Abstract
Mechanical ventilation (MV) is a life-saving respiratory support therapy, but MV can lead to diaphragm muscle injury (myotrauma) and induce diaphragmatic dysfunction (DD). DD is relevant because it is highly prevalent and associated with significant adverse outcomes, including prolonged ventilation, weaning failures, and mortality. The main mechanisms involved in the occurrence of myotrauma are associated with inadequate MV support in adapting to the patient’s respiratory effort (over- and under-assistance) and as a result of patient-ventilator asynchrony (PVA). The recognition of these mechanisms associated with myotrauma forced the development of myotrauma prevention strategies (MV with diaphragm protection), mainly based on titration of appropriate levels of inspiratory effort (to avoid over- and under-assistance) and to avoid PVA. Protecting the diaphragm during MV therefore requires the use of tools to monitor diaphragmatic effort and detect PVA. Diaphragm ultrasound is a non-invasive technique that can be used to monitor diaphragm function, to assess PVA, and potentially help to define diaphragmatic effort with protective ventilation. This review aims to provide clinicians with an overview of the relevance of DD and the main mechanisms underlying myotrauma, as well as the most current strategies aimed at minimizing the occurrence of myotrauma with special emphasis on the role of ultrasound in monitoring diaphragm function.
1. Introduction
Mechanical ventilation (MV) aims to ensure adequate gas exchange and to totally or partially replace the action of the respiratory muscles, which can be overloaded during acute respiratory failure. However, MV has widely recognized potentially harmful pulmonary effects [1,2] leading to the proposition of several ventilation strategies to limit the mechanical stress applied to the lungs [3]. More recently, it has been identified that MV can also injure the diaphragm due to a variety of supposed mechanisms, referred to as “myotrauma” [4], which leads to the impairment of the diaphragm function, referred to as ventilator-induced diaphragmatic dysfunction—VIDD [5].
VIDD is conceptualized as a reduction in the diaphragmatic force-generating capacity, specifically related to the use of MV [5] that occurs shortly after the onset of the MV [6] in a progressive, time-dependent manner [7], and is influenced by different MV modes and associated risk factors [7].
The recognition of diaphragm dysfunction (DD) is relevant in critically ill patients because it is a common event that occurs in the different stages of critical illness, since admission [8], during the early stages of MV [7], during weaning [9,10,11], and even in the recovery stages [12]. In addition, critically ill patients are often vulnerable to numerous risk factors concomitant with MV, such as sepsis, organ dysfunction, and medications that may contribute to diaphragmatic injury [8,13,14,15]. Also, there is compelling evidence on the unfavorable impact of diaphragmatic dysfunction on morbidity in critically ill patients, including weaning difficulties [7,8,9,10,11], ICU readmission [16], and mortality [8,17].
Considering the relevance of diaphragmatic dysfunction in critically ill patients, the current literature has been committed to prioritizing the care of patients under MV in order to monitor diaphragm function in the ICU and to minimize or avoid diaphragm myotrauma to prevent the development of VIDD [18].
Knowledge about the main mechanisms involved in the occurrence of myotrauma underlies the strategies that can be used to protect the diaphragm during MV [19,20].
The purpose of this review is to explore evolving concepts about the use of diaphragm ultrasound as a technique not only to assess diaphragm function but also to help monitor diaphragmatic effort for protective ventilation. We present an overview of the relevance of diaphragm dysfunction in critically ill patients on MV, its main mechanisms, and strategies to prevent it, focusing on ultrasound as a tool for monitoring diaphragmatic function.
2. Diaphragm Myotrauma-Mechanisms
Evidence of diaphragmatic muscle injury in critically ill mechanically ventilated patients has been widely appreciated and recognized [21] and is based on several clinical [7,22,23,24] and experimental studies [25,26,27,28,29].
To understand diaphragmatic dysfunction in critically ill patients, efforts have been made to standardize terminology, with the aim of ensuring communication between researchers. Thus, the term myotrauma has been adopted to refer broadly to the ventilator-associated diaphragmatic acute muscle injury [4].
According to the most current evidence, myotrauma is presumably associated with several mechanisms linked to the inappropriate management of MV, mainly related to the inadequacy of ventilatory support to suit the patient’s respiratory effort (over- and under-assistance) and as a result of AVP. The evidence for these mechanisms is summarized below [4]:
- Over-assistance myotrauma (disuse atrophy) represents the effect of excessive respiratory support and reduced respiratory drive/effort, resulting in disuse atrophy and weakness. It is the best documented form of myotrauma, in both experimental studies [30,31] and clinical studies reporting histological [24,32,33], functional [7], and imaging evidence of disuse atrophy [23,34,35,36]. It is important to emphasize that disuse atrophy can occur even in assisted ventilation modes [37].
- Under-assistance myotrauma (load-induced, concentric contraction) is a recognized form of muscle injury that occurs when ventilatory support is insufficient or unable to reduce the load on the diaphragm during increased respiratory drive (load-induced diaphragm injury). The persistence of high levels of respiratory efforts during under-assistance results in high muscle tension during concentric contraction [23,38]. In experimental models, the diaphragmatic injury is characterized by an inflammatory infiltration and the disruption of sarcomere and sarcolemma.
- Eccentric myotrauma (load-induced, eccentric contraction) occurs when there is contractile activity of the diaphragm during fiber lengthening instead of shortening. Eccentric contraction is observed in the expiratory phases of ventilation: (1) when the diaphragm exerts an expiratory brake to preserve the end-expiratory lung volume [39]; (2) in some forms of asynchrony (reverse triggering, early cycling, ineffective effort) [40,41,42].
- Expiratory myotrauma—in experimental models, it was observed that the use of high PEEP reduces the final expiratory length of the diaphragm and can cause loss of sarcomeres, resulting in longitudinal atrophy with impairment of the length-tension ratio of the diaphragm [43].
3. Diaphragm Dysfunction-Recognition
Considering the main mechanisms involved in myotrauma, more recently, the literature has been dedicated to the recognition and early monitoring of diaphragmatic dysfunction, allowing the appreciation and development of rational strategies with the potential to minimize or prevent VIDD [41] (Figure 1).
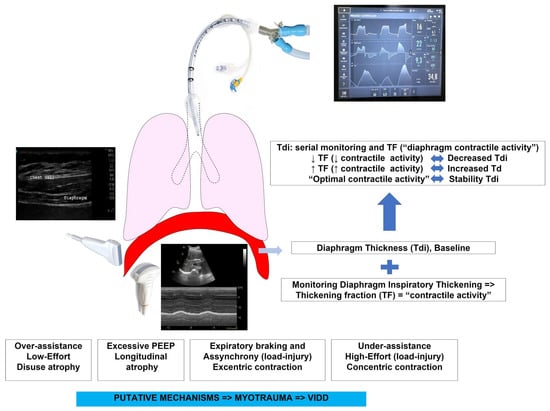
Figure 1.
Possible rationale use of ultrasound to monitor diaphragm function in critically ill patients on mechanical ventilation (monitoring effort, assessing atrophy, assessing PVA). TF—thickening fraction; Tdi—diaphragm thickness; PEEP—positive end-expiratory pressure; VIDD—ventilator-induced diaphragmatic dysfunction.
Any strategy aimed at protecting the diaphragm must examine its functional aspects, with a particular emphasis on monitoring the diaphragm’s effort [20]. The most grounded approach in recent literature is to maintain an adequate level of inspiratory diaphragmatic effort and curb different forms of AVP [20,41].
Various tools can be employed to monitor the function/activity of the diaphragm. However, the various peculiarities of these techniques make them more or less appropriate in critically ill patients [10,19,44]. The gold standard for assessing diaphragm function is based on measuring transdiaphragmatic pressure after magnetic stimulation of the phrenic nerves, which, however, is generally unavailable, thus requiring the development and implementation of more viable tests, among which diaphragmatic ultrasound emerged [19,20,41,42].
4. Diaphragm Ultrasound-DUS
Diaphragmatic ultrasonography has been shown to be a relevant tool for assessing diaphragm function that reached significance in critically ill patients due to its numerous advantages [45,46,47]: (a) The ultrasound devices needed to perform DUS are simple equipment, widely available in ICUs; (b) ultrasound machines are portable, which allow DUS to be performed at the bedside in a safe, repeatable and non-invasive way, without the need to transport the patient; (c) the improvement of the technique allows its fast, precise, reproducible, and repeatable execution.
The devices used to perform DUS have experienced advances (probes with better resolutions). In addition, the improvement and standardization of the technique allowed for the acquisition of reliable images of the diaphragm function [47,48,49].
4.1. Ultrasound of Diaphragm–Brief Review of the Technique
The diaphragm is a dome-shaped, musculo-fibrous membrane. It is the main inspiratory muscle. Evaluation of the diaphragm with ultrasound is based on its anatomy and function. During inspiration, when the diaphragm contracts, the muscle fibers shorten, thicken, and stiffen, displacing the entire musculotendinous structure of the diaphragm, lowering its dome, moving the abdominal contents caudally and expanding the lower thoracic cavity [47].
Using the ultrasound, the diaphragm may be explored through two acoustic windows [46,47,50] (Figure 2):
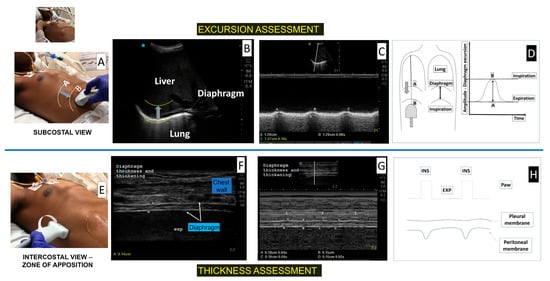
Figure 2.
Diaphragm ultrasound to assess excursion and thickness – technique description in a critical care patient on mechanical ventilation. (Panel A): Probe positioning on subcostal area. (Panel B): Bidimensional view displaying the diaphragm as a white hyperechoic curved line (yellow traced) separating lung from liver. (Panel C): M-Mode view displaying a normal excursion during tidal breathing after a brief disconnection of the ventilatory support. (Panel D): Graphic illustrative of the excursion measurement. (Panel E): Probe positioning on the intercostal area (zone of apposition, ZA)—after positioning the linear probe perpendicularly to the costal wall, we rotated the probe (counterclockwise) to obtain the corresponding ultrasound image on the right. (Panel F): Bidimensional view displaying the diaphragm as a hypoechoic structure surrounded by 2 hyperechoic lines (pleural and peritoneal membranes). (Panel G): M-Mode view displaying a normal inspiratory thickening of diaphragm during tidal breathing in a critical care patient on mechanical ventilation (I = inspiration; points A and C represent end-inspiratory diaphragm thickness; points B and D represent end-expiratory diaphragm thickness. (Panel H): Graphic illustrative of the thickness and thickening measurement.
- -
- In the subcostal region, the diaphragm is seen as a deep curved structure that separates the thorax from the abdomen;
- -
- In the mid-axillary intercostal region, in the zone of apposition (ZA), the diaphragm is identified as a three-layer structure; a hypoechoic inner muscle layer surrounded by two hyperechoic outer membranes (the peritoneum and pleura).
Thus, during diaphragm inspiratory contraction, the ultrasound may observe: (a) the inspiratory caudal displacement (excursion) of the diaphragm in the subcostal region; (b) the end-expiratory thickness of the muscle (at rest) and the thickening and stiffening of the diaphragm during inspiration, in the ZA.
In critically ill patients, a unilateral assessment of the right diaphragm is acceptable unless unilateral dysfunction is suspected (requiring bilateral assessment) [48].
Recently, a meeting of experts sought to outline a consensus focusing mainly on various technical/methodological aspects of ultrasound of the diaphragm. This consensus is therefore an important reference to standardize and universalize the performance of diaphragm ultrasound and should be regularly consulted in the application of the method.
Excursion assessment: a low-frequency probe (3.5–5 MHz) was positioned below the right costal margin, between the midclavicular and anterior axillary line, directing medial-cranially and dorsally, tracking the posterior third of the right hemidiaphragm in a two-dimensional (2D) mode. Next, the M-mode exploration line was positioned as perpendicular as possible in relation to the diaphragm domus, in order to measure the movement of anatomical structures over time, and therefore, measure diaphragm mobility by placing calipers at the bottom and top of the diaphragmatic inspiratory slope [47,51,52].
During inspiration, the diaphragm descended in the craniocaudal direction, towards the probe [46,47,50]. Thus, during inspiration, absent or greatly reduced excursion (below lower thresholds) or movement contrary to the probe (paradoxical) indicated an abnormality (dysfunction).
In patients on ventilatory support, a brief disconnection of the ventilator (T-tube) or maintaining minimal levels of CPAP was necessary to assess diaphragmatic movement and thus eliminate passive inflation bias by ventilator pressure [46]. The downward displacement of the diaphragm may result from the force of the diaphragm contraction by itself, and also the passive lung inflation performed by the ventilator, indicating that diaphragm excursion should only be assessed during unassisted breaths [53,54].
Excursion can be measured during tidal breathing and during maximal inspiratory effort in cooperative patients (best excursion) in order to assess diaphragm dysfunction [55].
Diaphragm thickness assessment: a high frequency linear probe (>7–10 MHz) was positioned perpendicular to the lateral chest wall, between the midaxillary and anterior axillary line, between the 9th and 10th intercostal space (apposition zone–ZA). The diaphragm is seen usually at a depth of two to four centimeters from the skin, as a hypoechoic inner muscle layer surrounded by the peritoneum and pleura membranes. Diaphragmatic thickness was measured at the end of expiration (Tdi,exp) and inspiration (Tdi,insp) as the distance between the diaphragmatic pleura and the peritoneum using the 2D or M-mode [47,56,57]. Although around 1.5 mm has been reported as a lower limit for normal diaphragm thickness in healthy individuals [58], in very thin healthy women, thickness values of up to 1.2 mm can be observed [57]. Diaphragm thickening fraction (TF) is defined as the percentage change in diaphragm thickness during inspiration [(Tdi,insp) − (Tdi,exp)/(Tdi,exp)] × 100 [46,47,50].
Diaphragm thickness (Tdi) may depict atrophy, while the thickening fraction (TF) represents diaphragm inspiratory activity (effort) [59,60,61].
Reference values for diaphragmatic excursion, thickness and thickening in healthy individuals are described in the Supplementary Table (Table S1).
4.2. Diaphragm Ultrasound in Respiratory Muscle Monitoring in Critically Ill Patients
The following is an overview of the recent evidence on diaphragmatic and intercostal (IC) ultrasound assessment, focusing on clinical applications aimed at promoting diaphragmatic protective MV strategies (Table 1).

Table 1.
An overview of recent evidence on diaphragmatic and intercostal ultrasound assessment, focusing on clinical applications aimed at promoting diaphragmatic protective mechanical ventilation strategies. ICU—Intensive Care Unit; DE—diaphragmatic excursion; Pdi—transdiaphragmatic pressure; MV—mechanical ventilation; DD—Diaphragm Dysfunction; SBT—Spontaneous breathing trial; PSV—pressure support ventilation; OR—odds ratio; ARF—acute respiratory failure; TF—thickening fraction; ICUAW—intensive care unit acquired weakness; Ptr,stim—twitch tracheal pressure; ACV—Assist control ventilation; US—ultrasound; MRC—Medical Research council; Tdi—Diaphragm thickness; OTI—orotracheal intubation; Pdrive—driving pressure; CMV—controlled mechanical ventilation; ΔTdi/d—Daily atrophy rate; SD—standard deviation; CPAP—Continuous Positive Airway Pressure; CSA—cross-sectional area; PPV—positive predictive value; DUS—diaphragmatic ultrasound; RR—respiratory rate; Pes—esophageal pressure; Pga—gastric pressure; NIV—noninvasive ventilation; SB—spontaneous breath; PTPdi—diaphragm pressure—time product; EAdi—diaphragmatic electrical activity; AMV—assisted mechanical ventilation; PTPes—esophageal pressure–time product; EXdi—diaphragmatic excursion; C—intercostal; RV—residual volume; FRC—functional residual capacity; TLC—total lung capacity; IC—intercostal; COPD—chronic obstructive pulmonary disease; FEV1—Forced Expiratory Volume; CT—Computerized Tomographic; WOB—work of breathing.
4.2.1. To Diagnose Diaphragmatic Dysfunction
Diaphragm dysfunction can be identified with DUS. Diaphragm dysfunction is characterized on DUS as an abnormality on diaphragmatic excursion indicated by reduced mobility (less than the reference value), absent, or paradoxical (mainly seen in deep breathing and sniff maneuvers) [62]. In critically ill patients on MV, the most commonly used criterion to indicate diaphragmatic dysfunction is a diaphragmatic excursion < 10–11 mm [11,63] (Figure 3).
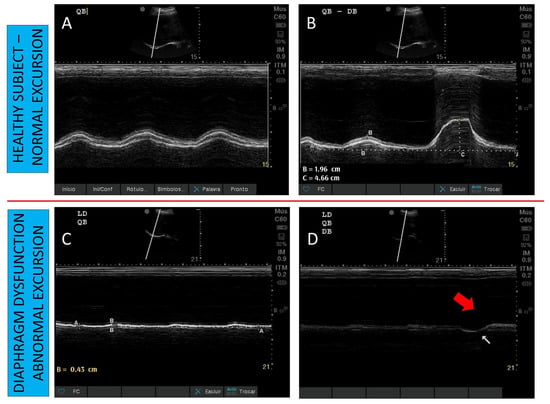
Figure 3.
Diaphragm ultrasound to monitor dysfunction according to diaphragmatic excursion. (Panel A): Normal excursion during tidal breathing in a healthy subject. (Panel B): Normal excursion during tidal and deep breathing in a healthy subject. (Panel C): Reduced excursion during tidal breathing in a patient with diaphragm dysfunction. (Panel D): Absent excursion during tidal breathing, and paradoxical excursion during deep breathing (red arrow) in a patient with diaphragm dysfunction.
Ultrasound-diagnosed DD is associated with adverse outcomes (longer MV and weaning times, as well as higher mortality). Abnormal diaphragmatic thickening fraction, defined as a diaphragmatic thickening fraction of <20%, has also been used to diagnose DD [64]. According to previous studies, the prevalence of DD has been found to be 28–38% among patients on MV eligible for an SBT [11,37], and 34% among patients on MV for prolonged periods [64]. Patients with DD seen on ultrasound had worse outcomes (prolonged MV, weaning failures and increased mortality) [11,63,64].
4.2.2. Ultrasound of Diaphragm to Monitor Diaphragm Atrophy
Diaphragm atrophy is a component of VIDD, and has been shown in experimental [31,76,77] and clinical studies that demonstrated the presence of histological atrophy (defined as a decrease in diaphragm fiber cross-sectional area in diaphragm biopsy) even after few hours of MV [7,21,24,37].
Several studies have used the measurement of diaphragmatic thickness at the end of expiration (Tdi) as a non-invasive surrogate of diaphragmatic muscle mass, thus allowing the assessment of diaphragmatic atrophy in critically ill patients, especially those on MV [45,78]. In addition, repeated assessment of Tdi over the days of MV may indicate changes in diaphragm configuration, including muscle thinning, that may be indicative of atrophy [22,23,34,35,36].
The wide range of values to determine the lower limit of Tdi (between 1.6 and 2.3 mm) both in healthy individuals and in critically ill patients on MV in different studies [56,57,58,78,79] makes it difficult to establish a cut-off to define atrophy in a single measurement. Currently, there is more consistent evidence on the relevance of serial thickness monitoring to define the occurrence of atrophy, one of the markers of diaphragm dysfunction [23,34,35,36,80]. Using DUS, atrophy has been defined as a decrease of 10% or more of the diaphragm in serial measurements [23,80].
Goligher et al. [23] studied the evolution of diaphragm thickness over time during MV in 107 adult patients. They found that over the first week, mainly in the first 72 h of MV, diaphragm thickness decreased (more than 10%) in 44% of patients, and this atrophy was associated with low diaphragm contractile activity. Later on, these authors reassessed whether diaphragm atrophy developing during MV could impact clinical outcomes [22]. They found that atrophy was associated with prolonged ventilation and ICU admission, and a higher risk of complications.
Subsequently, other studies observed the relationship between atrophy and MV [35,36]. Schepens et al. [35] described that diaphragm atrophy (mean change in thickness of 32%) occurs quickly after the onset of MV in 54 ICU adult patients. The degree of atrophy was associated with the length of MV [35]. Zambon et al. [36] used ultrasound to measure the diaphragm thickness daily, from the first day of MV till discharge in 40 adult patients, in order to quantify diaphragm atrophy and identify risk factors. They observed a gradual reduction in diaphragm thickness (estimated as a daily atrophy rate) which presented a linear relationship with ventilator support ranging from −7.5% under controlled MV to +2.3% during spontaneous breathing.
Vivier et al. [80] studied a sample of critically ill patients to assess serial diaphragm thickness during the first five days of critical illness. They found that diaphragm atrophy (Tdi decrease of ≥ 10%) occurred in 48% of patients, and atrophy was associated with septic shock, organ failure, or invasive MV.
Regarding a single measurement of Tdi to assess atrophy, Dot et al. [66] investigated whether expiratory thickness (Tdi) measured by ultrasound was able to predict diaphragm atrophy, defined by a decrease in diaphragm fiber cross-section area (CSA) obtained through diaphragm biopsy in 35 ventilated organ donors. They found that all of the donor group presented atrophy (reduced CSA), but decreased Tdi was observed in 74%. Diaphragm Tdi measurement demonstrated a high positive predictive value (96%) but a low negative predictive value (17%) for determining the presence of diaphragm atrophy, indicating that the diaphragm Tdi was able to detect atrophy, but cannot rule it out completely.
However, even a single Tdi measurement at the early stages of critical illness can provide relevant information. Recently, Sklar et al. [78] demonstrated that in critically ill patients on MV, a low diaphragmatic muscle mass (baseline Tdi of 2.3 mm or less) measured by ultrasound in the first 36 h after intubation, was associated with adverse clinical outcomes.
4.2.3. DUS to Monitor Effort–Diaphragm Protective Ventilation
Our understanding of the mechanisms of ventilator-induced diaphragmatic dysfunction (VIDD) has increased in recent years. Research now focuses on methods to monitor diaphragm function in parallel with efforts to prevent VIDD. The institution of assisted ventilation (“spontaneous breathing”) as early as possible seems to meet the efforts to prevent VIDD, but poses challenges to also comply with MV with “lung protection”.
Also, as already demonstrated in previous studies, diaphragmatic atrophy due to disuse can occur even in assisted ventilation [37,67,77] indicating that simply triggering the ventilator is not enough to prevent diaphragm atrophy. In addition, clinical variables and ventilator settings are not able to detect contractility and risk of diaphragm atrophy. [67].
At this moment, the titration of the inspiratory effort and the synchronization in the patient-ventilator interaction seem to provide the best evidence in the simultaneous protection of the lung and the diaphragm, although the efficacy of such strategies is mainly supported by physiological and epidemiological data [19,20,41,42,44].
Recent studies are now in course to assess the feasibility of strategies on titrating ventilation and sedation, in order to optimize the respiratory effort to achieve lung and diaphragm protective ventilation [81]. In a recent trial [82], inspiratory support was titrated based on a predefined “diaphragm-protective” range of transdiaphragmatic pressure swings (3–12 cm H2O). This strategy, based on patient breathing effort, increased the time that patients had this predefined “diaphragm-protective” effort without compromising tidal volumes and transpulmonary pressures.
Although in these previous studies the respiratory effort titration was based on the monitoring of respiratory pressures, some authors proposed that the DUS can be useful in assessing the contractile activity of the diaphragm, and therefore also in assessing the respiratory effort [19,20,22,44].
Assessment of the diaphragm thickening fraction (TF) as a surrogate of contractile activity of the diaphragm (the level of respiratory effort) is a reasonable approach [22,49]. Adjustment of ventilatory support to avoid excessive or insufficient ventilatory assistance may mitigate MV damage on the diaphragm. The titration of ventilatory support to maintain the contractile activity of the diaphragm (effort) within physiological limits may prevent changes in diaphragm configuration [22,23] (Figure 4).
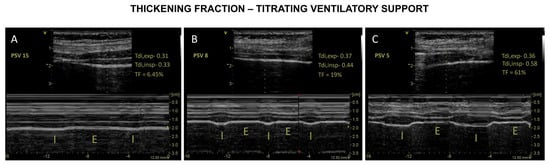
Figure 4.
Diaphragm ultrasound to monitor effort. Titrating effort according to thickening fraction (TF). Panel A—Reduced TF suggestive of over-assistance (PSV 15 cm H2O). Panel B—“Ideal” TF suggestive of appropriated effort (PSV 8 cm H2O). Panel C—Increased TF suggestive of under-assistance (PSV 5 cm H2O).
Although the optimal level of diaphragmatic activity is uncertain, Goligher et al. [23] showed that diaphragm thickness was stable over time, at levels of contractile activity that are typically observed in healthy subjects during resting tidal breathing. In this study, diaphragm contractile activity directly influenced the change in diaphragm thickness over time. For the first time, it was demonstrated that diaphragm thickness (Tdi) decreased over time during lower contractile activity (TF) while Tdi increased during higher contractile activity (TF). In a subsequent study of this group, a TF between 15–30% during the first few days of MV was associated with stable muscle thickness and a shorter duration of ventilation [22].
These findings along with studies that observed the existence of a correlation between TF and diaphragm effort [65,68] serve as an argument for assuming that maintaining a TF of 15–30% may indicate a safety threshold for titration of effort during MV [49].
However, it should be emphasized that the use of ultrasonography of the diaphragm, particularly the inspiratory thickening fraction (TF), as a surrogate for diaphragmatic effort, is still debated in the literature.
Transdiaphragmatic pressure (Pdi) represents the specific muscle strength of the diaphragm, and its measurement has been considered the gold standard for diaphragm function, particularly after the bilateral magnetic stimulation of phrenic nerves [83]. However, Pdi measurement has been neglected due to its problematic use in clinical settings (unavailability and invasiveness of esophageal and gastric catheters, expertise in interpretation) [84]. To overcome this, ultrasound has been proposed as a non-invasive tool to assess diaphragm function [45]. During inspiration, diaphragmatic contraction promotes the shortening of muscle fibers that can be observed in the apposition zone by ultrasound and quantified. The diaphragm thickening fraction (TF) is the magnitude of the increase in diaphragm thickness during inspiration [46]. Inspiratory thickening of the diaphragm has been proposed as a reflection of the magnitude of diaphragm effort [54], which can be corroborated by studies that evaluated diaphragm thickness in individuals with diaphragmatic paralysis, in which no thickening was seen on ultrasound in subjects who did not recover from diaphragmatic paralysis [85].
However, there are controversial findings regarding the ability of TF to estimate diaphragmatic effort. Vivier et al. [68] investigated whether the thickening fraction (TF) could be indicative of respiratory muscle effort in 12 patients who required planned non-invasive ventilation (NIV) after extubation. The work of breathing in this study was indicated by the transdiaphragmatic pressure-time product (PTPdi). Patients were evaluated during spontaneous breathing and during NIV at three levels of pressure support (5, 10 and 15 cm H2O). The authors found a significant correlation between TF and PTPdi, indicating that changes in diaphragm thickening correlate with the diaphragmatic work of breathing.
Umbrello et al. [54] investigated the performance of diaphragmatic contractile activity seen on ultrasound (diaphragm excursion and thickening fraction, TF) in comparison with classic indices of inspiratory muscle effort (esophageal pressure-time product (PTPes) and diaphragmatic pressure-time product (PTPdi)), during assisted MV in 25 patients admitted to the ICU after major elective surgery who fulfilled criteria for a trial of spontaneous breathing with pressure support (PS) ventilation at different levels of PS (0, 5 and 15 cmH2O). The authors observed that with increasing PS levels, parallel reductions were found between diaphragm TF, PTPes and PTPdi during tidal breathing. Diaphragm TF significantly correlated with PTPes and PTPdi. There was no correlation of any index with the excursion of the diaphragm.
Goligher et al. [45] investigated in five healthy subjects (validation study) the association between the diaphragm thickening fraction with the electrical activity of the diaphragm (EAdi). The TFdi and EAdi were positively correlated. At inspiratory volumes below 50% of inspiratory capacity, passive insufflation did not cause diaphragm thickening, indicating that at clinically relevant inspiratory volumes, diaphragm thickening reflects muscle contraction and not passive insufflation.
In order to estimate reliable measures for assessing respiratory effort, Umbrello et al. [73] investigated variations in esophageal (Delta Pes) and transdiaphragmatic (Delta Pdi) measurements and its derivations (esophageal pressure-time products (PTPes), transdiaphragmatic (PTPdi) and work of breathing (WOB)) in comparison with the variations in diaphragm thickening (TF) and parasternal intercostal thickening (TFic) in 21 critically ill patients on MV with pressure support (PS). Measurements were performed at three PS levels: baseline, 25% and 50% reduction. The authors found that TF was only weakly correlated with esophageal PTP, but this correlation improved after excluding patients with diaphragm dysfunction (as defined by the Gilbert index).
Unlike these previous studies [45,54,68,73], the relationship between thickening fraction and respiratory effort was not observed in other papers, as presented below.
Oppersma et al. [86] investigated the validation of speckle tracking (strain and strain rate) to assess the inspiratory diaphragmatic effort compared to the diaphragm thickening fraction, in 13 healthy volunteers during an inspiratory overload protocol (randomized from 0 to 50% of maximal inspiratory pressure). Diaphragm electrical activity (EAdi) and transdiaphragmatic pressures (Pdi) were also recorded. Strain and strain rate increased with progressive diaphragm loading. Both strain and strain rate were highly correlated with Pdi and EAdi, but TF was not influenced by inspiratory load variations and did not correlate with EAdi and/or Pdi.
Poulard et al. [87] investigated the global and intraindividual relationship between the diaphragmatic thickening fraction (TF) and transdiaphragmatic pressure (Pdi; the PTPdi was calculated) in 14 healthy subjects (in whom they applied variations in the external inspiratory threshold load) and 25 mechanically ventilated (MV) patients at various pressure support settings. They found that in healthy subjects, both changes in Pdi and PTPdi were moderately correlated with TF. In MV patients, changes in Pdi and TF were weakly correlated, indicating that TF was not able to infer the pressure output.
Recently, Steinberger et al. [88] investigated whether the diaphragmatic excursion (DE) and the thickening fraction (TF) measured by ultrasound could reflect the variation in esophageal pressure (Delta Pes) during continuous positive airway pressure (CPAP) ventilation in 46 patients hospitalized for COVID-19 pneumonia. The authors did not find any association between Delta Pes and DE or TF, although only a moderate correlation was observed between variations in Pes oscillation and variations in TF between PEEP and ZEEP.
These controversial findings may arise from many points. (1) Heterogeneity of the population studied: Goligher and Oppersma [45,86] investigated healthy individuals, while Poullard [87] assessed a mixed sample of healthy and mechanically ventilated patients; however, the other studies assessed specific populations of patients (patients requiring planned NIV after extubation [68], patients admitted to the ICU after major elective surgery who met criteria for an SBT [73] and patients with COVID-19 pneumonia on CPAP [88]). (2) The studies have different conditions to test effort: studies applied different protocols of inspiratory loading in healthy individuals [86,87] who could adopt diverse patterns of respiratory muscle recruitment. (3) Regarding the studies on patients, they could be on various configurations of lung volume and chest wall compliance [54,68,73]. (4) In critically ill patients, diaphragm dysfunction (DD) may influence the relationship between diaphragm thickening and inspiratory effort [73], but DD was not tested on the study of Steinberg [88]. (5) It is largely recognized that the thickening fraction associates with a wide range of PTPdi values, which may signify that the degree of diaphragmatic contraction and corresponding work of breathing may vary between subjects [86].
Although these controversies indicate that caution should be taken in interpreting TF as a substitute for respiratory effort, we believe that Goligher’s findings that correlate changes in diaphragm configuration (estimated by Tdi) with diaphragmatic contractile activity (estimated by thickening fraction) may indicate that TF offers a plausible alternative for estimating respiratory effort, whose monitoring is essential for the prevention of diaphragmatic myotrauma [22,23].
5. Patient–Ventilator Asynchrony (PVA)
Patient–ventilator asynchrony (PVA) can be defined as a mismatch between patient effort/demand and ventilator-delivered breaths (regarding time, flow, volume, or pressure) [89].
PVA is not uncommon and may occur in up to a quarter of mechanically ventilated patients [49,90,91], but is often ignored and underestimated.
PVA is associated with adverse effects such as dyspnea, increased work of breathing, auto-PEEP, worsening of pulmonary gas exchange, decreased quantity, and quality of sleep, leading to worse outcomes (increased use of sedation and neuromuscular blockade, prolonged MV, increased duration of MV, and increased mortality [90,92,93,94,95].
PVAs most commonly result from a mismatch in the patient-ventilator interaction during the trigger of the inspiratory cycle phases (ineffective effort, self-trigger, and double trigger) and the end of the inspiratory phase (premature or delayed cycling), in addition to an imbalance in the inspiratory flow (insufficient or excessive) [89].
PVA potentially impacts on diaphragm function and has been proposed as one of the mechanisms linking MV to diaphragm weakness, i.e., myotrauma [19].
Optimal patient-ventilator interaction, without asynchrony, would theoretically be ideal for the diaphragm [89]. More recently, it has been established that performing MV, with lung and diaphragm protection, requires the monitoring of respiratory effort [41]. The DUS can thus be a valuable tool for providing the assessment of the respiratory effort (by measuring the contractile activity of the diaphragm represented by the thickness fraction), in addition to providing the identification of structural alterations in the muscle [4].
As previously described, the main mechanisms associated with myotrauma are: over-assistance leading to respiratory effort suppression and disuse atrophy, under-assistance associated with high effort and load-injury during the inspiratory concentric contraction, eccentric contraction during the expiratory phase, and the longitudinal atrophy.
PVA-associated muscle injury is mainly related to eccentric contraction [4]. In certain types of asynchrony, the patient’s inspiratory efforts (such as ineffective effort) may occur during the expiratory phase, determining eccentric or plyometric contractions (contractions that occur during the fiber stretching) and causing injury to the diaphragm muscle fibers [96,97].
Although the visual inspection of the airflow, volume, and pressure signals on the mechanical ventilator display may point to asynchrony, PVAs may go unnoticed in this method [1,12].
The gold standard for detecting PVA is esophageal pressure monitoring (Pes), providing an accurate inspection of the patient’s inspiratory muscle effort and corresponding ventilatory supply. However, monitoring of Pes remains limited because it is commonly unavailable and has technical pitfalls (e.g., tight control of esophageal balloon volume and location) [89,98].
Diaphragmatic electrical activity (EAdi) is another tool indicated for monitoring PVA, and is also considered a reference technique [99], but with similar limitations to Pes to use in daily practice (unavailability, invasiveness, specialized training for interpretation) [49]. EAdi monitoring can detect trigger delays, early and late cycling, auto-triggering, double-triggering, and wasted efforts.
Considering that the inspiratory diaphragmatic activity (contraction) determines the changes in pleural pressure, it has been argued that DUS may be used to simultaneously monitor the function of the diaphragm and the breathing pattern in order to detect PVA [48,49].
Soilemezi et al. [100] employed simultaneous recordings of diaphragmatic displacement (DUS) and airway pressure to assess patient–ventilator asynchrony in three patients. The authors describe in this method three representative cases of asynchrony detection, demonstrating: (a) a patient with double triggering (the ventilator delivers two consecutive breaths for a single patient effort); (b) a patient with ineffective efforts (due to excessive ventilatory assistance and long insufflation times with shortening of the patient’s expiratory phase, which prevents the patient’s next inspiratory effort from exceeding intrinsic PEEP and activating the ventilator); (c) a reverse-triggered patient (when inspiratory efforts are triggered directly by mechanical breaths). The major limitation of this technique is the unavailability of continuous recordings.
Simultaneous observation of TF and Paw may indicate an auto-trigger PVA, when an assisted breathing cycle is observed without detection of inspiratory thickening [48,49].
Vivier et al. investigated the performance and accuracy of a new method based on the ultrasound analysis of diaphragm excursion (DE) or thickening combined with airway pressure to detect PVA. They found that this method (especially diaphragm thickening) was more accurate than flow and pressure waveform analysis alone, and had better feasibility than diaphragm EMG for detecting patient-ventilator asynchronies [101].
It should be noted that although DUS might be a reasonable alternative to detect most types of PVA [49], further studies are needed to determine its exact role [46,100].
6. Role of Ultrasound of the Diaphragm in the Assessment of Weaning
Weaning from MV is a process of gradual reduction of ventilatory support, configuring a challenge to the respiratory muscles, notably the diaphragm. Unsuccessful weaning from MV have worse outcomes increasing morbidity and mortality [102,103].
The main cause of weaning failure is an imbalance between the load and capacity of the respiratory system [104]. Identifying patients who are suitable or not for weaning avoids, on the one hand, the unnecessary use of MV with its inherent risks, and on the other hand, prevents premature weaning and its complications. For this characterization, clinical criteria (“readiness testing”) are employed in order to identify patients who are ready or not to wean from MV [103]. However, readiness testing can sometimes point to uncertainty regarding the patient’s ability to wean and, in these circumstances, the use of physiological tests and predictors of weaning can help identify patients who are ready or not to wean [104].
Diaphragm function assessed on ultrasound has been used as a predictor of weaning, primarily as a diagnostic test to predict extubation success [50,105].
Numerous studies have used the DUS to assess the prediction of weaning, and there are even meta-analyses and systematic reviews on the subject in the literature [50,105,106,107].
The earliest studies suggested that a successful extubation or weaning failure was likely with diaphragm excursion cut-off values of 11–14 mm [11] and when the diaphragm thickening fraction was lower than 30–36% [108].
However, recently Vivier et al. [80] assessed the accuracy of diaphragmatic excursion and thickening to predict extubation. DUS was performed before extubation, in a T-tube, in 191 patients who successfully underwent an SBT. Diaphragmatic dysfunction, defined as excursion < 10 mm or thickening < 30%, was not associated with an increased risk of extubation failure. Vetrugno et al. [109] also demonstrated recently that diaphragm thickening fraction (TF) was not predictive of weaning failure from MV, in 57 COVID-19 patients undergoing weaning from MV.
Regarding the value of DUS to predict weaning from MV, it must be assumed that the results are controversial, and general conclusions are not allowed at this moment.
This controversy seems to be mainly related to the heterogeneity regarding the population and study design, and on the characterization of the variables under test. There are marked variations in:
(1) the timing of the ultrasound assessment in relation to the spontaneous breathing test (SBT), patient position during the SBT,
(2) the standardization of the diaphragm evaluation technique with ultrasound in patients on ventilatory support (PEEP levels, pressure support),
(3) varying definitions of SBT failure, weaning failure, or extubation failure, which were not standardized across studies, making comparison between outcome measures difficult.
Furthermore, a substantial proportion of patients with diaphragmatic dysfunction seen on DUS could be successfully weaned from the ventilator [10] suggesting that in patients undergoing a successful SBT, extubation appears to be determined by factors other than diaphragm function [49].
Although diaphragmatic ultrasound is a promising diagnostic tool, to determine its role in predicting weaning, additional studies are needed to standardize [49] some relevant points in the technical aspect [48] and also regarded to the clinical question [110], suggesting that:
- -
- To identify patients at high risk of weaning failure, DUS is performed before SBT.
- -
- To predict the weaning outcome or to diagnose the cause of weaning failure, DUS is best performed after initiation and/or completion of an SBT.
7. Novel Techniques and Future Developments for Functional Imaging and Quantification of Tissue Properties
7.1. Tissue Doppler Imaging
Tissue Doppler Imaging (TDI) is an ultrasound technique that detects the change in the frequency of ultrasound signals reflected by moving structures, already widely used to assess cardiac function but only more recently applied to assess the diaphragm in adults [111] and neonates [112].
Although scarcely studied, recently Soilemezi et al. [113] presented interesting results, studying healthy volunteers (n = 20) with the aim of describing the pattern, reporting normal values, and assessing the reproducibility of diaphragmatic TDI waveform velocities during contraction (including peak contraction velocities (PCV) and relaxation (including maximal relaxation rates (TDI-MRR)). Also in this study, the authors recorded the pattern and values of diaphragmatic TDI in ICU intubated patients (n = 106) elected for a spontaneous breathing test, comparing cases of successful and unsuccessful weaning, and, in a subgroup of these patients (n = 24), they correlated TDI measurements with parameters derived from transdiaphragmatic pressure (Pdi). The results indicated the patterns of contraction and relaxation of the TDI diaphragm in normal subjects and in patients with successful and unsuccessful weaning. It was a notable finding that weaning failure patients exhibited significantly higher PCV and TDI-MRR velocities compared to healthy participants and weaning success patients, such that the higher the values of PCV and TDI-MRR during weaning, the greater the likelihood of weaning failure. In addition, in the subgroup of patients evaluated with Pdi, high correlation coefficients of TDI PCV with peak Pdi and PTPdi, and Pdi-MRR and TDI-MRR were demonstrated. These findings offer insights into the physiological behavior of patients with weaning failure using a non-invasive technique.
Cammarotta et al. [111] investigated whether the diaphragmatic function assessed by TDI (to measure the excursion velocity and acceleration) could help to discriminate the success of extubation (after 48 h) among 100 adult subjects who passed a 30-min spontaneous breathing trial (SBT). The TDI measurement was performed at the end of the SBT. They found that: (1) TDI parameters (collected at the end of an SBT) discriminated against individuals likely to exhibit extubation failure within 48 h after extubation (in these individuals the dTDI variables were significantly higher when compared to those who were successfully extubated). Inspiratory peak and mean velocity were good predictors of extubation failure after a successful SBT; TDI assessment was feasible and reproducible.
Although the preliminary results are very significant, it is important to point out that much progress is still needed in the standardization of the method that includes the determination of the diaphragmatic movement point of interest (ROI); influence of other factors, such as compliance of the rib cage and activation of accessory inspiratory and expiratory muscles [114].
7.2. Speckle Tracking Ultrasound (STUS)
Traditional methods to assess diaphragmatic function on ultrasound, such as measuring diaphragmatic excursion, diaphragm thickness and thickening fraction (TF), although consolidated, are limited to measuring the deformation of diaphragmatic muscle tissue in the transverse axis and therefore do not assess the ‘longitudinal’ muscle shortening, that is, the movement in the direction of the contracting muscle fibers.
Speckle tracking ultrasound (STUS) is a new method of analysis, already widely used in echocardiography [115], which allows observing the contraction of muscle fibers in the direction of movement (longitudinal).
A speckle represents a region of muscle tissue whose gray pattern on ultrasound remains relatively constant. The analysis of the STUS software is based on following (to track) a group of speckles during the contractile cycle, measuring their displacement and deformation (movement of the speckles in relation to each other). The degree of deformation is known as ‘strain’ while “strain rate” measures the deformation velocity. Because STUS tracks specific regions of interest it is considered relatively angle independent and tracking can help differentiate passive movement from active contraction.
The applicability of using STUS to investigate diaphragm movement was tested in different scenarios.
Hatam et al. [116] analyzed diaphragm deformation (transverse strain) in STUS as a parameter for respiratory load in healthy individuals (n = 13) submitted to NIV in CPAP (CPAP 5, PSV 5, 10 and 15) or unsupported (spontaneous breathing) and compared with inspiratory thickening fraction (TF). They found that both TF and transverse strain significantly increased under CPAP and PSV and that transverse strain correlated well with TF.
Oppersma et al. [86] evaluated the validity of speckle tracking ultrasound (strain and strain rate%) to quantify diaphragm contractility in healthy volunteers (n = 13) submitted to an inspiratory overload protocol (randomized from 0 to 50% of the maximum inspiratory pressure). Diaphragm electrical activity (EAdi), transdiaphragmatic pressures (Pdi) and thickening fraction were also recorded. They found that strain and strain rate, but not TF, increased with progressive loading of the diaphragm. Both strain and strain rate were highly correlated with Pdi and EAdi, but not TF. In this study, STUS was superior to conventional ultrasound techniques (TF) for estimating diaphragmatic contractility under inspiratory threshold loading.
Orde et al. [117] evaluated the applicability of STUS parameters (longitudinal strain) to analyze diaphragmatic contraction in healthy adults (n = 50) in comparison with the evaluation of diaphragm thickness, thickening fraction (TF) and excursion (diaphragm caudal displacement). They found a moderate correlation between right diaphragmatic longitudinal strain and TF, and a weak correlation between strain and excursion. Inter- and intra-rater variability was satisfactory for TF, excursion and strain.
Xu Q et al. [118] evaluated the feasibility and reproducibility of quantification of diaphragm longitudinal strain (DLS) by STUS (study A: in 25 healthy subjects and 20 mechanically ventilated patients), and aimed to determine whether the maximum DLS can be used to predict outcomes weaning (study B: multicenter retrospective, 96 patients elected for weaning, of which 56 were successfully weaned). Intra- and inter-operator reliability was good to excellent under conditions of eupnea, deep breathing and MV. DLS exhibited a fair linear relationship with diaphragmatic thickening fraction (TF) and diaphragmatic excursion (DE). For the prediction of successful weaning, the AUC of ROC curves of DLS was very similar to TF, but not superior to the rapid shallow breathing index.
Fritsch et al. [119] evaluated the feasibility of STUS for an evaluation of the diaphragm in a group of 20 patients after a coronary artery bypass graft procedure, in order to detect diaphragm dysfunction that would manifest as a decrease in the strain and strain rate parameters. Each patient received three ultrasonographic assessments: (1) preoperatively, (2) within 24 h, and (3) within 48 h after extubation. They found that the deformation of the diaphragm (strain) was reduced for about 24 h, but the contractile velocity (strain rate) remained stable or even increased. This increase in the strain rate was attributed to a change in the recruitment pattern of diaphragmatic fibers, which may reflect an increasing activation of type II fibers.
Although there are promising results, STUS lacks validation in a large study. In addition, the software for STUS analysis was designed to determine myocardial deformation, and they are “closed boxes” that need to be broken. Many studies performed offline analyses, demanding considerable time, and making applicability in a clinical situation difficult. Additional studies involving STUS in subjects with abnormal diaphragmatic function and/or critical illness, and comparison with electromyography or transdiaphragmatic pressure measurements may be needed.
7.3. Shear Wave Elastography
Shear wave elastography (SWE) is a new technique recently applied to assess the diaphragm, which consists of creating a source of vibration (focused acoustic impulse beam generated by the ultrasound probe), resulting in tissue deformation and generating a shear wave that can be quantified (converted into Shear Modulus, SM).
The SM expresses tissue biomechanical information and, therefore, is innovative for translating qualitative information about the properties of the diaphragm muscle. A higher SM indicates greater tissue stiffness.
In two previous studies of healthy subjects, SWE reproduced the diaphragmatic contractile activity.
Chino et al. [120] studied diaphragm function with SWE (shear modulus, SM) in 14 healthy male subjects at various levels of submaximal inspiratory tasks (at 15, 30, 45, 60, and 75% of the maximal inspiratory mouth pressure). They found that the diaphragm SM increased along with rising mouth pressure, but interestingly, the rate of SM increase decreases. Similar findings were observed by Bachasson et al. [121] who evaluated whether SWE (diaphragm shear modulus quantification, SMdi) could be used to assess diaphragm function compared to the measurement of transdiaphragmatic pressure (Pdi) in 15 healthy volunteers undergoing an inspiratory load protocol. They found that the mean Pdi was correlated with the mean SMdi and that changes in diaphragm stiffness assessed by SWE reflected changes in Pdi.
Aarab et al. [122] evaluated changes in the shear modulus (SM) and the relationship with changes in diaphragm thickness in patients during their ICU stay and also, in an experimental model, they characterized histological and force-producing changes in the diaphragm. As a translational study, it comprised a sample of critically ill patients (n = 102, of which 88 were mechanically ventilated) and mechanically ventilated piglets (in which transdiaphragmatic pressure and diaphragmatic biopsies were collected). The study observed a heterogeneous pattern of diaphragm configuration changes. A decrease or increase of more than 10% from the baseline was common in patients for thickness (86%) and SM (92%). Specifically, the SM remained unchanged in 8%, increased in 51%, and decreased in 41% of patients. Changes in the SM were inversely correlated with changes in diaphragm thickness in critically ill patients. A notable finding was that in the experimental model, the reduction in the SM was associated with diaphragm atrophy, lipid accumulation, and reduced strength.
Although Aarab’s [122] findings are notable and seem to corroborate the concepts of diaphragmatic myotrauma, it is still necessary to extend SWE studies by standardizing the technique (ideal probe location, influence of lung volume, moment of measurement of MS in relation to the respiratory cycle) and expanding studies in different models and scenarios for a pathophysiological understanding of the method [123].
8. Limitations
Although ultrasonography has advantages when compared to other methods of assessing diaphragm function, its limitations must be considered for proper interpretation. Patient positioning [56] and the operator’s expertise in performing the ultrasound are important in acquiring and interpreting the images [124]. However, studies that have tested the increase in the appropriate skills to perform ultrasound through training have described a learning curve considered fast, with satisfactory results [108,125], especially when they involve a theoretical-practical combination, as recently observed by Garofalo et al. [126] and including critical care patients [127]. Regarding the concerns about patient positioning, although in healthy patients varied postures can interfere with the thickness of the diaphragm [128], Baldwin et al. [79] observed good reproducibility (intraclass correlation coefficient (ICC) = 0.990, 95% confidence interval: 0.918–0.998) in measuring the end-expiratory diaphragm thickness in a semi-recumbent position, as usual in critically ill patients. Considering the concern about variations in diaphragm thickness along the surface of the muscle [129,130] in serial measurements, demarcating the placement of the ultrasound probe can improve measurement consistency (ensure repeatability) [23]. It is recognized that there is greater difficulty in visualizing the left diaphragm due to the smaller window of the spleen [23] and ICU patients [45]. However, it should be noted that many critical patients have pleural (effusions) and/or pulmonary (consolidations or atelectasis) alterations that, contrary to what one might imagine, facilitate the identification of hemidiaphragms [46]. In critically ill patients, a recent expert consensus indicates that unilateral assessment of the right hemidiaphragm is an acceptable substitute for the entire diaphragm, except in cases of suspected unilateral involvement, when then there is a need for bilateral assessment of the diaphragm [48]. Ultrasound can also be limited due to a poor acoustic window for the visualization of the diaphragm in obese patients [47,131,132]. Finally, although a correlation between the thickening fraction and inspiratory strength has been observed in healthy subjects [57], the DUS does not provide a direct measure of ventilatory force, probably because the other inspiratory muscles of the ribcage may partially contribute to ventilation, interfering with the contribution of the diaphragm [51]. Even so, the assessment of diaphragmatic function with ultrasound has demonstrated numerous important clinical implications related to the outcomes of critically ill patients. As the tool seems to be in constant evolution, a meeting of specialists recently registered the main observations about the ultrasound technique that must be appreciated for the correct interpretation, aiming to overcome the main limitations [48]. Not all the cited works are homogeneous in terms of their study design, standardization of the method, in the selection of patients, or compared with a reference gold standard method.
9. Future Directions
Although ultrasonography has evolved significantly in recent times, there is still a long way to go for its wide use in clinical practice. Regarding critical illness, it is expected that potential improvements in transducers and in machine presets can improve the visualization and measurement of variables. In addition, it is essential that we have more studies that contrast sonographic findings of the diaphragm with:
- -
- Histological findings of the muscle,
- -
- Interaction with other respiratory muscles,
- -
- Reference tools for PVA detection, and
- -
- Baseline measures of respiratory effort (such as work of breathing, PTP) and fatigue (such as TTI and relaxation rate).
Also, a technical improvement that allows automated image acquisition can make it a genuine monitoring tool.
10. Conclusions
Diaphragm dysfunction is frequent and is related to many adverse outcomes in critically ill patients on MV. Diaphragm protection is a recent concept based on strategies aimed at preventing myotrauma. Monitoring diaphragmatic function and identifying diaphragmatic dysfunction are fundamentals of this protection strategy. Diaphragm ultrasonography may represent a possible complementary, promising tool which could be useful for monitoring diaphragm function at the bedside, potentially allowing you to adapt ventilator settings to provide protective diaphragm ventilation. Homogeneous prospective studies are needed in terms of study design, standardization of the method, in the number and selection of patients, and which all are compared with a reference gold standard method.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics13061116/s1, Table S1: Reference values of DUS measurements in healthy subjects. [47,51,52,56,57,58,61,79,129,133,134,135,136,137,138].
Author Contributions
Conceptualization, P.V.S. and A.L.P.d.A.; methodology, P.V.S.; writing—original draft preparation, P.V.S., L.Z.C. and A.L.P.d.A.; writing—review and editing, P.V.S., L.Z.C. and A.L.P.d.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tremblay, L.N.; Slutsky, A.S. Ventilator-induced lung injury: From the bench to the bedside. Intensive Care Med. 2006, 32, 24–33. [Google Scholar] [CrossRef]
- Bates, J.H.; Smith, B.J. Ventilator-induced lung injury and lung mechanics. Ann. Transl. Med. 2018, 6, 378. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef]
- Goligher, E.C.; Brochard, L.J.; Reid, W.D.; Fan, E.; Saarela, O.; Slutsky, A.S.; Kavanagh, B.P.; Rubenfeld, G.D.; Ferguson, N.D. Diaphragmatic myotrauma: A mediator of prolonged ventilation and poor patient outcomes in acute respiratory failure. Lancet Respir. Med. 2019, 7, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Vassilakopoulos, T.; Petrof, B.J. Ventilator-induced diaphragmatic dysfunction. Am. J. Respir. Crit. Care Med. 2004, 169, 336–341. [Google Scholar] [CrossRef]
- Petrof, B.J.; Jaber, S.; Matecki, S. Ventilator-induced diaphragmatic dysfunction. Curr. Opin. Crit. Care 2010, 16, 19–25. [Google Scholar] [CrossRef]
- Jaber, S.; Petrof, B.J.; Jung, B.; Chanques, G.; Berthet, J.P.; Rabuel, C.; Bouyabrine, H.; Courouble, P.; Koechlin-Ramonatxo, C.; Sebbane, M.; et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am. J. Respir. Crit. Care Med. 2011, 183, 364–371. [Google Scholar] [CrossRef]
- Demoule, A.; Jung, B.; Prodanovic, H.; Molinari, N.; Chanques, G.; Coirault, C.; Matecki, S.; Duguet, A.; Similowski, T.; Jaber, S. Diaphragm dysfunction on admission to the intensive care unit. Prevalence, risk factors, and prognostic impact—A prospective study. Am. J. Respir. Crit. Care Med. 2013, 188, 213–219. [Google Scholar] [CrossRef]
- Jung, B.; Moury, P.H.; Mahul, M.; de Jong, A.; Galia, F.; Prades, A.; Albaladejo, P.; Chanques, G.; Molinari, N.; Jaber, S. Diaphragmatic dysfunction in patients with ICU-acquired weakness and its impact on extubation failure. Intensive Care Med. 2016, 42, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Dres, M.; Dubé, B.P.; Mayaux, J.; Delemazure, J.; Reuter, D.; Brochard, L.; Similowski, T.; Demoule, A. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am. J. Respir. Crit. Care Med. 2017, 195, 57–66. [Google Scholar] [CrossRef]
- Kim, W.Y.; Suh, H.J.; Hong, S.-B.; Koh, Y.; Lim, C.-M. Diaphragm dysfunction assessed by ultrasonography: Influence on weaning from mechanical ventilation. Crit. Care Med. 2011, 39, 2627–2630. [Google Scholar] [CrossRef]
- Demoule, A.; Molinari, N.; Jung, B.; Prodanovic, H.; Chanques, G.; Matecki, S.; Mayaux, J.; Similowski, T.; Jaber, S. Patterns of diaphragm function in critically ill patients receiving prolonged mechanical ventilation: A prospective longitudinal study. Ann. Intensive Care 2016, 6, 75. [Google Scholar] [CrossRef]
- Jung, B.; Nougaret, S.; Conseil, M.; Coisel, Y.; Futier, E.; Chanques, G.; Molinari, N.; Lacampagne, A.; Matecki, S.; Jaber, S. Sepsis is associated with a preferential diaphragmatic atrophy: A critically ill patient study using tridimensional computed tomography. Anesthesiology 2014, 120, 1182–1191. [Google Scholar] [CrossRef] [PubMed]
- Sassoon, C.S.; Zhu, E.; Fang, L.; Ramar, K.; Jiao, G.Y.; Caiozzo, V.J. Interactive effects of corticosteroid and mechanical ventilation on diaphragm muscle function. Muscle Nerve 2011, 43, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Supinski, G.S.; Ann Callahan, L. Diaphragm weakness in mechanically ventilated critically ill patients. Crit. Care 2013, 17, R120. [Google Scholar] [CrossRef]
- Adler, D.; Dupuis-Lozeron, E.; Richard, J.-C.; Janssens, J.-P.; Brochard, L. Does inspiratory muscle dysfunction predict readmission after intensive care unit discharge? Am. J. Respir. Crit. Care Med. 2014, 190, 347–350. [Google Scholar] [CrossRef]
- Medrinal, C.; Prieur, G.; Frenoy, É.; Robledo Quesada, A.; Poncet, A.; Bonnevie, T.; Gravier, F.E.; Lamia, B.; Contal, O. Respiratory weakness after mechanical ventilation is associated with one-year mortality—A prospective study. Crit. Care 2016, 20, 231. [Google Scholar] [CrossRef]
- Heunks, L.; Ottenheijm, C. Diaphragm-protective mechanical ventilation to improve outcomes in ICU patients? Am. J. Respir. Crit. Care Med. 2018, 197, 150–152. [Google Scholar] [CrossRef]
- Schepens, T.; Dianti, J. Diaphragm protection: What should we target? Curr. Opin. Crit. Care 2020, 26, 35–40. [Google Scholar] [CrossRef]
- Schepens, T.; Dres, M.; Heunks, L.; Goligher, E.C. Diaphragm-protective mechanical ventilation. Curr. Opin. Crit. Care 2019, 25, 77–85. [Google Scholar] [CrossRef]
- Jaber, S.; Jung, B.; Matecki, S.; Petrof, B.J. Clinical review: Ventilator-induced diaphragmatic dysfunction-human studies confirm animal model findings! Crit. Care 2011, 15, 206. [Google Scholar] [CrossRef]
- Goligher, E.C.; Dres, M.; Fan, E.; Rubenfeld, G.D.; Scales, D.C.; Herridge, M.S.; Vorona, S.; Sklar, M.C.; Rittayamai, N.; Lanys, A.; et al. Mechanical ventilation–induced diaphragm atrophy strongly impacts clinical outcomes. Am. J. Respir. Crit. Care Med. 2018, 197, 204–213. [Google Scholar] [CrossRef]
- Goligher, E.C.; Fan, E.; Herridge, M.S.; Murray, A.; Vorona, S.; Brace, D.; Rittayamai, N.; Lanys, A.; Tomlinson, G.; Singh, J.M.; et al. Evolution of diaphragm thickness during mechanical ventilation. Impact of inspiratory effort. Am. J. Respir. Crit. Care Med. 2015, 192, 1080–1088. [Google Scholar] [CrossRef]
- Levine, S.; Nguyen, T.; Taylor, N.; Friscia, M.E.; Budak, M.T.; Rothenberg, P.; Zhu, J.; Sachdeva, R.; Sonnad, S.; Kaiser, L.R.; et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N. Engl. J. Med. 2008, 358, 1327–1335. [Google Scholar] [CrossRef]
- Jiang, T.-X.; Reid, W.D.; Belcastro, A.; Road, J.D. Load dependence of secondary diaphragm inflammation and injury after acute inspiratory loading. Am. J. Respir. Crit. Care Med. 1998, 157, 230–236. [Google Scholar] [CrossRef]
- Liang, F.; Emeriaud, G.; Rassier, D.E.; Shang, D.; Gusev, E.; Hussain, S.N.A.; Sage, M.; Crulli, B.; Fortin-Pellerin, E.; Praud, J.P.; et al. Mechanical ventilation causes diaphragm dysfunction in newborn lambs. Crit. Care 2019, 23, 123. [Google Scholar] [CrossRef]
- Radell, P.J.; Remahl, S.; Nichols, D.G.; Eriksson, L.I. Effects of prolonged mechanical ventilation and inactivity on piglet diaphragm function. Intensive Care Med. 2002, 28, 358–364. [Google Scholar] [CrossRef]
- Anzueto, A.; Peters, J.I.; Tobin, M.J.; de los Santos, R.; Seidenfeld, J.J.; Moore, G.; Cox, W.J.; Coalson, J.J. Effects of prolonged controlled mechanical ventilation on diaphragmatic function in healthy adult baboons. Crit. Care Med. 1997, 25, 1187–1190. [Google Scholar] [CrossRef]
- Futier, E.; Constantin, J.M.; Combaret, L.; Mosoni, L.; Roszyk, L.; Sapin, V.; Attaix, D.; Jung, B.; Jaber, S.; Bazin, J.E. Pressure support ventilation attenuates ventilator-induced protein modifications in the diaphragm. Crit. Care 2008, 12, R116. [Google Scholar] [CrossRef]
- Sassoon, C.S.; Caiozzo, V.J.; Manka, A.; Sieck, G.C. Altered diaphragm contractile properties with controlled mechanical ventilation. J. Appl. Physiol. 2002, 92, 2585–2595. [Google Scholar] [CrossRef]
- Shanely, R.A.; Zergeroglu, M.A.; Lennon, S.L.; Sugiura, T.; Yimlamai, T.; Enns, D.; Belcastro, A.; Powers, S.K. Mechanical ventilation–induced diaphragmatic atrophy is associated with oxidative injury and increased proteolytic activity. Am. J. Respir. Crit. Care Med. 2002, 166, 1369–1374. [Google Scholar] [CrossRef]
- Hooijman, P.E.; Beishuizen, A.; Witt, C.C.; de Waard, M.C.; Girbes, A.R.; Spoelstra-de Man, A.M.; Niessen, H.W.; Manders, E.; van Hees, H.W.; van den Brom, C.E.; et al. Diaphragm muscle fiber weakness and ubiquitin-proteasome activation in critically ill patients. Am. J. Respir. Crit. Care Med. 2015, 191, 1126–1138. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.; Hooijman, P.E.; Beishuizen, A.; de Waard, M.C.; Paul, M.A.; Hartemink, K.J.; van Hees, H.W.H.; Lawlor, M.W.; Brocca, L.; Bottinelli, R.; et al. Diaphragm atrophy and weakness in the absence of mitochondrial dysfunction in the critically ill. Am. J. Respir. Crit. Care Med. 2017, 196, 1544–1558. [Google Scholar] [CrossRef]
- Grosu, H.B.; Im Lee, Y.; Lee, J.; Eden, E.; Eikermann, M.; Rose, K.M. Diaphragm muscle thinning in patients who are mechanically ventilated. Chest 2012, 142, 1455–1460. [Google Scholar] [CrossRef]
- Schepens, T.; Verbrugghe, W.; Dams, K.; Corthouts, B.; Parizel, P.M.; Jorens, P.G. The course of diaphragm atrophy in ventilated patients assessed with ultrasound: A longitudinal cohort study. Crit. Care 2015, 19, 422. [Google Scholar] [CrossRef]
- Zambon, M.; Beccaria, P.; Matsuno, J.; Gemma, M.; Frati, E.; Colombo, S.; Cabrini, L.; Landoni, G.; Zangrillo, A. Mechanical ventilation and diaphragmatic atrophy in critically ill patients: An ultrasound study. Crit. Care Med. 2016, 44, 1347–1352. [Google Scholar] [CrossRef]
- Marin-Corral, J.; Dot, I.; Boguña, M.; Cecchini, L.; Zapatero, A.; Gracia, M.P.; Pascual-Guardia, S.; Vilà, C.; Castellví, A.; Pérez-Terán, P.; et al. Structural differences in the diaphragm of patients following controlled vs assisted and spontaneous mechanical ventilation. Intensive Care Med. 2019, 45, 488–500. [Google Scholar] [CrossRef] [PubMed]
- Reid, W.; Huang, J.; Bryson, S.; Walker, D.; Belcastro, A. Diaphragm injury and myofibrillar structure induced by resistive loading. J. Appl. Physiol. 1994, 76, 176–184. [Google Scholar] [CrossRef]
- Pellegrini, M.; Hedenstierna, G.; Roneus, A.; Segelsjö, M.; Larsson, A.; Perchiazzi, G. The diaphragm acts as a brake during expiration to prevent lung collapse. Am. J. Respir. Crit. Care Med. 2017, 195, 1608–1616. [Google Scholar] [CrossRef]
- Akoumianaki, E.; Lyazidi, A.; Rey, N.; Matamis, D.; Perez-Martinez, N.; Giraud, R.; Mancebo, J.; Brochard, L.; Richard, J.M. Mechanical ventilation-induced reverse-triggered breaths: A frequently unrecognized form of neuromechanical coupling. Chest 2013, 143, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Dres, M.; Patel, B.K.; Sahetya, S.K.; Beitler, J.R.; Telias, I.; Yoshida, T.; Vaporidi, K.; Grieco, D.L.; Schepens, T.; et al. Lung-and diaphragm-protective ventilation. Am. J. Respir. Crit. Care Med. 2020, 202, 950–961. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Jonkman, A.H.; Dianti, J.; Vaporidi, K.; Beitler, J.R.; Patel, B.K.; Yoshida, T.; Jaber, S.; Dres, M.; Mauri, T.; et al. Clinical strategies for implementing lung and diaphragm-protective ventilation: Avoiding insufficient and excessive effort. Intensive Care Med. 2020, 46, 2314–2326. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, J.; van den Berg, M.; van der Pijl, R.; Hooijman, P.E.; Beishuizen, A.; Elshof, J.; de Waard, M.; Girbes, A.; Spoelstra-de Man, A.; Shi, Z.H.; et al. Positive end-expiratory pressure ventilation induces longitudinal atrophy in diaphragm fibers. Am. J. Respir. Crit. Care Med. 2018, 198, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Telias, I.; Spadaro, S. Techniques to monitor respiratory drive and inspiratory effort. Curr. Opin. Crit. Care 2020, 26, 3–10. [Google Scholar] [CrossRef]
- Goligher, E.C.; Laghi, F.; Detsky, M.E.; Farias, P.; Murray, A.; Brace, D.; Brochard, L.J.; Bolz, S.S.; Rubenfeld, G.D.; Kavanagh, B.P.; et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: Feasibility, reproducibility and validity. Intensive Care Med. 2015, 41, 642–649. [Google Scholar] [CrossRef]
- Matamis, D.; Soilemezi, E.; Tsagourias, M.; Akoumianaki, E.; Dimassi, S.; Boroli, F.; Richard, J.C.; Brochard, L. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013, 39, 801–810. [Google Scholar] [CrossRef]
- Santana, P.V.; Cardenas, L.Z.; de Albuquerque, A.L.P.; de Carvalho, C.R.R.; Caruso, P. Diaphragmatic ultrasound: A review of its methodological aspects and clinical uses. J. Bras. Pneumol. 2020, 46. [Google Scholar] [CrossRef]
- Haaksma, M.E.; Smit, J.M.; Boussuges, A.; Demoule, A.; Dres, M.; Ferrari, G.; Formenti, P.; Goligher, E.C.; Heunks, L.; Lim, E.H.T.; et al. EXpert consensus On Diaphragm UltraSonography in the critically ill (EXODUS): A Delphi consensus statement on the measurement of diaphragm ultrasound-derived parameters in a critical care setting. Crit. Care 2022, 26, 99. [Google Scholar] [CrossRef]
- Tuinman, P.R.; Jonkman, A.H.; Dres, M.; Shi, Z.H.; Goligher, E.C.; Goffi, A.; de Korte, C.; Demoule, A.; Heunks, L. Respiratory muscle ultrasonography: Methodology, basic and advanced principles and clinical applications in ICU and ED patients—A narrative review. Intensive Care Med. 2020, 46, 594–605. [Google Scholar] [CrossRef]
- Zambon, M.; Greco, M.; Bocchino, S.; Cabrini, L.; Beccaria, P.F.; Zangrillo, A. Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: A systematic review. Intensive Care Med. 2017, 43, 29–38. [Google Scholar] [CrossRef]
- Boussuges, A.; Gole, Y.; Blanc, P. Diaphragmatic motion studied by m-mode ultrasonography: Methods, reproducibility, and normal values. Chest 2009, 135, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Testa, A.; Soldati, G.; Giannuzzi, R.; Berardi, S.; Portale, G.; Silveri, N.G. Ultrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scanning in healthy subjects. Ultrasound Med. Biol. 2011, 37, 44–52. [Google Scholar] [CrossRef]
- Schepens, T.; Fard, S.; Goligher, E.C. Assessing diaphragmatic function. Respir. Care 2020, 65, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Umbrello, M.; Formenti, P.; Longhi, D.; Galimberti, A.; Piva, I.; Pezzi, A.; Mistraletti, G.; Marini, J.J.; Iapichino, G. Diaphragm ultrasound as indicator of respiratory effort in critically ill patients undergoing assisted mechanical ventilation: A pilot clinical study. Crit. Care 2015, 19, 161. [Google Scholar] [CrossRef]
- Lerolle, N.; Guérot, E.; Dimassi, S.; Zegdi, R.; Faisy, C.; Fagon, J.Y.; Diehl, J.L. Ultrasonographic diagnostic criterion for severe diaphragmatic dysfunction after cardiac surgery. Chest 2009, 135, 401–407. [Google Scholar] [CrossRef]
- Boon, A.J.; Harper, C.J.; Ghahfarokhi, L.S.; Strommen, J.A.; Watson, J.C.; Sorenson, E.J. Two-dimensional ultrasound imaging of the diaphragm: Quantitative values in normal subjects. Muscle Nerve 2013, 47, 884–889. [Google Scholar] [CrossRef]
- Cardenas, L.Z.; Santana, P.V.; Caruso, P.; de Carvalho, C.R.R.; de Albuquerque, A.L.P. Diaphragmatic ultrasound correlates with inspiratory muscle strength and pulmonary function in healthy subjects. Ultrasound Med. Biol. 2018, 44, 786–793. [Google Scholar] [CrossRef]
- Carrillo-Esper, R.; Pérez-Calatayud, Á.A.; Arch-Tirado, E.; Díaz-Carrillo, M.A.; Garrido-Aguirre, E.; Tapia-Velazco, R.; Peña-Pérez, C.A.; Espinoza-de Los Monteros, I.; Meza-Márquez, J.M.; Flores-Rivera, O.I.; et al. Standardization of sonographic diaphragm thickness evaluations in healthy volunteers. Respir. Care 2016, 61, 920–924. [Google Scholar] [CrossRef]
- Cohn, D.; Benditt, J.O.; Eveloff, S.; McCool, F.D. Diaphragm thickening during inspiration. J. Appl. Physiol. 1997, 83, 291–296. [Google Scholar] [CrossRef]
- Gottesman, E.; McCool, F.D. Ultrasound evaluation of the paralyzed diaphragm. Am. J. Respir. Crit. Care Med. 1997, 155, 1570–1574. [Google Scholar] [CrossRef]
- Ueki, J.; De Bruin, P.; Pride, N. In vivo assessment of diaphragm contraction by ultrasound in normal subjects. Thorax 1995, 50, 1157–1161. [Google Scholar] [CrossRef]
- Valette, X.; Seguin, A.; Daubin, C.; Brunet, J.; Sauneuf, B.; Terzi, N.; du Cheyron, D. Diaphragmatic dysfunction at admission in intensive care unit: The value of diaphragmatic ultrasonography. Intensive Care Med. 2015, 41, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Mariani, L.F.; Bedel, J.; Gros, A.; Lerolle, N.; Milojevic, K.; Laurent, V.; Hilly, J.; Troché, G.; Bedos, J.P.; Planquette, B. Ultrasonography for screening and follow-up of diaphragmatic dysfunction in the ICU: A pilot study. J. Intensive Care Med. 2016, 31, 338–343. [Google Scholar] [CrossRef]
- Lu, Z.; Xu, Q.; Yuan, Y.; Zhang, G.; Guo, F.; Ge, H. Diaphragmatic dysfunction is characterized by increased duration of mechanical ventilation in subjects with prolonged weaning. Respir. Care 2016, 61, 1316–1322. [Google Scholar] [CrossRef]
- Dubé, B.-P.; Dres, M.; Mayaux, J.; Demiri, S.; Similowski, T.; Demoule, A. Ultrasound evaluation of diaphragm function in mechanically ventilated patients: Comparison to phrenic stimulation and prognostic implications. Thorax 2017, 72, 811–818. [Google Scholar] [CrossRef]
- Dot, I.; Pérez-Terán, P.; Francés, A.; Díaz, Y.; Vilà-Vilardell, C.; Salazar-Degracia, A.; Chalela, R.; Barreiro, E.; Rodriguez-Fuster, A.; Masclans, J.R.; et al. Association between histological diaphragm atrophy and ultrasound diaphragm expiratory thickness in ventilated patients. J. Intensive Care 2022, 10, 40. [Google Scholar] [CrossRef] [PubMed]
- Urner, M.; Mitsakakis, N.; Vorona, S.; Chen, L.; Sklar, M.C.; Dres, M.; Rubenfeld, G.D.; Brochard, L.J.; Ferguson, N.D.; Fan, E.; et al. Identifying subjects at risk for diaphragm atrophy during mechanical ventilation using routinely available clinical data. Respir. Care 2021, 66, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Vivier, E.; Mekontso Dessap, A.; Dimassi, S.; Vargas, F.; Lyazidi, A.; Thille, A.W.; Brochard, L. Diaphragm ultrasonography to estimate the work of breathing during non-invasive ventilation. Intensive Care Med. 2012, 38, 796–803. [Google Scholar] [CrossRef]
- Cala, S.J.; Kenyon, C.M.; Lee, A.; Watkin, K.; Macklem, P.T.; Rochester, D.F. Respiratory ultrasonography of human parasternal intercostal muscle in vivo. Ultrasound Med. Biol. 1998, 24, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Wallbridge, P.; Parry, S.M.; Das, S.; Law, C.; Hammerschlag, G.; Irving, L.; Hew, M.; Steinfort, D. Parasternal intercostal muscle ultrasound in chronic obstructive pulmonary disease correlates with spirometric severity. Sci. Rep. 2018, 8, 15274. [Google Scholar] [CrossRef]
- Nakanishi, N.; Oto, J.; Ueno, Y.; Nakataki, E.; Itagaki, T.; Nishimura, M. Change in diaphragm and intercostal muscle thickness in mechanically ventilated patients: A prospective observational ultrasonography study. J. Intensive Care 2019, 7, 56. [Google Scholar] [CrossRef]
- Yoshida, R.; Tomita, K.; Kawamura, K.; Nozaki, T.; Setaka, Y.; Monma, M.; Ohse, H. Measurement of intercostal muscle thickness with ultrasound imaging during maximal breathing. J. Phys. Ther. Sci. 2019, 31, 340–343. [Google Scholar] [CrossRef]
- Umbrello, M.; Formenti, P.; Lusardi, A.C.; Guanziroli, M.; Caccioppola, A.; Coppola, S.; Chiumello, D. Oesophageal pressure and respiratory muscle ultrasonographic measurements indicate inspiratory effort during pressure support ventilation. Br. J. Anaesth. 2020, 125, e148–e157. [Google Scholar] [CrossRef] [PubMed]
- Dres, M.; Dubé, B.P.; Goligher, E.; Vorona, S.; Demiri, S.; Morawiec, E.; Mayaux, J.; Brochard, L.; Similowski, T.; Demoule, A. Usefulness of parasternal intercostal muscle ultrasound during weaning from mechanical ventilation. Anesthesiology 2020, 132, 1114–1125. [Google Scholar] [CrossRef] [PubMed]
- Dres, M.; Similowski, T.; Goligher, E.C.; Pham, T.; Sergenyuk, L.; Telias, I.; Grieco, D.L.; Ouechani, W.; Junhasavasdikul, D.; Sklar, M.C.; et al. Dyspnoea and respiratory muscle ultrasound to predict extubation failure. Eur. Respir. J. 2021, 58, 2100002. [Google Scholar] [CrossRef]
- Powers, S.K.; Shanely, R.A.; Coombes, J.S.; Koesterer, T.J.; McKenzie, M.; Van Gammeren, D.; Cicale, M.; Dodd, S.L. Mechanical ventilation results in progressive contractile dysfunction in the diaphragm. J. Appl. Physiol. 2002, 92, 1851–1858. [Google Scholar] [CrossRef]
- Hudson, M.B.; Smuder, A.J.; Nelson, W.B.; Bruells, C.S.; Levine, S.; Powers, S.K. Both high level pressure support ventilation and controlled mechanical ventilation induce diaphragm dysfunction and atrophy. Crit. Care Med. 2012, 40, 1254. [Google Scholar] [CrossRef]
- Sklar, M.C.; Dres, M.; Fan, E.; Rubenfeld, G.D.; Scales, D.C.; Herridge, M.S.; Rittayamai, N.; Harhay, M.O.; Reid, W.D.; Tomlinson, G.; et al. Association of low baseline diaphragm muscle mass with prolonged mechanical ventilation and mortality among critically ill adults. JAMA Netw. Open 2020, 3, e1921520. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, C.E.; Paratz, J.D.; Bersten, A.D. Diaphragm and peripheral muscle thickness on ultrasound: Intra-rater reliability and variability of a methodology using non-standard recumbent positions. Respirology 2011, 16, 1136–1143. [Google Scholar] [CrossRef]
- Vivier, E.; Muller, M.; Putegnat, J.B.; Steyer, J.; Barrau, S.; Boissier, F.; Bourdin, G.; Mekontso-Dessap, A.; Levrat, A.; Pommier, C.; et al. Inability of diaphragm ultrasound to predict extubation failure: A multicenter study. Chest 2019, 155, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Dianti, J.; Fard, S.; Wong, J.; Chan, T.C.Y.; Del Sorbo, L.; Fan, E.; Amato, M.B.P.; Granton, J.; Burry, L.; Reid, W.D.; et al. Strategies for lung-and diaphragm-protective ventilation in acute hypoxemic respiratory failure: A physiological trial. Crit. Care 2022, 26, 259. [Google Scholar] [CrossRef] [PubMed]
- de Vries, H.J.; Jonkman, A.H.; de Grooth, H.J.; Duitman, J.W.; Girbes, A.R.J.; Ottenheijm, C.A.C.; Schultz, M.J.; van de Ven, P.M.; Zhang, Y.; de Man, A.M.E.; et al. Lung-and diaphragm-protective ventilation by titrating inspiratory support to diaphragm effort: A randomized clinical trial. Crit. Care Med. 2022, 50, 192. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Sigala, I.; Vassilakopoulos, T. Diaphragmatic ultrasound as a monitoring tool in the intensive care unit. Ann. Transl. Med. 2017, 5, 79. [Google Scholar] [CrossRef]
- Summerhill, E.M.; El-Sameed, Y.A.; Glidden, T.J.; McCool, F.D. Monitoring recovery from diaphragm paralysis with ultrasound. Chest 2008, 133, 737–743. [Google Scholar] [CrossRef]
- Oppersma, E.; Hatam, N.; Doorduin, J.; van der Hoeven, J.G.; Marx, G.; Goetzenich, A.; Fritsch, S.; Heunks, L.M.A.; Bruells, C.S. Functional assessment of the diaphragm by speckle tracking ultrasound during inspiratory loading. J. Appl. Physiol. 2017, 123, 1063–1070. [Google Scholar] [CrossRef]
- Poulard, T.; Bachasson, D.; Fossé, Q.; Niérat, M.C.; Hogrel, J.Y.; Demoule, A.; Gennisson, J.L.; Dres, M. Poor correlation between diaphragm thickening fraction and transdiaphragmatic pressure in mechanically ventilated patients and healthy subjects. Anesthesiology 2022, 136, 162–175. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, I.; Chiodaroli, E.; Gattarello, S.; Cappio Borlino, S.; Chiumello, D. Diaphragmatic ultrasound and esophageal pressure in COVID-19 pneumonia during helmet CPAP. Intensive Care Med. 2022, 48, 1095–1096. [Google Scholar] [CrossRef] [PubMed]
- Holanda, M.A.; Vasconcelos, R.d.S.; Ferreira, J.C.; Pinheiro, B.V. Patient-ventilator asynchrony. J. Bras. Pneumol. 2018, 44, 321–333. [Google Scholar] [CrossRef] [PubMed]
- De Wit, M.; Miller, K.B.; Green, D.A.; Ostman, H.E.; Gennings, C.; Epstein, S.K. Ineffective triggering predicts increased duration of mechanical ventilation. Crit. Care Med. 2009, 37, 2740–2745. [Google Scholar]
- Tobin, M.J.; Jubran, A.; Laghi, F. Patient–ventilator interaction. Am. J. Respir. Crit. Care Med. 2001, 163, 1059–1063. [Google Scholar] [CrossRef] [PubMed]
- Beitler, J.R.; Sands, S.A.; Loring, S.H.; Owens, R.L.; Malhotra, A.; Spragg, R.G.; Matthay, M.A.; Thompson, B.T.; Talmor, D. Quantifying unintended exposure to high tidal volumes from breath stacking dyssynchrony in ARDS: The BREATHE criteria. Intensive Care Med. 2016, 42, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Yonis, H.; Gobert, F.; Tapponnier, R.; Guérin, C. Reverse triggering in a patient with ARDS. Intensive Care Med. 2015, 41, 1711–1712. [Google Scholar] [CrossRef] [PubMed]
- Blanch, L.; Villagra, A.; Sales, B.; Montanya, J.; Lucangelo, U.; Luján, M.; García-Esquirol, O.; Chacón, E.; Estruga, A.; Oliva, J.C.; et al. Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med. 2015, 41, 633–641. [Google Scholar] [CrossRef]
- Gilstrap, D.; MacIntyre, N. Patient–ventilator interactions. Implications for clinical management. Am. J. Respir. Crit. Care Med. 2013, 188, 1058–1068. [Google Scholar] [CrossRef] [PubMed]
- Branson, R.D.; Blakeman, T.C.; Robinson, B.R. Asynchrony and dyspnea discussion. Respir. Care 2013, 58, 973–989. [Google Scholar] [CrossRef]
- Sieck, G.C.; Ferreira, L.F.; Reid, M.B.; Mantilla, C.B. Mechanical properties of respiratory muscles. Compr. Physiol. 2013, 3, 1553. [Google Scholar]
- Thille, A.W.; Rodriguez, P.; Cabello, B.; Lellouche, F.; Brochard, L. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006, 32, 1515–1522. [Google Scholar] [CrossRef]
- Doorduin, J.; Van Hees, H.W.; Van Der Hoeven, J.G.; Heunks, L.M. Monitoring of the respiratory muscles in the critically ill. Am. J. Respir. Crit. Care Med. 2013, 187, 20–27. [Google Scholar] [CrossRef]
- Soilemezi, E.; Vasileiou, M.; Spyridonidou, C.; Tsagourias, M.; Matamis, D. Understanding patient–ventilator asynchrony using diaphragmatic ultrasonography. Am. J. Respir. Crit. Care Med. 2019, 200, e27–e28. [Google Scholar] [CrossRef]
- Vivier, E.; Haudebourg, A.F.; Le Corvoisier, P.; Mekontso Dessap, A.; Carteaux, G. Diagnostic accuracy of diaphragm ultrasound in detecting and characterizing patient–ventilator asynchronies during noninvasive ventilation. Anesthesiology 2020, 132, 1494–1502. [Google Scholar] [CrossRef]
- Epstein, S.K.; Ciubotaru, R.L.; Wong, J.B. Effect of failed extubation on the outcome of mechanical ventilation. Chest 1997, 112, 186–192. [Google Scholar] [CrossRef]
- Esteban, A.; Anzueto, A.; Frutos, F.; Alía, I.; Brochard, L.; Stewart, T.E.; Benito, S.; Epstein, S.K.; Apezteguía, C.; Nightingale, P.; et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: A 28-day international study. JAMA 2002, 287, 345–355. [Google Scholar] [CrossRef]
- Schmidt, G.A.; Girard, T.D.; Kress, J.P.; Morris, P.E.; Ouellette, D.R.; Alhazzani, W.; Burns, S.M.; Epstein, S.K.; Esteban, A.; Fan, E.; et al. Official executive summary of an American Thoracic Society/American College of Chest Physicians clinical practice guideline: Liberation from mechanical ventilation in critically ill adults. Am. J. Respir. Crit. Care Med. 2017, 195, 115–119. [Google Scholar] [CrossRef]
- Llamas-Alvarez, A.M.; Tenza-Lozano, E.M.; Latour-Perez, J. Diaphragm and lung ultrasound to predict weaning outcome: Systematic review and meta-analysis. Chest 2017, 152, 1140–1150. [Google Scholar] [CrossRef]
- Li, C.; Li, X.; Han, H.; Cui, H.; Wang, G.; Wang, Z. Diaphragmatic ultrasonography for predicting ventilator weaning: A meta-analysis. Medicine 2018, 97, e10968. [Google Scholar] [CrossRef]
- Qian, Z.; Yang, M.; Li, L.; Chen, Y. Ultrasound assessment of diaphragmatic dysfunction as a predictor of weaning outcome from mechanical ventilation: A systematic review and meta-analysis. BMJ Open 2018, 8, e021189. [Google Scholar] [CrossRef]
- DiNino, E.; Gartman, E.J.; Sethi, J.M.; McCool, F.D. Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax 2014, 69, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Vetrugno, L.; Orso, D.; Corradi, F.; Zani, G.; Spadaro, S.; Meroi, F.; D’Andrea, N.; Bove, T.; Cammarota, G.; De Robertis, E.; et al. Diaphragm ultrasound evaluation during weaning from mechanical ventilation in COVID-19 patients: A pragmatic, cross-section, multicenter study. Respir. Res. 2022, 23, 210. [Google Scholar] [CrossRef] [PubMed]
- Mayo, P.; Volpicelli, G.; Lerolle, N.; Schreiber, A.; Doelken, P.; Vieillard-Baron, A. Ultrasonography evaluation during the weaning process: The heart, the diaphragm, the pleura and the lung. Intensive Care Med. 2016, 42, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Cammarota, G.; Boniolo, E.; Tarquini, R.; Vaschetto, R. Diaphragmatic excursion tissue Doppler sonographic assessment. Intensive Care Med. 2020, 46, 1759–1760. [Google Scholar] [CrossRef]
- Maurizio, R.; Rinaldi, V.E.; Camerini, P.G.; Salvatori, C.; Leonardi, A.; Bini, V. Right diaphragmatic peak motion velocities on pulsed wave tissue Doppler imaging in neonates: Method, reproducibility, and reference values. J. Ultrasound Med. 2019, 38, 2695–2701. [Google Scholar] [CrossRef]
- Soilemezi, E.; Savvidou, S.; Sotiriou, P.; Smyrniotis, D.; Tsagourias, M.; Matamis, D. Tissue Doppler imaging of the diaphragm in healthy subjects and critically ill patients. Am. J. Respir. Crit. Care Med. 2020, 202, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- McCool, F.D.; Tzelepis, G.E. Tissue Doppler imaging of the diaphragm: A new kid on the block? Am. J. Respir. Crit. Care Med. 2020, 202, 921–922. [Google Scholar] [CrossRef]
- Blessberger, H.; Binder, T. Two dimensional speckle tracking echocardiography: Basic principles. Heart 2010, 96, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Hatam, N.; Goetzenich, A.; Rossaint, R.; Karfis, I.; Bickenbach, J.; Autschbach, R.; Marx, G.; Bruells, C.S. A novel application for assessing diaphragmatic function by ultrasonic deformation analysis in noninvasively ventilated healthy young adults. Ultraschall Med.—Eur. J. Ultrasound 2014, 35, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Orde, S.R.; Boon, A.J.; Firth, D.G.; Villarraga, H.R.; Sekiguchi, H. Diaphragm assessment by two dimensional speckle tracking imaging in normal subjects. BMC Anesthesiol. 2015, 16, 43. [Google Scholar] [CrossRef]
- Xu, Q.; Yang, X.; Qian, Y.; Hu, C.; Lu, W.; Cai, S.; Hu, B.; Li, J. Comparison of assessment of diaphragm function using speckle tracking between patients with successful and failed weaning: A multicentre, observational, pilot study. BMC Pulm. Med. 2022, 22, 459. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, S.J.; Hatam, N.; Goetzenich, A.; Marx, G.; Autschbach, R.; Heunks, L.; Bickenbach, J.; Bruells, C.S. Speckle tracking ultrasonography as a new tool to assess diaphragmatic function: A feasibility study. Ultrasonography 2022, 41, 403. [Google Scholar] [CrossRef] [PubMed]
- Chino, K.; Ohya, T.; Katayama, K.; Suzuki, Y. Diaphragmatic shear modulus at various submaximal inspiratory mouth pressure levels. Respir. Physiol. Neurobiol. 2018, 252, 52–57. [Google Scholar] [CrossRef]
- Bachasson, D.; Dres, M.; Niérat, M.C.; Gennisson, J.L.; Hogrel, J.Y.; Doorduin, J.; Similowski, T. Diaphragm shear modulus reflects transdiaphragmatic pressure during isovolumetric inspiratory efforts and ventilation against inspiratory loading. J. Appl. Physiol. 2019, 126, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Aarab, Y.; Flatres, A.; Garnier, F.; Capdevila, M.; Raynaud, F.; Lacampagne, A.; Chapeau, D.; Klouche, K.; Etienne, P.; Jaber, S.; et al. Shear wave elastography, a new tool for diaphragmatic qualitative assessment: A translational study. Am. J. Respir. Crit. Care Med. 2021, 204, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Jonkman, A.H.; de Korte, C.L. Shear wave elastography of the diaphragm: Good vibrations? Am. J. Respir. Crit. Care Med. 2021, 204, 748–750. [Google Scholar] [CrossRef] [PubMed]
- Khurana, J.; Gartner, S.C.; Naik, L.; Tsui, B.C. Ultrasound identification of diaphragm by novices using ABCDE technique. Reg. Anesth. Pain Med. 2018, 43, 161–165. [Google Scholar] [CrossRef]
- Sanchez de Toledo, J.; Munoz, R.; Landsittel, D.; Shiderly, D.; Yoshida, M.; Komarlu, R.; Wearden, P.; Morell, V.O.; Chrysostomou, C. Diagnosis of abnormal diaphragm motion after cardiothoracic surgery: Ultrasound performed by a cardiac intensivist vs. fluoroscopy. Congenit. Heart Dis. 2010, 5, 565–572. [Google Scholar] [CrossRef]
- Garofalo, E.; Bruni, A.; Pelaia, C.; Landoni, G.; Zangrillo, A.; Antonelli, M.; Conti, G.; Biasucci, D.G.; Mercurio, G.; Cortegiani, A.; et al. Comparisons of two diaphragm ultrasound-teaching programs: A multicenter randomized controlled educational study. Ultrasound J. 2019, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Pirompanich, P.; Romsaiyut, S. Use of diaphragm thickening fraction combined with rapid shallow breathing index for predicting success of weaning from mechanical ventilator in medical patients. J. Intensive Care 2018, 6, 6. [Google Scholar] [CrossRef]
- Hellyer, N.J.; Andreas, N.M.; Bernstetter, A.S.; Cieslak, K.R.; Donahue, G.F.; Steiner, E.A.; Hollman, J.H.; Boon, A.J. Comparison of diaphragm thickness measurements among postures via ultrasound imaging. PMR 2017, 9, 21–25. [Google Scholar] [CrossRef]
- Wait, J.L.; Nahormek, P.A.; Yost, W.T.; Rochester, D.P. Diaphragmatic thickness-lung volume relationship in vivo. J. Appl. Physiol. 1989, 67, 1560–1568. [Google Scholar] [CrossRef]
- McKenzie, D.; Gandevia, S.; Gorman, R.; Southon, F. Dynamic changes in the zone of apposition and diaphragm length during maximal respiratory efforts. Thorax 1994, 49, 634–638. [Google Scholar] [CrossRef]
- Sarwal, A.; Walker, F.O.; Cartwright, M.S. Neuromuscular ultrasound for evaluation of the diaphragm. Muscle Nerve 2013, 47, 319–329. [Google Scholar] [CrossRef]
- Saad, M.; Pini, S.; Danzo, F.; Mandurino Mirizzi, F.; Arena, C.; Tursi, F.; Radovanovic, D.; Santus, P. Ultrasonographic assessment of diaphragmatic function and its clinical application in the management of patients with acute respiratory failure. Diagnostics 2023, 13, 411. [Google Scholar] [CrossRef]
- Harris, R.; Giovannetti, M.; Kim, B. Normal ventilatory movement of the right hemidiaphragm studied by ultrasonography and pneumotachography. Radiology 1983, 146, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Gerscovich, E.O.; Cronan, M.; McGahan, J.P.; Jain, K.; Jones, C.D.; McDonald, C. Ultrasonographic evaluation of diaphragmatic motion. J. Ultrasound Med. 2001, 20, 597–604. [Google Scholar] [CrossRef]
- Kantarci, F.; Mihmanli, I.; Demirel, M.K.; Harmanci, K.; Akman, C.; Aydogan, F.; Uysal, O. Normal diaphragmatic motion and the effects of body composition. J. Ultrasound Med. 2004, 23, 255–260. [Google Scholar] [CrossRef]
- Spiesshoefer, J.; Herkenrath, S.; Henke, C.; Langenbruch, L.; Schneppe, M.; Randerath, W.; Boentert, M. Evaluation of respiratory muscle strength and diaphragm ultrasound: Normative values, theoretical considerations, and practical recommendations. Respiration 2020, 99, 369–381. [Google Scholar] [CrossRef]
- Boussuges, A.; Rives, S.; Finance, J.; Chaumet, G.; Vallée, N.; Risso, J.-J.; Brégeon, F. Ultrasound assessment of diaphragm thickness and thickening: Reference values and limits of normality when in a seated position. Front. Med. 2021, 8, 1982. [Google Scholar] [CrossRef] [PubMed]
- Haaksma, M.E.; van Tienhoven, A.J.; Smit, J.M.; Heldeweg, M.L.A.; Lissenberg-Witte, B.I.; Wennen, M.; Jonkman, A.; Girbes, A.R.J.; Heunks, L.; Tuinman, P.R. Anatomical variation in diaphragm thickness assessed with ultrasound in healthy volunteers. Ultrasound Med. Biol. 2022, 48, 1833–1839. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).