
Detection of Tumour-Targeted IRDye800CW Tracer with Commercially Available Laparoscopic Surgical Systems

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
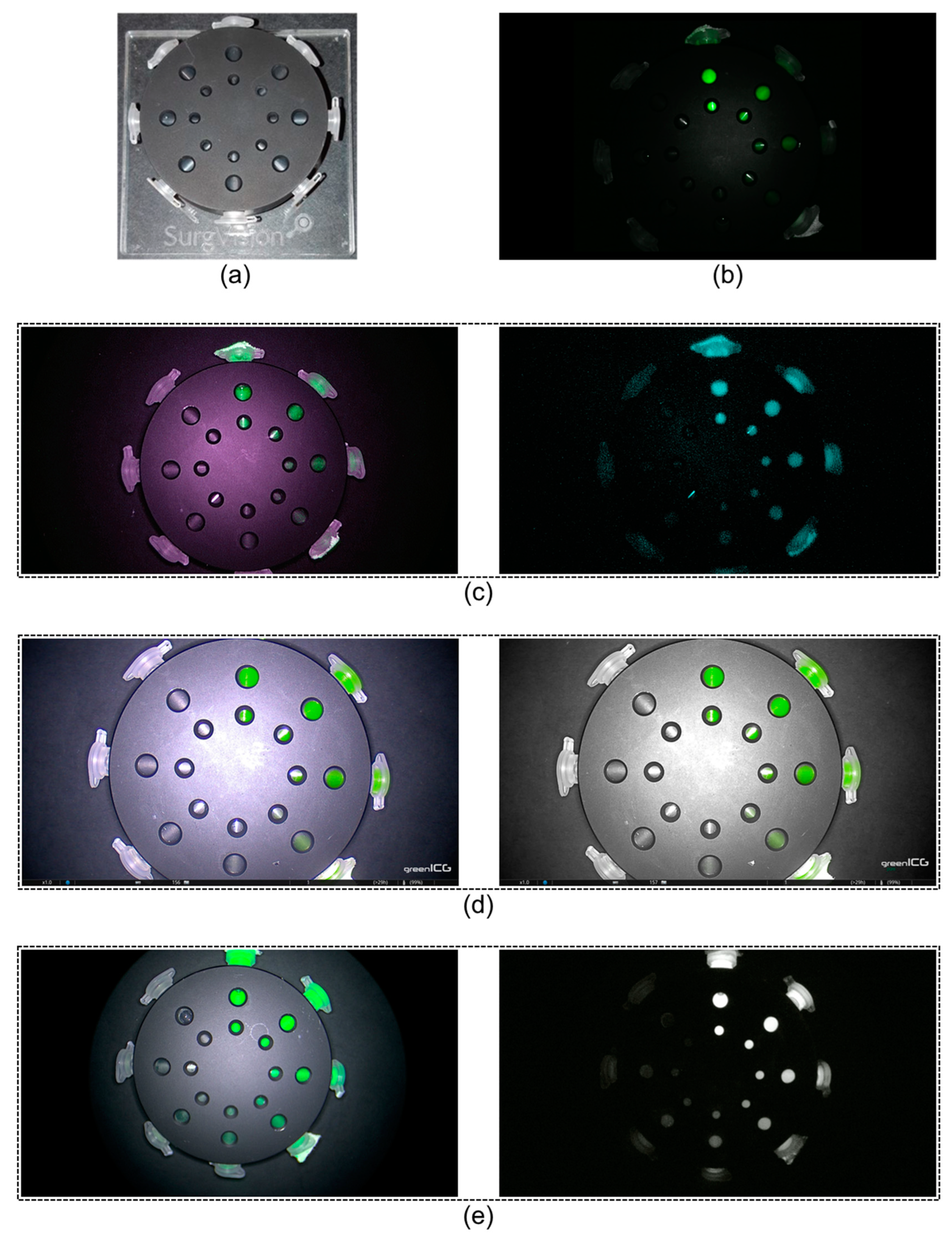
2.1. Phantom Set-Up
2.2. Laparoscopic Near-Infrared Fluorescence Systems
2.3. Measurements
2.4. Data Analyses
mean signal of background
3. Results
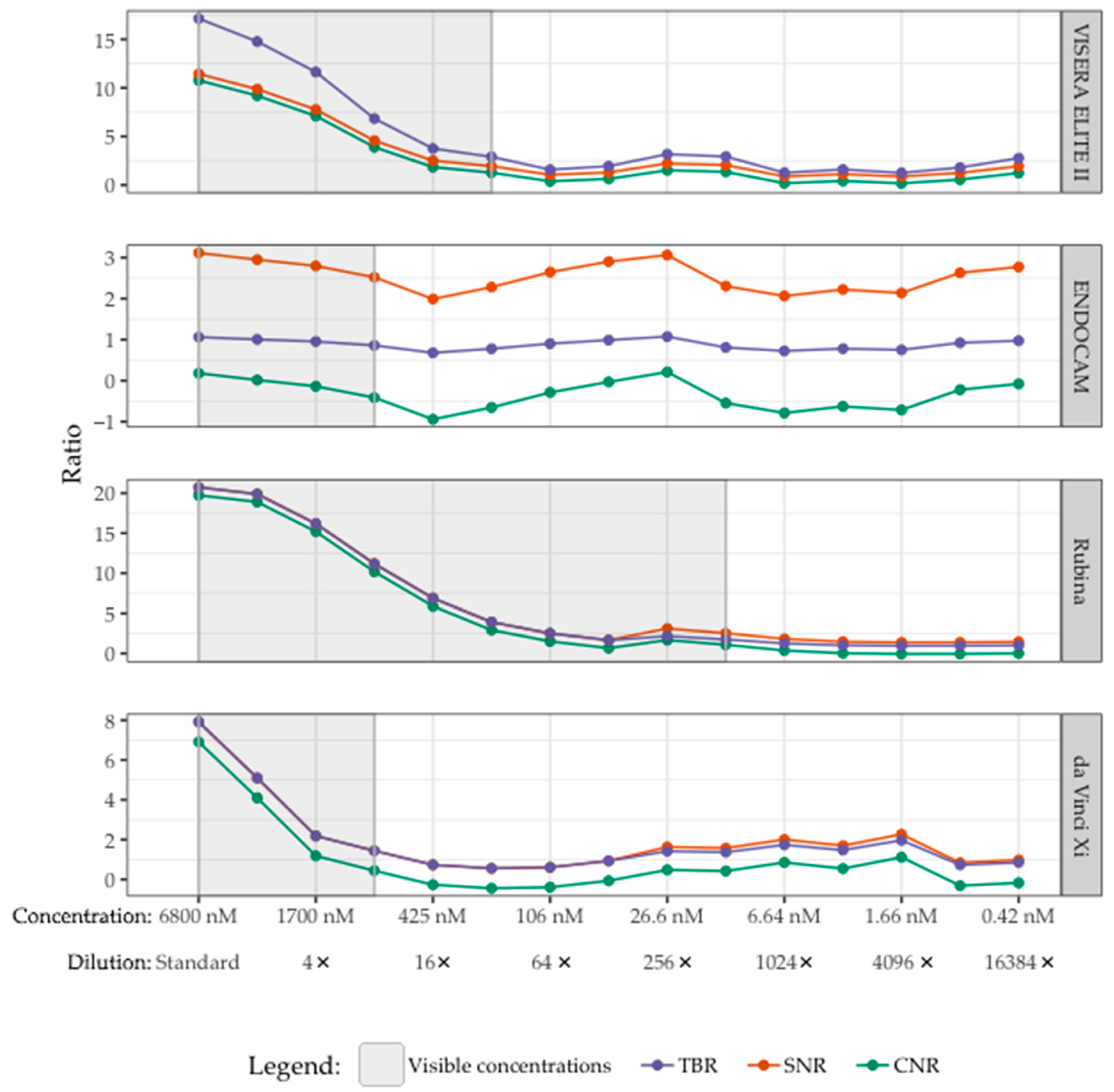
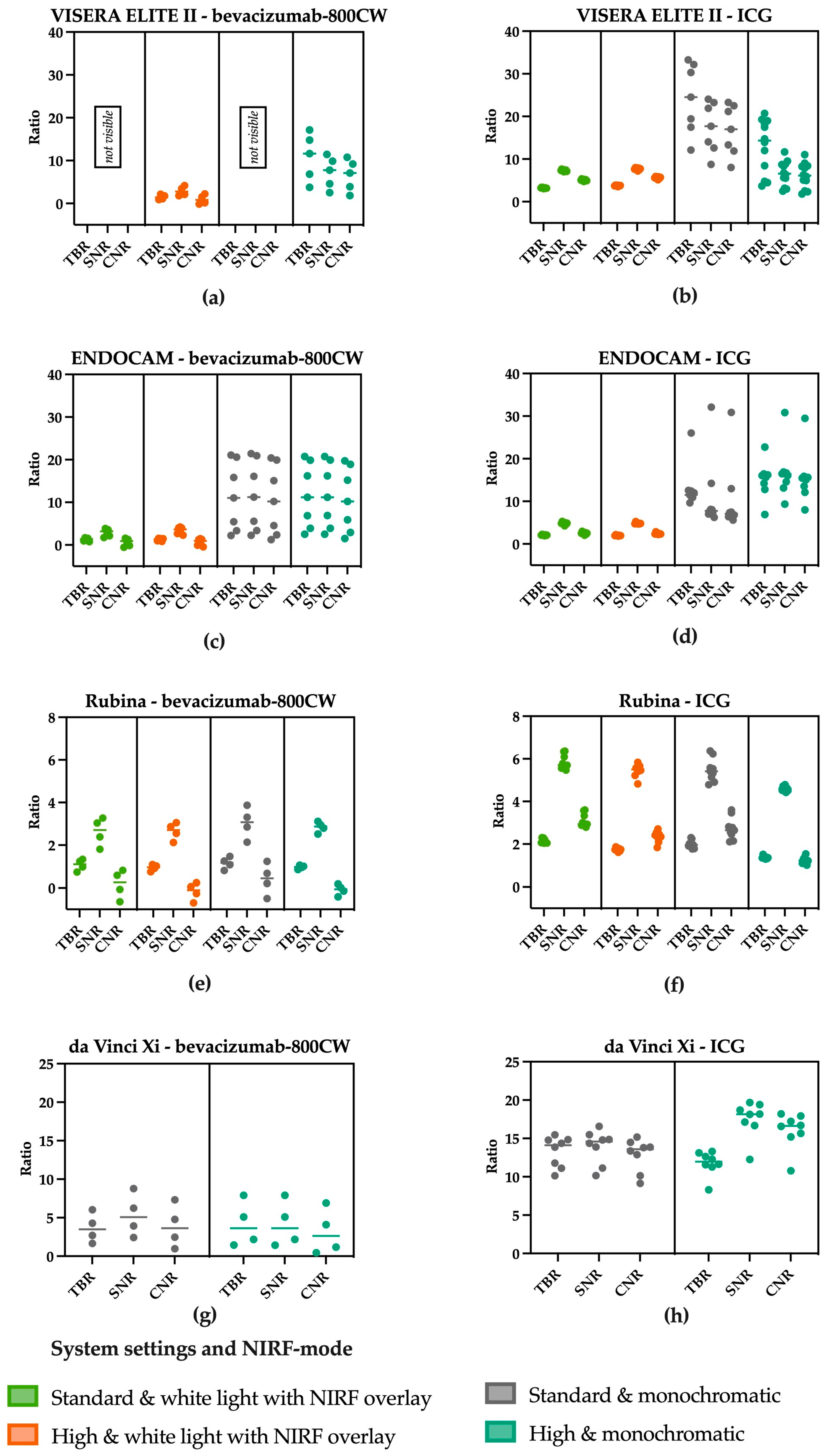
3.1. Influence of System Settings and NIRF Mode on Visibility
3.2. Influence of Working Distance on Visibility
3.3. Visibility of Bevacizumab-800CW
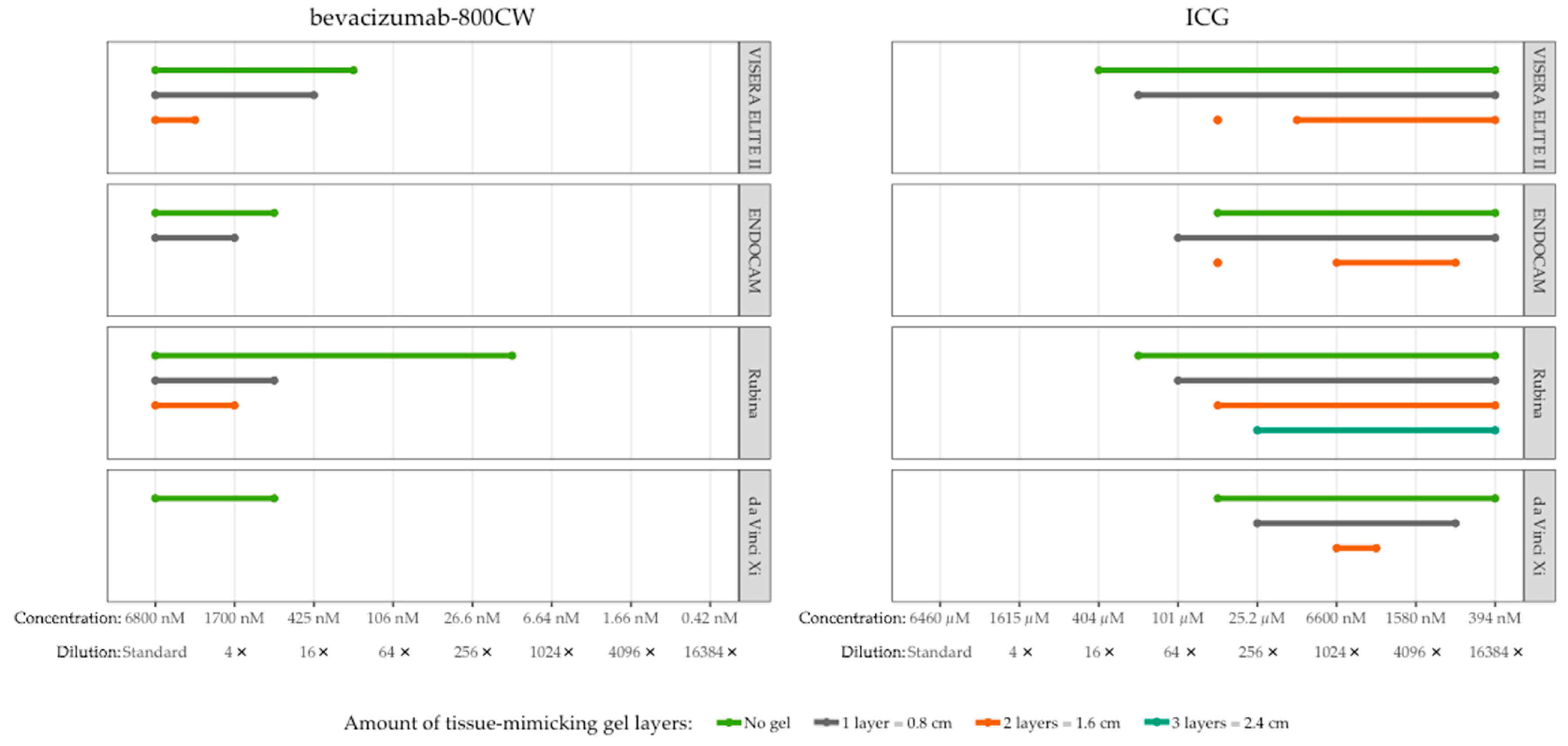
3.4. Tissue Penetration of Bevacizumab-800CW and ICG
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Dilution from the Standard Stock | Bevacizumab-800CW | ICG | ||
|---|---|---|---|---|---|
| mg/mL | Molar Concentration (M) | mg/mL | Molar Concentration (M) | ||
| 1 | Standard | 1.00 | 6.80 × 10−3 | 5.00 | 6.46 |
| 2 | 2 | 0.50 | 3.40 × 10−3 | 2.50 | 3.23 |
| 3 | 4 | 0.25 | 1.70 × 10−3 | 1.25 | 1.61 |
| 4 | 8 | 1.25 × 10−1 | 8.50 × 10−4 | 6.25 × 10−1 | 8.07 × 10−1 |
| 5 | 16 | 6.25 × 10−2 | 4.25 × 10−4 | 3.13 × 10−1 | 4.04 × 10−1 |
| 6 | 32 | 3.13 × 10−2 | 2.13 × 10−4 | 1.56 × 10−1 | 2.02 × 10−1 |
| 7 | 64 | 1.56 × 10−2 | 1.06 × 10−4 | 7.81 × 10−2 | 1.01 × 10−1 |
| 8 | 128 | 7.81 × 10−3 | 5.31 × 10−5 | 3.91 × 10−2 | 5.05 × 10−2 |
| 9 | 256 | 3.91 × 10−3 | 2.66 × 10−5 | 1.95 × 10−2 | 2.52 × 10−2 |
| 10 | 512 | 1.95 × 10−3 | 1.33 × 10−5 | 9.77 × 10−3 | 1.26 × 10−2 |
| 11 | 1024 | 9.77 × 10−4 | 6.64 × 10−6 | 4.88 × 10−3 | 6.31 × 10−3 |
| 12 | 2048 | 4.88 × 10−4 | 3.32 × 10−6 | 2.44 × 10−3 | 3.15 × 10−3 |
| 13 | 4096 | 2.44 × 10−4 | 1.66 × 10−6 | 1.22 × 10−3 | 1.58 × 10−3 |
| 14 | 8192 | 1.22 × 10−4 | 8.30 × 10−7 | 6.10 × 10−4 | 7.89 × 10−4 |
| 15 | 16,384 | 6.10 × 10−5 | 4.15 × 10−7 | 3.05 × 10−4 | 3.94 × 10−4 |
| Laparoscope Manufacturer | VISERA ELITE II Olympus | ENDOCAM Logic 4k Richard Wolf | IMAGE1 S™ 4U Rubina KARL STORZ | da Vinci XiIntuitive Surgical |
|---|---|---|---|---|
| Short name | VISERA ELITE II | ENDOCAM | Rubina | da Vinci Xi |
| NIRF excitation source, power | Xenon, 300W [78] | LED, 15W | LED, undisclosed | Laser, undisclosed |
| Excitation wavelength | Undisclosed | 760–810 nm | Undisclosed | 802–805 nm [79] |
| NIRF emission filter | Undisclosed | Undisclosed | Undisclosed | Undisclosed |
| System settings | No automatic gain. Manual intensity control | Automatic gain. Manual brightness control. | No automatic gain. Intensity manually adjustable | Automatic gain. Manual brightness control. |
| Fluorescence view mode(s) | 1. “Standard mode”: White light with green overlay 2. “Infrared enhancement mode”: Monochromatic with blue overlay (6 field) | 1. “greenICG mode”: White light with green overlay 2. “greenICG pure mode”:Monochromatic with green overlay | 1. White light with green/blue overlay 2. Monochromatic 3. Intensity map (not used in this study) | 1. “Firefly”: Monochromatic with green overlay |
| System components | ||||
| Camera head | OLYMPUS CH-S200-XZ-EA (N5766550) | LOGIC HD CAMERA HEAD GREEN (85525812) | IMAGE1 S 4U Rubina, Opal1 NIR/ICG camera head (TH121) | Standard da Vinci Xi set-up (not the Endoscope Plus) |
| Light source | CLV-S200-IR (N5427050) | Light source LED green ENDOLIGHT (5165002) | Power LED RUBINA, OPAL1 NIR/ICG (TL400) | |
| Optic | WAIR100A (W8IR100A) | TELESCOPES 0° Ø 10 MM (8934461) | TIPCAM1 RUBINA (26003BRA) | |
| Video processor | OLYMPUS OTV-S200 (N5426850) | LOGIC 4K CAMERA CONTROLLER (5525301) | IMAGE1 S CONNECT II (TC201EN) | |
| Cable | WA03310A (WA03310A) | FIBER LIGHT CABLE Ø 5 MM (806550231) | Fiber Optic Light Cable, 300 cm, 4.8 mm (495TIP) | |
| Other | Not applicable | Not applicable | IMAGE1 S 4U-LINK (TC304) | |
| Indications and field of use for fluorescence | Indication An IR telescope is designed for fluorescence imaging in the near infrared range using indocyanine green (ICG) as dye. A filterexclusively designed for ICG is built into the telescope. Light of suitable wavelength passes through the filter and enhances visualization on compatible imaging systems. | Indication The products are used for the following indications in various medical disciplines:
Contra-indication For fluorescence endoscopy (this relates to the indications of visceral blood flow, lymph node mapping and fluorescence cholangiography) please follow the specifications of the fluorescence dye manufacturer. | Indication NIR/ICG fluorescent light sources are intended for generating light in endoscopic and microscopic diagnostic examinations and in surgical procedures. Intended use For fluorescence endoscopy (this relates to the indications of visceral blood flow, lymph node mapping and fluorescence cholangiography) please follow the specifications of the fluorescence dye manufacturer. Contra-indication For fluorescence endoscopy (this relates to the indications of visceral blood flow, lymph node mapping and fluorescence cholangiography) please follow the specifications of the fluorescence dye manufacturer. | Indications for use [79] Upon intravenous administration and use of an ICG drug product consistent with its approved label, the da Vinci Fluorescence Imaging Vision System and the da Vinci Firefly Imaging System are intended to provide real-time endoscopic visible and near-infrared fluorescence imaging. The da Vinci Fluorescence Imaging Vision System and the da Vinci Firefly Imaging System enable surgeons to perform minimally invasive surgery using standard endoscopic visible light as well as visual assessment of vessels, blood flow and related tissue perfusion, and at least one of the major extrahepatic bile ducts (cystic duct, common bile duct or common hepatic duct), using near infrared imaging. Fluorescence imaging of biliary ducts with the da Vinci Fluorescence Imaging Vision System and da Vinci Firefly Imaging System are intended for use with standard of care white light and, when indicated, intraoperative cholangiography. The device is not intended for standalone use for biliary duct visualization. Upon interstitial administration and use of an ICG drug product consistent with its approved label, the da Vinci Fluorescence Imaging Vision System and the da Vinci Firefly Imaging System is used to perform intraoperative fluorescence imaging and visualization of the lymphatic system, including lymphatic vessels and lymph nodes. |

References
- Galema, H.A.; Meijer, R.P.J.; Lauwerends, L.J.; Verhoef, C.; Burggraaf, J.; Vahrmeijer, A.L.; Hutteman, M.; Keereweer, S.; Hilling, D.E. Fluorescence-Guided Surgery in Colorectal Cancer; A Review on Clinical Results and Future Perspectives. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2022, 48, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Chen, G.; Zhang, Y.; Wu, F.; Wang, Q. Advanced Fluorescence Imaging Technology in the Near-Infrared-II Window for Biomedical Applications. J. Am. Chem. Soc. 2020, 142, 14789–14804. [Google Scholar] [CrossRef]
- Kosaka, N.; Ogawa, M.; Choyke, P.L.; Kobayashi, H. Clinical Implications of Near-Infrared Fluorescence Imaging in Cancer. Future Oncol. 2009, 5, 1501–1511. [Google Scholar] [CrossRef] [PubMed]
- Young, J.K.; Figueroa, E.R.; Drezek, R.A. Tunable Nanostructures as Photothermal Theranostic Agents. Ann. Biomed. Eng. 2012, 40, 438–459. [Google Scholar] [CrossRef]
- Bashkatov, A.N.; Genina, E.A.; Kochubey, V.I.; Tuchin, V.V. Optical Properties of Human Skin, Subcutaneous and Mucous Tissues in the Wavelength Range from 400 to 2000 Nm. J. Phys. D Appl. Phys. 2005, 38, 2543. [Google Scholar] [CrossRef]
- Speich, R. Anaphylactoid Reactions after Indocyanine-Green Administration. Ann. Intern. Med. 1988, 109, 345. [Google Scholar] [CrossRef]
- She, W.H.; Cheung, T.T.; Chan, M.Y.; Chu, K.W.; Ma, K.W.; Tsang, S.H.Y.; Dai, W.C.; Chan, A.C.Y.; Lo, C.M. Routine Use of ICG to Enhance Operative Safety in Emergency Laparoscopic Cholecystectomy: A Randomized Controlled Trial. Surg. Endosc. 2022, 36, 4442–4451. [Google Scholar] [CrossRef] [PubMed]
- Schouw, H.M.; Huisman, L.A.; Janssen, Y.F.; Slart, R.H.J.A.; Borra, R.J.H.; Willemsen, A.T.M.; Brouwers, A.H.; van Dijl, J.M.; Dierckx, R.A.; van Dam, G.M.; et al. Targeted Optical Fluorescence Imaging: A Meta-Narrative Review and Future Perspectives. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4272–4292. [Google Scholar] [CrossRef]
- Harlaar, N.J.; Koller, M.; de Jongh, S.J.; van Leeuwen, B.L.; Hemmer, P.H.; Kruijff, S.; van Ginkel, R.J.; Been, L.B.; de Jong, J.S.; Kats-Ugurlu, G.; et al. Molecular Fluorescence-Guided Surgery of Peritoneal Carcinomatosis of Colorectal Origin: A Single-Centre Feasibility Study. Lancet Gastroenterol. Hepatol. 2016, 1, 283–290. [Google Scholar] [CrossRef]
- Lwin, T.M.; Turner, M.A.; Amirfakhri, S.; Nishino, H.; Hoffman, R.M.; Bouvet, M. Fluorescence Molecular Targeting of Colon Cancer to Visualize the Invisible. Cells 2022, 11, 249. [Google Scholar] [CrossRef] [PubMed]
- LI-COR Biosciences IRDye® Infrared Dyes. Available online: https://www.ld.ru/w/licor/IRDye_brochure_web.pdf (accessed on 8 January 2023).
- AAT Bioquest Spectrum [Li-Cor IRDye 800CW]. Available online: https://www.aatbio.com/fluorescence-excitation-emission-spectrum-graph-viewer/li_cor_irdye_800cw (accessed on 8 January 2023).
- Landsman, M.L.; Kwant, G.; Mook, G.A.; Zijlstra, W.G. Light-Absorbing Properties, Stability, and Spectral Stabilization of Indocyanine Green. J. Appl. Physiol. 1976, 40, 575–583. [Google Scholar] [CrossRef]
- DSouza, A.V.; Lin, H.; Henderson, E.R.; Samkoe, K.S.; Pogue, B.W. Review of Fluorescence Guided Surgery Systems: Identification of Key Performance Capabilities beyond Indocyanine Green Imaging. J. Biomed. Opt. 2016, 21, 80901. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, L.; Koch, M.; de Jong, J.; Adams, A.; Glatz, J.; Kranendonk, M.; Terwisscha van Scheltinga, A.; Jansen, L.; de Vries, J.; Lub-de Hooge, M.; et al. Tumor-Specific Uptake of Fluorescent Bevacizumab-IRDye800CW Microdosing in Patients with Primary Breast Cancer: A Phase I Feasibility Study. Clin Cancer Res. 2017, 23, 2730–2741. [Google Scholar] [CrossRef] [PubMed]
- Nagengast, W.B.; Hartmans, E.; Garcia-Allende, P.B.; Peters, F.T.M.; Linssen, M.D.; Koch, M.; Koller, M.; Tjalma, J.J.J.; Karrenbeld, A.; Jorritsma-Smit, A.; et al. Near-Infrared Fluorescence Molecular Endoscopy Detects Dysplastic Oesophageal Lesions Using Topical and Systemic Tracer of Vascular Endothelial Growth Factor A. Gut 2019, 68, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Tjalma, J.J.J.; Koller, M.; Linssen, M.D.; Hartmans, E.; de Jongh, S.J.; Jorritsma-Smit, A.; Karrenbeld, A.; de Vries, E.G.; Kleibeuker, J.H.; Pennings, J.P.; et al. Quantitative Fluorescence Endoscopy: An Innovative Endoscopy Approach to Evaluate Neoadjuvant Treatment Response in Locally Advanced Rectal Cancer. Gut 2020, 69, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Mulder, B.G.S.; Koller, M.; Duiker, E.W.; Sarasqueta, A.F.; Burggraaf, J.; de Meijer, V.E.; Vahrmeijer, A.L.; Hoogwater, F.J.H.; Bonsing, B.A.; van Dam, G.M.; et al. Intraoperative Molecular Fluorescence Imaging of Pancreatic Cancer by Targeting Vascular Endothelial Growth Factor: A Multicenter Feasibility Dose-Escalation Study. J. Nucl. Med. 2023, 64, 82–89. [Google Scholar] [CrossRef]
- Vonk, J.; Voskuil, F.J.; de Wit, J.G.; Heeman, W.T.; Nagengast, W.B.; van Dam, G.M.; Feijen, R.A.; Korsten-Meijer, A.; van der Vegt, B.; Witjes, M. Fluorescence Grid Analysis for the Evaluation of Piecemeal Surgery in Sinonasal Inverted Papilloma: A Proof-of-Concept Study. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1640–1649. [Google Scholar] [CrossRef] [PubMed]
- Steinkamp, P.J.; Vonk, J.; Huisman, L.A.; Meersma, G.-J.; Diercks, G.F.H.; Hillebrands, J.-L.; Nagengast, W.B.; Zeebregts, C.J.; Slart, R.H.J.A.; Boersma, H.H.; et al. VEGF-Targeted Multispectral Optoacoustic Tomography and Fluorescence Molecular Imaging in Human Carotid Atherosclerotic Plaques. Diagnostics 2021, 11, 1227. [Google Scholar] [CrossRef]
- Steinkamp, P.J.; Pranger, B.K.; Li, M.-F.; Linssen, M.D.; Voskuil, F.J.; Been, L.B.; van Leeuwen, B.L.; Suurmeijer, A.J.H.; Nagengast, W.B.; Kruijff, S.; et al. Fluorescence-Guided Visualization of Soft-Tissue Sarcomas by Targeting Vascular Endothelial Growth Factor A: A Phase 1 Single-Center Clinical Trial. J. Nucl. Med. 2021, 62, 342–347. [Google Scholar] [CrossRef]
- De Jongh, S.J.; Tjalma, J.J.J.; Koller, M.; Linssen, M.D.; Vonk, J.; Dobosz, M.; Jorritsma-Smit, A.; Kleibeuker, J.H.; Hospers, G.A.P.; Havenga, K.; et al. Back-Table Fluorescence-Guided Imaging for Circumferential Resection Margin Evaluation Using Bevacizumab-800CW in Patients with Locally Advanced Rectal Cancer. J. Nucl. Med. 2020, 61, 655–661. [Google Scholar] [CrossRef]
- Vonk, J.; de Wit, J.G.; Voskuil, F.J.; Koldijk, M.; Rácz, E.; Hooghiemstra, W.T.R.; Doff, J.J.; Diercks, G.F.H.; van Dam, G.M.; Witjes, M.J.H.; et al. Fluorescence Molecular Imaging Using Cetuximab-800CW in Cutaneous Squamous Cell Carcinoma Surgery: A Proof-of-Concept Study. Br. J. Dermatol. 2022, 187, 810–812. [Google Scholar] [CrossRef]
- Vonk, J.; de Wit, J.G.; Voskuil, F.J.; Tang, Y.H.; Hooghiemstra, W.T.R.; Linssen, M.D.; van den Broek, E.; Doff, J.J.; de Visscher, S.A.H.J.; Schepman, K.-P.; et al. Epidermal Growth Factor Receptor-Targeted Fluorescence Molecular Imaging for Postoperative Lymph Node Assessment in Patients with Oral Cancer. J. Nucl. Med. 2022, 63, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Linssen, M.D.; Hooghiemstra, W.T.R.; Jorritsma-Smit, A.; Allersma, D.P.; Dijkstra, G.; Nagengast, W.B. Development and Characterisation of Antibody-Based Optical Imaging Probes for Inflammatory Bowel Disease. Pharmaceuticals 2021, 14, 922. [Google Scholar] [CrossRef]
- Zhao, X.; Gabriëls, R.Y.; Hooghiemstra, W.T.R.; Koller, M.; Meersma, G.J.; Buist-Homan, M.; Visser, L.; Robinson, D.J.; Tenditnaya, A.; Gorpas, D.; et al. Validation of Novel Molecular Imaging Targets Identified by Functional Genomic MRNA Profiling to Detect Dysplasia in Barrett’s Esophagus. Cancers 2022, 14, 2462. [Google Scholar] [CrossRef]
- Linssen, M.D.; Ter Weele, E.J.; Allersma, D.P.; Lub-de Hooge, M.N.; van Dam, G.M.; Jorritsma-Smit, A.; Nagengast, W.B. Roadmap for the Development and Clinical Translation of Optical Tracers Cetuximab-800CW and Trastuzumab-800CW. J. Nucl. Med. 2019, 60, 418–423. [Google Scholar] [CrossRef]
- Ter Weele, E.J.; Terwisscha van Scheltinga, A.G.T.; Linssen, M.D.; Nagengast, W.B.; Lindner, I.; Jorritsma-Smit, A.; de Vries, E.G.E.; Kosterink, J.G.W.; Lub-de Hooge, M.N. Development, Preclinical Safety, Formulation, and Stability of Clinical Grade Bevacizumab-800CW, a New near Infrared Fluorescent Imaging Agent for First in Human Use. Eur. J. Pharm. Biopharm. Off. J. Arb. Pharm. Verfahr. 2016, 104, 226–234. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services Food and Drug Administration Center for Drug. Evaluation and Research (CDER) Guidance for Industry, Investigators, and Reviewers—Exploratory IND Studies. Available online: https://www.fda.gov/media/72325/download (accessed on 2 March 2023).
- European Medicines Agency (EMA). ICH Guideline M3(R2) on Non-Clinical Safety Studies for the Conduct of Human Clinical Trials and Marketing Authorisation for Pharmaceuticals; European Medicines Agency: Amsterdam, The Netherlands, 2013.
- Tewari, T.; Mukherjee, S. Microdosing: Concept, Application and Relevance. Perspect. Clin. Res. 2010, 1, 61–63. [Google Scholar]
- Burt, T.; Young, G.; Lee, W.; Kusuhara, H.; Langer, O.; Rowland, M.; Sugiyama, Y. Phase 0/Microdosing Approaches: Time for Mainstream Application in Drug Development? Nat. Rev. Drug Discov. 2020, 19, 801–818. [Google Scholar] [CrossRef] [PubMed]
- Sikkenk, D.; Consten, E.; Nagengast, W. Clinicaltrials.Gov—Fluorescent Sentinel Lymph Node Identification in Colon Carcinoma Using Submucosal Bevacizumab-800CW. (IBIZA-1). Available online: https://clinicaltrials.gov/ct2/show/NCT05498051?term=bevacizumab-800CW&recrs=ab&cntry=NL&draw=2&rank=2 (accessed on 1 March 2023).
- Sikkenk, D.; Nagengast, W.; Consten, E. Clinicaltrials.Gov—Fluorescent Sentinel Lymph Node Identification in Colon Carcinoma Using Intravenous Bevacizumab-800CW. (IBIZA-2). Available online: https://clinicaltrials.gov/ct2/show/NCT05497726?term=bevacizumab-800CW&recrs=ab&cntry=NL&draw=2&rank=1 (accessed on 1 March 2023).
- Korb, M.L.; Huh, W.K.; Boone, J.D.; Warram, J.M.; Chung, T.K.; de Boer, E.; Bland, K.I.; Rosenthal, E.L. Laparoscopic Fluorescent Visualization of the Ureter With Intravenous IRDye800CW. J. Minim. Invasive Gynecol. 2015, 22, 799–806. [Google Scholar] [CrossRef]
- Liss, M.A.; Farshchi-Heydari, S.; Qin, Z.; Hickey, S.A.; Hall, D.J.; Kane, C.J.; Vera, D.R. Preclinical Evaluation of Robotic-Assisted Sentinel Lymph Node Fluorescence Imaging. J. Nucl. Med. 2014, 55, 1552–1556. [Google Scholar] [CrossRef] [PubMed]
- Hoogstins, C.; Burggraaf, J.J.; Koller, M.; Handgraaf, H.; Boogerd, L.; van Dam, G.; Vahrmeijer, A.; Burggraaf, J. Setting Standards for Reporting and Quantification in Fluorescence-Guided Surgery. Mol. Imaging Biol. 2019, 21, 11–18. [Google Scholar] [CrossRef]
- Yuan, B.; Chen, N.; Zhu, Q. Emission and Absorption Properties of Indocyanine Green in Intralipid Solution. J. Biomed. Opt. 2004, 9, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Voskuil, F.J.; Steinkamp, P.J.; Zhao, T.; van der Vegt, B.; Koller, M.; Doff, J.J.; Jayalakshmi, Y.; Hartung, J.P.; Gao, J.; Sumer, B.D.; et al. Exploiting Metabolic Acidosis in Solid Cancers Using a Tumor-Agnostic PH-Activatable Nanoprobe for Fluorescence-Guided Surgery. Nat. Commun. 2020, 11, 3257. [Google Scholar] [CrossRef]
- Pleijhuis, R.; Timmermans, A.; De Jong, J.; De Boer, E.; Ntziachristos, V.; Van Dam, G. Tissue-Simulating Phantoms for Assessing Potential near-Infrared Fluorescence Imaging Applications in Breast Cancer Surgery. J. Vis. Exp. 2014, 51776. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding Interobserver Agreement: The Kappa Statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Koller, M.; Qiu, S.-Q.; Linssen, M.D.; Jansen, L.; Kelder, W.; de Vries, J.; Kruithof, I.; Zhang, G.-J.; Robinson, D.J.; Nagengast, W.B.; et al. Implementation and Benchmarking of a Novel Analytical Framework to Clinically Evaluate Tumor-Specific Fluorescent Tracers. Nat. Commun. 2018, 9, 3739. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Allende, P.; Glatz, J.; Koch, M.; Tjalma, J.; Hartmans, E.; Terwisscha van Scheltinga, A.; Symvoulidis, P.; van Dam, G.; Nagengast, W.; Ntziachristos, V. Towards Clinically Translatable NIR Fluorescence Molecular Guidance for Colonoscopy. Biomed. Opt. Express 2013, 5, 78–92. [Google Scholar] [CrossRef]
- Welvaert, M.; Rosseel, Y. On the Definition of Signal-to-Noise Ratio and Contrast-to-Noise Ratio for FMRI Data. PLoS ONE 2013, 8, e77089. [Google Scholar] [CrossRef]
- Song, X.; Pogue, B.W.; Jiang, S.; Doyley, M.M.; Dehghani, H.; Tosteson, T.D.; Paulsen, K.D. Automated Region Detection Based on the Contrast-to-Noise Ratio in near-Infrared Tomography. Appl. Opt. 2004, 43, 1053–1062. [Google Scholar] [CrossRef]
- Dempsey, G.T.; Vaughan, J.C.; Chen, K.H.; Bates, M.; Zhuang, X. Evaluation of Fluorophores for Optimal Performance in Localization-Based Super-Resolution Imaging. Nat. Methods 2011, 8, 1027–1036. [Google Scholar] [CrossRef]
- Te Velde, E.A.; Veerman, T.; Subramaniam, V.; Ruers, T. The Use of Fluorescent Dyes and Probes in Surgical Oncology. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2010, 36, 6–15. [Google Scholar] [CrossRef]
- Pang, Z.; Yan, W.; Yang, J.; Li, Q.; Guo, Y.; Zhou, D.; Jiang, X. Multifunctional Gold Nanoclusters for Effective Targeting, Near-Infrared Fluorescence Imaging, Diagnosis, and Treatment of Cancer Lymphatic Metastasis. ACS Nano 2022, 16, 16019–16037. [Google Scholar] [CrossRef]
- Mok, H.; Jeong, H.; Kim, S.-J.; Chung, B.H. Indocyanine Green Encapsulated Nanogels for Hyaluronidase Activatable and Selective near Infrared Imaging of Tumors and Lymph Nodes. Chem. Commun. (Camb). 2012, 48, 8628–8630. [Google Scholar] [CrossRef]
- Holzer, W.; Mauerer, M.; Penzkofer, A.; Szeimies, R.M.; Abels, C.; Landthaler, M.; Bäumler, W. Photostability and Thermal Stability of Indocyanine Green. J. Photochem. Photobiol. B 1998, 47, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Saxena, V.; Sadoqi, M.; Shao, J. Enhanced Photo-Stability, Thermal-Stability and Aqueous-Stability of Indocyanine Green in Polymeric Nanoparticulate Systems. J. Photochem. Photobiol. B 2004, 74, 29–38. [Google Scholar] [CrossRef]
- Prahl, S. Optical Absorption of Indocyanine Green (ICG). Available online: https://omlc.org/spectra/icg/index.html (accessed on 8 January 2023).
- KleinJan, G.H.; Bunschoten, A.; van den Berg, N.S.; Olmos, R.A.V.; Klop, W.M.C.; Horenblas, S.; van der Poel, H.G.; Wester, H.-J.; van Leeuwen, F.W.B. Fluorescence Guided Surgery and Tracer-Dose, Fact or Fiction? Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1857–1867. [Google Scholar] [CrossRef] [PubMed]
- Carr, J.A.; Franke, D.; Caram, J.R.; Perkinson, C.F.; Saif, M.; Askoxylakis, V.; Datta, M.; Fukumura, D.; Jain, R.K.; Bawendi, M.G.; et al. Shortwave Infrared Fluorescence Imaging with the Clinically Approved Near-Infrared Dye Indocyanine Green. Proc. Natl. Acad. Sci. USA 2018, 115, 4465–4470. [Google Scholar] [CrossRef] [PubMed]
- Heuveling, D.A.; Visser, G.W.M.; de Groot, M.; de Boer, J.F.; Baclayon, M.; Roos, W.H.; Wuite, G.J.L.; Leemans, C.R.; de Bree, R.; van Dongen, G.A.M.S. Nanocolloidal Albumin-IRDye 800CW: A near-Infrared Fluorescent Tracer with Optimal Retention in the Sentinel Lymph Node. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1161–1168. [Google Scholar] [CrossRef]
- Tanaka, E.; Choi, H.S.; Fujii, H.; Bawendi, M.G.; Frangioni, J.V. Image-Guided Oncologic Surgery Using Invisible Light: Completed Pre-Clinical Development for Sentinel Lymph Node Mapping. Ann. Surg. Oncol. 2006, 13, 1671–1681. [Google Scholar] [CrossRef]
- Hartmans, E.; Tjalma, J.J.J.; Linssen, M.D.; Allende, P.B.G.; Koller, M.; Jorritsma-Smit, A.; Nery, M.E.S.d.O.; Elias, S.G.; Karrenbeld, A.; de Vries, E.G.E.; et al. Potential Red-Flag Identification of Colorectal Adenomas with Wide-Field Fluorescence Molecular Endoscopy. Theranostics 2018, 8, 1458–1467. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, G.; van den Berg, N.S.; Nishio, N.; Juniper, G.; Pei, J.; Zhou, Q.; Lu, G.; Lee, Y.-J.; Ramos, K.; Iagaru, A.H.; et al. Metastatic and Sentinel Lymph Node Mapping Using Intravenously Delivered Panitumumab-IRDye800CW. Theranostics 2021, 11, 7188–7198. [Google Scholar] [CrossRef]
- Tummers, W.S.; Miller, S.E.; Teraphongphom, N.T.; van den Berg, N.S.; Hasan, A.; Longacre, T.A.; Fisher, G.A.; Bonsing, B.A.; Vahrmeijer, A.L.; Gambhir, S.S.; et al. Detection of Visually Occult Metastatic Lymph Nodes Using Molecularly Targeted Fluorescent Imaging during Surgical Resection of Pancreatic Cancer. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2019, 21, 883–890. [Google Scholar] [CrossRef]
- Hart, Z.P.; Nishio, N.; Krishnan, G.; Lu, G.; Zhou, Q.; Fakurnejad, S.; Wormald, P.J.; van den Berg, N.S.; Rosenthal, E.L.; Baik, F.M. Endoscopic Fluorescence-Guided Surgery for Sinonasal Cancer Using an Antibody-Dye Conjugate. Laryngoscope 2020, 130, 2811–2817. [Google Scholar] [CrossRef] [PubMed]
- Bonfield, H.E.; Knauber, T.; Lévesque, F.; Moschetta, E.G.; Susanne, F.; Edwards, L.J. Photons as a 21st Century Reagent. Nat. Commun. 2020, 11, 804. [Google Scholar] [CrossRef] [PubMed]
- Hollins, B.; Noe, B.; Henderson, J.M. Fluorometric Determination of Indocyanine Green in Plasma. Clin. Chem. 1987, 33, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Mindt, S.; Karampinis, I.; John, M.; Neumaier, M.; Nowak, K. Stability and Degradation of Indocyanine Green in Plasma, Aqueous Solution and Whole Blood. Photochem. Photobiol. Sci. Off. J. Eur. Photochem. Assoc. Eur. Soc. Photobiol. 2018, 17, 1189–1196. [Google Scholar] [CrossRef]
- van den Bos, J.; Wieringa, F.P.; Bouvy, N.D.; Stassen, L.P.S. Optimizing the Image of Fluorescence Cholangiography Using ICG: A Systematic Review and Ex Vivo Experiments. Surg. Endosc. 2018, 32, 4820–4832. [Google Scholar] [CrossRef]
- van Willigen, D.M.; van den Berg, N.S.; Buckle, T.; KleinJan, G.H.; Hardwick, J.C.; van der Poel, H.G.; van Leeuwen, F.W. Multispectral Fluorescence Guided Surgery; a Feasibility Study in a Phantom Using a Clinical-Grade Laparoscopic Camera System. Am. J. Nucl. Med. Mol. Imaging 2017, 7, 138–147. [Google Scholar]
- Vreeburg, M.T.A.; Azargoshasb, S.; van Willigen, D.; Molenaar, T.; van Oosterom, M.N.; Buckle, T.; Slof, L.J.; Klop, M.; Karakullukcu, B.; Donswijk, M.; et al. Comparison of Two Hybrid Sentinel Node Tracers: Indocyanine Green (ICG)-(99m)Tc-Nanocolloid vs. ICG-(99m)Tc-Nanoscan from a Nuclear Medicine and Surgical Perspective. Eur. J. Nucl. Med. Mol. Imaging 2023. [Google Scholar] [CrossRef]
- Wit, E.M.K.; KleinJan, G.H.; Berrens, A.-C.; van Vliet, R.; van Leeuwen, P.J.; Buckle, T.; Donswijk, M.L.; Bekers, E.M.; van Leeuwen, F.W.B.; van der Poel, H.G. A Hybrid Radioactive and Fluorescence Approach Is More than the Sum of Its Parts; Outcome of a Phase II Randomized Sentinel Node Trial in Prostate Cancer Patients. Eur. J. Nucl. Med. Mol. Imaging 2023. [Google Scholar] [CrossRef]
- Frederiks, C.N.; Overwater, A.; Bergman, J.J.G.H.M.; Pouw, R.E.; de Keizer, B.; Bennink, R.J.; Brosens, L.A.A.; Meijer, S.L.; van Hillegersberg, R.; van Berge Henegouwen, M.I.; et al. Feasibility and Safety of Tailored Lymphadenectomy Using Sentinel Node-Navigated Surgery in Patients with High-Risk T1 Esophageal Adenocarcinoma. Ann. Surg. Oncol. 2023, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mulita, F.; Verras, G.-I.; Anagnostopoulos, C.-N.; Kotis, K. A Smarter Health through the Internet of Surgical Things. Sensors 2022, 22, 4577. [Google Scholar] [CrossRef] [PubMed]
- Azargoshasb, S.; Boekestijn, I.; Roestenberg, M.; KleinJan, G.H.; van der Hage, J.A.; van der Poel, H.G.; Rietbergen, D.D.D.; van Oosterom, M.N.; van Leeuwen, F.W.B. Quantifying the Impact of Signal-to-Background Ratios on Surgical Discrimination of Fluorescent Lesions. Mol. Imaging Biol. 2022, 25, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Deken, M.M.; Bos, D.L.; Tummers, W.S.F.J.; March, T.L.; van de Velde, C.J.H.; Rijpkema, M.; Vahrmeijer, A.L. Multimodal Image-Guided Surgery of HER2-Positive Breast Cancer Using [(111)In]In-DTPA-Trastuzumab-IRDye800CW in an Orthotopic Breast Tumor Model. EJNMMI Res. 2019, 9, 98. [Google Scholar] [CrossRef]
- Qin, Z.; Hall, D.J.; Liss, M.A.; Hoh, C.K.; Kane, C.J.; Wallace, A.M.; Vera, D.R. Optimization via Specific Fluorescence Brightness of a Receptor-Targeted Probe for Optical Imaging and Positron Emission Tomography of Sentinel Lymph Nodes. J. Biomed. Opt. 2013, 18, 101315. [Google Scholar] [CrossRef]
- Gabriels, R.Y.; van Heijst, L.E.; Hooghiemstra, W.T.R.; van der Waaij, A.M.; Kats-Ugurlu, G.; Karrenbeld, A.; Robinson, D.J.; Tenditnaya, A.; Ntziachristos, V.; Gorpas, D.; et al. Detection of Early Esophageal Neoplastic Barrett Lesions with Quantified Fluorescence Molecular Endoscopy Using Cetuximab-800CW. J. Nucl. Med. 2023, 64. [Google Scholar] [CrossRef]
- Gao, R.W.; Teraphongphom, N.; de Boer, E.; van den Berg, N.S.; Divi, V.; Kaplan, M.J.; Oberhelman, N.J.; Hong, S.S.; Capes, E.; Colevas, A.D.; et al. Safety of Panitumumab-IRDye800CW and Cetuximab-IRDye800CW for Fluorescence-Guided Surgical Navigation in Head and Neck Cancers. Theranostics 2018, 8, 2488–2495. [Google Scholar] [CrossRef]
- Zhou, Q.; van den Berg, N.S.; Kang, W.; Pei, J.; Nishio, N.; van Keulen, S.; Engelen, M.A.; Lee, Y.-J.; Hom, M.; Vega Leonel, J.C.M.; et al. Factors for Differential Outcome Across Cancers in Clinical Molecule-Targeted Fluorescence Imaging. J. Nucl. Med. 2022, 63, 1693–1700. [Google Scholar] [CrossRef]
- Zhang, Z.; Fang, C.; Zhang, Y.; Su, S.; Li, B.; Liu, G.; Hu, Z.; Tian, J. NIR-II Nano Fluorescence Image Guided Hepatic Carcinoma Resection on Cirrhotic Patient. Photodiagnosis Photodyn. Ther. 2022, 40, 103098. [Google Scholar] [CrossRef]
- Sterkenburg, A.J.; Hooghiemstra, W.T.R.; Schmidt, I.; Ntziachristos, V.; Nagengast, W.B.; Gorpas, D. Standardization and Implementation of Fluorescence Molecular Endoscopy in the Clinic. J. Biomed. Opt. 2022, 27, 074704. [Google Scholar] [CrossRef]
- Olympus CLV-S200-IR—Xenon Light Source: Product Details + Technical Specifications (PDF). Available online: https://www.olympus-europa.com/medical/en/Products-and-Solutions/Products/Product/CLV-S200-IR.html (accessed on 23 March 2023).
- Food & Drug Administration Da Vinci Fluorescence Imaging Vision System, Da Vinci Firefly Imaging System. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf21/K213710.pdf (accessed on 23 March 2023).






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikkenk, D.J.; Sterkenburg, A.J.; Schmidt, I.; Gorpas, D.; Nagengast, W.B.; Consten, E.C.J. Detection of Tumour-Targeted IRDye800CW Tracer with Commercially Available Laparoscopic Surgical Systems. Diagnostics 2023, 13, 1591. https://doi.org/10.3390/diagnostics13091591
Sikkenk DJ, Sterkenburg AJ, Schmidt I, Gorpas D, Nagengast WB, Consten ECJ. Detection of Tumour-Targeted IRDye800CW Tracer with Commercially Available Laparoscopic Surgical Systems. Diagnostics. 2023; 13(9):1591. https://doi.org/10.3390/diagnostics13091591
Chicago/Turabian StyleSikkenk, Daan J., Andrea J. Sterkenburg, Iris Schmidt, Dimitris Gorpas, Wouter B. Nagengast, and Esther C. J. Consten. 2023. "Detection of Tumour-Targeted IRDye800CW Tracer with Commercially Available Laparoscopic Surgical Systems" Diagnostics 13, no. 9: 1591. https://doi.org/10.3390/diagnostics13091591
APA StyleSikkenk, D. J., Sterkenburg, A. J., Schmidt, I., Gorpas, D., Nagengast, W. B., & Consten, E. C. J. (2023). Detection of Tumour-Targeted IRDye800CW Tracer with Commercially Available Laparoscopic Surgical Systems. Diagnostics, 13(9), 1591. https://doi.org/10.3390/diagnostics13091591