
Low-Risk Women with Suspicious Microcalcifications in Mammography—Can an Additional Breast MRI Reduce the Biopsy Rate?

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design and Population
2.2. Mammography
2.3. Breast Magnetic Resonance Imaging
2.4. Breast MRI Image Evaluation
2.5. Statistical Analysis
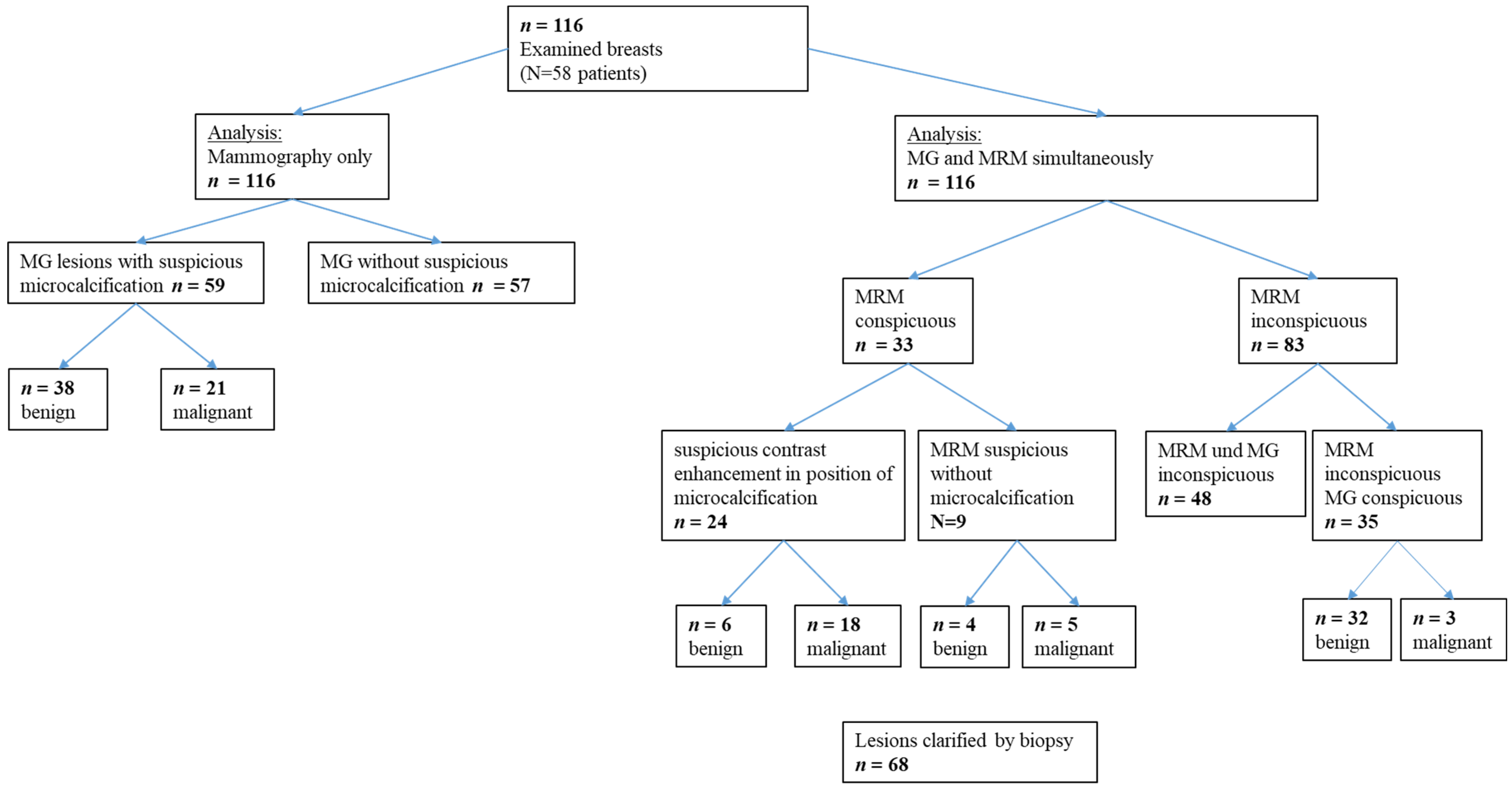
3. Results
3.1. Breast MRI and MG Examinations
3.2. Characteristics of Trial Population
3.3. Histology
3.4. Histology of Lesions with Suspicious MCs in MG
- -
- A total of 14/21 (67%) of the malignant lesions represented a DCIS: high-grade in 7/14 cases (50%), intermediate-grade in one case (7%) and low-grade in six cases (43%).
- -
- A total of 7/21 (33%) malignant findings showed an invasive carcinoma. Two exclusively invasive carcinomas (no special type (NST), one G1 and one G2). A total of 5/7 of the invasive carcinomas were associated with DCIS (one NST G1 with low-grade DCIS, two NST G2 each with an intermediate-grade and high-grade DCIS, one NST G3 with a high-grade DCIS and one invasive tubular carcinoma one associated with a high-grade DCIS).
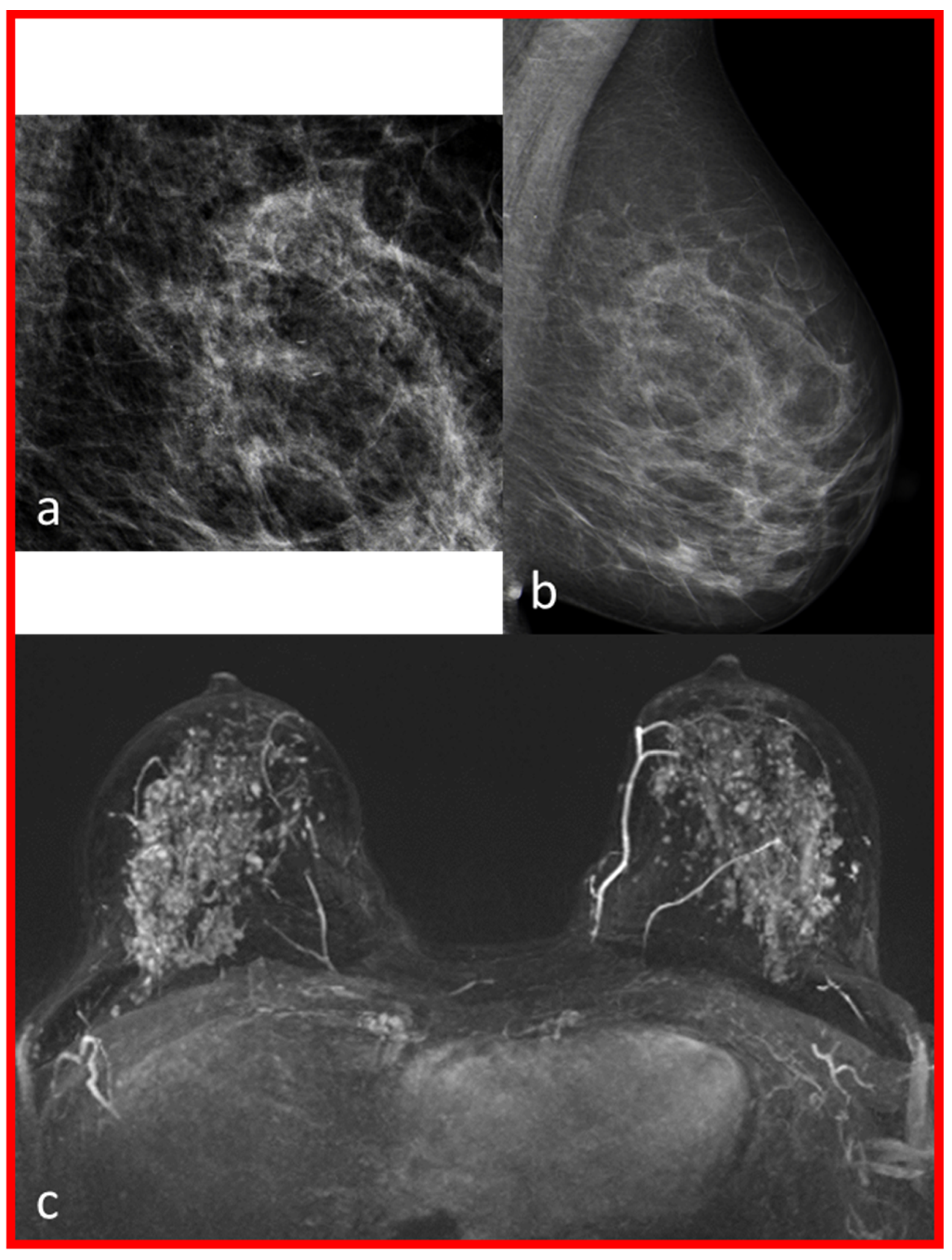
3.5. Histology of Lesions Additionally Detected in Breast MRI
3.6. Comparison of the Diagnostic Accuracy of MG and MG Plus Breast MRI in Evaluation of MCs
3.7. Results of the Additionally Performed Breast MRI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krebs in Deutschland 2017/2018. Robert Koch Institut—Zentrum für Krebsregisterdaten. Available online: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/kid_2021/kid_2021_c50_brust.pdf?__blob=publicationFile (accessed on 20 February 2023).
- Siu, A.L.; U.S. Preventive Services Task Force. Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016, 164, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Bennani-Baiti, B.; Baltzer, P.A. MR Imaging for Diagnosis of Malignancy in Mammographic Microcalcifications: A Systematic Review and Meta-Analysis. Radiology 2017, 283, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Rominger, M.; Wisgickl, C.; Timmesfeld, N. Breast microcalcifications as type descriptors to stratify risk of malignancy: A systematic review and meta-analysis of 10665 cases with special focus on round/punctate microcalcifications. Rofo 2012, 184, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Bluekens, A.M.; Holland, R.; Karssemeijer, N.; Broeders, M.J.; den Heeten, G.J. Comparison of digital screening mammography and screen-film mammography in the early detection of clinically relevant cancers: A multicenter study. Radiology 2012, 265, 707–714. [Google Scholar] [CrossRef]
- Cilotti, A.; Iacconi, C.; Marini, C.; Moretti, M.; Mazzotta, D.; Traino, C.; Naccarato, A.G.; Piagneri, V.; Giaconi, C.; Bevilacqua, G.; et al. Contrast-enhanced MR imaging in patients with BI-RADS 3-5 microcalcifications. Radiol. Med. 2007, 112, 272–286. [Google Scholar] [CrossRef]
- Stomper, P.C.; Davis, S.P.; Weidner, N.; Meyer, J.E. Clinically occult ductal carcinoma in situ detected with mammography: Analysis of 100 cases with radiologic-pathologic correlation. Radiology 1989, 172, 235–241. [Google Scholar] [CrossRef]
- Verschuur-Maes, A.H.; van Gils, C.H.; van den Bosch, M.A.; De Bruin, P.C.; van Diest, P.J. Digital mammography: More microcalcifications, more columnar cell lesions without atypia. Mod. Pathol. 2011, 24, 1191–11977. [Google Scholar] [CrossRef]
- Feeley, L.; Kiernan, D.; Mooney, T.; Flanagan, F.; Hargaden, G.; Kell, M.; Stokes, M.; Kennedy, M. Digital mammography in a screening programme and its implications for pathology: A comparative study. J. Clin. Pathol. 2011, 64, 215–219. [Google Scholar] [CrossRef]
- Jobsen, J.J.; Scheijmans, L.J.E.E.; Smit, W.G.J.M.; Stenfert Kroese, M.C.; Struikmans, H.; van der Palen, J. Breast-conserving therapy for primary Ductal Carcinoma in Situ in The Netherlands: A multi-center study and population-based analysis. Breast 2018, 42, 3–9. [Google Scholar] [CrossRef]
- Kuhl, C.K.; Strobel, K.; Bieling, H.; Leutner, C.; Schild, H.H.; Schrading, S. Supplemental Breast MR Imaging Screening of Women with Average Risk of Breast Cancer. Radiology 2017, 283, 361–370. [Google Scholar] [CrossRef]
- Stehouwer, B.L.; Merckel, L.G.; Verkooijen, H.M.; Peters, N.H.; Mann, R.M.; Duvivier, K.M.; Mali, W.P.; Peeters, P.H.; Veldhuis, W.B.; van den Bosch, M.A. 3-T breast magnetic resonance imaging in patients with suspicious microcalcifications on mammography. Eur. Radiol. 2014, 24, 603–609. [Google Scholar] [CrossRef]
- Greenwood, H.I.; Heller, S.L.; Kim, S.; Sigmund, E.E.; Shaylor, S.D.; Moy, L. Ductal carcinoma in situ of the breasts: Review of MR imaging features. Radiographics 2013, 33, 1569–1588. [Google Scholar] [CrossRef]
- Peters, N.H.; Borel Rinkes, I.H.; Zuithoff, N.P.; Mali, W.P.; Moons, K.G.; Peeters, P.H. Meta-analysis of MR imaging in the diagnosis of breast lesions. Radiology 2008, 246, 116–124. [Google Scholar] [CrossRef]
- Lehman, C.D.; Gatsonis, C.; Kuhl, C.K.; Hendrick, R.E.; Pisano, E.D.; Hanna, L.; Peacock, S.; Smazal, S.F.; Maki, D.D.; Julian, T.B.; et al. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N. Engl. J. Med. 2007, 356, 1295–1303. [Google Scholar] [CrossRef]
- Kuhl, C.K.; Schrading, S.; Bieling, H.B.; Wardelmann, E.; Leutner, C.C.; Koenig, R.; Kuhn, W.; Schild, H.H. MRI for diagnosis of pure ductal carcinoma in situ: A prospective observational study. Lancet 2007, 370, 485–492. [Google Scholar] [CrossRef]
- Saadatmand, S.; Obdeijn, I.M.; Rutgers, E.J.; Oosterwijk, J.C.; Tollenaar, R.A.; Woldringh, G.H.; Bergers, E.; Verhoef, C.; Heijnsdijk, E.A.; Hooning, M.J.; et al. Survival benefit in women with BRCA1 mutation or familial risk in the MRI screening study (MRISC). Int. J. Cancer 2015, 137, 1729–1738. [Google Scholar] [CrossRef]
- Evans, D.G.; Kesavan, N.; Lim, Y.; Gadde, S.; Hurley, E.; Massat, N.J.; Maxwell, A.J.; Ingham, S.; Eeles, R.; Leach, M.O.; et al. MRI breast screening in high-risk women: Cancer detection and survival analysis. Breast Cancer Res. Treat 2014, 145, 663–672. [Google Scholar] [CrossRef]
- Passaperuma, K.; Warner, E.; Causer, P.A.; Hill, K.A.; Messner, S.; Wong, J.W.; Jong, R.A.; Wright, F.C.; Yaffe, M.J.; Ramsay, E.A.; et al. Long-term results of screening with magnetic resonance imaging in women with BRCA mutations. Br. J. Cancer 2012, 107, 24–30. [Google Scholar] [CrossRef]
- Mann, R.M.; Athanasiou, A.; Baltzer, P.A.T.; Camps-Herrero, J.; Clauser, P.; Fallenberg, E.M.; Forrai, G.; Fuchsjäger, M.H.; Helbich, T.H.; Killburn-Toppin, F.; et al. Breast Cancer Screening in Women with Extremely Dense Breasts Recommendations of the European Society of Breast Imaging (EUSOBI). Eur. Radiol. 2022, 32, 4036–4045. [Google Scholar] [CrossRef]
- Sickles, E.; D’Orsi, C.J.; Bassett, L.W. ACR BI-RADS® Mammography. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Vereinbarung von Qualitätssicherungsmaßnahmen nach § 135 Abs. 2 SGB V zur kurativen Mammographie (Mammographie-Vereinbarung). 2011: Deutsches Ärzteblatt International Jg. 108 Heft 14. A-791–A-796. Available online: https://www.referenzzentrum-ms.de/site/assets/files/2132/kurative_mammographie_endversion.pdf (accessed on 21 February 2023).
- Morris, E.A.; Lee, C.H. ACR BI-RADS® Magnetic Resonance Imaging. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Bent, C.K.; Bassett, L.; D’Orsi, C.J.; Sayre, J. The positive predictive value of BI-RADS microcalcification descriptors and final assessment categories. AJR Am. J. Roentgenol. 2010, 194, 1378–1383. [Google Scholar] [CrossRef]
- Aminololama-Shakeri, S.; Abbey, C.K.; Gazi, P.; Prionas, N.D.; Nosratieh, A.; Li, C.S.; Boone, J.M.; Lindfors, K.K. Differentiation of ductal carcinoma in-situ from benign micro-calcifications by dedicated breast computed tomography. Eur. J. Radiol. 2016, 85, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Strobel, K.; Schrading, S.; Hansen, N.L.; Barabasch, A.; Kuhl, C.K. Assessment of BI-RADS category 4 lesions detected with screening mammography and screening US: Utility of MR imaging. Radiology 2015, 274, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.C.; Wong, F.L.; Jamison, P.M.; Jones, S.F.; Galaska, L.; Brady, K.T.; Wethers, B.; Stokes-Townsend, G.A. Implementation of the National Breast and Cervical Cancer Early Detection Program: The beginning. Cancer 2014, 120 (Suppl. S16), 2540–2548. [Google Scholar] [CrossRef] [PubMed]
- Akita, A.; Tanimoto, A.; Jinno, H.; Kameyama, K.; Kuribayashi, S. The clinical value of bilateral breast MR imaging: Is it worth performing on patients showing suspicious microcalcifications on mammography? Eur. Radiol. 2009, 19, 2089–2096. [Google Scholar] [CrossRef] [PubMed]
- Mandelson, M.T. Breast Density as a Predictor of Mammographic Detection: Comparison of Interval- and Screen-Detected Cancers. J. Natl. Cancer Inst. 2000, 92, 1081–1087. [Google Scholar] [CrossRef]
- Boyd, N.F.; Guo, H.; Martin, L.J.; Sun, L.; Stone, J.; Fishell, E.; Jong, R.A.; Hislop, G.; Chiarelli, A.; Minkin, S.; et al. Mammographic density and the risk and detection of breast cancer. N. Engl. J. Med. 2007, 356, 227–236. [Google Scholar] [CrossRef]
- Straub, L.; Riedel, J.; Luppa, P.B.; Wissing, J.; Artmann, A.; Kiechle, M.; Seifert-Klauss, V.R. Mammographic Density and Vitamin D Levels—A Cross-sectional Study. Geburtshilfe Frauenheilkd. 2017, 77, 257–267. [Google Scholar] [CrossRef]
- Bakker, M.F.; de Lange, S.V.; Pijnappel, R.M.; Mann, R.M.; Peeters, P.H.M.; Monninkhof, E.M.; Emaus, M.J.; Loo, C.E.; Bisschops, R.H.C.; Lobbes, M.B.I.; et al. Supplemental MRI Screening for Women with Extremely Dense Breast Tissue. N. Engl. J. Med. 2019, 381, 2091–2102. [Google Scholar] [CrossRef]
- Fasching, P.A.; Gass, P.; Häberle, L.; Volz, B.; Hein, A.; Hack, C.C.; Lux, M.P.; Jud, S.M.; Hartmann, A.; Beckmann, M.W.; et al. Prognostic effect of Ki-67 in common clinical subgroups of patients with HER2-negative, hormone receptor-positive early breast cancer. Breast Cancer Res. Treat 2019, 175, 617–625. [Google Scholar] [CrossRef]
- Freitas, V.; Li, X.; Amitai, Y.; Au, F.; Kulkarni, S.; Ghai, S.; Mulligan, A.M.; Bromley, M.; Siepmann, T. Contralateral Breast Screening with Preoperative MRI: Long-Term Outcomes for Newly Diagnosed Breast Cancer. Radiology 2022, 304, 297–307. [Google Scholar] [CrossRef]
- Baltzer, P.A.T.; Bennani-Baiti, B.; Stöttinger, A.; Bumberger, A.; Kapetas, P.; Clauser, P. Is breast MRI a helpful additional diagnostic test in suspicious mammographic microcalcifications? Magn. Reson. Imaging 2018, 46, 70–74. [Google Scholar] [CrossRef]
- Narod, S.A.; Iqbal, J.; Giannakeas, V.; Sopik, V.; Sun, P. Breast Cancer Mortality After a Diagnosis of Ductal Carcinoma In Situ. JAMA Oncol. 2015, 1, 888–896. [Google Scholar] [CrossRef]
- Feinberg, J.; Wetstone, R.; Greenstein, D.; Borgen, P. Is DCIS Overrated? Cancer Treat Res. 2018, 173, 53–72. [Google Scholar] [CrossRef]
- Sagara, Y.; Julia, W.; Golshan, M.; Toi, M. Paradigm Shift toward Reducing Overtreatment of Ductal Carcinoma In Situ of Breast. Front. Oncol. 2017, 7, 192. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Benign Lesions (n = 36) | Malignant Lesions (n = 22) | (p-Value) | |
|---|---|---|---|
| Age in years Median (range) | 57 (45–74) | 57.5 (45–80) | 0.290 |
| Menopausal status Premenopausal n (%) Postmenopausal n (%) | 6 (15.4%) 30 (84.6%) | 6 (28.6%) 16 (71.4%) | 0.306 |
| Average BMI (Kg/m²) (SD) | 25.72 (5.26) | 25.98 (3.35) | 0.855 |
| Breast density n (%) a b c d | 3 (8.33%) 11 (30.56%) 19 (52.78%) 3 (8.33%) | 3 (13.64%) 12 (54.55%) 6 (27.27%) 1 (4.55%) | 0.048 * |
| Average number of children (SD) | 1.67 (0.92) | 1.67 (1.07) | 1.000 |
| Patient | MA | BPE | Breast MRI | D | MG | Modality | Histology/IHC/TNM |
|---|---|---|---|---|---|---|---|
| 1 | I | Mild | Mass, circumscribed, oval | c | Localization outside the MG coverage near the chest wall | Core biopsy guided by ultrasound | 1.4 cm G1 NST/ER 90%, PR 30%, Ki-67 5%, HER2 negative/pT1c pN0 L0 V0 Pn1 G1 |
| 2 | II | Moderate | NME, segmental, heterogeneous | b | No MCs | MRI-guided vacuum-assisted biopsy | 13.4 cm low-grade DCIS |
| 3 | II | Moderate | NME, linear | b | Unilateral MCs in different position | MRI-guided vacuum-assisted biopsy | 0.6 cm G1 tubular carcinoma/ER 90%, PR 30%, KI-67 10%, HER2 negative/pT1b pN0 L0 V0 Pn0 G1 associated with 3.2 cm low-grade DCIS |
| 4 | I | Minimal | Mass, irregular, not circumscribed-spiculated, heterogeneous | b | Unilateral MCs in different position | Core needle biopsy | 0.5 cm G3 NST/ER 90%, PR negative, Ki-67 60%, HER2 negative/ypT0 pN0 L0 V0 Pn0 |
| 5 | II | Moderate | NME, grouped, regional | c | No MCs | Partial excision | 0.7 cm G2 NST//ER 90%, PR 40% Ki-67 20% HER2 negative/pT1b pN0 L0 V0 Pn0 G2 associated with 5.0 cm low-grade DCIS |
| 6 | I | Mild | NME, linear, heterogeneous | b | No MCs | Duct excision | Fibrocystic changes |
| 7 | I | Mild | NME, diffuse, heterogeneous | b | No MCs | Core needle biopsy guided by ultrasound | UDH |
| 8 | I | Minimal | NME, linear, homogeneous | c | Unilateral MCs in different position | Partial excision | Fibrocystic changes |
| 9 | I | Moderate | NME, focal, homogeneous | c | Unilateral MCs in different position | Partial excision | FEA |
| Patient | MA | BPE | ACR | Histology and Size | Shape and Distribution |
|---|---|---|---|---|---|
| 1 | 2 | Moderate | B | Intermediate-grade DCIS (6.5 cm) | No contrast enhancement in the position of macrocalcifications, multiple small foci on both sides. |
| 2 | 1 | Marked | C | Low-grade DCIS (0.15 cm) | No contrast enhancement in the position of macrocalcifications. |
| 3 | 1 | Marked | C | Low-grade DCIS (5.6 cm) | No contrast enhancement in the position of macrocalcifications, multiple cysts on both sides. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pöschke, P.; Wenkel, E.; Hack, C.C.; Beckmann, M.W.; Uder, M.; Ohlmeyer, S. Low-Risk Women with Suspicious Microcalcifications in Mammography—Can an Additional Breast MRI Reduce the Biopsy Rate? Diagnostics 2023, 13, 1197. https://doi.org/10.3390/diagnostics13061197
Pöschke P, Wenkel E, Hack CC, Beckmann MW, Uder M, Ohlmeyer S. Low-Risk Women with Suspicious Microcalcifications in Mammography—Can an Additional Breast MRI Reduce the Biopsy Rate? Diagnostics. 2023; 13(6):1197. https://doi.org/10.3390/diagnostics13061197
Chicago/Turabian StylePöschke, Patrik, Evelyn Wenkel, Carolin C. Hack, Matthias W. Beckmann, Michael Uder, and Sabine Ohlmeyer. 2023. "Low-Risk Women with Suspicious Microcalcifications in Mammography—Can an Additional Breast MRI Reduce the Biopsy Rate?" Diagnostics 13, no. 6: 1197. https://doi.org/10.3390/diagnostics13061197
APA StylePöschke, P., Wenkel, E., Hack, C. C., Beckmann, M. W., Uder, M., & Ohlmeyer, S. (2023). Low-Risk Women with Suspicious Microcalcifications in Mammography—Can an Additional Breast MRI Reduce the Biopsy Rate? Diagnostics, 13(6), 1197. https://doi.org/10.3390/diagnostics13061197