | 1.2010–78.360 | 0.033 |
| Hemoglobin (≥13.1 vs. <13.1 g/dL) | 0.450 | 0.150–1.344 | 0.153 | - | - | - |
| Gleason score 5 (yes vs. no) | 1.473 | 0.461–4.703 | 0.513 | - | - | - |
| Initial PSA (≥413 vs. <413 ng/mL) | 0.745 | 0.249–2.226 | 0.599 | - | - | - |
| Time to PSA nadir (≥ 6 vs. <6 months) | 0.161 | 0.042–0.602 | 0.007 | - | - | - |
| PSA level 3 months after the start of first-line treatment (≥0.55 vs. <0.55 ng/mL) | 7.191 | 1.608–32.170 | <0.001 | 10.840 | 1.3620–86.360 | 0.024 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakane, K.; Watanabe, H.; Naiki, T.; Takahara, K.; Yasui, T.; Miyake, H.; Shiroki, R.; Koie, T. Trends in the Use of Second-Generation Androgen Receptor Axis Inhibitors for Metastatic Hormone-Sensitive Prostate Cancer and Clinical Factors Predicting Biological Recurrence. Diagnostics 2023, 13, 1661. https://doi.org/10.3390/diagnostics13091661
Nakane K, Watanabe H, Naiki T, Takahara K, Yasui T, Miyake H, Shiroki R, Koie T. Trends in the Use of Second-Generation Androgen Receptor Axis Inhibitors for Metastatic Hormone-Sensitive Prostate Cancer and Clinical Factors Predicting Biological Recurrence. Diagnostics. 2023; 13(9):1661. https://doi.org/10.3390/diagnostics13091661
Chicago/Turabian StyleNakane, Keita, Hiromitsu Watanabe, Taku Naiki, Kiyoshi Takahara, Takahiro Yasui, Hideaki Miyake, Ryoichi Shiroki, and Takuya Koie. 2023. "Trends in the Use of Second-Generation Androgen Receptor Axis Inhibitors for Metastatic Hormone-Sensitive Prostate Cancer and Clinical Factors Predicting Biological Recurrence" Diagnostics 13, no. 9: 1661. https://doi.org/10.3390/diagnostics13091661
APA StyleNakane, K., Watanabe, H., Naiki, T., Takahara, K., Yasui, T., Miyake, H., Shiroki, R., & Koie, T. (2023). Trends in the Use of Second-Generation Androgen Receptor Axis Inhibitors for Metastatic Hormone-Sensitive Prostate Cancer and Clinical Factors Predicting Biological Recurrence. Diagnostics, 13(9), 1661. https://doi.org/10.3390/diagnostics13091661